
Abstract
Introduction
C
In the diabetes area, R2R has been used for daily adaptation of basal insulin, 3 meal boluses, and for adapting a cost function residing in a control algorithm. 4 Recently, an R2R update of basal insulin therapy based on continuous glucose monitoring (CGM) measurements 5 and an R2R closed-loop strategy 6 have been tested in silico with the UVA/Padova simulator. 7
Encouraged by the positive in silico results, 5,6 we proposed that the T1D subjects enrolled in a recent 1-month closed-loop clinical trial 8 to extend their closed-loop treatment with an additional month by using an early prototype of R2R adaptive AP (R2R-AP) for 24 h/day in free-living conditions, that is, with no clinical supervision and no protocol constraints. Data from the last week of R2R-AP versus the last week of non-adaptive AP (NA-AP) were compared, with time-in-target range (3.9–10 mmol/L) over 24 h as the primary endpoint.
By comparing the performance of the adaptive with the non-adaptive version of the same algorithm, this proof-of-concept study offers a first quantitative assessment of the improvement brought by adaptation to closed-loop control. Further, this trial represents the first test in free-living conditions of our R2R-AP system, a step toward a second generation of AP prototypes, although still in an early stage of development.
Research Design and Methods
Study design and participants
In 2014, a multinational, randomized, crossover open-label study in patients with T1D was completed on a population of 32 patients. The aim was to investigate the use of an NA-AP during evening and night at home versus sensor augmented pump (SAP) therapy. 9 After the completion of this study, 20 out of the 32 patients from medical centers at the universities of Amsterdam (the Netherlands), Montpellier (France), and Padova (Italy) consented to participate in a 1-month single-arm extension study with the aim of investigating the use of an NA-AP 24 h per day in free-living conditions. 8 Of these 20 patients, 18 were enrolled in the present second extension study. The main inclusion criteria were age 18–69 years, a diagnosis of T1D for at least 6 months according to the American Diabetes Association criteria, 10 a body mass index of <35 kg/m2, and a concentration of HbA1c between 7.5% and 10% (58–86 mmol/mol). To mitigate risk, patients with severe hypoglycemia in the past year or ketoacidosis in the past 6 months were excluded from participation in the study. For the complete inclusion and exclusion criteria list, see Kropff et al. 9 The potential participants were provided with an information letter and a consent form, which were specific to the extension study. This trial was performed in accordance with the Declaration of Helsinki, and it was approved by the institutional ethics review board at each site.
AP platform
The AP system used in this study was the same as that used in the preceding studies. 8,9 The AP was composed of a Dexcom G4 Platinum CGM (Dexcom, San Diego, CA), an Accu-Check Spirit Combo insulin pump (Roche Diagnostics, Mannheim, Germany), and the Diabetes Assistant (DiAs) 11 developed at the University of Virginia (Charlottesville, VA) on which the R2R-AP algorithm was implemented. The DiAs consists of an Android (Google, Inc., Mountain View, CA) Nexus 5 (LG Group, Seoul, South Korea) smartphone equipped with a communication, control, and user interface software connected to the CGM and to the insulin pump via Bluetooth. The DiAs was initialized with the patient's basal insulin pattern, carbohydrate-to-insulin ratio (CR), and correction factor. In case of system dysfunction and unsuccessful troubleshooting, the control algorithm was automatically deactivated after 30 min and the pump basal rate was reset to the patient's pre-study basal rate. The patients interacted with the DiAs graphical user interface, 12 which allows real-time inputs such as meal announcements, pre-meal capillary glucose level, or self-administered hypoglycemia treatment. The DiAs interface displays CGM and insulin delivery graphs, and it provides hypo- and hyperglycemia alerts through a traffic lights representation. DiAs also allows for secured data streaming over the internet to a remote telemedicine website 13 through the smart-phone 3G connection. In this study, the telemedicine was used only for technical reasons: No clinical 24/24 h monitoring was in place, and no automatic alert message was sent by the telemedicine website to the study team. However, since the system tested in this trial is an early-stage prototype, the engineering team was allowed to access the telemedicine to verify the prototype functioning.
Non-adaptive artificial pancreas
The non-adaptive control algorithm is the so-called Modular model predictive control (MPC), a control algorithm based on the modular architecture discussed in Patek et al., 14 and previously presented in Kovatchev et al. 15 The architecture is composed of two main modules. The first is the continuous safety module, which implements a safety supervision algorithm in charge of reducing insulin injections suggested by the control algorithm if hypoglycemia is forecasted. The second is the real-time control module implementing the MPC described in Toffanin et al., 16 which adjusts the nominal basal insulin delivery (patient's basal profile) and the meal boluses in real time based on the past CGM data and on an estimate of the patient's glycemic status. This control algorithm, ported on the DiAS platform, has been tested extensively in semi-controlled hotel studies 17 and outpatients 9 ; in particular, it was used day and night for 1 month in free-living conditions. 8
Adaptive R2R-AP
By design, the proposed MPC algorithm operates real-time corrections to the basal insulin and to the meal bolus. Using these patient-specific signals as a reference allows informing the controller of important clinical knowledge. Given their important role in the proposed control strategy, these reference signals might have a relevant impact on final control performance. The basal profile and the CR pattern (determining meal boluses) are entered by the patient during the initialization phase but may be inadequate due to a sub-optimal initialization and/or to the patient changes over time (inter-day variability). To mitigate these problems, we introduced the R2R-AP, that is, the NA-AP enriched with an additional module implementing the R2R strategy described in Toffanin et al. 6 This latter module is devoted to the daily automatic adaptation of the patient's nocturnal basal insulin and diurnal CR pattern. Nocturnal basal insulin is the basal insulin needed during nighttime (00:00–08:00), whereas diurnal CR pattern is the set of CR values considered for daytime meals (08:00–00:00). The goal is to optimize the tuning of these parameters and to adapt them to the slow inter-day variability. Based on the blood glucose (BG) control observed in the previous run (day k), the R2R algorithm modifies these parameters and updates the controller for the next run (day k + 1). Since the major concern is to avoid hypoglycemia, the R2R updating law is primarily designed to minimize the percentage of time spent below 3.9 mmol/L, and parameters are modified accordingly. Once this primary goal is achieved, a secondary updating law is designed to reduce the percentage of time spent above 10 mmol/L and to bring the average BG to the desired target. Of note, each CR in the pattern is updated separately. The algorithm can handle cases when there are more than the three main CR intervals (breakfast, lunch, and dinner) to accommodate real-life needs. Daytime basal profile is not updated. No restrictions are applied to the patient's usual habits. However, in some instances, during a particular interval, the associated parameter could not be updated for that day. For example, the nocturnal basal insulin is not updated if a meal is consumed during nighttime or if temporary basal insulin modifications during nighttime occur. CR updates are aborted in case of manual user interventions on insulin delivery or in case of meals that are not compatible with the R2R algorithm. This last situation can be generated by multiple meals in the same CR interval or because of previous meals interfering with the evaluation of the performance indices associated with the current meal. Multiple meals are detected if two or more meals announced in the same CR interval are separated by at least 120 min. Otherwise, the announced meals are considered as different events of the same meal and the CR is not discarded for possible R2R updates. Moreover, both nocturnal basal and CR updates are aborted in case of insufficient data for computing the performance indices, for example, not enough time spent in closed-loop, insufficient data from CGM, or system failures. A complete description of the R2R-AP algorithm can be found in Toffanin et al. 6 This algorithm was previously tested in silico with the UVA/Padova simulator, 7 and the results obtained are also reported in Toffanin et al. 6 The R2R-AP algorithm has been implemented on the DiAs, and this early-stage prototype was tested for the first time in the trial presented in this article.
Procedures
Each patient received a refreshment training of ∼2 h on the AP platform at the clinical research center. The study personnel checked that each patient was proficient in the study device use, including the insulin pump and the CGM. After the training, the Bluetooth connections were established; the R2R-AP was initiated and turned in the closed-loop mode. The study procedures were then identical to those of the previous 4-week study extension. 8 There were no limitations on diet and normal daily activities, including exercise.
The CGM glucose alarm thresholds for hypo- and hyperglycemia were initially set at 5.0 and 11.1 mmol/L, respectively, but they could be modified by the patients. For safety, patients were instructed to test for ketones (Freestyle Precision Xtra β-Ketone; Abbott, North Chicago, IL), whether capillary glucose was >16.7 mmol/L, and to perform a capillary glucose test before making clinical decisions regarding insulin dosing or hypo- and hyperglycemia treatment. Patients were requested to check for catheter occlusion/dislodgement and pump dysfunction in case of hyperglycemia without obvious explanation, to calibrate their CGM twice daily, and to perform at least four capillary glucose measurements per day. Patients were free to adjust their meal bolus. Device data were read out at the end of the study.
Outcome metrics
R2R-AP versus NA-AP
The main aim of this study was to show the benefits of R2R-AP with respect to NA-AP after 1 month of system use. To this purpose, we evaluated glucose control during the last week of both 1-month interventions (R2R-AP and NA-AP) by using standard outcome measures. 18 Indeed, as was concluded from our in silico analyses, 6 3 weeks is the minimum time of use before benefits of the daily adjustments performed by the R2R-AP can be detected.
The primary endpoint was the percentage of time spent in target range (3.9–10 mmol/L, time-in-target) over 24 h during the last week of the study. Secondary endpoints included the percentage of time-in-tight-target (3.9–7.8 mmol/L, time-in-tight-target), mean BG, standard deviation (SD) of BG, percentage of time below 3.9 mmol/L (time-in-hypo), below 3.3 mmol/L, above 10 mmol/L (time-in-hyper), above 13.9 mmol/L, and total daily insulin use, all evaluated over the same weeks. The same outcome indices were also evaluated during nighttime (0:00–8:00), daytime (8:00–0:00), and wake-up time (7:00–8:00) as a proxy for fasting glucose.
R2R-AP: safety
Safety was assessed by the frequency of moderately severe (>15 min, <2.8 mmol/L) and overall (>15 min, <3.9 mmol/L) hypoglycemic episodes, and adverse events.
R2R-AP: technical performance
As a proxy of the technical performance of the R2R-AP system, we evaluated the percentage of time in closed-loop. For the technical performance of the R2R strategy, we evaluated the number of successful daily updates operated by R2R-AP compared with the theoretical maximum number of updates expressed as a percentage. CGM accuracy was evaluated through mean absolute relative difference (MARD) with respect to capillary glucose concentration.
R2R-AP: impact on the adapted clinical parameters
To quantify the impact of the R2R updates on the adapted clinical parameters, the distribution of the maximum percentage variation with respect to the original values was evaluated based on the parameters in which the percentage of successful updates was at least 20% of the possible theoretical updates.
R2R-AP: trends in time of glucose metrics differences
Glucose control metrics are expected to gradually improve over time, as the R2R adapt diurnal CRs and nocturnal basal insulin infusion based on the previous day performance. Therefore, we assessed the trend in the paired difference between R2R-AP and NA-AP per day over time of time-in-target, time-in-tight-target, time-in-hyper, and mean glucose with the aim of evaluating the possible advantages over time of R2R-AP versus NA-AP.
Statistical methods
Data analysis was based on a modified intention-to-treat principle. Only patients who completed at least 3 weeks of R2R-AP use over 24 h were considered for analysis. All glucose indices have been computed from CGM data.
The outcome indices are reported as median (25th, 75th percentiles) for non-normally distributed data and as mean (SD) otherwise.
R2R-AP versus NA-AP
To evaluate the statistical significance of the difference of each index, a paired-sample t-test was used for normally distributed data. Otherwise, if at least one distribution was non-normal, the nonparametric Wilcoxon signed-rank test was used. These tests are two tailed, and the considered level of significance was 0.05. Moreover, a paired difference (Δ) with its confidence interval (CI) for each pair was computed. In case of normal distribution of differences, the paired difference is shown as mean Δ (2.5% CI–97.5% CI); otherwise, the paired difference is shown as median Δ (2.5% CI–97.5% CI). For calculation of 95% CI for non-normally distributed differences, the Hodges-Lehmann procedure 19 was considered.
R2R-AP: trends in time of glucose metrics differences
The trend in time of the paired difference of glucose control metrics was evaluated as follows: For each patient (n = 18), the paired difference between the metric achieved by R2R-AP and NA-AP during each day was computed. A model describing a linear-in-time variation of the difference under consideration was then fitted by least squares. Thus, the trend in time was defined as the slope of the fitted line. If the identified trends distribution was normal, the mean trend was verified to be significantly different from zero by a paired-sample t-test. Conversely, in case of non-normal trends distribution, the median trend was compared with zero with a Wilcoxon signed-rank test. Both tests are two tailed, and the considered significance level was 0.05.
All analyses were performed with the Matlab Statistic toolbox (version 9.1).
Results
Eighteen T1D subjects participated in the study, and all of them completed the 4-week study period. The baseline characteristics of the subjects are reported in Table 1.
Baseline characteristics of the 18 T1D subjects who completed the extension experiments and who were included in the data analysis.
For categorical variables, n (%) is presented. For continuous variables, mean (SD) is presented.
CSII, continuous subcutaneous insulin infusion; T1D, type 1 diabetes; SD, standard deviation.
R2R-AP versus NA-AP
The primary and secondary outcomes are shown in Table 2. The outcomes achieved during the night, at wake-up time, and during the day are shown in Tables 3 –5, respectively. Figure 1 shows the daily median glucose trends achieved over the last week, surrounded by colored shadows representing the 25th and 75th percentiles. The R2R-AP improvements become more pronounced over the night, whereas the profiles converge again during the morning, are graphically similar during the day, and start to diverge over the evening.

Glucose profile over 24 h for NA-AP and adaptive R2R-AP. Trends are shown in terms of median (central solid line) and 25th–75th percentiles (shadowed regions). NA-AP, non-adaptive artificial pancreas; R2R-AP, run-to-run artificial pancreas.
Outcomes evaluated on the last week of the study 24 h per day.
Mean (SD) or bmedian (25th, 75th percentiles).
Paired difference (Δ): amean Δ (2.5% CI–97.5% CI) or bmedian Δ (2.5% CI–97.5% CI).
NA-AP, non-adaptive artificial pancreas; R2R-AP, run-to-run adaptive artificial pancreas; LBGI, low blood glucose index; HBGI, high BG index; CI, confidence interval; SD, standard deviation; CV, coefficient of variation.
Outcomes evaluated during each night of the last week of the study.
Significant differences have P-value in bold format.
Mean (SD) or bmedian (25th, 75th percentiles).
Paired difference (Δ): amean Δ (2.5% CI–97.5% CI) or bmedian Δ (2.5% CI–97.5% CI).
Outcomes evaluated during wake-up time in the last week of the study.
Significant differences have P-value in bold format.
Mean (SD) or bmedian (25th, 75th percentiles).
Paired difference (Δ): amean Δ (2.5% CI–97.5% CI) or bmedian Δ (2.5% CI–97.5% CI).
Outcomes evaluated during each day of the last week of the study.
Mean (SD) or bmedian (25th, 75th percentiles).
Paired difference (Δ): amean Δ (2.5% CI–97.5% CI) or bmedian Δ (2.5% CI–97.5% CI).
Twenty-four-hour glucose
Overall, a difference of Δ = 5.08% (P = 0.099) was achieved on time-in-target by R2R-AP versus NA-AP, whereas a difference of Δ = 6.08% (P = 0.0508) was achieved on time-in-tight-target. A difference of Δ = −5.19% (P = 0.10) was obtained in time-in-hyper (>10 mmol/L), whereas the differences on the other outcomes were negligible. None of these differences were statistically significant.
Nighttime glucose
Time-in-target was increased by 9.70% (P = 0.034), and this difference was significant. Time-in-hyper was reduced by 10.26% (P = 0.0266), and this reduction was also significant and not accompanied by an increased risk of hypoglycemia. Indeed, neither time-in-hypoglycemia (<3.9 mmol/L) nor the number of hypoglycemic events was increased. A difference of Δ = 9.38% (P = 0.065) in time-in-tight target, and of Δ = −0.58 mmol/L (P = 0.08) in mean glucose were also observed, even though these differences were not statistically significant.
Wake-up glucose
Mean glucose at wake-up time was decreased by 1.11 mmol/L (P = 0.0199), time-in-tight-target was increased by 21.58% (P = 0.0027), the median time-in-target range was increased (92.43% vs. 84.54%, P = 0.0249), and the median time above target was almost halved (7.57% vs. 14.29%, P = 0.0468). All the differences were statistically significant. Further, time-in-hypoglycemia was 0.00 (0.00, 0.00) with both treatments.
Daytime glucose
A comparison between R2R-AP and NA-AP showed neither material nor statistically significant differences. Nevertheless, R2R-AP was equally safe as NA-AP.
Insulin
No significant changes were found in insulin delivery between R2R-AP and NA-AP in all the considered daily subintervals. In the 24-h period, a nearly significant increase in the percentage of total insulin delivered as basal, Δ = 4.77% P = 0.0518, was seen.
R2R-AP: safety
As for the NA-AP, 8 the R2R-AP proved to be safe: No difference was found in low BG index and high BG index, 20 no serious adverse events occurred, including no severe hypoglycemic episodes as defined by The Diabetes Control and Complications Trial, 21 and no hospitalization for ketoacidosis was seen.
R2R-AP: technical performance
The R2R-AP system technical performance was evaluated on 15 patients since three patients experienced problems in collecting this information. Overall, CGM accuracy expressed as MARD with respect to capillary glucose concentration was 12.32% (10.79, 14.83). During the last week of the study, R2R-AP was active 86.55% (81.39, 92.62) of the time, similar to the NA-AP system, 90.76% (81.09, 93.99), P = 0.93. Nocturnal basal was successfully updated by the R2R-AP 62% of the time. In contrast, only 23% of diurnal CR updates were successfully completed by R2R-AP. The classification of the achieved non-successful updates is displayed in Figure 2: left panel for nocturnal basal and right panel for diurnal CR.
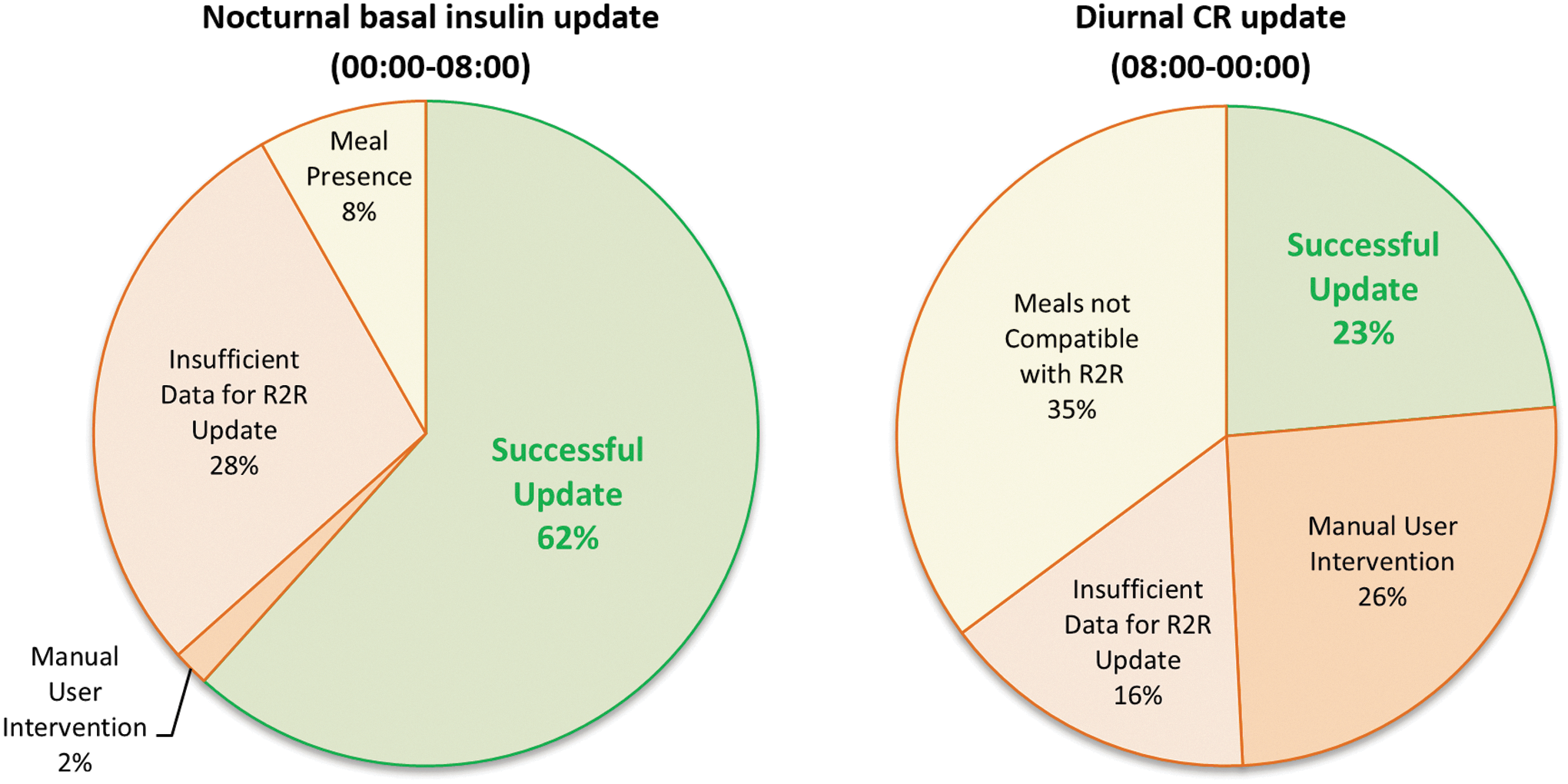
Left panel. Aborted nocturnal basal insulin update classification. Right panel. Aborted diurnal carbohydrate-to-insulin ratio pattern update classification.
R2R-AP: impact on the adapted clinical parameters
The parameters successfully adapted by the R2R algorithm resulted in a maximum percentage variation of 34.33% (21.24) for nocturnal basal insulin, and of 13.09% (8.58, 17.95) for diurnal CRs.
R2R-AP: trends in time of glucose metrics differences
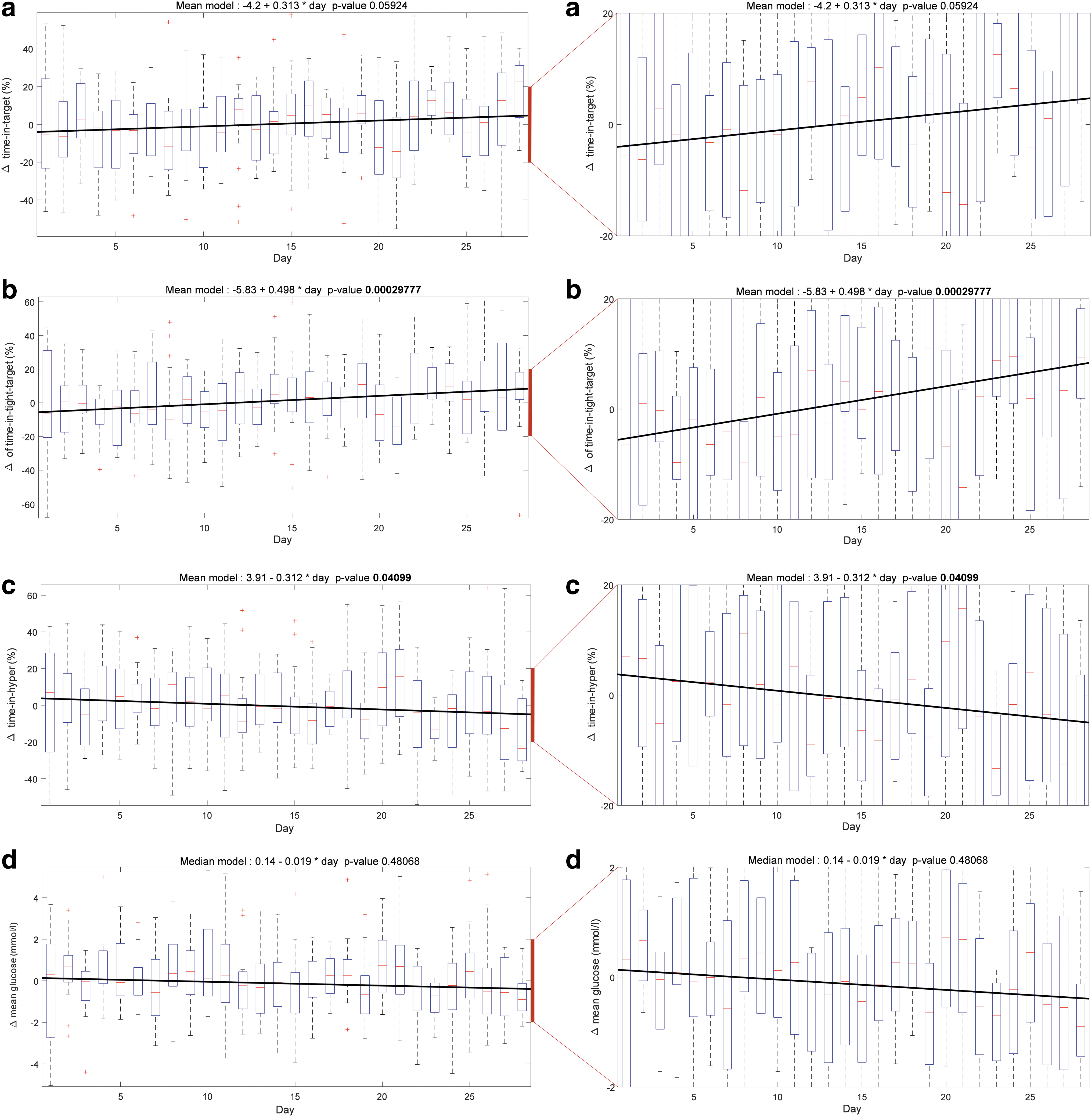
Figure 3 shows the daily variation in the difference of the control metrics achieved by R2R-AP versus NA-AP. For each day, a boxplot of the paired difference between the considered metric of R2R-AP and NA-AP is shown. The red line represents the median and the box goes from 25th to 75th percentiles (lower and upper quartiles), including 50% of the data. The red crosses are the outliers, and the whiskers mark the data in the 1.5 interquartile range with respect to lower and upper quartiles. For each metric, a linear model was computed for each of the 18 patients: The 18 linear models were then averaged (mean or median) to identify a trend in time, which is represented by the black solid line. In each considered control metric, the slopes of the trend in time were compared with respect to zero to verify whether positive or negative variations were achieved by R2R-AP. A positive slope was observed for time-in-tight-target (Fig. 3b, P < 0.001), whereas a negative slope was observed for time-in-hyper (Fig. 3c, P = 0.041). A mean slope of 0.313% per day was achieved in time-in-target (Fig. 3a, P = 0.059), whereas a mean slope of −0.019 mmol/l per day was observed for mean glucose (Fig. 3d, P = 0.481). Figure 4 shows the boxplot associated with the slopes' distributions of each considered metric difference. Distributions of mean glucose and time-in-hyper are negatively biased, whereas distributions of time-in-target and time-in-tight-target are positively biased.

Boxplots of the slopes' distributions associated to the trend in time of mean glucose [mmol/(L·day)], time-in-tight-target (%/day), time-in-target (%/day), and time-in-hyper (%/day). Each boxplot goes from 25th to 75th percentiles, and the red lines denote the medians. For each metric, the patient's slope is computed by fitting a linear model on the difference between R2R-AP and NA-AP. The P-value of the comparison of the slopes' distributions with respect to zero is also shown.
Discussion
The development of adaptive strategies that are aimed at improving glucose control of the currently available AP systems is a topic of major interest. To the best of our knowledge, this study is the first attempt to assess quantitatively whether and how much an R2R adaptation on top of a control algorithm can improve closed-loop glucose control in free-living conditions with respect to the same algorithm without adaptation. In particular, the major novelty is related to the specific adaptation mechanism tested in this trial, since the R2R strategy differs substantially from other approaches proposed in literature. 22 –25 In El-Khatib et al. 22 and Eren-Oruklu et al., 23 the control adaptation is obtained by updating online the model parameters at each sampling time (5 or 10 min); whereas in Zisser et al. 24 and Palerm et al., 25 the R2R strategies were based on few daily self-monitoring blood glucose measurements to adapt meal boluses in an SAP therapy. Differently, the proposed approach performs small daily changes of nocturnal basal (00:00–08:00) and daily CR (08:00–00:00) based on CGM measurements, so that each day both basal and CR are updated. Further, the proposed R2R-AP system is an early-stage prototype that was never tested in previous trials. As such, no direct comparison of this study should be done with other trials of the literature that were designed to assess the efficacy of AP prototypes in an advanced state of development and solidly tested earlier. 26 –30
Since a certain number of technical issues were expected, the study team interaction with the patients was neither reduced or prevented. However, the telemedicine system was only used for data collection purposes, and not for offering medical support. Indeed, no 24/24 h monitoring was in place, no automatic alert message was sent by the telemedicine system to the study team, and the clinical team never contacted the patients for medical reasons (such as hypoglycemia or hyperglycemia) based on telemedicine information.
The major improvement achieved by R2R-AP versus NA-AP was registered during the night (00:00–08:00), where time-in-target was significantly increased and time-in-hyper was significantly reduced without resulting in a significant increase of time-in-hypo (Table 3). The improved nocturnal glucose control resulted in a better glucose control at wake-up time (07:00–08:00), where time-in-target and time-in-tight-target were significantly increased with mean glucose and time-in-hyper was significantly reduced without increasing hypoglycemic episodes (Table 4). These improvements are particularly evident in Figure 1: Median glucose is lowered during the night by R2R-AP, and it is maintained within 3.9–7.8 mmol/L at wake-up time. The nocturnal results support the notion that an R2R-AP is safe and effective at further improving nighttime glycemic control versus NA-AP.
Collected data show that R2R-AP and NA-AP are performed similarly during the day (08:00–00:00), as shown in Table 5. Similar performance could be explained by the conservative policy that was implemented for safety reasons, which limited the number of successful updates in daily CR patterns. In fact, the CR update mechanism was designed under the assumption that a meal bolus was followed by at least 3 h of closed-loop control without other perturbations such as snacks or correction boluses, so that the control performance achieved in that period was a good indicator of CR efficacy. When tested in free-living conditions with no protocol restrictions, a number of unexpected events were faced by R2R-AP, thus impeding the update to happen. An exhaustive representation of the causes of missing CR updates is depicted in Figure 2 (right panel). In 35% of the cases, other meals/snacks occurred within <3 h from another meal, preventing both CRs from being updated. Moreover, the patient modified 26% of meal boluses suggested by the closed-loop algorithm. In all these cases, the conservative policy did not allow the execution of the adaptation. Although only 23% of diurnal CRs were successfully updated, a significant positive tendency to increase time-in-tight-target and to decrease time-in-hyper was observed by considering all the days and the entire month of the study, as shown in Figures 3b and 3c, respectively. Further, although the results were not significant, both time-in-target (Fig. 3a) and mean glucose (Fig. 3d) were improved during the entire month. Figure 2 (left panel) shows the causes of missing nocturnal (00:00–08:00) basal insulin updates. The manual user interventions were practically absent (2%), insufficient data were faced in 28% of cases, and the presence of meals was limited to 8%. Therefore, the nocturnal basal insulin was successfully updated by R2R-AP 62% of the times, resulting in a substantially improved nocturnal glucose control.
Finally, a natural question when dealing with adaptive algorithms is whether or not the algorithm converged to some “true/optimal” values of the parameters over the month. This question cannot be answered on real data: A “true/optimal” value is not known, but, and more importantly, it is unclear even whether the R2R algorithm should exhibit any sort of convergence or not. In fact, the adaptation mechanism is expected to follow the (unknown) variation of patients' insulin need over time, compensating for them, rather than converging to a constant value. In this article, we investigated whether the changes performed by the R2R algorithm were effective in improving the glucose control metrics. Algorithm convergence can only be assessed in silico, where the ground-truth is available, and this analysis was proposed for the R2R algorithm in Toffanin et al. 6
The limited number of participants and the reduced number of daily CR updates are the two major limitations of this study. Other limitations include the non-randomized design and the risk of a selection bias because the use of NA-AP and R2R-AP systems was proposed to subjects who had previously enrolled in another AP study. Further, since the study is not a randomized crossover one, we cannot statistically explore the potential impact of a learning effect. Nevertheless, the patients used the R2R-AP after 3 months of NA-AP use (2 month during the study reported in Kropff et al. 9 and one further month during the study reported in Renard et al. 8 ). Being already expert users of this technology, we can assume that the learning curve was completed. In support of this assumption, we note that the impact on glucose control of a potential learning effect should be expected during the day, when the patients are awake and interact with the system (the interactions are also reflected by the diurnal manual user interventions, which are equal to 26%). On the contrary, a significant improvement of glucose control occurred during the night (only 2% of manual user interventions).
Conclusion
To the best of our knowledge, this is the first article assessing glucose control achieved by an R2R-AP versus the NA-AP version of the same algorithm by considering the same group of patients (n = 18) in two 1-month single-arm clinical studies in free-living conditions. The aim of this study is to systematically analyze whether and to what extent adaptation is beneficial when used on top of closed-loop control. R2R-AP significantly improved the glucose control performance during the night. Moreover, even though daily CRs updates were limited by a conservative policy, an improvement of trends in time of the paired differences between R2R-AP and NA-AP is observed by considering all days of the study month.
Despite the acknowledged limitations, in particular the number of participants, the non-randomized crossover design, and the possible bias because of the inclusion of patients involved in previous AP studies, the proposed strategy tested in free-living conditions is a relevant proof-of-concept for future AP development. This outpatient study shows the potential advantages of an adaptive AP based on an R2R strategy that is designed to improve glucose control.
Future work will include longer testing of a less conservative version of the R2R update strategy that will likely increase the rate of successful updates in the presence of external disturbances and unexpected events.
Footnotes
Acknowledgments
The authors thank patients and their family members for their continued dedication during the extension study. They also thank Dexcom, Inc. and Roche Diabetes Care AG for providing research material support. This study was funded by the European Commission, Framework Program 7 (FP7-ICT-2009-4 grant number 247138). This work was also supported by the Ministero dell'Istruzione, Università e Ricerca (Italian Ministry of Education, Universities and Research) through the project “Learn4AP: Patient-Specific Models for an Adaptive, Fault-Tolerant Artificial Pancreas” (initiative “SIR: Scientific Independence of young Researchers”, project ID: RBSI14JYM2) and through the project “FORGETDIAB: Forget Diabetes: Adaptive Physiological Artificial Pancreas” (initiative “PRIN: Progetti di Ricerca di Interesse Nazionale”, project ID: 2015PJ28EP_001).
Role of the Funding Source
Neither the European Commission, which supported the study, nor Dexcom Inc. or Roche Diabetes Care AG, which provided research material support, had any influence on the trial design, analysis, or preparation of the article, nor had access to any of the trial data. C.T., J.K., J.P., L.M., M.M., R.V., and S.D.F. had access to the raw data. The corresponding author had full access to all of the data and the final responsibility to submit them for publication.
Contributors
All authors reviewed and provided edits and comments on article drafts. In addition, the authors had the following responsibilities: M.M.: development of the algorithm, data analysis, and drafting of the article; J.K.: main study physician responsible for the trial in Amsterdam; S.D.F.: senior engineer responsible for the trial in Padova and assisting the trial in Amsterdam, data analysis, and drafting the article; J.P.: senior engineer responsible for the trial in Montpellier; R.V.: engineer providing technical support during the trial in Padova; R.C.: engineer providing technical support during the trial in Padova and assisting the trial in Amsterdam; C.T.: development of the algorithm and data analysis; F.D.P.: control engineer responsible for control algorithm implementation on the DiAs; G.L.: computer scientist responsible for the design and implementation of the remote monitoring system used during the trial.; A.F.: main study physician responsible for the trial in Montpellier; F.B. and S.G.: clinicians providing medical support to the patients during the trial in Padova; A.A.: coordinating physician for the performance of the trial in Padova; P.K.-H.: chief engineer of the DiAs smartphone-based system and user interface; B.P.K.: principal investigator at UVA, development of the DiAs system; D.B.: main study physician in Padova, drafting of the article; L.M.: principal investigator of Pavia Unit, algorithm development, data analysis, and drafting of the article; J.H.D.: principal investigator in Amsterdam, design of the protocol, and drafting of the article; E.R.: principal investigator of Montpellier, drafting of the protocol and the article; C.C.: principal investigator in Padova, design of the protocol, data analysis, and drafting of the article.
Author Disclosure Statement
C.C., C.T., and L.M. hold patent applications related to the study control algorithms; C.C. has received research support from Sanofi-Aventis and Adocia. B.P.K. holds patent applications related to the study technology and has served as an advisor to Becton, Dickinson, and Company (BD) and Sanofi-Aventis and has received research support from Animas, Inc., BD, Dexcom, Insulet, Roche Diagnostics, Sanofi-Aventis, and Tandem Diabetes Care; stock ownership: TypeZero Technologies. E.R. is a consultant/advisor for Menarini Diagnostics, Abbott, Cellnovo, Dexcom, Eli-Lilly, Johnson & Johnson (Animas, LifeScan), Medtronic, Novo-Nordisk, Roche Diagnostics, and Sanofi-Aventis and has received research grant/material support from Abbott, Dexcom, Insulet, and Roche Diagnostics. J.H.D. is a consultant/advisor on the speakers' bureau for Dexcom, Johnson & Johnson (Animas, LifeScan), and Roche Diagnostics. P.K.-H. holds patent applications related to the study technology, serves as the CTO of TypeZero Technologies, and has stock ownership in TypeZero Technologies. No other potential conflicts of interest relevant to this article are reported.