
Abstract
Introduction:
Fasting Ramadan carries a high risk for patients with type 1 diabetes (T1DM). Data on the optimum insulin regimen in these patients are limited.
Objectives:
To compare glucose profiles in patients with T1DM who use continuous subcutaneous insulin infusion (CSII) compared with those who use multiple daily injections (MDI) insulin regimen during Ramadan fast. The primary outcome was rates of hypoglycemia. Other outcomes included glycemic control, number of days needed to break fasting, and acute glycemic complications.
Methods:
Patients with T1DM who were on CSII or MDI and decided to fast Ramadan were recruited. Glucose data collected using self-monitoring of blood glucose (SMBG) and continuous glucose monitoring (CGM) were compared in the two groups, CSII and MDI, and glucose control was assessed by measuring serum fructosamine levels.
Results:
A total of 156 patients were recruited, 61 on CSII and 95 on MDI. There was no difference in the rate of mild hypoglycemia <4.4 mmol/L (<80 mg/dL) (8.6% ± 6.1% in the CSII group and 9.85% ± 9.34% in the MDI group, P = 0.96). The mean rate of severe hypoglycemia <2.7 mmol/L (<50 mg/dL) was also not different in both groups (0.99% ± 1.7% in the CSII group compared to 1.7% ± 4.7% in the MDI group, P = 0.23). There was no difference in glycemic control as measured by fructosamine levels or the number of days that patients have to stop fasting. Glucose variability was significantly better in CSII group (SMBG; standard deviation [SD] 66.9 ± 15.3 vs. 76.9 ± 29.9, P = 0.02) (CGM; SD 68.1 ± 19.6 vs. 78.7 ± 24.9, P = 0.04). No diabetic ketoacidosis was reported in either group.
Conclusion:
In patients with T1DM who fast Ramadan, there was no difference in rates of hypoglycemia or hyperglycemia between CSII and MDI. However, CSII was associated with less glucose variability.
Introduction
M
Large gaps remain in understanding the best treatment choices needed to help patients with diabetes fast Ramadan safely. Published studies comparing different treatment modalities in patients with type 1 diabetes who fast Ramadan are very sparse and do not extend beyond observational reports and case series. 6 –16
Continuous subcutaneous insulin infusion (CSII) (or Insulin pump therapy) is an appealing strategy that offers flexibility and precision to administering insulin. In selected patients, insulin pump therapy has been shown to be associated with better glucose control and a possible reduction in the incidence of hypoglycemia when compared with multiple daily injections (MDI) insulin regimen. 17,18
The primary aim of this study was to compare rates of glucose control in patients with type 1 diabetes who use insulin pump and those who are on a multiple daily insulin injection regimen during Ramadan fast.
Materials and Methods
The study was a prospective cohort study that involved three National Guard Hospitals located in three cities (Dammam, Alahsa, and Riyadh) in Saudi Arabia. The primary aim of the study was to compare rates of glucose control in patients with type 1 diabetes who use insulin pump and those who are on a multiple daily insulin injection regimen during Ramadan fast. Other studied outcomes included glucose variability, weight changes, and number of days that patients had to stop fasting.
Patients were recruited from the diabetes clinics and were eligible if their age was 14 years or older, had a diagnosis of type 1 diabetes for at least 6 months, and were on either insulin pump or multiple daily insulin injection regimen. Patients had to be willing to perform self-monitoring of blood glucose (SMBG) and have no other contraindication to fast Ramadan. Patients on insulin pump were required to be on this therapy for at least 3 months. All patients were using the same pump (MiniMed Paradigm Real-Time 722 by Medtronic). MDI regimen included a basal insulin (Glargine or Detemir) combined with a rapid-acting insulin (Aspart, Glulisine, or Lispro). Patients were excluded if they were pregnant, cannot or were unwilling to fast, cannot perform SMBG, and had renal or hepatic impairment, adrenal insufficiency, psychiatric illness, or history of alcoholism.
The institutional review board of Ministry of National Guard Health Affairs (MNGHA) approved the study. All participants signed an informed consent. The study was sponsored through a grant from King Abdullah International Medical Research Center (KAIMRC). Roche pharmaceutical company provided the glucometers (Accu-Check Performa®), glucose strips, and lancets free of charge and was not involved in the design and conduct of the study. The study was registered at
Patients with type 1 diabetes attending diabetes clinics were offered to participate. For each patient recruited on insulin pump therapy, one patient on MDI regimen was recruited. Within the 2 months before the month of Ramadan, patients were screened and offered participation. Baseline demographic data were collected using paper questionnaires and clinical examination, while baseline laboratory tests included glycated hemoglobin (HbA1c) and fructosamine. Patients were provided with the same glucometer (Accu-Check Performa by Roche). Patients were asked to check capillary glucose six to seven times per day, every 2–4 h during the fast, prebreakfast meal (iftar), premidnight and 2 h postmidnight, and predawn meal (Sahour). All patients received formal education on aspects of diabetes in Ramadan by certified diabetes educators. Patients were offered to come during Ramadan for a 6-day continuous glucose monitoring (CGM) placement using iPro® device (Medtronic, MN), but this was not compulsory. iPro is a blind CGM device, so patients were not able to monitor their own blood glucose. It was assured at the time of insertion that patients were fasting. All patients were required to return for follow-up visits within 2 weeks after the end of Ramadan. In this visit, data from glucometers were downloaded and laboratories were drawn for HbA1c and fructosamine. In addition, patients were required to fill up a paper questionnaire on events in Ramadan. Due to the risk of fasting in patients with type 1 diabetes and following professional guidelines of target fasting/premeal glucose levels of 4.4–7.2 mmol/L (80–130 mg/dL), 19 a capillary glucose value of <4.4 mmol/L (80 mg/dL) was defined as mild hypoglycemia. Severe hypoglycemia was defined as a capillary glucose level of <2.7 mmol/L (50 mg/dL) or if the patient required assistance during the episode. Significant hyperglycemia was defined as a capillary glucose of >13.9 mmol/L (250 mg/dL). Patients were advised to stop their fast if they had hypoglycemia or significant hyperglycemia.
Statistical analysis
Data were entered and analyzed using the Statistical Package of Social Sciences. Continuous results were expressed as means and standard deviations (SDs) or medians and interquartile ranges according to the data distribution, and categorical data were presented as proportions with 95% confidence intervals. Between-group comparison was done using a Student's t-test or Mann–Whitney U test where the data are not normally distributed. For categorical data, chi-square test (with Yates' correction or Fisher's exact test where appropriate) was used. Paired t-test was used to compare pre-Ramadan versus post-Ramadan data. The level of statistical significance was chosen as P ≤ 0.05 (two sided).
Results
A total of 409 patients were screened, of which 211 were deemed eligible and offered participation. Of those, 175 patients agreed to participate. After excluding withdrawals, 156 patient were included, 61 on insulin pump and 95 on MDI. Out of 156, SMBG data were available for 116 patients: 46 patients on insulin pump, of which 37 had CGM placement, and 70 patients on MDI regimen, of which 41 had CGM placement. The baseline characteristics of patients are shown in Table 1.
BMI, body mass index; HbA1c, glycated hemoglobin; MDI, multiple daily injections.
The mean age was 23.4 ± 06.1 in the insulin pump group and 21.3 ± 06.3 in the MDI group. The majority of insulin pump patients were females (70.5%) and of higher education (51.7%). The mean duration of diabetes as well as body mass index were not different in both groups, while the baseline HbA1c was significantly lower in the insulin pump group compared to the MDI group (HbA1c 8.0 ± 1.1 vs. 8.8 ± 01.7, P = 0.045).
SMBG data
Mean blood glucose was not different between the insulin pump and MDI groups (11 ± 2.8 mmol/L vs. 10.5 ± 2.5 mmol/L, P = 0.332) (Table 2). Glucose variability as measured by SD of SMBG was significantly less in the insulin pump group compared to the MDI group (3.7 ± 0.85 vs. 4.2 ± 1.6, P = 0.02). Mean rates of mild hypoglycemia (<4.4 mmol/L) were less in the insulin pump group than in the MDI group, however, not statistically different (8.6 ± 6.1 vs. 9.85 ± 9.34, P = 0.962). Similarly, rates of severe hypoglycemia <2.7 mmol/L were not statistically different in the insulin pump and MDI groups (0.99 ± 1.7 vs. 1.7 ± 4.7, respectively, P = 0.23). The low blood glucose index and high blood glucose index were not different between patients in the insulin pump and MDI groups. Mean rate of significant hyperglycemia (glucose level of >13.9 mmol/L) was higher in the insulin pump group (54.1 ± 26.02 vs. 43.1 ± 25.2, P = 0.029) compared to the MDI group. For a subgroup of patients (n = 49, 10 pump and 39 MDI), data were available on hypoglycemia <3.8 and <2.2 mmol/L; the mean rates were (7.3 ± 5.9 vs. 10.6 ± 10.3, P = 0.673) and (0.7 ± 1.1 vs. 2.5 ± 4.8, P = 0.976), respectively. In addition, for patients with HbA1c <7.5 before Ramadan (n = 20, 8 pump and 12 MDI), comparison results confirm no statistical difference in rates of mild or severe hypoglycemia (11.4 ± 7.6 in pump vs. 12.9 ± 10.6 in MDI, P = 0.72) and (0.7 ± 1.4 in pump vs. 1.6 ± 2.8 in MDI, P = 0.97), respectively.
BG, blood glucose; SD, standard deviation.
CGM data
Mean blood glucose was not different between the insulin pump and MDI groups (9.6 mmol/L ± 2.2 vs. 9.9 mmol/L ± 2.6, P = 0.33) (Fig. 1 and Table 3). Glucose variability was significantly less in the insulin pump group compared to the MDI group (SD 3.7 ± 1.0 vs. 4.3 ± 1.3, respectively; P = 0.04). Rates of hypoglycemia <3.8 mmol/L were not different in the insulin pump and MDI groups (3.05 ± 2.08 vs. 3.8 ± 3.44, respectively, P = 0.24) (Fig. 2). Similarly, rates of severe hypoglycemia <2.7 mmol/L were not different in both groups (1.2 ± 1.5 vs. 1.17 ± 1.5, respectively; P = 0.89). Rates of significant hyperglycemia were also not different in both groups (10.5 ± 5.2 vs. 9.85 ± 5.2, respectively, P = 0.58).

Comparison of average blood sugar with standard error as measured by CGM distributed through different times of the day in relation to meals. Sleeping hours, Ramadan reversed sleep pattern; Iftar, breakfast meal at Sunset; Sahour, predawn meal; CGM, continuous glucose monitoring.
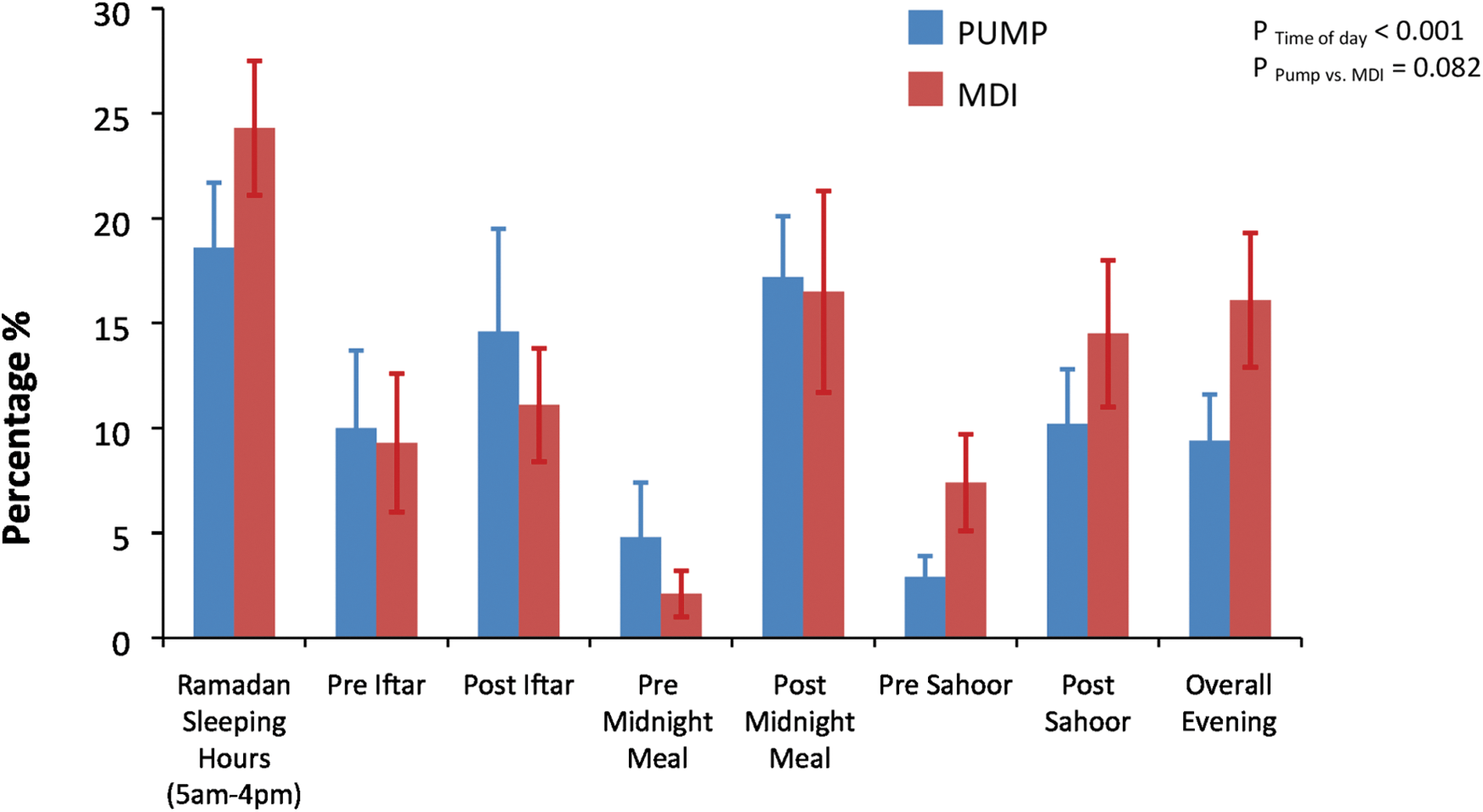
Hypoglycemia rate (%) according to different times of day as measured by CGM. Results are mean with standard error; Sleeping hours, Ramadan reversed sleep pattern; Iftar, breakfast meal at Sunset; Sahour, predawn meal.
Data are mean ± SD. Excursions are defined as number of all consecutive recordings outside the limit; Duration is percentage of time spent at defined blood sugar range per 1 week.
AUC, area under curve.
Glucose control and safety of fast
Glucose control before Ramadan was significantly better in the insulin pump group compared to the MDI group (HbA1c 8.0 ± 1.1 vs. 8.8 ± 01.7, P = 0.045). This deteriorated after Ramadan in both groups with continuation of better control in the insulin pump group (HbA1c 8.4 ± 1.3 in the insulin pump group vs. 9.3 ± 02.1 in the MDI group, P = 0.02). Levels of serum fructosamine were not different between both groups before Ramadan (385.6 ± 76.1 μmol/L in the insulin pump group vs. 409.2 ± 95.5 μmol/L in the MDI group, P = 0.126). These levels increased after Ramadan in both groups, but continued to be not different between the groups (392.8 ± 60.1 in CSII vs. 405.9 ± 84.4 in MDI, P = 0.61).
More patients on insulin pump managed to fast the whole month of Ramadan without the need to break their fast: 31.2% versus 22.1% of patients in the MDI group could achieve this (P = 0.41). There was no difference in the average number of days that fasting had to be stopped between both groups (4.1 ± 5.3 in the insulin pump group compared to 5.7 ± 5.8 in MDI, P = 0.23). The main reasons for stopping fasting was hypoglycemia (81.2% in the insulin pump group and 88.7% in the MDI group), followed by significant hyperglycemia (18.7% and 18.9% respectively).
There were two hospitalizations in the MDI group, one due to severe hyperglycemia and the other due to severe hypoglycemia. One visit to the emergency department was reported in the insulin pump group due to hyperglycemia. No case of diabetic ketoacidosis was reported during Ramadan in both groups.
Both groups lost weight after Ramadan. In the insulin pump group, pre-Ramadan weight was (69.3 ± 21.2) kg versus (67.0 ± 17.1) kg post-Ramadan (P = 0.245), while in the MDI group, pre-Ramadan weight was (66.2 ± 15.1) kg versus (64.6 ± 14.3) kg post-Ramadan (P = 0.118).
Discussion
Despite recommendations from professional organizations against fasting Ramadan, a significant number of patients with type 1 diabetes insist on fasting. 3,5 The main concern for patients with type 1 diabetes during Ramadan fast is hypoglycemia and to a lesser extent hyperglycemia. The EPIDIAR was a large epidemiological study that looked at features of patients with diabetes who fast Ramadan. The study found that 42.8% of patients with type 1 diabetes fast Ramadan and the incidence of severe hypoglycemia was increased by 4.7 times, while the risk of hyperglycemia was increased by five times in these patients. 5 The ideal insulin regimen to help patients with type 1 diabetes fast Ramadan safely remains not known. Only few studies have documented the safety and efficacy of different insulin regimens on Ramadan fasting in patients with type 1 diabetes. 9,13,16 Kadiri et al. reported on patients with type1 diabetes during Ramadan fasting using insulin lispro instead of regular human insulin combined with intermediate acting insulin taken twice daily. 6 The regimen that included insulin lispro showed improvement in postprandial glucose levels and was associated with fewer hypoglycemic events. A small study that included 22 patients with type 1 diabetes during Ramadan fast found that glucose levels were better in patients on multiple daily insulin injections regimen compared to conventional twice-daily insulin regimen, but with higher rates of hypoglycemia. 9
Insulin pump therapy was found to be associated with better glucose control compared with MDI when used in selected patients with type 1 diabetes. 17,18 The evidence for hypoglycemia is less clear. Most studies do not show a difference in rates of hypoglycemia between insulin pump therapy and MDI. A Cochrane review found that severe hypoglycemia appeared to be reduced in patients on insulin pump therapy compared to MDI, although no difference was observed in the frequency of nonsevere hypoglycemia. 18 A few studies are available on the use of insulin pump therapy in patients with type 1 diabetes during Ramadan Fast. 13 –16 The largest series reported included 49 patients and found that 61.2% of these patients could fast the whole month of Ramadan with no consequences, while hypoglycemia occurred in 34.7% of patients, necessitating breaking the fast. 9 The only published data on the comparison between insulin pump therapy and insulin injections during Ramadan fast used twice-daily conventional insulin. 13 This study found that rates of hypoglycemia was much less in patients on insulin pump therapy (16%) compared to 29% in the conventional insulin regimen group, while glucose control was better in the insulin pump therapy group (mean HbA1c 7.8%) compared to the conventional insulin group (mean HbA1c 9.1%).
To our knowledge, our study provides the first data about glucose profiles of patients with type 1 diabetes who use insulin pump therapy compared to those who use MDI during Ramadan fast. We found that hypoglycemia rates were not statistically different in both groups. Rates of hyperglycemia were higher in patients on insulin pump when using SMBG data, but were not different when assessed using CGM. Short-term glycemic control as assessed by fructosamine levels did not differ in both groups. The main concern from fasting Ramadan for patients with type 1 diabetes is hypoglycemia and to a lesser extent hyperglycemia. Hypoglycemia is common during Ramadan fast in patients with type 1 diabetes and is the most common cause that necessitates breaking the fast. 2,3 We found that the rate of severe hypoglycemia was low (mean 1.3%). Studies that included patients with type 1 diabetes who are on insulin pump during Ramadan reported no episodes of severe hypoglycemia. 11,13 –16
Reported rates of nonsevere hypoglycemia in these patients were very variable (14.2%, 13 16%, 16 and 34.7% 14 ). We found that the mean rate of mild hypoglycemia was 9.2%. A possible explanation for this wide variation is the different criteria used and different patient populations. Some studies used hypoglycemia along with the inability of patients to continue fasting as a criterion, while others used the absolute number of glucose level either capillary or interstitial through CGM. We found that glycemic variability was less in patients on insulin pump therapy compared to those on MDI, a finding that concurs with studies of patients in the nonfasting state. 19 –21 The clinical significance of this finding in patients during Ramadan fast is not known and deserves further studies.
Patients with type 1 diabetes are categorized as very high risk and previous guidelines recommended against fasting Ramadan. 2 Our data showed that these patients can safely fast Ramadan, a finding that concurs with other observations. 11,14 –16 However, a significant number of our patients had to break their fast due to hypoglycemia. Therefore, a careful selection of these patients with assurance of adequate education and supervision is important as acknowledged by the recent guidelines from the international diabetes federation. 3
Our study has several limitations. The self-selective nature of our two groups of patients and the absence of randomization could make it difficult to generalize the results. The baseline characteristics in both groups that were well-matched should have reduced the related bias. CGM data were not available for all patients since this was voluntary.
In conclusion, glucose control and rates of hypoglycemia were not different in patients with type 1 diabetes during Ramadan fast whether they used insulin pump therapy or MDI insulin regimen. Further larger randomized studies are needed to confirm these findings and determine the role of glucose variability in this population.
Footnotes
Acknowledgments
The study was sponsored through a grant from King Abdullah International Medical Research Center (KAIMRC). We gratefully acknowledge the generosity of ROCH pharmaceuticals for providing the glucometers, glucose strips, and lancets free of charge. Our thanks and appreciation to the efforts of our study site coordinators: Ms. Amal Aljaafari, Ms. Fatme Elhabbal, Ms. Suzan Oraibi, and Ms. Shahinaz Bashir, and to our diabetes educators: Ms. Mehad Awad, Ms. Faiza Haider, Ms. Sultana Alenazi, Ms. Rasha Alwehaib, Ms. Sabah Alshuwish, and Ms. Rahab Hamad. We also thank Dr. Waleed Tamimi, Head division of Clinical Chemistry at King Andulaziz Medical City, Riyadh, for his advice and support. Parts of this study were presented as poster presentation at the Endocrine Society's 98th Annual Meeting and Expo, April 1–4, 2016, Boston—SAT-700 on April 2, 2016.
Author Disclosure Statement
No competing financial interests exist.