
Abstract
Background:
We update the psychometric properties of the Hypoglycemia Fear Survey-Parents of Young Children (HFS-PYC), a 26-item measure of parents' hypoglycemia fear for young children using an insulin pump.
Methods:
We combined three similar datasets for the analyses. The data analyzed included parents' responses to the HFS-PYC and a demographic form. For a subset of children (n = 91), we also analyzed self-monitoring of blood glucose data. We used confirmatory factor analysis (CFA) to confirm the measure's original factor structure. Additional analyses examined reliability and validity of a revised HFS-PYC for parents of young children using pumps.
Results:
We analyzed data from 116 parents (93% mothers). Mean child age and HbA1c were 5.2 ± 1.3 years and 8.2% ± 1.1%, respectively. CFA identified a 22-item two-factor solution (χ2 (208, n = 116) = 368.688, P < 0.001, root mean square error of approximation = 0.08, comparative fit index = 0.94, and Tucker-Lewis index = 0.93) with factors corresponding to the original subscales: worry and behavior. The revised subscales demonstrated at least adequate internal consistency (Cronbach's alpha >0.65). Correlations revealed significant negative associations between current HFS-PYC worry scores and children's mean daily blood glucose and percent of very high glucose levels per day, suggesting less fear among parents of young children with elevated glycemic levels. In addition, there was a positive association with the percent of glucose levels in target, suggesting greater hypoglycemia fear among parents of children who have better control.
Conclusions:
Results provide preliminary evidence for the reliability and validity of a reduced 22-item HFS-PYC for parents of children using insulin pumps.
Introduction
H
FH is a term used to describe severe anxiety-like symptoms related to glucose management as well as the use of hypoglycemic avoidance behaviors. 5,7 –9 Past research suggests that FH is reported by up to 60% of parents of young children based on self-report using the Hypoglycemia Fear Survey-Parents of Young Children (HFS-PYC). 8,9
The HFS-PYC is a reliable and valid measure of FH adapted from an existing adult questionnaire, the Hypoglycemia Fear Survey. 9,10 In the development phase of the HFS-PYC, a five-member panel of diabetes care providers (e.g., one physician, one nurse educator, one dietitian educator, and two psychologists) reviewed potential items to ensure good content validity. Then, a preliminary form of the HFS-PYC was administered to a sample of parents of young children with T1D to determine its initial psychometrics. 9
However, one challenge to ongoing use of the HFS-PYC is that it was originally tested in a sample of children who were 70% conventionally managed for insulin because that was still a primary insulin regimen at the time. Now, data from the T1D Exchange suggest that ∼69% of young children use an insulin pump for daily management, 11 but an updated evaluation of psychometric properties of the HFS-PYC in a sample of parents of children using a pump has not been published. Thus, the purpose of this study was to use confirmatory factor analysis (CFA) to confirm the psychometrics of the HFS-PYC in a sample of parents with children who use an insulin pump for their daily treatment.
Methods
Data were compiled from three projects, completed over 5 years, which recruited young children with T1D and a parent. For all three projects, the inclusion/exclusion criteria were similar. Families were eligible if they had a child with T1D who was between the ages of 1–7 years, their child had T1D for at least 6 months before study enrollment, their child used an insulin pump for daily management, and the family spoke English. Families were ineligible to participate in any of the three projects if their child had some other form of diabetes, their child had a chronic condition in addition to T1D that might further complicate their child's medical management (e.g., kidney disease), or if their child was taking any medications that could disrupt glycemic control (e.g., systemic steroids).
Before combining the samples, we compared the studies and found no differences in their demographics or parents' hypoglycemia fear scores, suggesting that it was acceptable to proceed with the new larger data set. It was necessary to have this larger data set to proceed with a CFA of the HFS-PYC. 12
Procedure
For all three projects, we obtained appropriate institutional review board approval from each of the participating hospitals ahead of subject enrollment.
To enroll eligible families, a member of the research team contacted families by telephone or in person during routine diabetes clinic visits. During enrollment, we explained each study, answered questions, and completed the informed consent. Families then completed a series of questionnaires, which included a demographic form and the HFS-PYC. 8,9 In all cases, we obtained a measure of the child's most recent glycated hemoglobin (HbA1c) from his/her medical chart. In a subset of children (n = 91), we also collected at least 14 days of self-monitoring blood glucose data from children's glucometers to calculate measures of glycemic variability. Parents who participated were reimbursed between $25 and $50, depending on each study's protocol.
Measures
Hypoglycemia fear survey-parents of young children 9
This is a 26-item questionnaire that was modified from the Hypoglycemia Fear Survey-Parent (HFS-P) 7 to make it more appropriate for use with parents of children with T1D who are less than 8 years old. Similar to the HFS-P, the HFS-PYC was developed to yield two subscales, the worry subscale, which assesses parents' fear and worry related to the occurrence of a low blood glucose event for their child, and the behavior subscale, which measures parents' behaviors related to preventing a low blood glucose event. For each item, parents respond using a five-point Likert scale (1 = never, 5 = very often). Subscale scores are then obtained by tallying the items corresponding to either the worry (16 items expected) or behavior (10 items expected) subscales.
Demographic and medical history form
Parents reported on demographic characteristics of their child (e.g., age, sex, time since diagnosis) and themselves (e.g., relationship with their child and marital status), and provided the necessary information to estimate the families' socioeconomic level (e.g., parents' education and employment).
Analysis
We conducted our CFA using Mplus Version 7.31. 13 Before conducting our CFAs, we screened the data for outliers and violations of normality and one item (item #8 Always carry fast-acting sugar) fell beyond the recommended guidelines for skewness (−3.713) and kurtosis (14.195), suggesting that this item may not differentiate among individuals in this population and therefore was omitted from all subsequent analyses.
We then specified a two-factor measurement model based on the original factor structure of the HFS, 10 allowing latent factors to correlate freely. Because the items used a five-point Likert scale, we modeled all items as ordinal data using the weighted least-squares mean and variance-adjusted estimation. 14,15 We examined multiple fit indices to evaluate model fit: chi-square (χ2), the comparative fit index (CFI), the Tucker-Lewis index (TLI), and the root mean square error of approximation (RMSEA). CFI and TLI values range from 0 to 1; values >0.90 indicate an acceptable model fit and values >0.95 indicate a good model fit. 16,17 The RMSEA represents population error variance, with values between 0.08 and 0.05 indicative of an acceptable model fit and values <0.05 indicative of good fit. 17,18
We used SPSS Version 22 19 to examine internal consistency of the final model subscales and full scale, associations between HFS-PYC subscales and daily average blood glucose, and comparisons with published research.
Results
Participants
There were 116 child–parent dyads in our sample (93% mothers). The sample of children had a mean age of 5.2 ± 1.3 years (range, 2.0–7.9). Fifty percent of the children were male, 91% were described by their parent as non-Hispanic white, and all children used an insulin pump for daily diabetes care. At the time of data collection, the HbA1c target in children <6 years old was between 7.5% and 8.5% and it was ≤8% in children 6–12 years old. 1 The HbA1c values for the present sample of children ranged from 5.70% to 12.70% (M = 8.2% ± 1.1%; 40.5% of HbA1c values were in the recommended range).
Confirmatory factor analysis
The initial CFA model, using 25 items of the original HFS-PYC, demonstrated an acceptable fit to the data, χ2 (274, n = 116) = 423.292, P < 0.001, RMSEA = 0.07, CFI = 0.94, and TLI = 0.94. However, standardized factor loadings for three items fell below 0.30: items 2 (“Avoid allowing my child to be away from me/in someone else's care when his/her sugar is likely to be low,” standardized loading = 0.07, P = 0.59), 5 (“Feed my child as soon as I feel or see the first signs of a low blood sugar,” standardized loading = 0.22, P = 0.02), and 9 (“Keep my child quiet if I think his/her blood sugar could go low (i.e., avoid hard play or activity),” standardized loading = 0.16, P = 0.15). Thus, we removed these items and conducted a subsequent CFA. Results of this CFA revealed an acceptable fit for the 22-item two-factor model: χ2 (208, n = 116) = 368.688, P < 0.001, RMSEA = 0.08, CFI = 0.94, and TLI = 0.93 and standardized factor loadings ranged between 0.32 and 0.83. The factor loadings for the final two-factor model are presented in Figure 1.
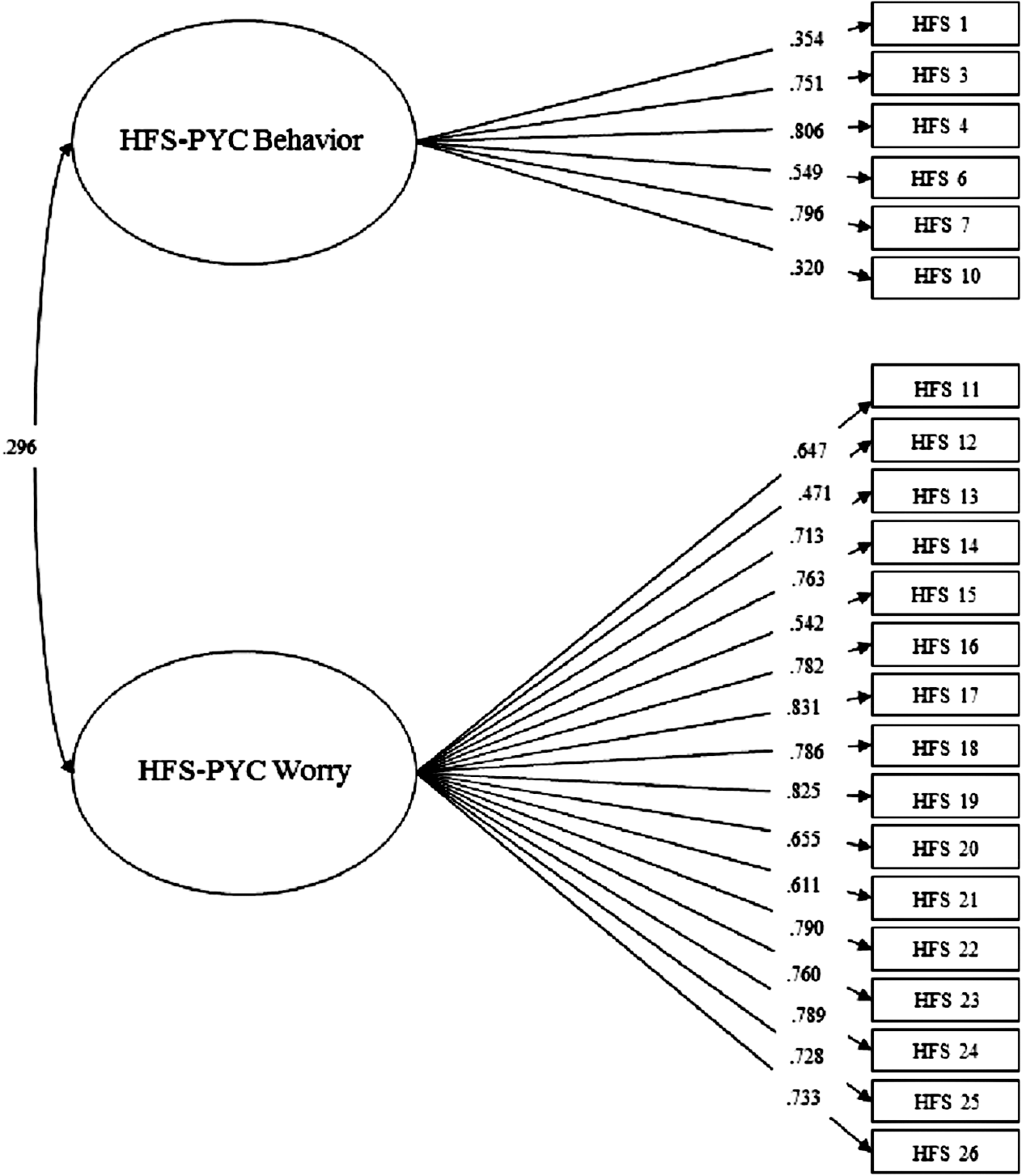
The confirmatory factor analysis results for the Hypoglycemia Fear Survey-Parents of Young Children (HFS-PYC) in parents of young children who are using an insulin pump. All standardized path coefficients are significant at P < 0.01.
Reliability and validity
With items 2, 5, 8, and 9 removed based on the CFA results, we examined the reliability and validity of an updated HFS-PYC. The updated HFS-PYC worry subscale (α = 0.92) demonstrated excellent internal consistency, whereas the HFS-PYC behavior subscale demonstrated an internal consistency in the lower acceptable range (α = 0.68). Correlations between the HFS-PYC factors indicated that they are related, but distinct, constructs (Fig. 1). The HFS-PYC worry subscale negatively correlated with children's average daily blood glucose (r = −0.267, P = 0.01) and the percent of very high glucose levels (>250 mg/dL; r = −0.227, P = 0.03). However, the HFS-PYC worry subscale positively correlated with the percent of glucose levels between 70 and 180 mg/dL (r = 0.274, P = 0.008), suggesting greater FH in parents of children who are in better glycemic control. There were no correlations between the updated six-item HFS-PYC behavior subscale and children's glucose levels.
HFS score comparisons with published outcomes
Calculating subscale scores using the reduced 22-item HFS-PYC, parents in the present sample reported a mean worry score of 45.2 ± 14.2 and a mean behavior score of 17.2 ± 4.1. However, to allow for comparisons with published scores, 7 –10 we adjusted for the number of subscale items by calculating a mean item score for each subscale, yielding a mean item score of 2.8 ± 0.88 for the worry subscale and a mean item score of 2.9 ± 0.69 for the behavior subscale.
Using the mean item scores and a series of one-sample t-tests with unequal variances, results showed significantly higher worry scores for parents in the present sample when compared with mothers of conventionally managed young children 9 and adult patients with T1D (P's ≤ 0.01). 10 There was also a trend found suggesting higher worry scores for parents in the present sample when compared with published data from mothers of preadolescent youth (P = 0.07). 7 For the behavior score, parents in the present sample reported higher mean item scores than did adult patients (P ≤ 0.001), but lower mean item scores than mothers of conventionally managed young children and mothers of preadolescent youth (P ≤ 0.001).
Discussion
The HFS-PYC is the only available measure of FH for parents of young children. However, until now, there were no data available establishing its measurement properties in a sample of parents of young children using an insulin pump.
Study findings indicated that for this parent population, a two-factor structure corresponding to parents' behaviors and worries surrounding hypoglycemia best captures FH. These results also suggest that four original items from the behavior subscale may not contribute to the measurement of parental FH in young children on pump therapy. For instance, one item (i.e., item #8) demonstrated significant negative skew, suggesting that this item may not differentiate elevated FH from more typical levels in parents of young children using pump therapy. Furthermore, insufficient factor loadings for items 2, 5, and 9 indicate that these items may not provide meaningful information for the measures of FH in the current population. Interestingly, in a recent study with parents and adolescents with T1D, researchers identified a two-factor structure within the HFS behavior subscale corresponding to potentially adaptive (e.g., “Avoid being alone when blood glucose could drop”) versus maladaptive (e.g., “Try to run blood sugars a little high to be safe”) behaviors. 20 Although we did not directly test for these subfactors in our analyses, items 2, 5, and 9 do reflect potentially adaptive behaviors to prevent low blood glucose, which may explain why they did not load on a factor that also included potentially maladaptive behaviors. Thus, as a future study, it may be important to confirm if a two-subfactor structure exists for the HFS-PYC behavior scale in a larger sample of parents.
Overall, for the present sample, the HFS-PYC demonstrated good internal consistency. The HFS-PYC behavior subscale had the lowest internal consistency, which could be attributed to a limited number of items (i.e., 6 vs. 16 items). However, it is notable that previous studies using the 10-item version of this subscale report comparable internal consistency values (e.g., 0.62 and 0.70). 8,9 Furthermore, studies using the HFS and HFS-P also report lower internal consistency for the behavior subscale. 7,10 Thus, it is also possible that this subscale is not as sensitive to behaviors indicative of FH because it combines both adaptive and maladaptive behaviors to prevent low blood glucose. 20
As a measure of validity, we correlated our modified HFS-PYC questionnaire with children self-monitoring blood glucose levels. While previous research has been inconsistent regarding the association between parents' FH and children's glycemic control, 5,8,9 our findings revealed that the HFS-PYC worry subscale was negatively associated with children's average daily blood glucose and the percent of very high glucose levels and positively associated with the percent of blood glucose levels in the target range. It is possible we were able to measure these associations, while past research was not, because we employed a very specific definition of target blood glucose according to Bergenstal et al.'s 21 recommendations for standardizing glucose reporting. However, it is also possible parents of children with higher blood glucose reported less worry because they purposely allowed their child to run above target as a way to reduce the chance of low blood glucose and their fear of a low, suggesting that a more complicated association between parents' FH and children's glycemic control may exist. Because these were correlations, cause and effect cannot be determined. Therefore, one recommendation for the future would be a longitudinal study to see if a temporal relationship between parents' FH and children's glycemic levels could potentially unravel the nature of this association.
A comparison of parents' scores on the HFS-PYC behavior and worry subscales with published scores yielded mixed results. Higher worry scores for current study parents when compared with parents of preadolescent youth 22 and adult patients with T1D 22 may be explained by young children's difficulties with reporting symptoms of hypoglycemia due to cognitive and communication immaturity as well as their greater susceptibility to glycemic variability. 1 In contrast, parents in the present study may have reported higher worry scores than mothers of conventionally managed young children 22 because the pump may prevent their child from experiencing as much glycemic variability as conventionally managed children do, leading to parents of children on pumps having less experience and lower confidence in managing hypoglycemia successfully and higher fear. 23,24 Interestingly, consistent with previous research using the HFS-P, 25 we found that parents of young children on pumps reported lower mean scores on the HFS-PYC behavior subscale compared with parents of conventionally managed young children. 22 One possible explanation for this finding is the increased flexibility of pump therapy, which allows parents to make insulin adjustment more easily and to reduce reliance on behaviors that may overcompensate for hypoglycemia, such as feeding large snacks. 26 –28
Limitations and future directions
Limitations of our study include the homogeneity of our sample and our cross-sectional design. Because the majority of the study sample included families of young children who self-identified as non-Hispanic white, the study results may not generalize to parents from other racial or ethnic backgrounds. However, because the study sample has a racial/ethnic diversity similar to that of the US population of youth with T1D, 29 we expect our modified HFS-PYC will be applicable to the majority of parents of young children with T1D and future research can investigate its psychometric properties in a more racially or ethnically diverse sample. Since we were limited to cross-sectional data, we cannot assess test-retest reliability of our modified HFS-PYC, nor examine the temporal association between parents' HFS-PYC scores and children's glycemic levels. However, both of these questions can be addressed in a future longitudinal study as well as measuring for other forms of validity such as convergent and divergent validity.
Conclusion
This study provides support for use of a modified version of the HFS-PYC in parents of young children on insulin pump therapy. Our results show that the original two-factor structure of the HFS-PYC fits the data well, with the removal of four items from the behavior subscale. Therefore, we recommend that researchers and clinicians who use the HFS-PYC in parents of young children on insulin pumps consider removing these items when calculating the behavior subscale and total score. Additionally, we encourage researchers to conduct further assessment of the validity of the HFS-PYC to better establish its psychometric properties.
Footnotes
Acknowledgments
This research was supported, in part, by grants K23-DK076921 and R03-DK090288 (to S.R.P.) from the National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases and grant R21-HD081502 (to S.R.P.) from the National Institutes of Health/Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors would like to thank the families who gave of their time to participate in the projects included in this study.
Author Disclosure Statement
No competing financial interests exist.