
Abstract
Background:
Lipohypertrophy (LH) is a complication of insulin therapy. We assessed LH prevalence, risk factors, insulin usage, and clinical and health economic effects in China.
Methods:
In four cities, 401 adult patients injecting insulin ≥1 year were surveyed for diabetes/insulin injection history and practices, pen needle reimbursement (PNR), and health resource utilization, followed by structured examination and HbA1c testing. Differences between those with and without LH were evaluated by Student's t-test or the Wilcoxon rank sum test. Insulin costs were calculated.
Results:
Patients were 59.6 ± 11.5 years old; 50% male; 93.5% type 2 diabetes. LH prevalence was 53.1%. Compared to those without LH, patients with LH had higher body mass index (BMI; 26 vs. 24.8 kg/m2) and HbA1c (8.2% vs. 7.7% [66 vs. 61 mmol/mol]), took 11 IU (0.13 IU/kg or 31.7%) more insulin costing $1.4 versus $1.0 (RMB 9.5 vs. 6.8) daily, reused PNs more times, and had less PNR (all P ≤ 0.003). LH patients correctly rotated injection sites less often (67.6% vs. 92.3%, P < 0.0001). By stepwise logistic regression, BMI, needle reuse frequency, and PNR remained modestly associated with LH prevalence (odds ratios [OR] <1.9; P ≤ 0.03); weight-adjusted insulin dose and incorrect site rotation showed ORs of nearly 7 and 8.4, respectively (P ≤ 0.001). Extrapolated to 9 million insulin-injecting patients in China and adjusted for therapy adherence, LH-related excess annual insulin consumption cost is estimated at nearly $297 million (RMB 2 billion).
Conclusions:
LH is common in China and associated with worse glycemic control, despite nearly one-third greater insulin consumption, with large cost implications. Proper injection technique education may reduce LH prevalence.
Introduction
L
However, LH is common—when formally sought—and prevalence in various studies ranges from ∼20% to >70%, with higher frequency in subjects who repeatedly inject in restricted areas. 2,3,5 –13 It manifests as swelling and/or hardening of SC adipose tissue at injection or infusion sites. LH may be visible but commonly requires direct palpation (normal adipose tissue should have gelatin-like consistency such that the skin and fat can be pinched nearly together between an examiner's fingers). LH lesions are often described as movable and firm or rubbery, akin to clusters of grapes, but some are softer. The etiology of LH is not well understood; morphologically it appears as heterogeneous but predominantly enlarged adipocytes with varying degrees of fibrous tissue. In one histopathological report, the enlarged adipose cells appeared to extend into the dermis. 14 Chronic insulin therapy, more daily injections, repeated injections (or infusion) into the same body site, and needle reuse have been consistently associated with LH prevalence, which is usually higher in type 1 than type 2 diabetes 3,5 –12 —suggesting a local growth or injury response to insulin deposition by needle or catheter. All types of insulin and all sizes of needles (both pen and syringe), as well as infusion catheters, have been associated with LH. 6,9,10,12,15
LH is important clinically due to reported negative effects on the absorption and action of insulin, as well as increasing insulin uptake variability. 11 –13,16 –22 Nearly all earlier studies reported significant reductions in insulin absorption (some measured as clearance of radio-labeled insulin from injection sites) and glucose-lowering effect and, in some, elevations in HbA1c in affected patients. In one trial (n = 8), the observed differences in postmeal glycemic excursions and CGM profiles with injections into LH versus normal tissue were not significant. 22 Case reports have described marked reductions in insulin total daily dose (TDD) requirements and improvements in both glycemic control and variability when subjects with LH were taught to inject into normal SC tissue. 12,19 In aggregate, this suggests that many patients with LH consume excess insulin due to poor absorption and are at greater risk for glycemic variability and/or hypoglycemia if they occasionally inject into normal adipose tissue; however, the evidence base is of variable quality by today's standards. Teaching patients with LH to inject into healthy tissue and to rotate their injection sites may be effective in improving overall glycemic control. 13
There are no published reports specifically addressing LH in insulin-requiring patients in China. We conducted this study to evaluate LH prevalence there, the clinical characteristics of patients with LH, associated risk factors, injection technique practices, and the differences in insulin consumption compared to patients without LH.
Methods
This multicenter observational study was conducted at university hospital (Class 3) clinics in Beijing, Zhengzhou, Chongqing, and Nanjing; the former two sites were located in provinces that did not provide reimbursement for insulin PNs, whereas the latter two had provincial pen needle reimbursement (PNR) policy in place. Sequential patients attending the clinics were invited to participate in the study. Eligible patients were adults ages 18–80 with diabetes receiving insulin continuously by pen injection for at least 1 year, body mass index (BMI) ≥18.5 kg/m2, and able to respond to the study questionnaire. Exclusion criteria included any history of skin disorders, surgical operation with scars or trauma at insulin injection sites, and hematologic conditions affecting HbA1c assay. We excluded patients taking insulin by syringe or insulin pump, since pens are used by >95% of Chinese patients.
The study questionnaire covered demographics and medical history, diabetes history, injection history and regimen, injection technique training and practices, frequency of hypoglycemia (self-reported), health resource utilization, employment and income status, and impact of diabetes on work status and productivity. A study nurse reviewed patient responses to the survey for quality, accuracy, and completeness. Proper site rotation was defined as moving injections in a sequential manner; patients responded to the rotation question (Yes/No) and then the nurse asked the patient to demonstrate their method of injection site rotation. Only patients who moved sites and spaced injections at least 1 cm from the previous injection were considered to perform correct site rotation. Patients also indicated the size of the injection area they used within the body site, compared to templates such as a stamp, credit card, playing card, or postcard.
Patients next underwent a structured physical examination of height and weight, visual inspection and palpation of all injection sites, and HbA1c testing. Study staff who performed examinations were trained to detect LH, first with models or mannequins, and then with patients known to have LH lesions. Examinations took place in warm rooms (to avoid shivering) with oblique lighting to aid visual inspection, and examiners' hands were washed and warmed. Examiners did not know patient responses to survey questions in about 75% of cases. For abdominal examinations, patients lay supine in their underwear on the examination table with knees drawn up to relax abdominal musculature. Ultrasound gel was applied to examiners' fingers and the subject's abdomen, and palpation of injection areas performed. Light-to-moderate pressure with small sweeps of the finger tips was used to detect LH lesions. When found, lesion dimensions (longest diameter and perpendicular length) were marked with a pen, measured, and recorded. The number of lesions in an area was noted, but dimensions only recorded for the largest lesion. For the thigh, patients were examined sitting with knees bent and feet on the floor. The arm and buttock were similarly evaluated (patient standing for the latter), if the patient injected at such sites. The study was conducted according to Good Clinical Practice standards, CFDA regulations and guidance, and the Declaration of Helsinki. The protocol was approved by the ethics committee at each study hospital, and all subjects provided written informed consent.
Statistical methodology
In a previous worldwide survey concerning Injection Technique practices, 15 31% of insulin-injecting patients in China indicated they had seen “small bumps or swelling at injection sites.” About 12% had swelling in the abdomen when examined by nurses (not specifically trained to detect LH), and another 6% in the thigh. We therefore assumed that prevalence of LH would be ∼15%. For a SE of 2% around the observed prevalence from our study, we needed 319 subjects and increased the sample size to 400 patients across the four study sites.
Estimates of costs associated with LH-related insulin consumption were derived from the study findings. Incremental cost of excess insulin used was estimated by multiplying the observed prevalence of LH, the number of insulin-injecting patients in China corrected for therapy adherence, the observed differences in insulin TDD between the groups with and without LH, and the cost per Unit of insulin in China (0.04 USD or 0.25 RMB) (IMS CHPA, MIDAS Quarterly data, 2Q 2015) (Exchange rate 1 USD = 6.68 RMB, September 5, 2016).
Descriptive statistics (mean, median, SD, or 95% confidence interval [CI]) were developed and contingency tables evaluated using chi-square as well as Student's t-test or the Wilcoxon Rank Sum test. Means or medians were assessed by analysis of variance. Pearson's correlations were calculated between TDD insulin and both BMI and weight. Logistic regression was used to analyze risk factors for LH, including duration of insulin therapy, number of daily injections, gender, BMI, weight-adjusted insulin dose, HbA1c, incorrect site rotation, pen needle (PN) length, PNR, and frequency of PN reuse, to calculate the point estimate and 95% CI of the odds ratio (OR) for each factor. Next, significant risk factors were selected stepwise and subsequent point estimate and OR calculated. Statistical significance was considered at P < 0.05. Statistical calculations were performed with SAS v9.2. This article reports the main clinical findings and analyses of LH-related insulin consumption costs. Other analyses will be prepared separately related to LH and health resource utilization, PNR, income, and employment impact.
Results
Demographics
Of 403 patients who provided informed consent, 401 completed study procedures with results reported here. Table 1 provides clinical and demographic information. Patients were nearly 60 years old, 50% male, with BMI 25.4 kg/m2. More than 98% had some medical insurance; other than one subject in Zhengzhou, subjects there and in Beijing did not have PNR, while 53% and 89% of subjects in Nanjing and Chongqing did, respectively. Patients had diabetes for nearly 12 years, >93% type 2, and had been taking insulin a mean of 5.8, range 1–29.3 years.
Clinical characteristics for all subjects and for those with and without lipohypertrophy, based on responses to questionnaire and confirmed by healthcare professional. Data are represented in n (percentage), unless otherwise stated.
P-value for those with lipohypertrophy versus those without. Hypoglycemia is self-reported within the past 6 months.
BMI, body mass index.
LH findings
Overall LH prevalence was 53.1% (95% CI 48.2–58.0), most commonly found in the abdomen (52.4%), which was used by 391 or 97.5% of subjects, followed by the thigh (LH in 15.5%, 13/84 subjects) and arm (9.4%, 6/64 subjects); LH was not present in the buttocks, but only 29 (7.2%) subjects used this area for injections. In those with LH, a mean of 2.3 (SD 2.2) lesions were found and ranged from 1 to 20. The average length of the longest lesion dimension was 16.1 mm, and maximum 80 mm. We recorded whether LH lesions were visible in the last 110 subjects examined, of whom 45 had LH. In 8% or 17.8% of these subjects, LH lesions were visible. LH was present in 19/26 (73.1%) subjects with type 1 diabetes versus 193/374 subjects (51.6%) with type 2 diabetes (P = 0.034).
Duration of diabetes did not differ significantly between those with and without LH; duration of insulin injection was numerically longer in those with LH, P = 0.069 (Table 1). Mean HbA1c was 8.0% (SD 1.7%) or 64 mmol/mol in the study population. Compared to patients without LH, those with LH had higher BMI (26.0 vs. 24.8 kg/m2), took more insulin daily (38.1 vs. 27.1 IU), more weight-adjusted insulin (by 31.7%, 0.54 vs. 0.41 IU/kg), and had 0.5% higher HbA1c (8.2% vs. 7.7% [66 vs. 61 mmol/mol]), all P ≤ 0.003. Subject BMI ranged from 18.8 to 41.4 kg/m2, with ∼31% between 18.5 and 24 kg/m2, 51% between 24 and 28 kg/m2, and 18%> 28 kg/m2. LH prevalence in these BMI subgroups is shown in Table 1; the largest proportion (49.3%) of the 213 subjects with LH had BMI between 24 and <28 kg/m2. Viewed differently, 56 of 123 (45.5%) subjects with BMI <24 kg/m2 had LH, compared to 105/205 (51.2%) with BMI between 24 and <28 kg/m2, and 52/73 (71.2%) subjects with BMI ≥28 kg/m2. There was a significant positive relationship between BMI and LH prevalence, P = 0.002. There were no significant differences between males and females for LH prevalence, duration of diabetes or of insulin injection, percent with correct site rotation, frequency of needle reuse, and insulin TDD (data not shown).
Figure 1 presents the relationship between BMI and TDD of insulin in all subjects. Pearson's r values for correlation were not significant: 0.277 for TDD and BMI and 0.247 for TDD and weight (kg). There were also no significant relationships between TDD and BMI in the subgroups with or without LH.
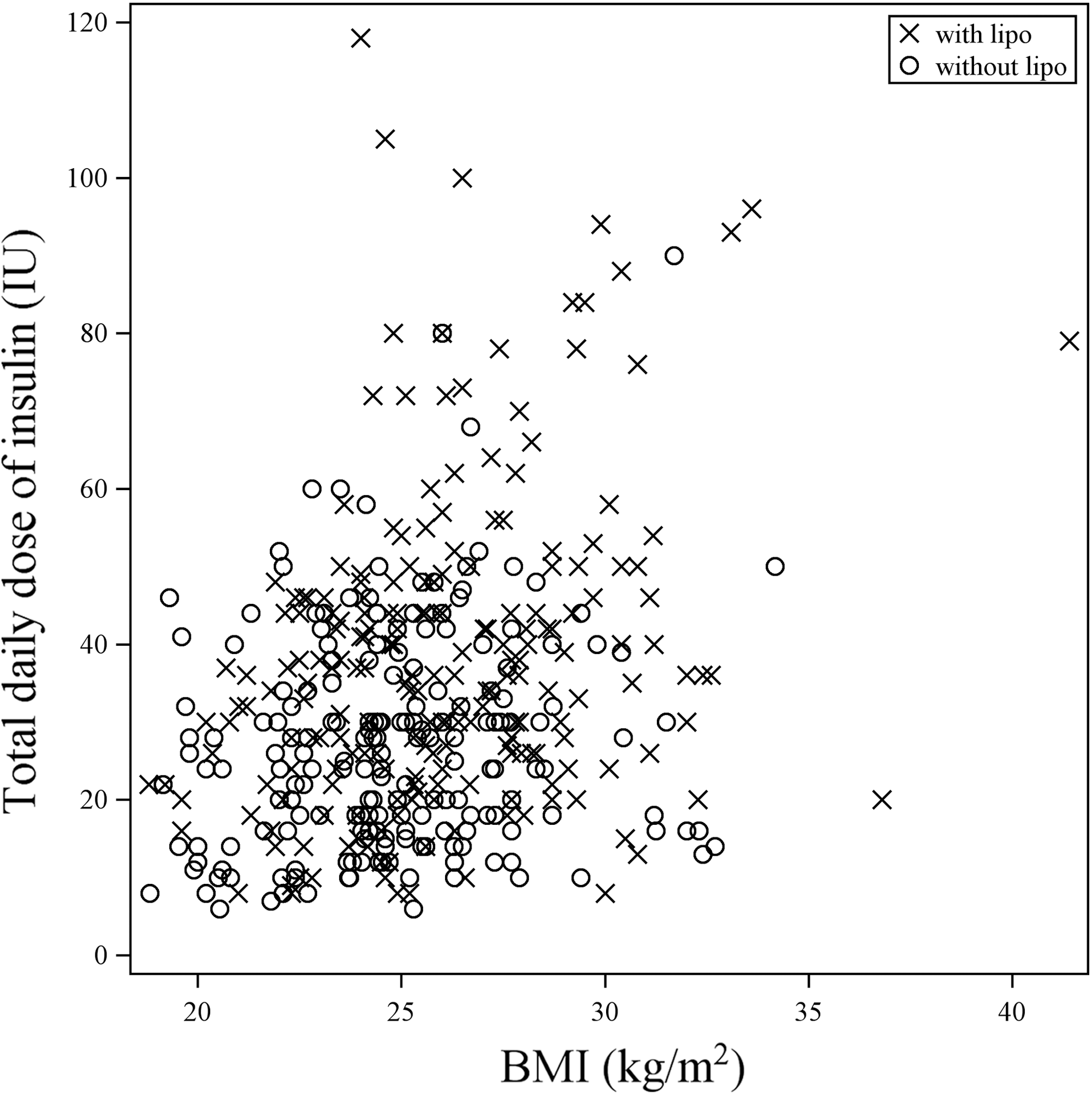
Scatter plot for body mass index (BMI) versus total daily dose (TDD) of insulin in all study subjects. R = 0.277, R 2 = 0.077. Correlations were also assessed separately between BMI and TDD of insulin in subjects with and without lipohypertrophy, with R values = 0.284 and 0.159, respectively. lipo, lipohypertrophy.
Table 2 provides information related to the insulin injection technique. Ninety percent of participants had received any injection training (∼15% within the past 12 months), and nearly 97% claimed they rotated their injection sites; correct site rotation was documented in more subjects without LH (92.3%) than in those with LH (67.6%), p < 0.0001. Needle reuse was reported by 95% of patients and did not differ between those with and without LH; however, median frequency of reuse was significantly greater in those with LH, 13 times versus 7.5 times (P = 0.003), with one subject (with LH) taking insulin twice daily reporting use of a single needle for 6 months, or 360 times. Patients with LH took >20% more injections daily, P < 0.001. Patients in the study most commonly used 5 mm needles (nearly 60%), followed by 6 mm, 8 mm, and 9.6% who used 4 mm—there were no differences between those with or without LH. In the most commonly used injection site (abdomen), patients reported using a variety of injection size areas—most commonly that of a playing card (nearly 43%). There were marginal differences in the distribution of the size of injecting areas between those with and without LH, P = 0.061. Lack of PNR was more common in those with LH, approximately 72% versus 56% in those without LH (P = 0.001), Table 2.
Data are n (percentage), or mean (SD), or median as noted.
P-value for those with lipohypertrophy versus those without.
By stepwise logistic regression, five factors demonstrated significant independent correlation with LH prevalence (Table 3). Increasing BMI, needle reuse frequency, and lack of PNR had ORs for LH prevalence between 1.1 and 1.9, P ≤ 0.03. Total weight-adjusted insulin dose and lack of correct site rotation had ORs of nearly 7.0 and 8.4, respectively, with P < 0.001 and P < 0.0001.
For stepwise logistic regression, included variables are age (years), gender, BMI (kg/m2), PN reimbursement status (Yes, No), duration of insulin therapy (years), ever received Instructions on injection (Yes, No), correct site rotation (Yes, No), number of daily injections, total daily insulin dose per weight (IU/kg), HbA1c (%), needle length (≥6 mm vs. 4 mm and 5 mm), and PN reuse (frequency ≤7 times, frequency >7 times).
P < 0.05 significant.
β, coefficient; CI, confidence interval; OR, odds ratio; PN, pen needle.
Insulin consumption-related costs
Insulin consumption-related costs were calculated as described in Methods, based on data in Table 1, and extrapolating to 9 million insulin-injecting patients in China (IMS Health Project Report, China, December 2014). On an annual basis, assuming perfect adherence to injection therapy, we estimate incremental LH-related insulin consumption in China to cost $705 million (RMB 4.7 billion). However, IMS data indicate that insulin-injecting patients in China adhere to their insulin regimen at an average rate of about 42%, or 154 insulin injection days per year (IMS Health Project Report, China, December 2014). In this case, LH-related excess insulin consumption in China is estimated at $297 million (RMB 2 billion).
Discussion
We report the first prospectively designed study of insulin injection-related LH prevalence in China and document several major clinical findings. First, the condition is common—53.1% among adults taking insulin by pen for at least 1 year. Second, several risk factors demonstrate associations with LH by stepwise logistic regression analysis, particularly weight-adjusted insulin dose and lack of correct injection site rotation. Third, patients in China with LH have clinically relevant worse glycemic control with HbA1c 0.5% higher than those without LH, despite using nearly one-third more insulin daily (IU/kg). Fourth, the additional insulin used by Chinese patients with LH is estimated to carry a substantial (and potentially avoidable) incremental cost to the healthcare system. Recent estimates of insulin sales in China totaled $1.35 billion (RMB 9 billion) in 2014 (IMS Health Project Report, China, December 2014). Our conservatively estimated $297 million (RMB 2 billion) cost of additional insulin used by Chinese patients with LH represents about 22% of the total insulin market in China.
The finding that over half of the patients examined had LH by physical examination is consistent with several other studies, 2,6 –13,15 and remarkably similar to the recent report by Blanco et al. 12 They examined 430 patients with insulin-requiring diabetes—253 type 2, and 177 type 1 diabetes, and found LH in 56% and 76% of their type 2 and type 1 diabetes patients, respectively. Hence, the apparent prevalence of LH in insulin-requiring type 2 diabetes is nearly the same in Spain and in China. In Turkey, Vardar examined 215 patients (86% type 2) and detected LH on physical examination in 48.8%, overall. 9 A recently-published study of injection technique in type 2 diabetic patients in general hospital clinics in China reported LH prevalence of 35.3%—the examiners were not specifically trained for LH detection. 23 Clearly, LH is common when it is sought systematically. However, patients report very limited frequency of inspection of their injection sites by their healthcare professionals; in a recent survey of >13,000 insulin-taking subjects in 42 countries, only 28% reported having their injection sites examined at each visit, and 39% could not remember this ever being done. 15 Modern injection technique recommendations strongly advise the inspection of insulin injection sites at least annually. 24
Besides lack of correct site rotation and daily insulin dosage, other risk factors associated with LH by logistic regression in our study include BMI, frequency of needle reuse, and lack of PN reimbursement. Blanco also found lack of proper site rotation and frequency of needle reuse—especially more than five times—to be strongly related to LH prevalence (both P ≤ 0.008). 12 Vardar and others reported comparable findings. 6,9,11 The evidence suggests that repeated local site trauma (by injection, blunted needle tips, and so on) coupled with the anabolic properties of insulin leads to adipocyte hypertrophy. LH also occurs with syringe injection and is being found more commonly in chronic insulin pump patients; 2,3,25 in some, the effects on catheter placement and insulin absorption are substantial enough to require discontinuation of infusion therapy and a return to multiple injections, due to more flexibility in injection site access—which may have implications for the performance of future closed loop artificial pancreas systems 26 (and Hirsch, Irl. Personal communication 2015).
The difference in insulin TDD in our patients was considerable—11 IU on an absolute basis for patients with LH (38.1 vs. 27.1 IU) and nearly one-third on a relative weight-adjusted basis (0.54 vs. 0.41 IU/kg). Blanco 12 found patients with type 2 diabetes, and LH used an average 21 IU more insulin daily than those without LH: 62 versus 41 IU—a similar relative difference. Although BMI was increased in those with LH in our study, the difference was modest (∼1.2 kg), and we found that BMI accounted for <10% of the variation in insulin TDD (Fig. 1)—indicating other factors are more strongly related to insulin consumption. Both higher and lower BMI has been reported as a LH-associated risk factor, 6,7 but BMI has not been linked to LH in most prior studies.
A variety of evidence indicates that insulin absorption and action are blunted and reduced from injection into LH tissue versus normal adipose layers. First, there are anecdotal case reports of marked reductions in insulin requirements and improvements in glycemic control (and variability) when patients with LH are taught to move injections to areas with normal adipose tissue. 12,19 Second, earlier studies found reduced insulin absorption for injections given in LH versus normal tissue, 16 –18,20,22 although several had methodological limitations such as older insulin assays, lack of rigorous control of prestudy glycemia, and small sample sizes. Third, two recent well-controlled crossover studies in type 1 diabetes reported marked reductions in insulin lispro pharmacokinetics (PK) and pharmacodynamics (PD) when injected into LH versus normal adipose tissue, through the first euglycemic clamps conducted to evaluate LH, and following mixed meal tolerance tests, both using a sensitive lispro-specific insulin assay. 27 Marked worsening of within-subject variability of insulin PK and PD was also documented for injections into LH tissue, consistent with clinical experience. 27
In their study, Blanco calculated estimated costs to the Spanish healthcare system of the additional insulin consumption by patients with LH—approximately 122 million Euro incremental spend, annually. 12 One limitation of their analysis, however, was the lack of reported HbA1c values. In our study, we found statistically and clinically significant increases in insulin dosing among patients with LH, as well as 0.5% higher HbA1c levels. We estimated sizeable incremental costs to the Chinese healthcare system for insulin consumption related to LH, even accounting for relatively poor injection adherence. The true healthcare costs appear to be both immediate (higher insulin consumption) and longer term (increased likelihood of microvascular complications related to worse glycemic control).
These findings have direct implications for the care of Chinese (and other) patients requiring insulin. Clinical examination of injection and infusion sites needs to become routine in diabetes clinics; healthcare professionals should be trained to evaluate patient injection sites for LH on a regular basis—at least annually. The basics of good injection technique are easily taught and should be reinforced. Injection site rotation—although claimed by >95% of our patients—needs to be reemphasized, and patients should be asked to demonstrate their rotation practices when seen in the clinics. In our study, only 68% of patients with LH demonstrated correct site rotation versus 92% of those without LH, P < 0.0001. Needle reuse as a categorical variable was not associated with LH; however, it is very common (>93% in each group). Further analysis showed that needle reuse frequency is an important risk factor associated with LH prevalence (similar to Blanco 12 )—this can be reduced, potentially, by implementing PNR policy at the city level and on a broader scale regionally. If these types of interventions can be associated with improved outcomes, the net impact should be very cost effective, if not cost saving.
Study limitations include the observational cross-sectional nature of the investigation. We can associate differences in glycemic control, insulin dosing, site rotation, and so on with the presence of LH, but cannot ascribe causality for the LH condition. However, the recent report on insulin PK-PD in patients with LH 27 provides very strong evidence that LH indeed causes reduced insulin uptake and worsens variability of insulin absorption. Prospective randomized controlled trials are needed to confirm the clinical outcome benefits of injection technique training on correct site rotation and reducing needle reuse (as well as using short PNs to increase injection site flexibility) in patients with LH, building on prior uncontrolled work. 13 We elected not to perform biopsies for histopathological examination, so the diagnosis of LH is based on physical examination, which can vary between observers. Unfortunately, there is no noninvasive “gold standard” to diagnose LH today. The number of subjects we evaluated (401) was adequate to obtain a small CI around our point estimate of LH prevalence in China, which is similar to other studies. We only studied adults at Class 3 academic center diabetes clinics; the prevalence of LH in younger patients, in pump patients, and in Class 2 centers and Community Health Centers is not known with precision and may even be greater than what we observed.
To summarize, we have demonstrated that LH is common (53.1%) in adult insulin-injecting patients in China, in Class 3 medical center clinics in four cities. It is associated with significantly worse glycemic control (HbA1c 0.5% higher), despite nearly one-third greater insulin consumption each day, compared to patients without LH. Major risk factors are weight-adjusted daily insulin dose and particularly lack of proper site rotation; lesser factors include BMI, frequency of needle reuse, and lack of PNR. The additional insulin consumed by subjects with LH, adjusted for treatment adherence, is estimated to cost $297 million (RMB 2 billion) annually; estimates in other countries can be easily developed. LH should be largely preventable and treatable by basic injection technique training to reinforce proper site rotation and reduction in needle reuse. Healthcare professionals should inspect patients' injection (and infusion) sites routinely and provide education on proper injection technique.
Footnotes
Acknowledgments
This study was funded by BD (Becton, Dickinson & Co., Inc.), a manufacturer of insulin syringes and PNs.
The authors thank Dan Wang, Pingpin Jin, and Luan Luan for their assistance in study coordination and site monitoring. The authors also thank all of the patients and clinic staff for their participation in the study.
Parts of this study were presented in abstract form at the 75th Scientific Sessions of the American Diabetes Association, Boston, MA, June 5–9, 2015, and at the 51st Annual Meeting of the European Association for the Study of Diabetes, Stockholm, Sweden, September 14–19, 2015.
Authors' Contributions
L.J., Z.S., and the BD coauthors were responsible for the study design, protocol, and statistical analysis plans. Data analysis was primarily performed by J.L. and reviewed by all coauthors. Final responsibility for the decision to submit the article for publication was made jointly by all authors.
L.J., Z.S., Q.L., and G.Q. researched the data. L.J.H. wrote the first draft of the article, which was reviewed and edited by all other coauthors for substantive content, in particular L.J. and Z.W. J.L. performed data analyses and responded to suggestions from other authors. All authors have reviewed the final manuscript and approved the decision to submit for publication. L.J. and L.J.H. are the guarantors of this work and, as such, have had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
L.J., Z.S., Q.L., and G.Q. received compensation from BD as study investigators. L.J. and Z.S. received honoraria as lecture fees from BD, in part, to present study posters at scientific meetings. Z.W., J.L., A.B.C., and L.J.H. are employees of BD. No other potential dualities of interest relevant to this article were reported.