
Abstract
Background:
Electrochemiluminescence (ECL) assays have shown promise for enhancing the prediction of type 1 diabetes (T1D) with autoantibodies. We thus studied relatives of T1D patients to determine whether ECL assays can be used to refine risk assessments for T1D among individuals either positive for single GADA or single mIAA autoantibodies.
Subjects and Methods:
TrialNet Pathway to Prevention (PTP) study participants with either GADA or mIAA single autoantibodies were tested for ECL positivity during their participation in the TrialNet PTP study. Those ECL positive (ECL+) were compared with those ECL negative (ECL−) for conversion to multiple autoantibodies, 6-month glycemic progression (PS6M), and the progression to T1D.
Results:
The progression to multiple autoantibodies was significantly higher for those GADA/ECL+ (n = 107) than those GADA/ECL− (n = 78) (P = 0.001) and for those mIAA/ECL+ (n = 24) than those mIAA/ECL− (n = 63) (P < 0.001). The hazard ratios with 95% confidence intervals were 3.42 (1.58–7.39; P < 0.01) for GADA and 8.15 (3.02–22.00; P < 0.001) for mIAA. GADA/ECL+ and mIAA/ECL+ participants had significantly higher PS6M values than their ECL− counterparts (P = 0.001 for GADA and P = 0.009 for mIAA). Of those GADA/ECL+, 14% progressed to T1D; of those mIAA/ECL+, 17% progressed to T1D. Only 1 individual (positive for GADA) of the 141 who was ECL− progressed to T1D (median follow-up: 5 years).
Conclusion:
ECL measurements appear to have utility for natural history studies and prevention trials of individuals with single autoantibodies. Those ECL+ are at appreciable risk for developing multiple autoantibodies and for glycemic progression toward T1D, whereas those ECL− are at very low risk.
Introduction
R
Risk could also vary according to a characteristic of the single autoantibody that is present, such as autoantibody affinity, which can be defined as the strength of interaction between an epitope and an autoantibody binding site. Recent evidence suggests that assessments of islet autoantibodies using a technique that quantitates electrochemical reactions, electrochemiluminescence (ECL), are indicative of autoantibody affinity and improve the overall prediction of T1D. 4 –7 Thus, we have studied TrialNet Pathway to Prevention (PTP) participants, all relatives of T1D patients, to determine whether ECL assays can be used to refine risk assessments for T1D among individuals either positive for GADA alone or mIAA alone.
Subjects and Methods
Subjects
The PTP study (formerly called the TrialNet Natural History study) has previously been described. 8 Relatives of T1D patients positive for at least one autoantibody are followed with 2-h oral glucose tolerance test (OGTT) surveillance for the development of T1D. Samples from a subset of the autoantibody-positive participants were tested for ECL-GADA and ECL-IAA during their participation in the PTP. The samples used in the analysis were based on sample availability; most samples were obtained at screening. From that subset, participants with either single biochemical autoantibody positivity for GADA or mIAA were then selected for analysis.
Procedures
All PTP participants had OGTTs performed semiannually before 2012. Subsequently, those considered to be at lower risk were followed on an annual basis. (ECL has not been used to determine the frequency of follow-up in the PTP.) For the OGTTs, samples were obtained in the fasting state, and at 30, 60, 90, and 120 min after the ingestion of a 1.75 g per kilogram glucose dose (maximum: 75 g of carbohydrate). Glucose and C-peptide measurements were obtained from the samples. Another OGTT was performed for diagnostic confirmation if a fasting glucose value was ≥126 mg/dL and/or a 2-h glucose value was ≥200 mg/dL. If both thresholds were not exceeded on the confirmatory OGTT, participants were followed semiannually. Diagnoses of T1D were also made from clinical presentation. T1D was diagnosed according to American Diabetes Association criteria.
All of those included in the analyses had measurements of GADA, mIAA, IA-2A, ZnT8A, and islet cell autoantibodies. There was confirmation for all single autoantibodies according to the PTP protocol. The progression to multiple autoantibodies at follow-up visits was not confirmed, since that is not part of the PTP protocol. Islet cell autoantibodies were not considered in the analysis due to overlap with several biochemical autoantibodies and resultant uncertainty in interpretation. Since ZnT8A measurements were not consistently performed during follow-up, only GADA, mIAA, and IA-2A were considered for analyses of progression from single to multiple (≥2) autoantibodies.
ECL assays
ECL assays for both mIAA and GADA have been previously described. 4 –7 Briefly, serum samples were mixed with both SULFO-TAG- and biotin-labeled antigen proteins (either proinsulin or GADA) for overnight incubation at 4°C. The antigen–antibody complexes with biotin were captured by a streptavidin-coated plate, and SULFO-TAG gave the signals with ECL. The results were expressed as an index against internal standard positive controls of either insulin or GADA monoclonal antibody. The ECL assay cutoff indexes of 0.006 for mIAA or 0.023 for GADA were set at the 99th percentile over 100 healthy controls, and the ECL interassay coefficiencies of variation were 4.8% (n = 20) for mIAA and 8.8% (n = 10) for GADA, respectively. In the 2015 IASP Workshop, sensitivities and specificities for the ECL assays were 60% and 98%, respectively, for mIAA, and 78% and 96%, respectively, for GADA, among patients with newly diagnosed T1D.
Islet autoantibody radioassay
The radioassays for mIAA, GADA, IA-2A, and ZnT8A used in the present study were all performed in the Barbara Davis Center laboratory as the TrialNet reference laboratory and the assay methods were previously published. 9 –11 In the 2015 IASP Workshop, sensitivities and specificities were 52% and 100%, respectively, for mIAA, 82% and 99%, respectively, for GADA, 72% and 100%, respectively, for IA-2A, and 70% and 97%, respectively, for ZnT8A.
Data analysis
T-tests and chi-square tests were utilized to compare groups. Kaplan–Meier curves were generated to examine the occurrence of multiple autoantibodies, and differences between the curves were assessed with log-rank tests. Cox proportional hazards regression was used to obtain hazard ratios with 95% confidence intervals. ECL measurements were performed before the first OGTT. Systematic surveillance for progression to the first occurrence of multiple autoantibodies and to diagnosis was not initiated until after that OGTT. There were no significant differences in the intervals from the ECL determinations to the first OGTTs between those ECL+ and those ECL− for either GADA or mIAA. The 6-month Glycemia Progression Scale (PS6M) 12 was calculated. This is a measure of change in the glucose sum (from 30-, 60-, 90-, and 120-min values) of OGTTs from baseline to 6 months after baseline. The PS6M indicates the difference between the actual glucose sum at 6 months and the glucose sum at 6 months that would be expected for nonprogressors to T1D. Statistical significance was based on two-sided P-values.
Results
Characteristics of the PTP participants who were included in the analysis are shown in Table 1. There were no significant differences in the mean ± SD ages between the ECL groups for either those with only GADA (GADA/ECL+ vs. GADA/ECL−) or those with only mIAA (mIAA/ECL+ vs. mIAA/ECL−). The percentage female was significantly higher in the mIAA/ECL+ group than in the mIAA/ECL− group (56% vs. 29%; P = 0.028).
Mean ± SD.
P = 0.028 for difference (GADA only = single autoantibody positivity for GADA; mIAA only = single autoantibody positivity for mIAA).
ECL, electrochemiluminescence.
The GADA/ECL+ and mIAA/ECL+ individuals had substantially higher rates of progression from single to multiple autoantibodies than those ECL−, as reflected by the hazard ratios shown in Table 2 (GADA: 3.42 [95% CI: 1.58–7.39], P = 0.002; mIAA: 8.15 [95% CI: 3.02–22.00], P < 0.001). The table also shows the appreciably higher 3-year risk estimates of those who were ECL+. Consistent with the hazard ratios, the cumulative incidence for the progression to multiple autoantibodies (Fig. 1) was greater for both GADA/ECL+ (P = 0.001) and mIAA/ECL+ (P < 0.001).
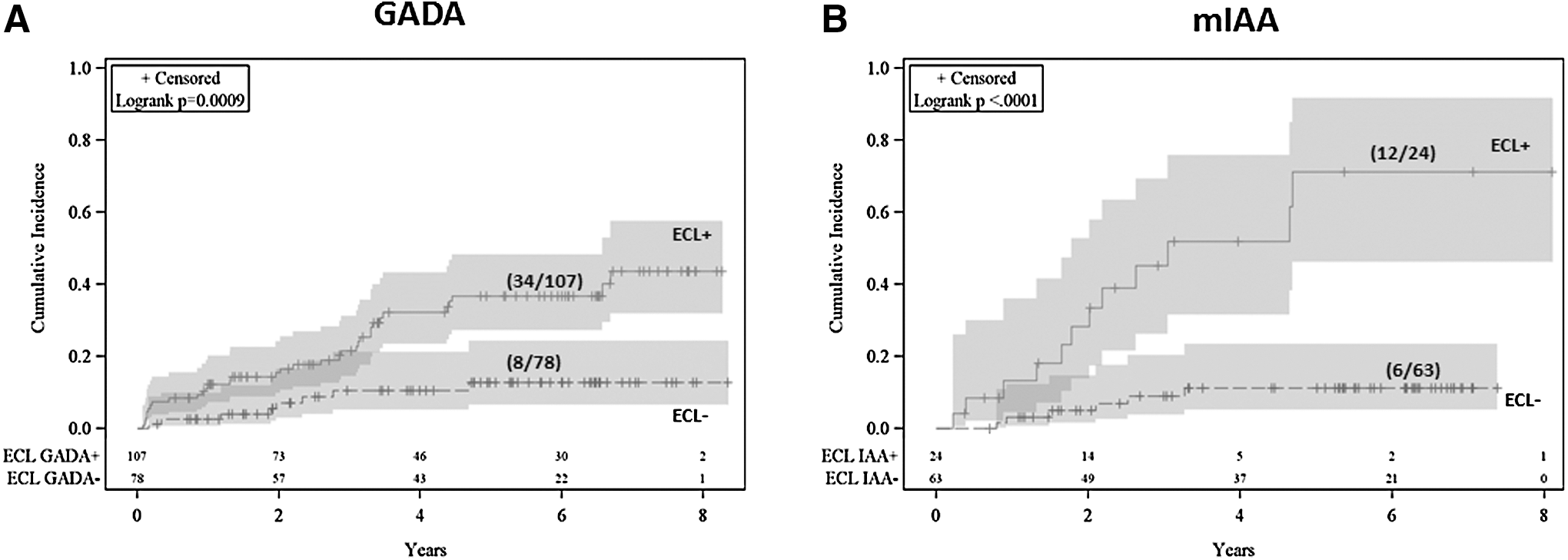
Shown are cumulative incidence curves according to ECL status for progression to multiple autoantibodies among Pathway to Prevention participants with single GADA autoantibodies
P = 0.002.
P < 0.001 (GADA only = single autoantibody positivity for GADA; mIAA-only = single autoantibody positivity for mIAA).
Table 3 shows PS6M values of PTP participants with single GADA or single mIAA autoantibodies according to their ECL status. The mean PS6M values of both the GADA/ECL+ and mIAA/ECL+ participants were greater than zero (expected value for nonprogressors). In contrast, the mean PS6M values were less than zero for those ECL−. GADA/ECL+ and mIAA/ECL+ participants both had significantly higher PS6M values than their ECL− counterparts (P = 0.001 for GADA and P = 0.009 for mIAA).
Mean ± SD (GADA only = single autoantibody positivity for GADA; mIAA only = single autoantibody positivity for mIAA).
Of the 107 who were GADA/ECL+, 15 (14%) progressed to T1D (median follow-up from the first OGTT to the diagnosis of T1D: 4.6 years), and of the 24 mIAA/ECL+, 4/24 (17%) progressed to T1D (median follow-up: 3.1 years). Only 1 of the 78 in the GADA/ECL− group progressed to T1D; none of the 63 in the mIAA/ECL− group progressed to T1D. The median follow-up for both the GADA/ECL− and mIAA/ECL− groups was 5.0 years.
Discussion
The number of autoantibodies is a known predictor of T1D. 1,2 However, other factors such as autoantibody affinity and autoantibody levels have been shown to influence the risk for T1D. 13,14 Since ECL assays are indicative of autoantibody affinity, we examined their use for refining the prediction of progression toward T1D in individuals with one positive autoantibody. The findings clearly showed that ECL measurements can be used for this purpose in those with either single GADA or single mIAA autoantibodies. Those who were ECL+ had a higher rate of progression to multiple autoantibodies, a greater increase in glycemia over 6 months, and a higher likelihood of being diagnosed with T1D.
It appears that the risk for T1D of the single autoantibody ECL+ relatives might not be sufficient for inclusion in prevention trials with T1D as an endpoint. However, their rate of progression to multiple autoantibodies and their degree of glycemic progression suggest that they could be suitable for trials that utilize those endpoints. The rate of progression to multiple autoantibodies would likely have been higher if ZnT8A had also been systematically measured during follow-up.
The negative PS6M values of those ECL− indicate that they tended to have even less glycemic progression than nonprogressors (expected to have on average a PS6M value of zero). However, a small number of those ECL− did develop multiple autoantibodies. Thus, although ECL− individuals would not be suitable for clinical trials, it appears that they are still at some risk, although a very low one, for progressing to T1D. The lack of short-term glycemic progression among those ECL− suggests that the pathologic process has not as yet had appreciable metabolic consequences. It would be of interest for future studies to determine whether ECL positivity is a prerequisite for glycemic progression.
The basis for the relationship between T1D risk and autoantibody affinity (as indicated by ECL status) is not known. The findings are consistent with other reports showing the enhanced prediction accuracy of ECL measurements. 4 –7 The finding in the present report of a greater progression to multiple autoantibodies among those ECL+ is similar to the finding from a prior TrialNet study. 6 The numbers included in the present study were smaller, since we excluded those who did not have the requisite OGTTs for the PS6M analysis. Also, the prior study did not include hazard ratios for progression to multiple autoantibodies. An analysis of progression to multiple autoantibodies was included in the present report, since it is complementary to the PS6M metabolic progression analysis. The findings showed that among the same participants, ECL positivity concurrently predicted both greater metabolic progression and autoantibody progression. There are no prior studies of the influence of ECL on both glycemic progression and the progression to multiple autoantibodies in the same cohort of individuals with single autoantibodies.
Including both the PS6M and the progression to multiple autoantibodies as endpoints in the same cohort shows how the PS6M can contribute to the efficiency of studies. The PS6M 12 was developed for use as an indicator of glycemic progression over a fixed 6-month period. A rationale for its development was that it could be useful as an endpoint for assessing short-term effects of T1D markers or as an intermediate endpoint for T1D prevention trials. The findings in this report provide support for its utility in those research settings. Differences between the ECL+ and ECL− groups were statistically significant for the PS6M as an endpoint after a fixed follow-up of only 6 months; the analysis of progression to multiple autoantibodies entailed an open-ended longer period of follow-up.
There were study limitations that include the following: samples were obtained on the basis of availability; some samples were not collected at screening; and the protocol was changed in 2012 to annual follow-up for low-risk participants. With regard to the last limitation, the vast majority of those studied would have entered the PTP before 2012 and ECL status was not a criterion for follow-up. Although it is possible that these limitations could have introduced bias, the directionality of any bias is not evident.
In conclusion, ECL measurements appear to have utility for natural history studies and prevention trials of individuals who have single positive autoantibodies. Those ECL+ could be included in studies of autoantibody and glycemic progression. It would appear that these individuals deserve systematic surveillance for progression to T1D. In contrast, surveillance of those ECL− could be performed on an infrequent basis.
Footnotes
Acknowledgments
The sponsor of the study was the Type 1 Diabetes TrialNet Pathway to Prevention Study Group. Type 1 Diabetes TrialNet Pathway to Prevention Study Group is a clinical trials network funded by the National Institutes of Health (NIH) through the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institute of Allergy and Infectious Diseases, and The Eunice Kennedy Shriver National Institute of Child Health and Human Development through the cooperative agreements. TrialNet is funded by NIH grants U01 DK061010, U01 DK061034, U01 DK061042, U01 DK061058, U01 DK085465, U01 DK085453, U01 DK085461, U01 DK085463, U01 DK085466, U01 DK085499, U01 DK085504, U01 DK085505, U01 DK085509, U01 DK103180, U01-DK103153, U01-DK085476, U01-DK103266, and the Juvenile Diabetes Research Foundation International (JDRF).
Author Disclosure Statement
No competing financial interests exist with regard to this article for any of the authors. J.M.S. analyzed data and wrote the manuscript. L.Y. performed the assays and reviewed the manuscript. J.S.S. conducted the study and reviewed the manuscript. J.P.K. conducted the study and reviewed the manuscript. P.A.G. conducted the study and reviewed the manuscript. D.B. performed programming and provided statistical support. D.M. performed the assays and reviewed the manuscript. J.P.P. conducted the study and reviewed the manuscript. A.K.S. conducted the study, reviewed the manuscript, and assisted in writing the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.