
Abstract
Background:
We compared glycemia, treatment satisfaction, sleep quality, and cognition using a nighttime Android-based hybrid closed-loop system (Android-HCLS) with sensor-augmented pump with low-glucose suspend function (SAP-LGS) in people with type 1 diabetes.
Materials and Methods:
An open-label, prospective, randomized crossover study of 16 adults (mean [SD] age 42.1 [9.6] years) and 12 adolescents (15.2 [1.6] years) was conducted. All participants completed four consecutive nights at home with Android-HCLS (proportional integral derivative with insulin feedback algorithm; Medtronic) and SAP-LGS. Primary outcome: percent continuous glucose monitoring (CGM) time (00:00–08:00 h) within target range (72–144 mg/dL). Secondary endpoints: percent CGM time above target (>144 mg/dL); below target (<72 mg/dL); glycemic variability (SD); symptomatic hypoglycemia; adult treatment satisfaction; sleep quality; and cognitive function.
Results:
The primary outcome for all participants was not statistically different between Android-HCLS and SAP-LGS (mean [SD] 59.4 [17.9]% vs. 53.1 [18]%; p = 0.14). Adults had greater percent time within target range (57.7 [18.6]% vs. 44.5 [14.5]%; p < 0.006); less time above target (42.0 [18.7]% vs. 52.6 [16.5]%; p = 0.034); lower glycemic variability (35 [10.7] mg/dL vs. 46 [10.7] mg/dL; p = 0.003); and less (median [IQR]) time below target (0.0 [0.0–0.4]% vs. 0.80 [0.0–3.9]%; p = 0.025). In adolescents, time below target was lower with Android-HCLS vs. SAP-LGS (0.0 [0.0–0.0]% vs. 1.8 [0.1–7.9]%; p = 0.011). Nocturnal symptomatic hypoglycemia was less (1 vs. 10; p = 0.007) in adolescents, but not adults (5 vs. 13; p = 0.059). In adults, treatment satisfaction increased by 10 points (p < 0.02). Sleep quality and cognition did not differ.
Conclusions:
Android-HCLS in both adults and adolescents reduced nocturnal hypoglycemia and, in adults, improved overnight time in target range and treatment satisfaction compared with SAP-LGS.
Introduction
For
Insulin pumps with a glucose-sensing function integrated as part of a single platform, referred to as SAP, have recently been further enhanced by a low-glucose suspend function (SAP-LGS) that halts insulin delivery when sensor glucose level falls below a predetermined threshold. SAP-LGS has been shown to reduce the duration and severity of hypoglycemia in comparison with SAP alone. 10,11 However, while suspension of insulin delivery reduces hypoglycemia, it does not directly address elevated glucose levels. 10 Data comparing CLS with SAP-LGS are limited to early feasibility studies, which lacked statistical power and did not demonstrate increased time in the target glucose range. 12,13
Previous studies evaluating SAP therapy in the management of type 1 diabetes have reported differences in glycemic outcomes that were, in part, dependent upon the age of participants. These observations were due to differences in utilization of the technology. 14,15 The relative performance of CLS in adult and adolescent populations remains to be fully explored. Initial data suggest favorable perceptions from adolescents using the new technology, although this merits further investigation in a wider group. 16 The impact of CLS upon sleep quality and cognitive function has not been explored previously. Few CLS studies have addressed important nonglycemia-related endpoints.
We aimed to compare nocturnal glucose control while using a CLS overnight (reverting to SAP-LGS during daytime) versus SAP-LGS used both during the night and daytime in adults and adolescents with type 1 diabetes. We hypothesized that overnight CLS would increase time in target glucose range and reduce hypoglycemia at night in adults and adolescents in comparison with SAP-LGS. We also aimed to determine participant satisfaction with the technology and its effect on sleep quality and cognitive performance.
Materials and Methods
The study was an open-label, prospective, randomized crossover study undertaken between February 2014 and October 2015. It compared glycemic control using an Android-based hybrid CLS (Android-HCLS), described below, with SAP-LGS at nighttime in adults and adolescents with type 1 diabetes. During the day, all participants used SAP-LGS. The study took place in Australia: adult participants attended St. Vincent's Hospital, Melbourne, and adolescents attended Princess Margaret Hospital for Children, Perth. Written informed consent was obtained from all participants, or their guardians, at screening. Following consent, participants were assigned four nights at home of SAP-LGS and Android-HCLS in random order. The study was approved by the Research and Ethics Committees of both hospitals.
Participants
Adult participants were recruited from the clinics of three university hospitals in Melbourne (St. Vincent's Hospital, The Alfred Hospital, and the Royal Melbourne Hospital). Adolescent participants were recruited from clinics at Princess Margaret Hospital.
Criteria for inclusion were defined so as to minimize risk to participants in a study involving a prototype investigational device being tested at home. Inclusion criteria were age ≥24 years (adults) or 12–18 years (adolescents); type 1 diabetes of >1 year duration; fasting C-peptide level <0.15 ng/mL; using insulin pump therapy for >3 months with appropriate use of a bolus calculator; HbA1c level <8.5% (<69 mmol/mol); and willing and able to undertake the study protocol. Exclusion criteria were total insulin (100 IU/mL) dose >150 units per day; an episode of diabetic ketoacidosis within the last 4 weeks; >2 severe hypoglycemic episodes within the last 12 months; renal impairment (eGFR <60 mL/min/1.73 m2); and pregnancy, breastfeeding, or planned pregnancy within the study time frame.
Study devices
The Android-HCLS used was a prototype hybrid CLS requiring participant-initiated bolus administration for meals. It incorporated an insulin pump (Veo, Medtronic, Northridge, CA), glucose sensor, and transmitter (Enlite, Medtronic) linked through a translator to an adaptive proportional integral derivative algorithm with insulin feedback (Version 4.0; Medtronic) embedded in an Android phone, as described previously. 13 Data were transmitted to the cloud in real time, allowing remote monitoring.
Study protocol
At the screening visit, a physical examination was performed and demographic data recorded (Fig. 1). Venous blood was drawn for HbA1c, anti-insulin antibodies, and fasting C-peptide levels. Study questionnaires were completed.
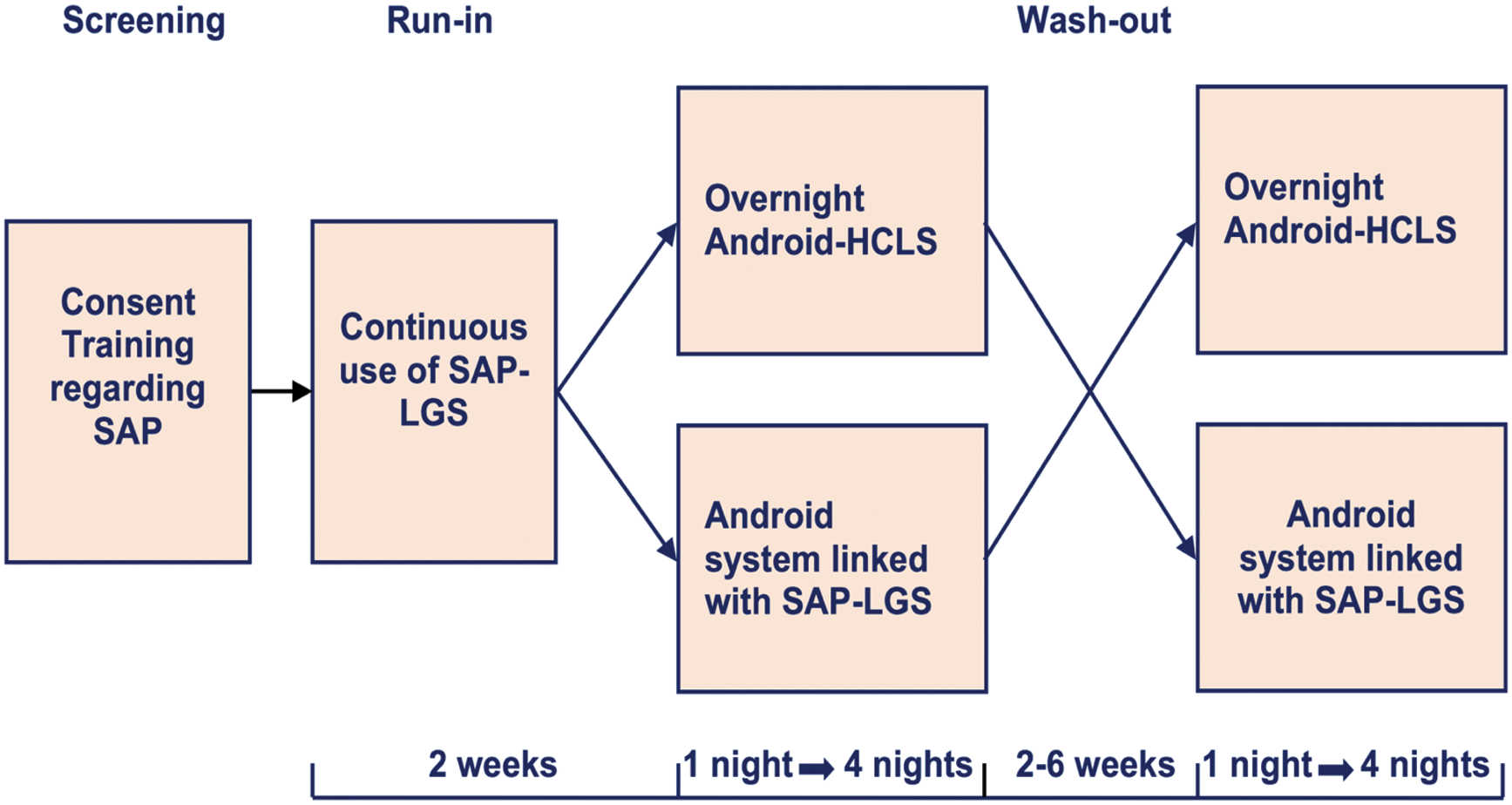
Overview of study design.
Participants were provided with study devices, in which the insulin delivery parameters from their own pumps were entered. All received training regarding the use of SAP-LGS and were advised to calibrate sensors at least twice daily as per the manufacturer's instructions. The glucose threshold for suspension of insulin delivery was set at 60 mg/dL. All underwent a 2-week run-in period to familiarize participants with the protocol, to optimize insulin delivery parameters, and to confirm protocol adherence. Participants were requested to use SAP-LGS >80% of the time and upload their pump to web-based software (Carelink™, Minimed, Medtronic, Northridge, CA) once per week during run-in. They were instructed to administer all bolus insulin using the inbuilt bolus calculator.
Two weeks following screening, participants were admitted for one night to the Clinical Trials Centre (CTC). Those randomized to Android-HCLS received training regarding the operation of the system, which was activated during the overnight stay in the CTC. Those randomized to SAP-LGS continued in SAP-LGS mode overnight and had their diabetes education reviewed. Participants then used SAP-LGS continuously until their corresponding at-home study, which was scheduled within 2 weeks of randomization.
During the four consecutive nights of the at-home study, participants assigned Android-HCLS were instructed to activate the closed loop 2 h following the evening meal and resume SAP-LGS on waking, before breakfast. Participants were required to calibrate just before activating the closed-loop mode. If the calibration glucose was above target, a correction was automatically delivered by the closed-loop system. Participants were not instructed to routinely check finger-prick glucose readings or to calibrate overnight once CLS was active.
Those assigned to SAP-LGS continued overnight in this mode with remote monitoring activated, but without the CLS function engaged. They were advised to check their glucose levels before retiring and respond as per usual practice to match the calibration reading required for CLS initialization. During both Android-HCLS and SAP-LGS phases, all participants consumed 300 mL of orange juice between 02:00 and 03:00 h on the fourth night at home. No restrictions were placed on diet or physical activity.
Participants undertook the alternate study arm between 2 and 6 weeks following completion of the first at-home phase. Between study phases, participants continued using SAP-LGS. The number of contacts between the research teams and participants for Android-HCLS and SAP-LGS study phases were matched.
Randomization and masking
Randomization was performed by coauthors, A.S. and M.I.D.B., using a computerized sequence generation, which was concealed through sealed opaque envelopes until run-in completion. Following the run-in, study sequence for participants was unmasked by the research nurses (M.M.L., J.C.H., and C.L.B.). Neither members of the study team nor participants were blinded to the intervention.
Study assessments
Glycemia, insulin delivery, C-peptide, and anti-insulin antibody status
Glucose sensor, glucose meter, carbohydrate intake, and insulin delivery data were uploaded. Symptomatic hypoglycemia confirmed by a finger-prick capillary glucose measurement of <72 mg/dL was documented.
Blood samples for 1,5-anhydroglucitol, a dietary monosaccharide lost in the urine with glycosuria and hyperglycemia, 17 were collected on the morning before the first night at home and on the morning following the fourth night at home and analyzed on a single run using a spectrophotometric assay (Glycomark, Inc., New York, NJ) on a Cobas Integra 400+ autoanalyzer (Roche, Switzerland) with an intra-assay CV <5% and the operator masked to sample identity and order. HbA1c was measured by HPLC in a routine clinical laboratory. C-peptide was measured by chemiluminescent microparticle immunoassay (Abbott Architect; Abbott Laboratories, Abbot Park, IL) with a lower limit of quantification of 0.03 nmol/L. Plasma anti-insulin antibodies were measured by an in-house radioimmunoassay, adapted from a published method. 18
Satisfaction with diabetes treatment
At baseline, adults completed the diabetes treatment satisfaction questionnaire (DTSQ) status (DTSQs) 19 and, after four nights of Android-HCLS at home, they completed the DTSQ change version (DTSQc). 20 Instructions were adapted for the study design, comparing Android-HCLS experiences with usual treatment.
Diabetes distress and fear of hypoglycemia
At baseline, diabetes distress was assessed by Problem Areas in Diabetes (PAID) 21 and fear of hypoglycemia by Hypoglycemia Fear Survey, version 2 (HFS-II) 22 or Children's Hypoglycemia Fear Survey (CHFS). 23
Cognitive functioning
During the at-home Android-HCLS and SAP-LGS phases, participants self-administered cognitive assessments twice daily (AM and PM), including the Stanford Sleepiness Scale (assessing self-reported alertness) 24 and self-administered objective cognitive function tasks (Cogstate). 25 CogState (detection and identification) tasks were presented on a laptop computer and required participants to make a speedy response as soon as a playing card flipped over. Total task duration was ∼5 min. Performance metrics were correct response time and accuracy (percentage correct). Individual data points were excluded if blood glucose was <72 or >270 mg/dL either during or within 45 min of the test session commencing.
Sleep quality
Self-reported sleep quality was assessed using a modified Pittsburgh Sleep Quality Index (PSQI) to measure sleep over 1 week. 26 Objective measures of sleep quality were obtained using actigraphy data (total sleep time, sleep onset latency, sleep efficiency, wakefulness after sleep onset, motor activity [total and average activity counts]).
Participant safety
All significant adverse events were collected, including, but not restricted to, severe hypoglycemia and diabetic ketoacidosis. All participants were monitored remotely overnight in real time while on both the Android-HCLS and the SAP-LGS stages by clinical and technical study team members. In addition, each participant had a responsible adult companion, knowledgeable in diabetes care, present during the study nights. A medical and technical helpline was available to all participants. Throughout the study, data related to patient safety were monitored by an independent board. Withdrawal of participants could occur if the investigator or safety monitoring committee deemed that termination was in the best interests of the participant.
Statistical analysis
The standard deviation (SD) for percent time within CGM target range for our study population was estimated at 15% based on data collected previously. 14 Informed by available published data, 27 we anticipated that the Android-HCLS would increase overnight sensor glucose percent time within the target range of 72–144 mg/dL during the at-home phase of the study (primary outcome) from 64% to 78%. It was estimated that 12 participants would provide >80% power at the 5% level to detect this difference in primary outcome between Android-HCLS and SAP-LGS.
Secondary glycemia-related outcomes included percent time above target (>144 mg/dL) and below target (<72 and <54 mg/dL) glucose ranges; area under the curve (AUC) >144 mg/dL; mean sensor glucose; and glycemic variability, as reflected by SD glucose. Exploratory secondary endpoints were treatment satisfaction, cognition, and sleep quality.
Intention-to-treat analyses of glycemic outcomes were restricted to the four nights of at-home data. The prestated definition of overnight was 20:00–08:00 h. This was subsequently modified to 00:00–08:00 h in the light of experience as many adult participants would return from work late in the evening and then eat dinner. The initiation of the Android-HCLS in some instances was close to midnight. Normally distributed data were analyzed using mixed linear models and presented as mean (SD). Variables with non-normal distributions were transformed and, if distribution remained non-normal, nonparametric analyses were performed (Wilcoxon signed-rank test) and data presented as median (interquartile range).
Role of the funding source
The study sponsors had no role in the study design, data collection, interpretation of data, composition of the article, or the decision to submit the article for publication.
Results
We approached 17 adults and 13 adolescents, of whom 16 and 13 (respectively) consented to participate in the study. One adolescent withdrew consent immediately after the screening visit because of the demands associated with the protocol and therefore no data were available for analysis. Data from all 16 adults and 12 adolescents who received intended treatment were analyzed for the primary outcome. Baseline characteristics are summarized in Table 1. Median diabetes distress (PAID) and fear of hypoglycemia (HFS-W) scores were very low, while diabetes treatment satisfaction (DTSQs) was high.
All data are mean (SD), median (IQR) or N.
N = 10. DTSQs: Diabetes Treatment Satisfaction Questionnaire status (scored 0–36); DTSQ items 2 and 3 (scored 0–6); PAID: Problem Areas in Diabetes (scored 0–100); HFS-II: Hypoglycemia Fear Survey, version 2 (scored 0–4); CHFS: Children Hypoglycemia Fear Survey (scored 0–4). All scored such that higher scores reflect greater satisfaction, perceived frequency of hyper/hypoglycemia, diabetes-specific distress, or fear of hypoglycemia.
SD, standard deviation.
Overnight glycemia (00:00–08:00 h)
The primary outcome, percent time within target range (72–144 mg/dL) between 00:00 and 08:00 h, for all study participants did not differ between Android-HCLS and SAP-LGS (mean [SD] 59.4 [17.9]% vs. 53.1 [18]%; p = 0.14). Sensor glucose was significantly higher at 00:00 h for Android-HCLS compared with SAP-LGS, but did not differ at 08:00 h. Percent time <72 mg/dL, percent time <54 mg/dL, and AUC <72 mg/dL were significantly lower with Android-HCLS as was the number of symptomatic hypoglycemic episodes overnight (6 vs. 23; p = 0.0016) and glycemic variability reflected by SD. Other parameters did not differ (Table 2).
Mean (SD).
Median [interquartile range].
Android-HCLS, Android-based hybrid closed-loop system; SAP-LGS, sensor-augmented pump with low-glucose suspend function.
Comparison of Android-HCLS versus SAP-LGS in adults (Table 2) revealed percent time within target range (72–144 mg/dL) with Android-HCLS to be higher. Percent time >144 mg/dL, AUC >144 mg/dL, percent time <72 mg/dL, percent time <54 mg/dL, AUC <72 mg/dL, and glycemic variability reflected by glucose SD were lower with Android-HCLS. The number of symptomatic hypoglycemic episodes overnight with Android-HCLS versus SAP-LGS did not differ significantly in adults (5 vs. 13; p = 0.059).
In the adolescents, there was no difference in percent time within target range (72–144 mg/dL) when comparing Android-HCLS with SAP-LGS. Mean glucose levels were higher, percent time <72 mg/dL and AUC <72 mg/dL were less, and the number of symptomatic hypoglycemic episodes overnight were fewer (1 vs. 10; p = 0.007) in Android-HCLS versus SAP-LGS (Table 2).
There was no evidence of an incremental improvement in glycemia over three successive nights with Android-HCLS (data not shown). Analysis of the data between 02:00 and 06:00 h comparing nights 1–3 versus night 4 when the orange juice was consumed at 02:00 h revealed median [IQR] for AUC >144 mg/dL during Android-HCLS to be higher for all participants on night 4 than on nights 1–3 (73.8 [27.6, 148.0] min·mg/dL vs. 6.3 [0, 49.0] min·mg/dL; p = 0.004), for adults (48.1 [20.1, 174.1] min·mg/dL vs. 6.3 [0, 80.1] min·mg/dL; p = 0.044), or adolescents (96.4 [49.5, 145.7] min·mg/dL vs. 5.3 [0, 33.2] min·mg/dL; p = 0.041). When AUC for night 4 between 02:00 and 06:00 h using Android-HCLS was compared with SAP-LGS for all participants, for adults, or for adolescents, there were no significant differences (data not shown).
There was no effect of randomization order upon glycemic outcomes. No significant impact was observed on the primary endpoint by anti-insulin antibody titer or timing of the evening meal.
Overall glycemia (08:00–08:00 h)
There were no differences in any CGM parameters when comparing Android-HCLS versus SAP-LGS for all participants over the entire day (Table 3). There were no statistically significant differences in the change in 1,5 anhydroglucitol levels between days 1 and 4 during Android-HCLS versus SAP-LGS for all participants (mean [SD] 0.22 [1.03] μg/mL vs. 0.60 [1.00]μg/mL; p = 0.21).
Mean (SD).
Median [interquartile range].
AUC, area under the curve.
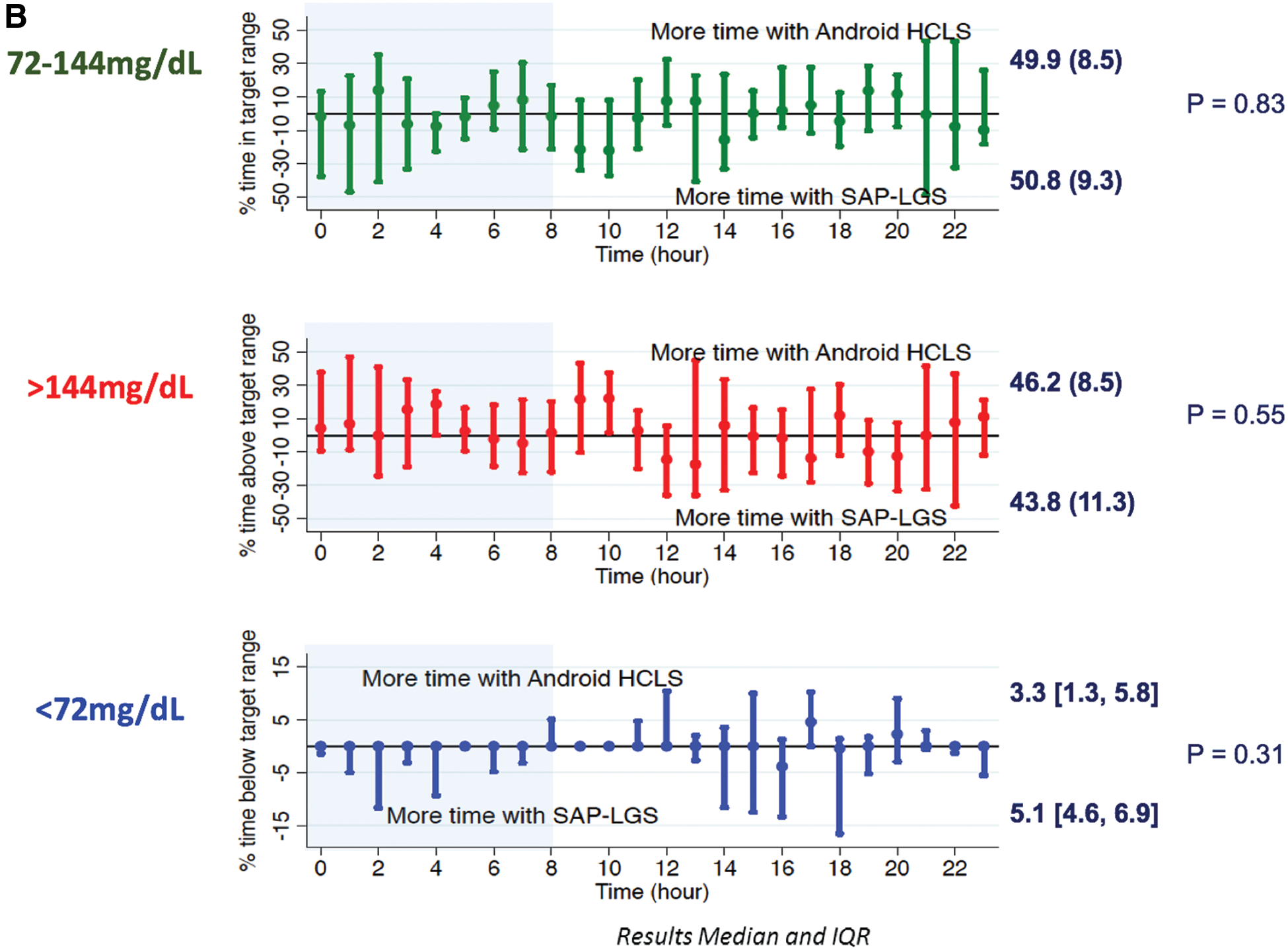
Adults with Android-HCLS compared with SAP-LGS spent a higher percent time in target range (72–144 mg/dL), had a lower mean glucose, and less percent time >144 mg/dL. In adults, the increased time in target range overnight persisted through to the first half of the following day (Fig. 2). In adolescents, there was no difference in percent time in target range (72–144 mg/dL). There was a reduction in SD with Android-HCLS compared with the SAP-LGS phase (Table 3).

Profiles showing the difference between the Android-HCLS activated overnight with reversion to SAP-LGS during the day versus SAP-LGS night and day in adults
Glycemia: adults versus adolescents
At night, between 00:00 and 08:00 h, adults spent less percent time than adolescents within target range (72–144 mg/dL) while on SAP-LGS (mean [SD] 44.5 [14.5]% vs. 64.9 [15.7]%; p = 0.003), but while on Android-HCLS overnight, there was no difference (57.7 [18.6]% vs. 61.7 [17.6]%; p = 0.56). During the day (08:00–00:00 h), there was no difference between adults and adolescents in the percent time in target range (72–144 mg/dL) with overnight SAP-LGS (46.6 [15.9]% vs. 43.7 [8.5]%; p = 0.55), but with overnight Android-HCLS, percent time in target range the next day was greater in adults than adolescents (53.1 [12.1]% vs. 43.9 [10.1]%; p = 0.03). See Figure 3.

Percent time within target range (72–144 mg/dL) in adults versus adolescents at nighttime: 00:00–08:00 h
Android-HCLS utilization and insulin delivery parameters
Adults ate their evening meals at a mean time of 19:45 h (SD = 50 min) and adolescents at 18:15 h (20 min). Android-HCLS activation in adults was at 21:40 h (70 min) and in adolescents 20:30 h (20 min). Adults and adolescents used the Android-HCLS for a mean (SD) of 548.2 (63.0) min/night and 605.6 (124.5) min/night, respectively. The percent time in active closed loop between 00:00 and 08:00 h was 90.0 (7.0)% for adults and 89.1 (16.4)% for adolescents.
During the SAP-LGS study nights (00:00–0800 h), adults experienced a total of 1.1 (1.3) low-glucose alerts, followed by 0.8 (1.05) insulin delivery suspensions for a total duration of 21.3 (31.3) min over the four nights. In adolescents, there were 1.3 (1.4) alerts, 1.1 (1.4) suspensions, and total duration time in suspension of 69.1 (113.6) min over the four nights. The aggregate insulin delivered over the four nights (00:00–08:00 h) did not differ significantly between the Android-HCLS and SAP-LGS either in adults (37.4 [12.6] vs. 39.9 [15.1] units, respectively, p = 0.15) or adolescents (42.1 [8.6] vs. 37.1 [7.3] units, respectively, p = 0.14).
Treatment satisfaction, cognitive functioning, and sleep quality
Compared with their usual diabetes treatment, adults were more satisfied with Android-HCLS (median DTSQc score: +10 points; p < 0.02). Two participants reported being less satisfied with Android-HCLS. Both had issues related to overnight failure in the linkage of the insulin pump with the android controller resulting in alarms and sleep disruption.
For cognitive functioning and sleep quality, data from 170 (66.4%) adult and 122 (63.5%) adolescent tasks were analyzed in those with glucose levels between 72 and 270 mg/dL at the time of testing (Table 4). There were no significant differences in objective cognitive performance or self-reported alertness between Android-HCLS and SAP-LGS in adults or adolescents. Nor were there any clinically significant differences between Android-HCLS and SAP-LGS in the objective sleep parameters measured using Actigraph. There was a small but statistically significant difference in PSQI score, which was worse for Android-HCLS.
Safety and android-HCLS performance
There were no episodes of severe hypoglycemia or diabetic ketoacidosis during the study. All episodes of symptomatic hypoglycemia were recognized and self-treated by the participants. No intervention by the study team remotely monitoring the participants overnight was required for hypoglycemia, hyperglycemia, or ketosis in either study phase. There were six phone contacts for hypoglycemia, all on the SAP-LGS nights. All had been recognized and self-treated by the participants. During the fourth study night, when the orange juice was ingested, there were no major hyperglycemic excursions requiring intervention on the part of the participant or study team and the CL function remained engaged.
Mean Absolute Relative Difference (MARD) between sensor and capillary glucose measurements for adults was 14.9% derived from 1077 paired measurements and 16.7% for adolescents derived from 742 paired measurements and it did not differ between study arms. The loss of closed loop for 10% of the time was due to loss of connectivity between the pump and the android platform with the system defaulting to safe basal insulin delivery, resulting in six phone contacts in the Android-HCLS phase. There were also five such alerts in the SAP-LGS phase. One phone contact in each phase related to difficulties in linking the devices before retiring to bed. There were no major sensor failures on either study phase requiring sensor replacement.
Discussion
This study has demonstrated an improvement in nocturnal glycemic control with short-term Android-HCLS use at home compared with SAP-LGS in adults and adolescents with type 1 diabetes. Both adults and adolescents experienced a reduction in nocturnal hypoglycemia and glycemic variability. In adults, Android-HCLS also resulted in a higher percent time in target range, with reductions in time spent above and below target. In contrast, the main benefit observed in adolescents was limited to less time spent below the glucose target range. On average, adults were more satisfied with Android-HCLS than their usual treatment, with which they were already highly satisfied. The system performed well without any major safety issues. In addition to glycemia-related endpoints, cognition and sleep quality were also explored, although there were no differences between study phases.
Our glucose-related findings in adults are consistent with prior research indicating that CLS technology can improve glycemia, by increasing time in target glucose range, in people with type 1 diabetes compared with SAP therapy. 1,3,4,6,7 To the best of our knowledge, CLS has only been previously compared with SAP-LGS in early feasibility studies in young adults and adolescents, 12,13 with no improvement in time within target glucose range observed. The present study demonstrated an increased time within target glucose range in adults with nocturnal use of an Android-HCLS relative to SAP-LGS.
Hypoglycemia was significantly less frequent in both adults and adolescents compared with SAP-LGS. Evidence suggests that the most consistent benefit of LGS across age groups is in hypoglycemia reduction. 10,11
The threshold for suspension of insulin delivery in our study was set to 60 mg/dL. Bergenstal et al. 10 incorporated a suspend threshold of 70–90 mg/dL. It is possible that incorporating a higher glucose suspend threshold level in our study may have further lowered the rate of hypoglycemia in the SAP-LGS comparator group. The cutoff of 60 mg/dL for LGS was selected because it reflected clinical practice at the adult site at the time of study design (mid-2013) with higher suspend thresholds impacting alarm fatigue and adherence. Nevertheless, the LGS function was triggered on a number of occasions in both adults and adolescents, even in this short-duration study. It is thus likely that without LGS, the percent time spent in low-glucose ranges and the number of hypoglycemic episodes would have been greater during open-loop nights and the relative benefit in hypoglycemia reduction even more apparent.
The differential impact of the Android-HCLS on glycemia in adults and adolescents is of interest. Most protocols investigating the impact of CLS on glycemia have been restricted to either adult participants 4,7,8 or to children and adolescents. 3,9,12,28,29 Those publications reporting outcomes in both adults and adolescents have either been restricted to the clinic 30 or studies have implemented different protocols for the two populations. 1,5,12 Nimri et al. 6 conducted an at-home, randomized crossover study with 11 adults and 12 children/adolescents and De Bock et al. 13 studied four adults and four adolescents using an Android-HCLS, but neither reported results for adults and children separately.
It is relevant that adult behavior during this study was characterized by meals eaten at irregular times, later in the evening, which is common in Australia. This was associated with delayed activation of the Android-HCLS. While our analysis did not indicate that meal time impacted upon the primary outcome, time in target range overnight, we recognize that the study was not powered to investigate this association.
Unlike adults, Android-HCLS did not increase adolescents' percent time within target glucose range. This divergence in outcomes could not be accounted for by differences in Android-HCLS utilization. Despite less pre-study CGM experience, and in particular no prior SAP-LGS experience, utilization of the Android-HCLS by adults and adolescents during the study was equally high. Adolescents achieved excellent overnight glycemic control, as reflected by 64.9% of time between 00:00 and 08:00 h spent within target (72–144 mg/dL) range, even while using SAP-LGS. The recruitment of adolescents into the study and associated study-related activities may have resulted in behavioral changes that increased engagement by participants and their families in their diabetes management, thereby impacting positively on overnight glycemia independently of CLS use. In addition, during the study while adolescent glucose levels overnight were significantly better than the adults, no significant difference was noted during the day. This may have been a reflection of parental oversight and meal choices in the evening/overnight being more guided by parents than in the daytime.
We acknowledge that our results in adolescents contrast with some prior studies reporting improved time in target range with overnight use of CL. 1,9
Thabit et al. 1 reported the percent time in target range as 34.4% during control nights. Adolescents in our study had a very high percent time in target range (61.7%) during nights on the comparator, which would make any further improvement with CLS challenging. It should be noted that our study benchmarked the CLS against a more sophisticated comparator, SAP-LGS, than did previous studies, which did not use LGS. Furthermore, the CLSs, including the control algorithms, used in the two studies were different.
Conversely, despite equivalent times in target range overnight while using Android-HCLS in adults and adolescents, the percent time in target range the following day (08:00–00:00 h) was greater in the adults than the adolescents, which, at 53.1%, was almost 10% greater than the adolescents. Potential contributing factors may relate to bolus insulin administration and the timing of meals, food choices, and increased insulin resistance, which characterize this younger age group. 31 In addition, the adolescents had very limited prior experience with CGM compared with the adults and this may have impacted daytime glycemia while using SAP-LGS. Limiting CL function to the nighttime may not address the most clinically relevant part of the day for adolescents. Engaging a CL function for the entire day may be a more effective strategy to increase time in target glucose range in youth.
Circulating levels of 1,5 anhydroglucitol are inversely related to hyperglycemic excursions over days to weeks, 17 a shorter time frame than HbA1c. While 1,5 anhydroglucitol levels increased during both Android-HCLS and SAP-LGS study phases, reflecting better glucose control, the differences between the two were not statistically significant. It is possible that a CLS targeting overnight glucose levels may have only a minor impact on daytime postprandial glucose excursions determining 1,5 anhydroglucitol. Longer periods of observation with CL activated over the entire 24-h cycle may be needed to be reflected fully in changes in 1,5 anhydroglucitol levels.
Even though the Android-HCLS under evaluation represented a prototype with multiple separate components (pump, sensor, transmitter, translator, and android phone), participant acceptance and utilization of the technology were high. Despite a high level of satisfaction with their usual diabetes treatment at baseline in the 16 adults who completed the study, 14 reported an increment in treatment satisfaction with the system. The two participants who reported a reduction in satisfaction experienced technical difficulties with linking the multiple components.
Current systems are moving toward a single integrated unit. Neither subjective nor objective measures of cognitive functioning differed between Android-HCLS and SAP-LGS for adults or adolescents. It should be recognized that these were exploratory endpoints and that studies with larger numbers and of longer duration may be required to evaluate an effect. The statistical difference observed in sleep quality (PSQI score) may be explained by two outlier nights in a single participant when parenting an unwell restless child resulting in very high scores, indicating poor sleep quality, during the Android-HCLS phase.
As the DTSQ has been validated only in adults, treatment satisfaction was not evaluated in the adolescent group, which requires future investigation. An additional limitation of this study is its short duration. It remains to be determined if glycemic benefits, participants' satisfaction, and their high engagement level over four days can be sustained in the longer term. If so, then these glycemic improvements will translate to a reduction in risk of acute and long-term complications and may improve quality of life. However, it is also possible that this early iteration of the technology (reflected in the numerous separate components comprising the Android-HCLS) may have become burdensome if used beyond four nights. CLS technology is evolving rapidly and current generation devices under evaluation have the CLS as a single platform.
Participants in this study were established users of insulin pumps (and most adults had experience with CGM), had relatively low levels of diabetes distress, high satisfaction, near optimal glycemic control, and were highly motivated to take part in the research. As such, they were ideal candidates for investigating this early phase of new technology. The transition from usual care to the Android-HCLS appeared not to be a major hurdle and this most likely influenced their assessment and satisfaction with the Android-HCLS. To explore expectation and experience of the Android-HCLS, we also conducted a parallel qualitative study, which will be reported separately.
In addition, the centers responsible for the conduct of this study were experienced in the clinical management of type 1 diabetes and research involving diabetes-related technology. Finally, the remote monitoring implemented with this protocol would not be sustainable as part of usual care in Australia. It would be important to evaluate the impact of this technology in those with type 1 diabetes with varying levels of prior engagement with technology and those attending specialist clinics without a research interest in the technology when integrated as part of routine care.
We believe that artificial pancreas technology will continue to improve and may soon become available for in-home clinical use. It is desirable that such technology be available to all who may benefit and wish to use a system, but it is likely that the cost, including of ongoing consumables such as glucose sensors, will be prohibitive for many individuals and payers (including national healthcare systems and Private health insurance companies).
To guide both individual and funding agency decisions in their choice of insulin delivery and glucose monitoring systems, it is important to also provide additional information regarding the advantages and disadvantages of CLS use, such as effects on quality of life, sleep, cognition, and vascular health, all of which can be impaired by type 1 diabetes, and health economics analyses. We assessed quality of life, sleep quality, and cognition in this study, but longer term studies are preferable. We recommend that future closed-loop studies include such additional measures.
In summary, in this comparison of Android-HCLS and SAP-LGS in adults and adolescents who were experienced users of insulin pump therapy, adults experienced increased time spent within the target glycemic range during Android-HCLS, while both participant groups experienced less time spent in the hypoglycemic range. Utilization of the system (and adults' treatment satisfaction) was high. These findings are very promising, but longer term and larger studies with 24-h closed-loop function are now needed in a broader spectrum of people with type 1 diabetes and implemented by mainstream providers more reflective of usual healthcare.
Footnotes
Acknowledgments
The authors thank all study participants and their companions; Dr. Vijaya Sundararajan and Dr. Sara Vogrin for their advice regarding the statistical analysis; Ms. Judy Gooley and Mr. Wade Brownlee for coordination and assistance in the laboratory; Ms. Kate Galloway for assistance in collecting sleep data; Dr. Andrzej Januszewski for 1,5 anhydroglucitol analyses; and Ms. Varuni Obeyesekere for technical assistance in preparing the manuscript. Funding was provided by JDRF International. Material support was provided by Medtronic.
Author Disclosure Statement
A.S., M.I.D.B., D.J., M.M.L., J.C.H., C.B., N.P., L.B., C.H., A.K., K.K., G.M.W., S.T., and E.A.D. declare no competing financial interests. P.G.C. has received lecturing fees from Medtronic. N.K., B.G., and A.R. are employees and stockholders of Medtronic. A.J.J. is on an advisory board for Medtronic Diabetes and Abbott Diabetes and has received honoraria from Medtronic and Sanofi. R.J.M. reports travel support from Novo Nordisk, Sanofi, and Boehringer Ingelheim; is a member of an advisory board for Boehringer Ingelheim; and has received lecture fees from Bayer, Astra Zeneca, MSD, Novartis, Boehringer Ingelheim and Novo Nordisk. J.S. is a member of advisory boards for Roche Diagnostics and Janssen Pharmaceuticals; has received research support from Abbott and Sanofi; and educational support from Lilly, Medtronic, and Novo Nordisk. T.W.J. has received honoraria and speakers' fees from Medtronic. D.N.O. has been on an advisory board for Abbott Diabetes and has received speakers' fees and research support from Medtronic and Novo Nordisk.