
Abstract

Introduction
T
In this commentary, we expand the topic of the importance of meal detection to closed-loop control by presenting an in silico study using our metabolic simulation environment 2 to link the frequency of missed meal boluses to average glycemic control (e.g., estimated HbA1c) achieved during simulated 30-day scenarios. To avoid the influence on outcomes of any particular closed-loop control algorithm, we keep the simulated scenarios “simple” and limited to meal bolusing based on self-monitoring of blood glucose (SMBG) using glucose meters with error characteristics simulating real devices. In effect, this is a simulation of an aspect of self-treatment behavior (e.g., missed meal boluses), the detrimental effects of which can be mitigated by automated meal detection. Thus, the meal-detection and false-alarm rates of an algorithm, such as that presented by Weimer et al., 1 could be used to filter further our simulation data and to gauge the contribution of meal detection on outcomes, such as glycemic control. To perform such an in silico study, however, requires the implementation of a specific meal detector and a specific closed-loop control algorithm, which would be a subject of a subsequent investigation.
Challenges to Artificial Pancreas Systems
Patients with type 1 diabetes face the complex optimization problem to maintain strict glycemic control without increasing their risk of hypoglycemia. Recent technological advances have improved the ability of patients to achieve these goals. In particular, clinical trials of closed-loop glucose control technology have shown that it is possible to reduce levels of hyperglycemia (and thereby HbA1c), while at the same time reducing the risk of hypoglycemia. 3 –7 Despite the progress that has been made in the entire range of diabetes treatment technologies, including insulin pump therapy [Continuous Subcutaneous Insulin Infusion (CSII)], continuous glucose monitoring (CGM), and the artificial pancreas (AP), there are significant challenges still ahead. 7 In particular, many AP systems require significant patient involvement, for instance, the announcement of every meal. 8 Research projects are currently focusing on incorporating other physiological inputs to improve glycemic control and reduce the cognitive burden to the patient. For example, it is well known that exercise remains a significant challenge to AP systems, 9 and recent studies show that heart rate can be used to improve the effectiveness of closed-loop control. 10 Meal detection is another important signal that, if accurate, will contribute to the improvement of automated insulin delivery and to mitigating behavioral challenges, such as missed meal boluses.
Behavioral Aspects of Type 1 Diabetes
Until fully automated unobtrusive closed-loop control becomes widely available, type 1 diabetes will remain a largely behaviorally controlled condition. Patients with type 1 diabetes spend an average of 3 h a day managing their disease. In addition to counting carbs to correctly bolus each meal, there are many significant behavioral events that trigger perturbations of the metabolic system and thereby challenge its optimal control. These events are normal in daily life and include, but are not limited to, frequency and extent of meals and exercise, level of perception of, and self-treatment response to, symptoms of hypoglycemia, 11 –13 and response to stress. 14 Thus, moving toward personalized diabetes therapies and adaptive AP systems will require better understanding of self-treatment behaviors and their variability. Quantitative understanding and in silico reproducing of patient behavior will ultimately play a critical role in improving and personalizing the performance of closed-loop systems. Initial work in this direction has already shown some potential. For example, learning the nature and likelihood of certain typical behaviors and exploiting this information can result in a more adaptive closed-loop system that both improves glycemic control and reduces the cognitive burden of the patient. 15 In another instance, a clinical study showed that a control-to-range AP system can improve clinical outcomes by feed-forward signaling of heart rate as a proxy for physical activity intensity. 10
Meal Detection, Meal Boluses, and Glucose Control
To illustrate the importance of meal detection and appropriate subsequent action (e.g., appropriate meal bolus), we conducted a 30 day in silico experiment. These simulations were designed to highlight the relationship between patient behavior and effectiveness of a control scheme. More specifically, we used the UVA/Padova Type 1 diabetes simulator 2 to observe virtual “patients” undergoing intensive CSII therapy for 30 days. During this month, these patients skipped meal boluses with a certain probability, and based their dosing decisions on SMBG information. A virtual glucose meter was chosen from a set of 43 glucose meters and had error characteristics matching those of commercial meters reported in the literature. 16 A set of eight simulation replicates was conducted for each combination of glucose meter and probability of skipping a meal bolus, the latter varied from 0% to 100%. The rest of the patient behavior (meal amounts, times, etc.) was based on data collected by an observational study involving 55 patients with type 1 adults, who were followed over a month, documenting their meals and bolusing patterns. 17 As seen in Figure 1, average glycemic levels, expressed here as estimated HbA1c, increase with increasing frequency of skipped meal boluses.
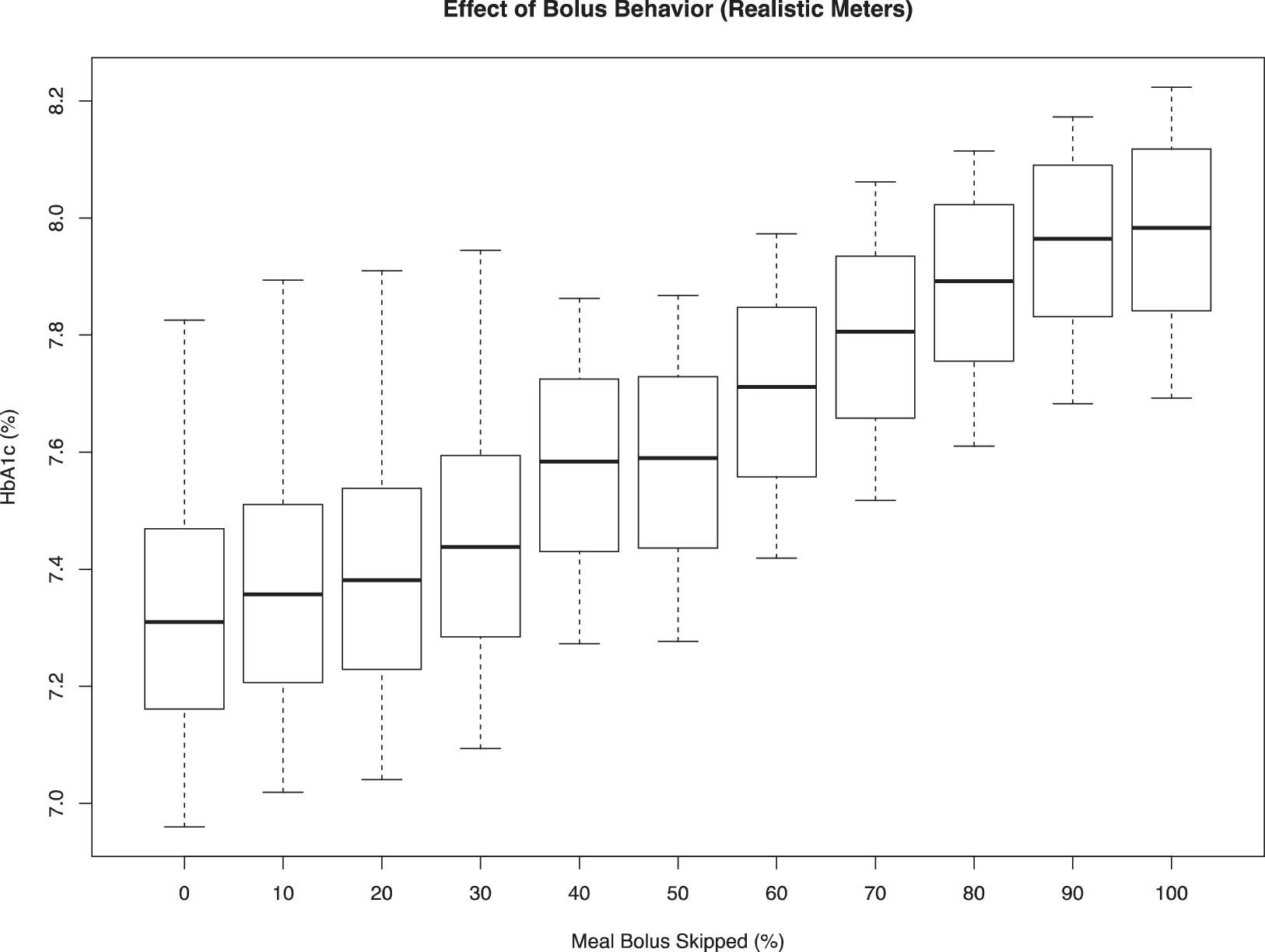
Response of average HbA1c observed by the population as a function of a behavioral parameter: percentage of meal bolus skipped. Each bar presents A1c levels obtained using 43 realistic (commercially available) meters. 16
Conclusions
The results of this in silico study highlight the interplay between one aspect of patient behavior, for example, the timing and accuracy of meal boluses, and glycemic control. The gradual deterioration of glycemic outcomes with poorly executed meal boluses suggests that improvement in meal detection technology, and thereby improvement in meal bolusing, would lead to better management of type 1 diabetes. This is particularly relevant in the context of AP systems, which can automatically mitigate the effects of skipped premeal boluses, provided that meals are accurately and timely detected. Thus, the work presented by Weimer et al. 1 is an important step toward improvement of closed-loop control, and is particularly relevant to the quest for a fully automated AP. Automated meal detection could be also used to assist patient behavior in the context of available CGM signal. Overall, accurate detection of meals and other metabolically important patient behaviors, such as physical activity, will play a significant role in improving all aspects of the technology-based treatment of diabetes, ranging from decision-support/advisory systems to fully automated closed-loop control.
Footnotes
Acknowledgments
The writing of this commentary and the database used were supported by grant R01 DK 085623 from the National Institute of Diabetes and Digestive Diseases and the Kidney, National Institutes of Health. The JDRF Artificial Pancreas Project at the University of Virginia supported the building of our computer simulation environment and currently supports the building of a behavioral simulator.
Author Disclosure Statement
E.C.N. served as an advisor to The Epsilon Group and has received research support from Insulet, Roche Diagnostics, Ascensia Diabetes Care, and the Juvenile Diabetes Research Foundation (JDRF). B.P.K. served as an advisor to Becton Dickinson and Company and Sanofi-Aventis, has received research support from BD, Dexcom, Roche Diagnostics, Sanofi-Aventis, and Tandem Diabetes Care, and is a shareholder in InSpark Technologies and TypeZero Technologies.