
Abstract
Background:
We aimed to compare glycemic control, insulin requirements, and outcomes in women with type 1 diabetes in pregnancy treated with continuous subcutaneous insulin infusion (CSII) and multiple daily injections (MDI).
Methods:
A retrospective cohort study was conducted of singleton pregnancies (>20 weeks gestation) in women with type 1 diabetes (2010–2015) at a specialist multidisciplinary maternity network in Australia. Antenatal characteristics, diabetes history and treatment details, and maternal and neonatal outcomes were compared for women with type 1 diabetes using CSII and MDI. Bolus calculator settings were reviewed for CSII. Data were obtained from individual medical records, linkage to pathology, and the Birthing Outcomes System database.
Results:
There were no differences in maternal characteristics or diabetes history between women managed with CSII (n = 40) and MDI (n = 127). Women treated with CSII required less insulin and less increase in total daily insulin dose/kg than MDI (40% vs. 52%). Both groups achieved similar glycemic control and no differences in pregnancy outcome. In the CSII group, carbohydrate:insulin ratios were intensified across gestation (30% breakfast, 27% lunch, 22% dinner), and insulin sensitivity factors (ISFs) changed little (7% breakfast, 0% lunch, −10% dinner).
Conclusions:
There was no difference in glycemic control or pregnancy outcomes in women using CSII or MDI managed in a multidisciplinary setting. Greater adjustments are needed to ISFs with CSII therapy. Overall, these data do not support recommending CSII in pregnancy with potentially higher patient and staff demands and costs and lack of improvement in HbA1c and pregnancy outcomes.
Introduction
T
Outside pregnancy, CSII may lower glycated hemoglobin (HbA1c) to a greater extent than multiple daily insulin injections (MDI), reduce severe hypoglycemic events, and improve quality of life in selected patients. 4 However, studies comparing CSII and MDI in pregnancy have had mixed results. Small studies have shown an increase in maternal weight, 5 diabetic ketoacidosis, 6 neonatal hypoglycaemia, 6 and birth weight with CSII therapy. 7 Others have suggested that CSII can improve HbA1c over MDI, 8 –11 in particular for women with complicated diabetes, 12 and may reduce maternal hypoglycemia. 10 Despite this, a Cochrane review of five single centre randomized trials in pregnancy (total n = 154 pregnancies) found little evidence to support one form of insulin administration over another. 7 A systematic review of seven cohort studies (total n = 777 with 14–86 women per group) reported similar improvements in HbA1c and no difference in pregnancy outcomes. 13 Notably, studies were biased with incomplete descriptions of methodology and outcomes. 13 These studies are frequently small, and CSII and MDI groups differ with regard to diabetes duration, complications, and baseline glycemic control. 11,12,14 Some studies include women who commenced CSII in pregnancy, 10 often due to failure to obtain adequate control with MDI, 14 and thus are not representative of the true effects of CSII therapy.
Few studies have evaluated changes in insulin requirement, carbohydrate ratios, and sensitivity across gestation in women using CSII. 15,16 Further insights would be valuable in counseling pregnant women and guiding clinicians in anticipating changes to insulin regimens to optimize control and minimize glucose fluctuations.
In women with type 1 diabetes managed with CSII compared with MDI in a quaternary universal healthcare system in a public hospital setting, we aimed to capture the model of care, diabetes history, insulin regimen, glycemic control, and diabetes complications. We also aimed to compare maternal and neonatal outcomes across the two groups. In women treated with CSII, we explored changes in insulin doses, carbohydrate ratios, and insulin sensitivity from preconception to delivery.
Methods
Study design and population
A retrospective cohort study was conducted of all singleton pregnancies with births >20 weeks gestation in women with preexisting type 1 diabetes (n = 167) at Monash Health from January 2010 to December 2015. Monash Health is one of the largest public health services in Australia, providing care for nearly 9500 births per year and encompassing Monash Diabetes, one of four recognized National Centers of Diabetes Excellence. The study was approved by the Monash Health Human Research Ethics Committee (Approval no. 14001Q).
Model of care
Data were captured on visits across reproductive stages from preconception to postpartum and on disciplines involved in care.
Diabetes, insulin regimen, and complications
Diabetes history and treatment details were obtained from individual medical records. Insulin type and doses (total daily dose [TDD], and U/kg) were recorded preconception and for each trimester. Data linkage to Monash Health pathology was used to incorporate glycated hemoglobin levels (HbA1c% or mmol/mol), measured by the Arkray Adams High Performance Liquid Chromatography Method (HA-8160, coefficient of variation 1.4%, Kyoto, Japan).
Maternal and neonatal outcomes
Maternal and neonatal outcome data were extracted from the Birthing Outcomes System (BOS) database, which includes standardized health information used for statutory data entry and reporting. Data are collated by midwives and include maternal demographics, medical and family history, obstetric history, antenatal care, labor complications, neonatal treatments, and complications.
Maternal outcomes examined were induction of labor, caesarean section, preterm birth (<37 weeks gestation), gestational hypertension (new onset hypertension from 20 weeks with blood pressure ≥140/90 mmHg), and preeclampsia (hypertension with proteinuria >300 mg/24 h or spot urine protein: creatinine ratio ≥0.03 g/mmol and/or renal, liver, neurological, or hematological system involvement). Neonatal outcomes examined included gestation at birth, birth weight, large for gestational age and small for gestational age (birth weight >90th centile and <10th centile adjusted for gestational age and sex), 17 neonatal intensive care unit admission (for potentially life-threatening conditions), neonatal hypoglycemia (blood glucose <2.6 mmol/L requiring 10% dextrose), jaundice (requiring phototherapy), apgar score <7 at 5 min, respiratory distress syndrome, shoulder dystocia, congenital malformations (major and minor), and perinatal death (stillbirth and neonatal death up to 28 days).
Insulin regimens in the subgroup of women treated with CSII
For women treated with CSII, electronic pump downloads and medical records were reviewed to obtain carbohydrate ratios and insulin sensitivity factors (ISFs).
Statistical analyses
Antenatal characteristics and maternal and neonatal outcomes were compared for women with type 1 diabetes using CSII and MDI. Categorical data were compared using Pearson chi-square or Fisher's exact tests. For continuous data, Student's t-tests or Mann–Whitney U tests were used as appropriate. A two-sided P-value of 0.05 was considered statistically significant. Analyses were performed using Stata version 12 (StataCorp, TX).
Results
Maternal demographics
Forty pregnancies (n = 37 women) were managed with CSII and 127 (n = 102 women) were managed with MDI. There was no significant difference in maternal age, BMI, parity, or smoking status between groups. There was a higher proportion of women born in Europe and America (P = 0.02) and fewer born in Australia (P < 0.01) in the CSII group (Table 1).
Student's t-test or Mann–Whitney U tests for continuous variables and chi-squared tests for categorical variables.
CSII, continuous subcutaneous insulin infusion; IQR, interquartile range; N/A, not applicable.
Model of care
The Monash Health diabetes in pregnancy service provides specialized endocrine, diabetes nurse educator, obstetric, midwifery, and neonatal services. Sixty percent of women in both groups attended preconception care. Women were initially managed in a preconception and early pregnancy clinic, then in a specialized multidisciplinary diabetes and maternity service from 12 weeks gestation. They were reviewed every 4 weeks until the third trimester, fortnightly, then weekly from 34–36 weeks gestation. Women on CSII downloaded their pumps fortnightly (or more frequently if required), then weekly after 34–36 weeks, and results were read either in clinic or over email by their educator and/or treating doctor as necessary. Following delivery, newborns of women with type 1 diabetes were routinely admitted to the special care nursery for observation. Women were reviewed on a daily basis by the endocrine team as inpatients, postdischarge at 1 week, and were then returned to their usual model of care. There were a similar number of visits in both groups, however, the relative proportion of time allocated to and spent by the medical team and diabetes nurse was reported to be higher in women using CSII.
Diabetes, insulin regimen, and complications
There was no difference in duration of diabetes between groups. All women on CSII therapy had been using this method for a median of 2 years (range 0.5–8 years), except one woman who commenced CSII in the second trimester. All women on CSII were using insulin aspart. Women on MDI therapy used glargine (50.5%), detemir (37.8%), or NPH (11.7%) as basal insulin. All bolus insulin was with rapid acting analogs (aspart 71.4%, lispro 25.9%, glulisine 0.9%) except for one woman who used regular insulin (0.9%).
TDD of insulin was significantly lower in the CSII compared with MDI group prepregnancy and in every trimester. TDD of insulin (U/kg) increased by 40% from the first to third trimester in the CSII group and 52% in the MDI group. There was no difference in proportion of basal and bolus insulin used between groups. Women treated with CSII had similar glycemic control to MDI in each trimester and throughout the pregnancy (median HbA1c 7.2% [55 mmol/mol] vs. 6.9% [52 mmol/mol], P = 0.51). There was no difference in microvascular complications, maternal rates of severe hypoglycemia, or diabetic ketoacidosis (Table 1).
Maternal and neonatal outcomes
There was no significant difference in gestational age at birth, neonatal sex, birth weight, or maternal or neonatal outcomes between groups (Table 2).
Chi-squared tests for categorical variables.
Congenital malformations: MDI (heart murmur, Cystic Fibrosis with Meckel's diverticulum, Tetralogy of Fallot, ectopic anus, Ventricular Septal Defect), CSII (Malposition of great vessels).
Perinatal deaths: MDI (three terminations, two intrauterine deaths at 34 and 37 weeks, 1 neonatal death extreme premature lung disease), CSII (one termination).
MDI, multiple daily injections.
Insulin regimens in the subgroup of women treated with CSII
There was intensification of carbohydrate-to-insulin ratios at breakfast, lunch, and dinner times from prepregnancy until the first trimester. Subsequently, ratios were lowered by 30% at breakfast, 27% at lunch, and 22% at dinner from the first to third trimesters. There was a small increase in the ISF from prepregnancy to the first trimester at lunch only. Changes in the ISF were made across the pregnancy from the first to third trimester: 7% increase in sensitivity at breakfast, 0% change at lunch, and 10% decrease in sensitivity at dinner (Table 3, Fig. 1).
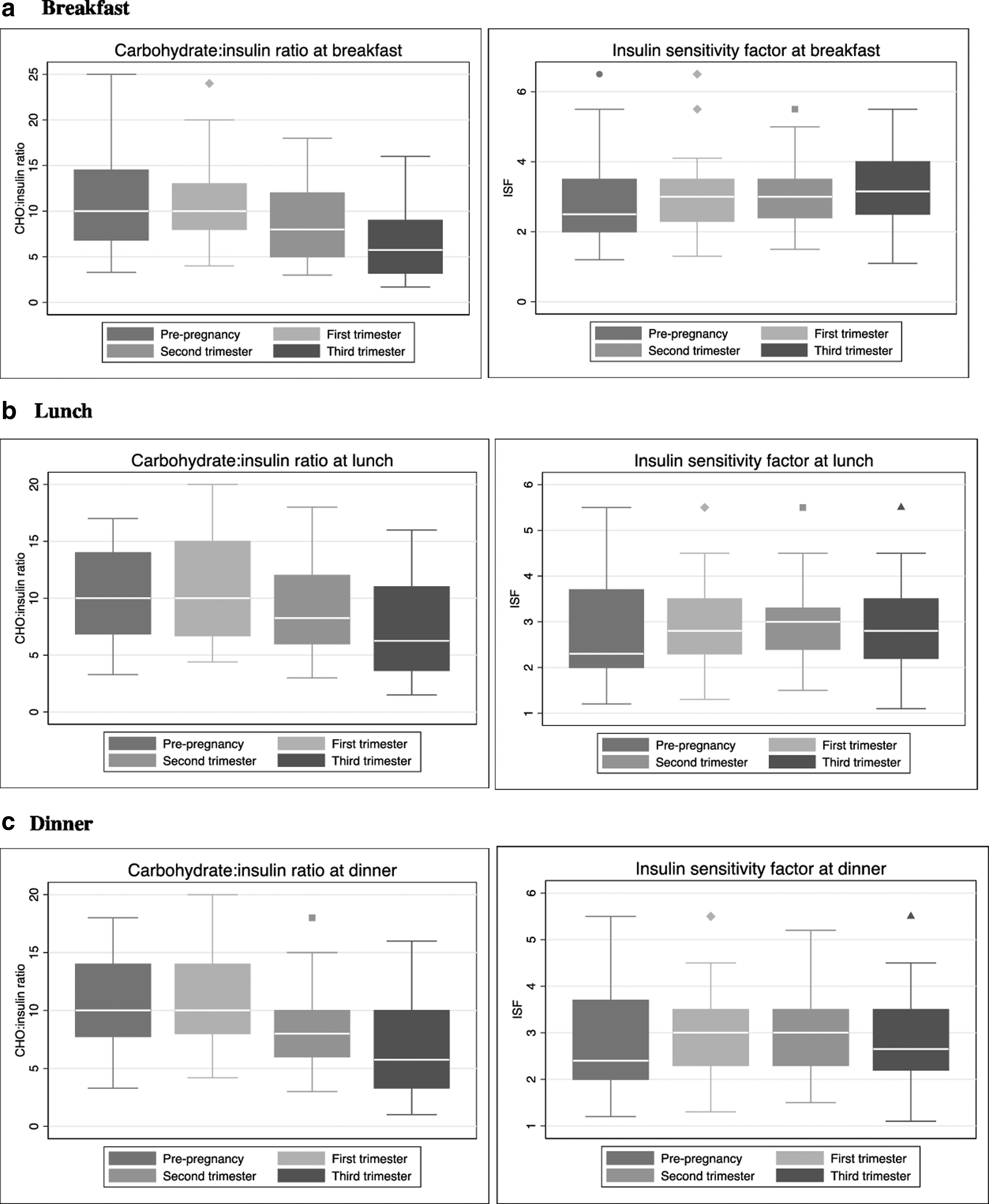
Changes in carbohydrate:insulin ratios and insulin sensitivity factor at meal times. ISF, insulin sensitivity factor.
Discussion
In one of the largest cohort studies in type 1 diabetes comparing CSII and MDI in pregnancy, we captured care provision, diabetes history, insulin regimens, glycemic control, diabetes complications, and maternal and neonatal outcomes. Sixty percent of women in both groups attended preconception and early pregnancy care, and all women were treated within the same model of care in a specialized multidisciplinary diabetes and maternity service. There was no difference between groups in maternal characteristics, duration of diabetes, glycemic control, and microvascular complications at baseline. Women treated with CSII required significantly less insulin than women treated with MDI at all stages of pregnancy and had a smaller increment in insulin dosage. Women treated with CSII and MDI achieved similar glycemic control throughout pregnancy and had no differences in diabetes complications, maternal and neonatal outcomes. In women with CSII, carbohydrate-to-insulin ratios were intensified from prepregnancy to the first trimester and across gestation, and ISFs changed little across gestation.
In this study, women with type 1 diabetes treated with CSII and MDI had similar diabetes duration, complications, and baseline glycemic control. This is unlike other studies in the area 8,11,12,14 and enabled direct comparison of insulin regimens, glycemic control, and diabetes complications throughout the pregnancy. Women using CSII required significantly less insulin to achieve equivalent glycemic control to MDI, and subsequently had less intensification of total daily insulin dose per kg (TDD/kg) during pregnancy (40% vs. 58%). Similarly, low TDD/kg in women using CSII has been reported in prior studies. 8,10,15,18 The proportions of basal to bolus insulin remained relatively stable, with no difference between groups. Lower insulin requirements with CSII have been described in other cohorts during pregnancy 8,10,19 , confirming improved efficacy in insulin delivery.
Tight glycemic control improves pregnancy outcomes in type 1 diabetes, 1 but it is unclear whether insulin delivery method improves control at a generally motivated life stage or improves outcomes. Prior studies have reported improved HbA1c in women on CSII during pregnancy 11 or earlier achievement of control, 8 however, these studies had higher rates of preconception care 8,11 and lower preconception HbA1c in the CSII group. 11 In one of the largest studies, Kekalainen et al. reported no difference in HbA1c during pregnancy (n = 48 CSII and n = 87 MDI), yet, women using CSII were older, had more diabetes complications, and were commenced on CSII preconception if not achieving HbA1c targets with MDI. 12 The literature remains inconclusive due to insufficient evidence and heterogeneity between studies preventing meta-analysis. 7,13 In our large-scale study of women treated with CSII compared with MDI in a multidisciplinary specialist unit, despite increased diabetes nurse and specialist input, there was no difference in glycemic control between groups preconception or during each trimester. Notably, there was a trend toward poorer control in the CSII group in the third trimester (P = 0.05), indicating that these women continue to need intensive titration throughout pregnancy to meet increasing insulin requirements. There was no difference in rates of microvascular progression, maternal hypoglycemia, or DKA between groups. Importantly, women in the CSII group had no episodes of severe hypoglycemia, and only one episode of DKA, a frequent concern in the event of pump failure. 6
Studies comparing pregnancy outcomes in women with type 1 diabetes treated with CSII and MDI have largely found no differences. 6,8,10,12,14,18 However, studies are frequently small 14,18 and underpowered for important pregnancy outcomes. 10,12,14 A 2016 Cochrane review found only five RCTs with 154 pregnancies in over 30 years (1984–2005) and reported no differences in pregnancy outcome. 7 Since these trials, CSII technology has progressed significantly with an emphasis on patient education, self-management, and use of bolus calculators. There is a need for well-designed RCTs with adequate power to examine pregnancy outcomes with different insulin delivery modes. More recently, Ranasinghe et al. were unable to rule out differences in pregnancy outcome in meta-analysis of seven observational studies (2008–2013) due to high risk of bias and heterogeneous outcome definitions. 13 In our relatively large and unbiased cohort with standardized outcome definitions, we too found no difference in maternal and neonatal outcomes. It is likely that this relates to the similar glycemic control achieved preconception and throughout pregnancy. Overall, this evidence does not support benefits in pregnancy outcome using CSII therapy in unselected patients with generally good control. Education is vital to enhance the effects of CSII therapy in pregnancy, and selected compliant, motivated and technically sophisticated patients generally manage best on CSII. The cost of CSII therapy 20 and time commitment from the patient and hospital staff are significant considerations, which require justification before advocating publicly funded CSII therapy. Notably, a recent study of closed loop insulin delivery in pregnancy showed more time in the normoglycemic range. 21 However, further data are required on the safety, efficacy, and feasibility of this method and on pregnancy outcomes. 21
There is little published evidence to guide adjusting CSII settings during pregnancy. Mathiesen et al. proposed that this may explain the lack of superiority of CSII in pregnancy. 16 In a multicentre Italian observational study of 101 women with a preconception HbA1c 6.9% (52 mmol/mol), TDD of insulin increased by 40% such that bolus insulin represented 60% of TDD, 15 similar proportions to that of our study. They found that carbohydrate to insulin (CHO:insulin) ratios decreased by 44% at breakfast, 16% at lunch, and 51% at dinner. 15 Notably, 28% of women were using CGM concurrently and 32.6% switched to CSII in pregnancy, which may explain large titrations. In a Danish cohort of 27 women from within an RCT of continuous glucose monitoring versus routine care, 16 CHO:insulin ratios declined fourfold and were most pronounced at breakfast (from median 12 [range 4–20] to median 3 [2–10]). In our real-world study without the benefit of CGM, CHO:insulin ratios declined by 30% at breakfast, 27% at lunch, and 22% at dinner. We also add to the literature by reporting changes in ISF during pregnancy. Surprisingly, we found very minimal changes in ISF, when reduced insulin sensitivity is the underlying physiological change driving insulin demands. Physicians do not have a uniform approach to titrating ISF, and thus, we need further research to guide practice in this area.
Strengths of this study include the large well-described cohort managed in an academic center by experienced clinicians. We examine standardized outcomes, enhancing generalizability of results. All women were on CSII before pregnancy (except one), women on CSII and MDI therapy had similar diabetes duration, rates of preconception care, diabetes complications, and glycemic control at baseline and were treated under the same model of care. This study provides a fair and accurate representation of the effects of CSII in pregnancy in an unselected population. However, literature in this area remains limited, and we suggest that a T1DM registry in pregnancy would be helpful to improve quality of care and reduce practice variations, particularly for CSII therapy. Our study is underpowered due to few events for many of the outcomes, and larger prospective studies are needed to validate our findings. We appreciate that this is an observational study and that HbA1c has limitations in pregnancy, and we were not able to provide detailed blood glucose data. Women in our cohort had “reasonable” but not “optimal” glycemic control, particularly in the CSII group in the third trimester, and although individual determinants cannot be examined, greater insulin dose escalation may have improved glycemic control. Continuous glucose monitoring (or sensor augmented pump therapy) would have been useful in this setting. We did not record changes in individual basal rates for women on CSII. We have not examined indication for CSII therapy nor have we evaluated quality-of-life effects of CSII therapy, important considerations in initiating therapy. Finally, women in Australia generally require private health insurance to fund CSII therapy, which is granted by the clinician based on patient preference, accessibility, and suitability. Given the findings of our study, we do not feel that this resulted in a treatment bias.
Conclusions
In women with type 1 diabetes treated with CSII compared with MDI insulin in a quaternary public hospital system, women usually received preconception care and were seen by a multidisciplinary team throughout pregnancy. Insulin was administered via CSII in one in four women with type 1 diabetes, and both groups achieved similar glycemic control throughout pregnancy. Insulin doses were lower with CSII. There was no difference in maternal or neonatal outcomes between groups, however, studies of larger sample size are needed to validate these findings. In women with CSII, carbohydrate to insulin ratios needed intensification, particularly in the second and third trimesters. However, more adaptation around ISFs is needed to improve bolus calculator settings and potentially further improve glycemic control. Overall, literature on CSII in pregnancy is limited, yet, extending prior small studies and a Cochrane review, our data do not support a benefit of CSII in unselected women with type 1 diabetes in pregnancy. Well-designed RCTs with adequate power to examine differences in glycemic control and pregnancy outcomes are needed before recommending CSII in pregnancy given potentially higher patient and staff demands and costs and the lack of evidence for improved HbA1c or better health outcomes in pregnancy.
Footnotes
Acknowledgments
The authors acknowledge senior biostatistician Sanjeeva Ranasinha (Monash Centre for Health Research and Implementation, Monash University) who provided advice on statistical methodology and Michelle Knight (Monash Women's Services, Monash Health) for her assistance in data acquisition.
Author Disclosure Statement
No competing financial interests exist. H.J.T. and J.A.B. are National Health and Medical Research Council (NHMRC) postdoctoral fellows. S.K.A. holds an NHMRC postgraduate scholarship.
Contribution to Authorship
S.K.A. developed study design, conducted data analysis and interpretation, and drafted the article. H.J.T. developed study design, interpreted data, and provided significant intellectual contribution and critical review of the article. M.S. and A.P. contributed to data collection and interpretation and critical review of the article. G.S., J.A.B., J.R., and E.M.W. contributed to data interpretation and critical review of the article. All authors approved the final version of the article.