
Abstract

ATTD 2016 Invited Speakers
DEVELOPING DISEASE-MODIFYING THERAPIES IN CHILDREN WITH TYPE 1 DIABETES
Type 1a (autoimmune) diabetes remains a tremendous burden both to individuals and society. Glycemic targets both in children (and adolescents especially) as well as adults are met only by a minority of patients. Changing the course of the disease by preventing or slowing down beta cell destruction rather than managing hyperglycemia would significantly impact the burden.
Studies aimed at both preventing the disease in at-risk pre-Type 1 subjects as well as intervening not only in new-onset cases, but also in established disease have been conducted over the past 30 years. Success has been limited.
Progress in our understanding of the genetics and natural history of the disease, incidence and prevalence, complications, quality of life, neurocognitive impact and response to therapy among others are critical to the design of disease modifying therapies.Clear data have emerged there are differences between adult-onset and pediatric-onset Type 1 disease.
Advances in our understanding of the natural history of Type 1 Diabetes throughout the lifespan have led to recent publications related to broader acceptance of a classification system for the presymptomatic stages of Type 1 diabetes and, importantly, more defined pathways for the development of disease modifying therapies in children.
CSII AND OTHER TECHNOLOGIES FOR PREVENTING BETA CELL FAILURE IN TYPE 2 DIABETES
The value and the utility of applying technology in the management of patients with poorly controlled insulin-treated type 2 diabetes (T2D) remain controversial. The OpT2mise randomized trial was designed to compare the effects of continuous subcutaneous insulin infusion (CSII) and multiple daily injection (MDI) on glucose profiles in patients with T2D. The results showed that CSII significantly improved selected glucometrics, compared with MDI, without increasing the risk of hypoglycemia. Another recent study looking at newly diagnosed T2D patients via the use of either CSII or CSII + sitagliptin therapy in controlling glucose variability and to prevent secondary complications of T2D showed that this treatment is superior to CSII monotherapy in terms of glucose variability. Oxidative stress is a detrimental feature of diabetes implicated in the progression of the disease and its complications. A study tested the hypothesis that improved glucose control, rather than insulin dose, is central to reduced oxidative stress in patients with T2D following CSII. CSII induces reduction of plasma ox-LDL in T2D patients as compared to patients on MDI suggesting that CSII may have an impact on factors associated with progression to complications. Finally, protection of beta cell function in T2D using CSII has been reported. Regarding glucose monitoring, recent studies utilizing self monitoring blood glucose (SMBG) as an integral component of diabetes care showed improvement in mean glucose, glycemic variability, metabolic risk factors, depression and diabetes-related distress, and health behaviors. The PRISMA study (Prospective, Randomized Trial on Intensive Self-Monitoring Blood Glucose Management Added Value in Noninsulin-Treated Type 2 Diabetes Mellitus Patients), to our knowledge the largest study of the effects of SMBG in patients with T2D, confirms the clinical usefulness and overall safety of using structured SMBG to provide guidance in the prescription of diabetes medications and lifestyle changes in non insulin-treated T2D. The effectiveness of continuous glucose monitoring (CGM) in the management of type 1 diabetic patients is well known. Differently in T2D its use is still a matter of debate because clinical trials in well-selected patient groups are lacking and less convincing evidence is available. Although many studies have evaluated glucose variability through different indices, MAGE, assessed by CGM, may be considered the best method to quantify glycaemic excursion. An improvement on glycaemic excursion in insulin-treated T2D patients by using RT-CGM has been reported, showing a significant reduction of the time spent in hypoglycaemic and hyperglycaemic ranges. Short-term intermittent use of RT-CGM appears effective in improving glycaemic control over a 12-week period without increasing the risk of hypoglycaemia. The effectiveness of RT-CGM is sustained during follow-up period compared with SMBG and without a greater intensification of medication over the course of the study. Larger clinical trials with longer follow-up are needed to evaluate not only the effectiveness of CGM in terms of improving glycaemic control but also the impact on quality of life and the adherence to the use of CGM as well as related cost issues. Even if it is too early to reach a general conclusion on the specific clinical indications, we believe that the RT-CGM can be used as a powerful motivational device to change patients lifestyle. We also suggest that short-term retrospective CGM use may be beneficial in certain clinical situations such as to detect nocturnal hypoglycaemia, to assist in the management of hypoglycaemia in T2D unawareness and when significant therapeutic changes are performed. In conclusion, modern technological devices including short message service reminder, online educational programs and clinician-patient electronic communication supporting coping and management are increasingly popular and represent very useful healthcare tools for T2D patients.
IS TYPE 1 DIABETES MELLITUS AN AUTOIMMUNE DISEASE?
Type 1 diabetes mellitus (T1DM) is considered to be an autoimmune disease based on genetic and clinical associations. Several of the most common associated genes including HLA, Insulin VNTR, CTLA4, AIRE, PTPN22, are immune regulators. Circulating islet and β-cell antibodies are hallmarks of autoimmunity present in ∼85% of patients considered T1DM.Yet more people harbor the same alleles and/or mutations without clinical diabetes. For example, inactivating mutations in the AIRE gene are responsible for APS1 in which Addison disease and hypoparathyroidism are common, yet T1DM is not. In APS2, Addison disease and Hashimoto thyroiditis accompany T1DM, yet co-existence of Addison with T1DM is rare. Markers of autoimmunity and various β cell Ab may exist for variable periods without clinical abnormalities. Autoimmune disease is more common in women, but the male: female of T1DM is equal. To initiate autoimmunity, an “environmental trigger” is proposed; to study genetics and autoimmune processes, the NOD mouse (female predominance of DM) has been extensively investigated. Whereas almost all immune regulatory approaches succeeded in the NOD mouse, almost 40 years of clinical trials with immune interventions failed to prevent, arrest, or reverse DM for extended periods. This dilemma has raised the question as to whether the β-cell is the “target of homicide”, i.e. autoimmune destruction by T cells, or has characteristics predisposing to its own demise as the “target of suicide”. This presentation discusses these competing narratives and proposes that self-destruct mechanism(s) explain the transitory success of modulating the autoimmune “cleanup” of a primary insult to the β-cells.
MULTI-CENTER RANDOMIZED CROSS-OVER ITALIAN PEDIATRIC SUMMER CAMP: AP VS SAP IN 5–9 YEAR OLD CHILDREN
Department of Information Engineering, University of Padova, Padova, Italy
Here we report the first outpatient AP trial in 5–8 year old children, using MMPC on DiAs in the PedArPan (PEDiatric ARtificial PANcreas) project.
Glucose control achieved in 3 days of AP use was compared against 3 days of parents-managed SAP.
The AP significantly reduced time-in-hypo with respect to SAP, 0.00%[0.00–2.22] vs 2.19%[0–12.3], p-value = 0.002, without significant worsening of time-in-target, 55.97%(22.53) vs 59.69% (21.24), p-value = 0.422, nor of time-in-tight-target (80–140 mg/dl), 31.27% (20.23) vs 33.02%(19.80), p-value = 0.668.
Overall (00:00–24:00)
A statistically significant 3-fold reduction of time-in-hypo, 1.93%[1.17–4.54] vs 6.67%[2.26–11.54], p-value <0.001, was recorded with the AP at the expenses of a statistically significant deterioration of time-in-target, 56.79%(13.47) vs 63.09%(10.98), p-value = 0.015.
Parents initiated manual interventions (via correction boluses or temporary basal rate settings) occurred 0[0-0] times with the AP vs 3.5[1–7] times in SAP. Closed-loop functioned for 96.97%[93.47-98.43] of the time.
In the summer of 2014, we initiated a two-phase long-term (6 months) trial evaluating at home a control-to-range closed-loop system – the wireless portable Diabetes Assistant (DiAs) developed at the University of Virginia. Phase 1 (1 month) recruited 30 patients with T1DM at 6 centers: the Universities of Virginia, Padova, Montpellier, Santa Barbara, Stanford University, and the Schneider Children's Medical Center of Israel. Phase 2 (5 months) continued with N = 14 patients at 5 sites; the study was coordinated by the Jaeb Center for Health Research.
Median subject characteristics: age = 45 years; duration of diabetes = 27 years; total daily insulin = 0.54 (U/kg/day); basal daily insulin = 0.22 (U/kg/day); 10/4 male/female.
HbA1c was reduced from 7.22% at the baseline to 7.03% (p = 0.25) at the end of the study. This was accompanied by a significant 3-fold reduction in the frequency of hypoglycemia from baseline to the last three months of CGM monitoring 4.1% vs. 1.3% (p < 0.001). Improvement in HbA1c was highly correlated with the percent time of system use, r = 0.59; in particular those with above-median system use (>70% of the time) achieved HbA1c reduction of 0.44%, from 7.19% at the baseline to 6.74% at the end of study.
We conclude that DiAs technology has matured enough, and is safe and effective for prolonged use at patient's homes. Excellent baseline glucose control (HbA1c) was preserved and further improved in the majority of patients. This was accompanied by a very significant reduction in the frequency and extent of hypoglycemia. Improvement in glucose control was tightly related to the degree of system use.
FLAT-SUGAR (GLYCEMIC VARIABILITY)
University of Washington, Seattle, USA
In short-duration diabetes, the DCCT and UKPDS have clearly shown that in glucose control defined as HbA1c can predict microvascular complications and longer term macrovascular disease. However, a closer look at the data suggests there is more than HbA1c, or mean glucose responsible for the complications of diabetes. The “glycemic variability (GV) hypothesis” notes that glucose fluctuation is at least one other etiologic factor. At a cellular level, GV has been shown to result in both reactive oxygen species accumulation and inflammatory activation. There are also several clinical trials suggesting GV is an important mechanism resulting in vascular complications. The problem is to date definitive data for the GV hypothesis is lacking. The study FLAT-SUGAR (FLuctuATion reduction with inSUlin and Glp-1 Added together) was designed as a feasibility study to prove it is possible to randomize two groups of patients while keeping HbA1c levels equivalent, yet show differences in GV. This was accomplished by using basal bolus insulin (BBI) in one group of “ACCORD-like” patients with type 2 diabetes and basal insulin with the GLP-1 RA exenatide (GLIPULIN) in the other group. The study was successful by showing similar HbA1c levels with more variability with the BBI therapy group. Many secondary endpoints were examined, and both ALT and SAA levels were shown to be lower with GLIPULIN. There was surprisingly little hypoglycemia and no severe hypoglycemia, so not surprisingly there were no differences between the groups in cardiac arrhythmias. FLAT-SUGAR was a successful study and we now feel it is possible to move forward to perform a definitive outcomes study to examine the role of GV in the complications of diabetes.
Pediatrics, University of Colorado Denver, USA
The majority of patients with T1D do not meet A1C goals established by major diabetes organizations. Hypoglycemia risks especially that of severe and a rising incidence of obesity along with associated morbidity in the T1D population limit intensification of insulin therapy in several cases. Noninsulin antihyperglycemic agents may enable T1D patients to achieve target A1C levels while using lower insulin dosages, which may reduce the risk of hypoglycemia. Several recently introduced antihyperglycemic classes hold promise as additional adjunctive therapy options that may help patients overcome barriers to optimal glucose control.
In the recent study from T1D Exchange participants, only 2% of adults reported taking pramlintide, the only agent approved by the U.S. Food and Drug Administration (FDA) for this purpose. The studies have reported significant improvement in A1c and weight loss with adjunctive pramlintide use. However most patients report significant upper GI side effects and increase in hypoglycemic episodes and thus limiting its use in clinical practice. Gradually increasing the dose of pramlintide may facilitate the use of this drug in T1D.
Studies of metformin have shown significant reductions in weight, insulin dose, and A1C, although in a meta-analysis, A1C reductions were not statistically significant.
Meanwhile, other older agents, such as colesevelam, a-glucosidase inhibitors, and thiazolidinediones (TZDs), have shown little or no promise in terms of glycemic control for patients with T1D.
In pilot studies, the SGLT2 inhibitor dapagliflozin and the GLP-1 receptor agonist liraglutide reduced blood glucose, weight, and insulin dose in patients with T1D. Phase 2 studies with the SGLT2 inhibitor empagliflozin and the dual SGLT1 and SGLT2 inhibitor sotagliflozin, which acts in the gut and the kidney, have demonstrated reductions in A1C, weight, and glucose variability without an increased incidence of hypoglycemia.
The sodium-glucose cotransporter (SGLT) inhibitors and the glucagon-like peptide 1 (GLP-1) receptor agonists may provide an effective approach to reducing some of the risks associated with intensive insulin therapy for T1D. Recent data on liragutide in T1D showed only modest effect and Novo-Nordisk has decided not to file with the FDA for its indication in T1D. Recent reports on DKA with SGLT 2 inhibitors and the FDA warning have cautioned the use of such medications in T1D. The drugs having combo SGLT 1&2 inhibitor effects may eliminate the DKA risk but are being currently evaluated. The role of many of these medications will be discussed during my talk.
London, United Kingdom
The International Diabetes Federation predicts that the fastest rise in prevalence of type 2 diabetes over the next decade will be in its African region. Although current rates of type 2 diabetes are relatively low in sub-Saharan African countries, people of African origin living abroad have significantly higher rates of diabetes than people of white ethnicity in the same environment. In on study in North East London, England, rates of diabetes were as high in the black communities as in the South Asians. In a recent study in South London, where approximately 20% of local residents are of black ethnicity, about 40% of people with new onset diabetes came from that group. They were younger at diagnosis and had higher HbA1c. By two years, HbA1c was not different between groups, but people of Black West African and Caribbean background were prescribed more medication to achieve this. Till now, relative cardio-protection has been noted in Black people with diabetes, associated with differences in lipid profile, but newer studies from the US suggest that this has changed. A greater prevalence of hypertension is thought to be associated with an observed higher risk of stroke. There is also a higher risk of atypical ketosis prone diabetes.
Differences in metabolic phenotype should help us tailor therapeutic and preventive interventions so it is important to understand them. There is evidence for hyperinsulinaemia in young people at high risk for diabetes in the black populations but the mechanisms of this are not fully understood. Whether early hyperinsulinism drives earlier diabetes through earlier beta cell exhaustion is also not proven. Studies are on-going to clarify the role of insulin resistance/sensitivity, both for carbohydrate and fat metabolism, and intra-organ fat deposition in the ethnic differences in metabolic phenotype. It is expected that such studies will underpin more focussed interventions to reduce the burden of type 2 diabetes in this high risk population.
Genetics and Epidemiology Section, Harvard Medical School, Joslin Diabetes Centerl
Nephrologe, Diabetologe, Hypertensiologe Ärztlicher Direktor Chefarzt Innere Medizin – Nephrologie Vivantes Klinikum im Friedrichshain Landsberger Allee 49 10249 Berlin
With the expiry of patent protection for several originator insulin analogue molecules, the availability of biosimilar insulin analogues will increase in the future. Current EMA guidelines for the approval of biosimilar insulin analogues specifically address the requirements for demonstration of comparability in structure, pharmacokinetics and pharmacodynamics, efficacy, safety, and immunogenicity of the active ingredient as well as the final formulated biosimilar product. However, insulin application devices are not addressed in these guidelines, although these devices, be it a pre-filled syringe, pen, or pump, are of particular importance for dosing accuracy and reproducibility as well as long-term patient compliance and adherence. Since the combinations of insulin and device may differ widely in their dosing characteristics, it cannot be assumed that an insulin biosimilar will be compatible with an existing administration device. In general, the EMA Medical Devices Directive (MDD) applies to all general medical devices. As a minimum requirement for an insulin biosimilar it is plausible that the device through which a biosimilar is administered must at least be able to match the reference medicine's device for convenience and comfort. Inferior usability could reduce treatment adherence and product uptake by the patients. On the other hand, current guidelines for biosimilars may be interpreted as to leave freedom to improve on the reference product's delivery devices. Therefore the design and user experience of the delivery device may serve as a key market differentiator to the reference or competing products even if they are clinically equivalent.
Saldanha and Santamore Pharma Consultants, Private Practice, Bel Air, USA
Much of the developing world has seen a significant rise in the treatment of diabetes primarily due to increasing awareness, which has led to larger rates of diagnosis and more willingness to seek treatment. Access to insulin is therefore more important than ever. The three major insulin manufacturers continue to dominate the landscape despite the availability of biosimilars in many countries. The market share they enjoy is similar to the more developed world. Many parties play a role in the acceptance and use of biosimilar insulins, from the respective Ministries of Health who approve the products and often provide them free of charge to patients, to the health care providers, and the ultimate consumers.
There are several factors that have contributed towards this situation. Barriers to entry and sustainability in the insulin business are significant. Pharmaceutical companies use a different business model and market segmentation when it comes to insulins in the developing world. Some of the factors that will be addressed include intellectual property, financial, clinical/regulatory, pricing, distribution, local partnerships and local manufacturing.
Some 15 years after its introduction in clinical practice, Continuous Glucose Monitoring (CGM) has become an established modality for diabetes treatment. There is sound evidence that patients can lower their HbA1c when using this technology, and spend less time in hypoglycaemia. Emerging evidence supports the notion that CGM can decrease the incidence of severe hypoglycemia, although the evidence for this indication is less abundant and has been criticized. The added value of CGM during pregnancy is unclear, but larger trials are under way. All this evidence has translated into a wide range of reimbursement status in various countries. In many countries reimbursement is still on a case-by-case basis. In those countries where there are formal reimbursement criteria, the interpretation and translation of the evidence base varies. An overview of the evidence supporting the use of CGM and its reimbursement will be given.
A BREAKTHROUGH IN GERMANY?
Research Instiute Diabetes FIDAM, Bad Mergentheim, Germany
In Germany, the Federal Joint Committee (G-BA) is responsible for legally binding decisions regarding the reimbursement of medical procedures (e.g., drugs, non-drug interventions, medical devices, etc.). Since 2004, the German Institute for Quality and Efficiency in Health Care (IQWiG) assesses the advantages and disadvantages of medical procedures on behalf of the G-BA. The IQWiG uses methods of evidence-based medicine for conducting systematic searches for studies which provide sufficiently reliable results, and for selecting and assessing those studies. Based on this research IQWiG produces evidence-based reports. IQWiG reports usually have a large impact on reimbursement decisions made by the Federal Joint Committee.
In May 2015, the IQWiG released a report about potential benefits of “continuous interstitial glucose monitoring (CGM) with real-time measurement devices in insulin-dependent diabetes mellitus”. The IQWiG included a total of 15 studies. The IQWiG report concluded that while there was evidence that CGM is beneficial with regard to HbA1c improvement in adults with type 1 diabetes, there was less clear evidence for the avoidance of severe hypoglycemia in this patient group. Furthermore, the IQWiG found an indication that CGM might be beneficial with regard to hypoglycemia avoidance and HbA1c improvement in children with type 1 diabetes.
Given the rather positive conclusion of the IQWIG report regarding the advantages of CGM there is a guarded optimism in Germany that reimbursement of decision will significantly improve. But the final assessment by the Federal Joint Committee regarding reimbursement of CGM use is still pending. In this presentation an overview about key results of the IQWIG Report will be presented along with the current development of the reimbursement situation of CGM in Germany.
Continuous glucose monitoring (CGM) is currently not funded routinely in the UK. The National Institute for Health and Care Excellence (NICE) has previously published technology appraisals (TA) for insulin pump therapy, but has not carried out a TA for CGM. Commissioners have a legal mandate to fund NICE TA recommendations, but not other NICE recommendations. NICE are due to publish a diagnostic assessment review of integrated sensor augmented pump systems in early 2016 but it is unlikely to have a significant impact on funding of these technologies. In August 2015 NICE published updated clinical guidelines for the management of children and young people with diabetes (NG18), and adults with type 1 diabetes (NG17). In NG18 NICE advised that children and young people with hypoglycaemic problems should be offered CGM, which is the strongest form of recommendation. In NG17 the advice was that CGM should be considered for adults with hypoglycaemic problems, a weaker recommendation. NICE performed a number of health economic analyses to define the cost-effectiveness of CGM for optimising control in those with an elevated HbA1c. Following these analyses it was recommended that CGM be considered if HbA1c >75 mmol/mol [9%] despite testing at least 10 times a day, and continued only if HbA1c can be sustained at or below 53 mmol/mol (7%) and/or there has been a fall in HbA1c of 27 mmol/mol (2.5%) or more. This guidance will form the basis for ongoing discussions about funding CGM for small groups of patients with type 1 diabetes.
WILL MEDICARE DELIVER?
Dexcom, Global Access, San Diego, USA
Medicare is the largest insurance program in the US, with over 50,000,000 beneficiaries; it is intended for people over the age of 65 or are disabled.
Despite the recognized clinical benefits, and the fact that nearly all commercial payors in the US have positive coverage policies for Type 1 patients and CGM, the fact that Medicare does not have provide coverage is perplexing. The coverage process is dictated by Federal Law, and is therefore bound by statute, and to a certain degree by interpretation by the Centers for Medicaid and Medicare Services (CMS), who administers the program.
All real time CGM devices available in the US require SMBG confirmation according to FDA labeling. CMS has determined that CGM devices do not meet the statutory definition of “durable medical equipment benefit category” and has labeled real time CGM a “precautionary” device since it requires SMBG confirmation. Thus, without a “benefit category” determination, CGM cannot be considered for coverage.
There are multiple efforts to resolve this Medicare issue for CGM:
1. Congressional legislation that will create a new benefit category and mandate coverage for CGM.
2. Individual Medicare beneficiaries that are appealing their denials thru the judicial process.
3. Manufacturers may independently pursue administrative action or non-adjunctive status.
The efforts to get Medicare coverage, the role of large national stakeholders/coalitions and expected timelines will be reviewed in this presentation. Data supporting the clinical value of CGM in the elderly population will also be reviewed.
Checking blood glucose levels on a daily basis is one of the landmarks for diabetes care. The use of real time continuous glucose monitoring (CGM) has been widely available for use by people with type 1 diabetes for more than 10 years. Because of imprecision of historical models and resulting safety concerns, CGM system to date is approved for use adjunctive to SMBG in patients with type 1 diabetes.
Newest products have shown a great improvement in accuracy and portability. When used on near-daily basis they are associated with lower HbA1c, a greater percentage of blood glucose values in the target range, and reduced time spent in hypoglycemia if compared with those who use traditional self-monitoring blood glucose (SMBG). Nevertheless, recent studies on large clinical databases have shown that only a small proportion of children and adolescents are using CGM in clinical practice, either if they are treated with multiple daily injections or insulin pumps.
Relatively few studies considered the use of CGM in subjects treated with Multiple Daily Injections (MDI), mainly in children and adolescents. Moreover little evidence about the impact of CGM on Health-Related Quality of Life (HRQOL) and treatment satisfaction of children with type 1 diabetes treated with MDI and their parents exists. New studies are needed to investigate if in the future CGM can replace SMBG in children and adolescents treated with MDI.
NIGHTSCOUT EXPERIENCE IN ITALIAN CHILDREN WITH TYPE 1 DIABETES
ospedale san raffaele, pediatric diabetology, milano, Italy
Menstual cyclicity, sleep efficiency and unplanned physical activity: glycemic response in women suffering from T1DM.
Scientific evidences available in literature regarding the correlation between female menstrual cycle, sleep quality and glycemic response are heterogeneous.
Our study aim is to point out further correlations between the variables mentioned in a sample of type 1 diabetic patients, in order to find which ones deserve further investigations to become clinically relevant.
10 T1DM women followed up at the A.O.U. Città della Salute e della Scienza or the A.O. Ordine Mauriziano in Turin, in CSII or MDI therapy, were recruited.
RT-CGM data, activity and sleep tracker (iHealth®) to monitor unplanned PA and sleep were collected
To establish ovulation, a digital test was used in order to notice the urinary LH peak.
During the 120 days continuous evaluation, we analyzed: glucose values, Insulin intake, SE, nocturnal awakenings, Steps/day, PSQI test (Pittsburg Sleep Quality Index).
In the studied population, we confirm: Increase of MBG in early luteal phase (ELP) or periovulatory phase (PP), Increase of GV in ELP or PP, Increased number of hypoglycemic episodes (<70 mg/dl) in early or late follicular phase and increased number of hyperglycemic episodes (>180 mg/dl) in early luteal phase, Not significant variations of II, Minimal variations regarding insulin intake, No significant intra-individual variations in SE throughout the menstrual cycle, Coherent results in a compared valuation of PSQI scores and SE, decrease of the number of steps/day in PP and luteal phase.
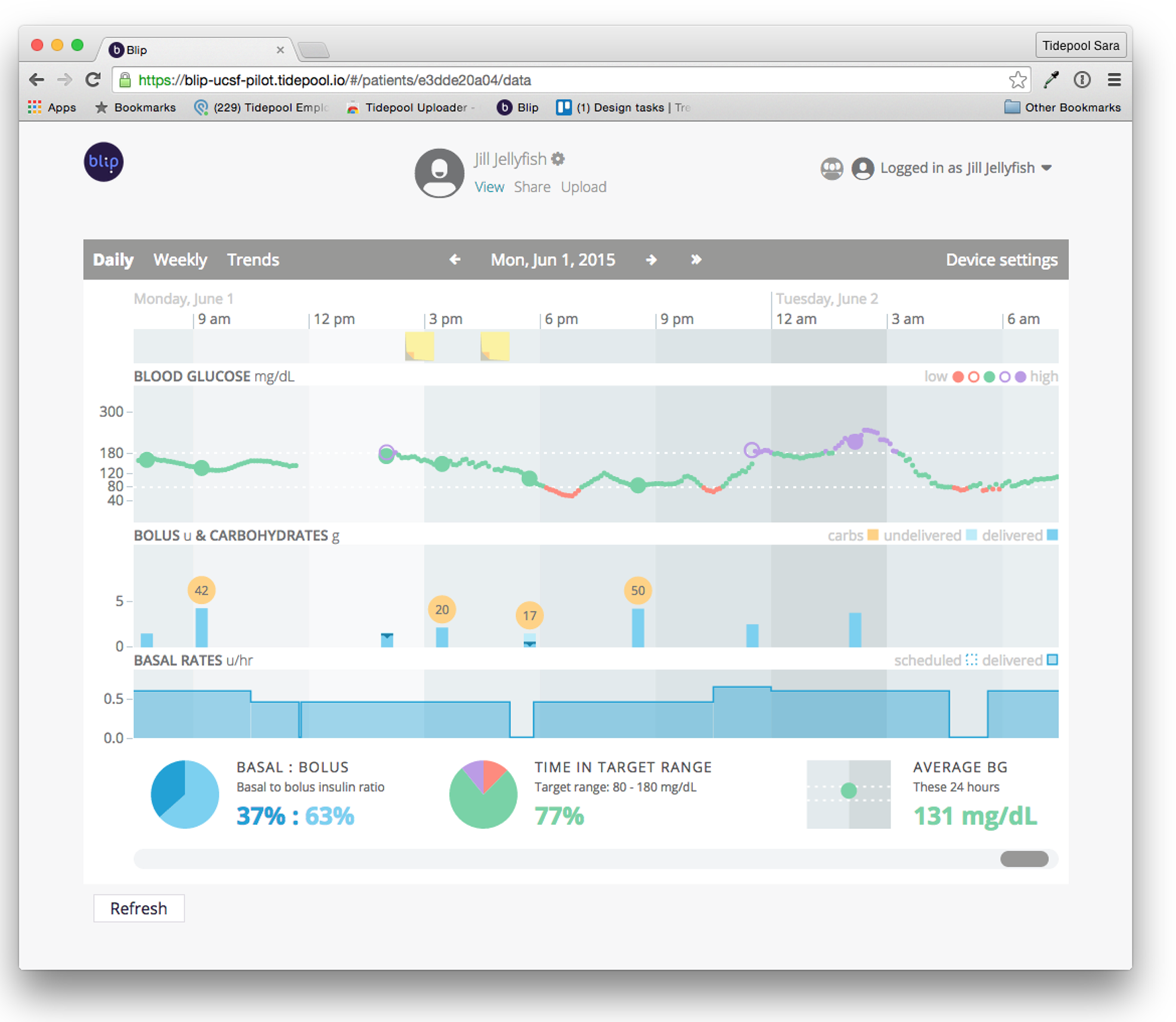
TIDEPOOL: AN OPEN SOURCE, EXTENSIBLE PLATFORM FOR DIABETES MANAGEMENT AND RESEARCH
Tidepool, Corporate Research and Development, Palo Alto, USA
Tidepool is a non-profit, open source organization building a platform and applications for patients, providers and researchers. Founded as a Silicon Valley startup, Tidepool's mission is to deliver technology that helps reduce the burden of managing Type 1 diabetes.
Tidepool has built a modern, extensible software platform that is freely available in source code form. The secure Tidepool Platform exposes modern application programming interfaces, enabling application developers, researchers and device makers to build custom application that take advantage of diabetes device data.
Tidepool has also built applications that leverage the Tidepool Platform. The Tidepool Uploader is a Chrome extension that enables uploading of data from blood glucose meters, continuous glucose monitors and insulin pumps via Mac or PC to the Tidepool cloud. Blip is a web-based application that integrates data from many different diabetes and fitness devices and presents it in intuitive, actionable form. Blip Notes is a companion mobile application that allows users to enter life context relevant to their diabetes therapy. Nutshell is a mobile application that keeps track of meal and exercise events and enables contextual recall and therapy optimization.
Tidepool uses “lean startup” and agile software development methodologies. Tidepool engages early and often with many end users, iterating quickly through functionality and user experience concepts with the goal of achieving the most usable and intuitive designs. Tidepool has built a regulatory quality system that leverages modern software development practices while meeting regulatory requirements.
What is the real interest for patients of “digital advisors” downloaded to smartphones in the form of “apps” or already incorporated in certain glucose meters or insulin pumps?
Diabetic patients currently have access to over 1 100 Apps, both free and paid; in most cases, these apps are not required to meet any quality criteria since they are not in fact declared as “medical mobile apps”. They vary greatly in terms of type and quality, and very few have so far been evaluated. The majority of these apps provide patients with support and/or advice functions. They collate certain data (capillary BG values, insulin doses, physical activity and levels of carbohydrates currently being consumed) and present them in legible fashion in the form of an electronic notebook. In addition, some apps allow sharing of this data with HCPs, either in real time, or subsequently, and allow feed-back to be received from the latter (usually via text message or automatic reminders). The aim of this first class of apps is to assist patients with their day-to-day choices but without necessarily seeking to impact glycaemic control.
The second class of apps, to which are attached more expectations but also more concerns, proposes adjustment of treatment and thus of insulin doses in particular. Most of these higher-risk apps, which must comply with the FDA definition of “medical devices”, currently provide no protection against - and may in fact actively contribute to - incorrect or inappropriate dose recommendations. In all, only 20 or so such downloadable “digital advisors” have undergone robust evaluation and have for the most part demonstrated significant impact on the primary endpoint. Among these systems, those enabling interaction between patient and HCP appear the most effective. Of the dozen or so systems targeting HbA1c, 8 showed a significant improvement of close to 1% vs. controls. These studies were nevertheless marked by considerable drop-out rates and there is currently little information available on the continued use of these advisors beyond completion of the evaluation phase. One of the most sophisticated of these systems is the Diabéo system, which has already demonstrated a 0.9% reduction in HbA1c at 6 months in DT1 patients with chronic imbalance and is currently undergoing clinical study with medico-economic evaluation over 2 years in 700 patients on MDI or insulin pump.
Bolus calculators incorporating medical devices, and which may also be classified as “digital advisors”, are required to meet quality criteria imposed in this sector by the regulatory authorities. Such bolus calculators have already demonstrated their value in compliance with both standard insulin treatment and pump therapy, particularly in patients with poor numeracy skills, and appear to have a favourable effect on glycaemic control.
This new category of “digital advisor” apps in the widest sense may, subject to robust clinical evaluation, prove extremely useful in diabetes management.
BEYOND THE ARTIFICIAL PANCREAS: TRANSLATING CLOSED-LOOP TECHNOLOGY INTO ADVISORY SYSTEMS AND CLOUD ANALYTICS
With research groups around world reporting encouraging results in outpatient clinical trials, the technical feasibility of the Artificial Pancreas (AP) is now firmly established. In the process, the research community has validated a number of key models and component technologies, including mathematical/simulation models of human physiology and sensors and drug delivery devices that facilitate automated signal processing, both leading to broadly applicable procedures for real-time and retrospective estimation of the patient's metabolic state. Indeed, the stage is now set to positively impact the lives of patients in the form of “decision support” technologies that make the best possible use of available data and are agnostic to the mode of insulin delivery. Examples include: (i) smart bolus/treatment wizards, including treatment advice in response to acknowledged physical activity, informed by continuous state estimation and real-time assessment of insulin sensitivity, (ii) meal and exercise detection algorithms that provide cues to the patient to consider treatment options, (iii) fault detection algorithms that increase patient situational awareness, (iv) risk profiling and stratification procedures that provide insights into patterns of hyper- and hypoglycemia in relation to self-treatment behavior and activities of daily living, and even (v) algorithms for individualized treatment optimization based on retrospective analysis of patient data in the cloud. This talk will argue that AP and decision support research activities are highly synergistic, highlighting recent technology developments at the University of Virginia (UVA) and featuring preliminary results from an ongoing feasibility trial with decision support components implemented atop the UVA Diabetes Assistant (DiAs) platform.
EXERCISE AND THE ARTIFICIAL PANCREAS: IS IT THE MOST DIFFICULT “HURDLE”?
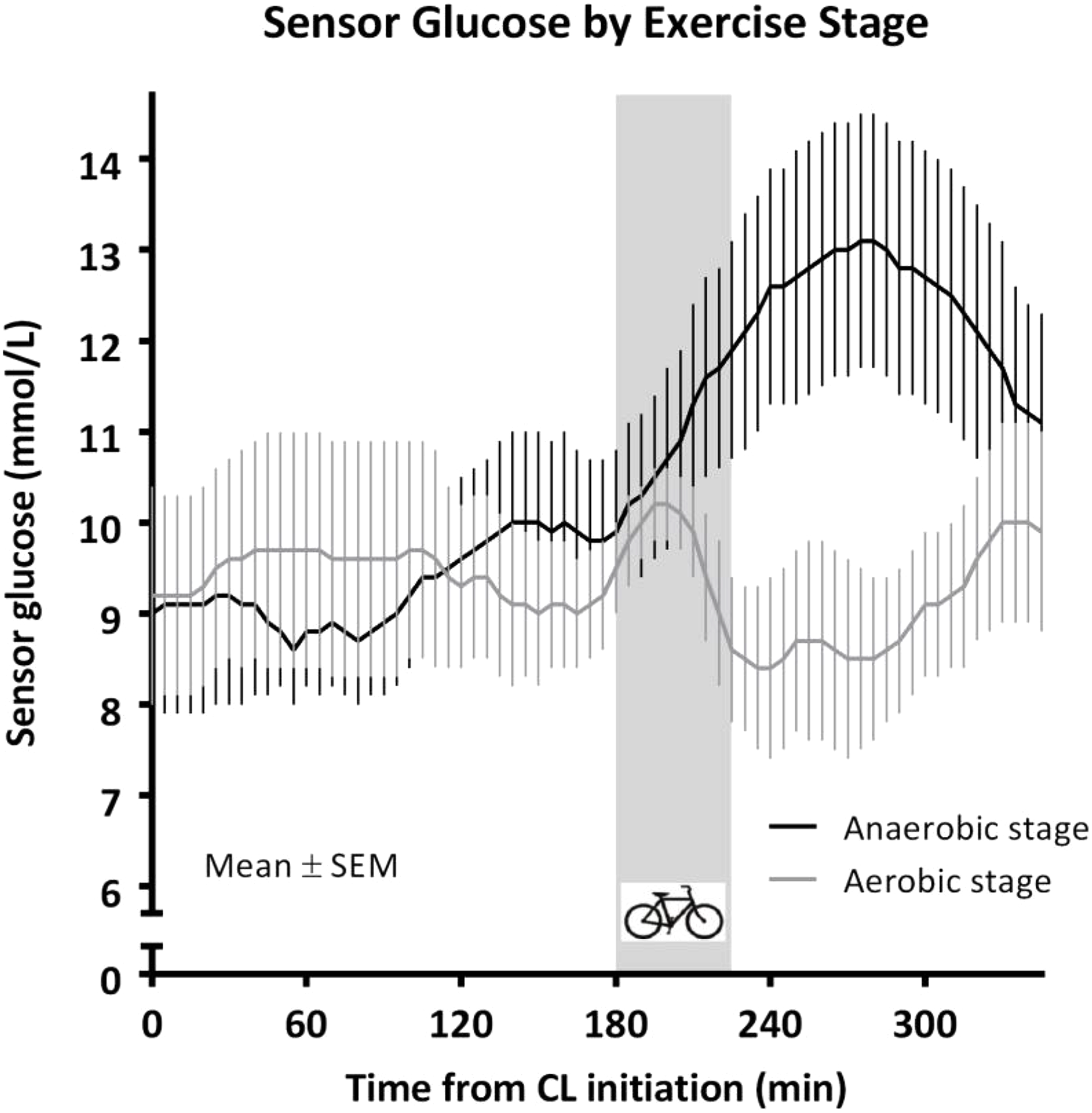
Exercise promotes health in people with diabetes; however, it can complicate blood glucose control. Factors affecting blood glucose fluctuations include exercise type, intensity and duration of the activity as well as the amount of insulin and food in the body when the exercise is performed. This lecture will discuss the main regulators of the blood glucose responses to different types of exercise in health and diabetes and highlight some of the main “hurdles” that exercise will pose for the development of the artificial pancreas.
AUXILIARY SIGNALS FOR THE CONTROL OF PHYSICAL ACTIVITY
UVA, Center for Diabete Technology, Charlottesville, USA
People with type 1 diabetes (T1D) are at continual risk for hypoglycemia, which is recognized as one of the principal impediments to optimal glycemic control. Physical activity in T1D has been associated with many health benefits such as reduced cardiovascular risks and improved psychological well-being, but also leads to imbalance between hepatic glucose production and muscle glucose disposal, increased insulin sensitivity and impaired counterregulatory response. As a probable consequence most adult with T1D partake in less PA than their non-diabetic counterparts.
Automated closed-loop control (CLC) could be a very significant tool in improving this situation; and CLC systems have been tested against a variety of glycemic disturbances with few proving as challenging as exercise: e.g. in a multisite study (adolescents and adults), we showed a 3 fold reduction of hypoglycemia overall and up to 6 fold post exercise and during the night afterwards, but no change during exercise. Using heart rate and accelerometers to inform the CLC system we showed a significantly reduced glycemic drop during exercise (adolescents and adults, inpatient and outpatient). Furthermore, analysis of this data allowed the development of mathematical models capable of predicting exercise induced glucose drop using recent history, leading to exercise advisory systems.
In conclusion, the advent of easy to use, cheap, devices capable of tracking physical activity, and the emergence of smart phone based medical devices to combine these signals with glucose and insulin records, are likely to enable patient specific automated and advisory systems dedicated to enabling safe exercise in T1D.
Elevated postprandial blood glucose levels constitute a global epidemic and a major risk factor for prediabetes and type-II diabetes, but existing dietary methods for controlling them have limited efficacy. Here, we continuously monitored week-long glucose levels in a 800-person cohort, measured responses to 46,898 meals, and found high variability in the response to identical meals, suggesting that universal dietary recommendations may have limited utility. We devised a machine-learning algorithm that integrates blood parameters, dietary habits, anthropometrics, physical activity, and gut microbiota measured in this cohort and showed that it accurately predicts personalized postprandial glycemic response to real-life meals. We validated these predictions in an independent 100-person cohort. Finally, a blinded randomized controlled dietary intervention based on this algorithm resulted in significantly lower postprandial responses and consistent alterations to gut microbiota configuration. Together, our results suggest that personalized diets may successfully modify elevated postprandial blood glucose and its metabolic consequences.
WHAT APPS CAN DO TO SUPPORT CARBS COUNTING?
Smartphone applications (apps) are widely available, increasingly used by patients and clinicians, and have the potential to improve diabetes care and self-management. Diabetes apps can facilitate self-monitoring by tracking and logging health information and reporting graphs and statistics based on patient input. The main nutrition features are food journals and databases of food composition, including information from restaurants and fast food chains and barcode scanners. The potential benefit of these apps is their ability to help people with diabetes to evaluate the amount of carbohydrates in the food they consume (carb counting).
Carb counting is crucial for diabetes management, particularly when using rapid-acting insulin, as the dose depends on the amount of carbohydrates consumed in a meal. Yet, accuracy in carb counting is not necessarily sufficient to determine the correct dose of insulin, as other factors influence the postprandial blood level, including glycemic load, dietary fiber, fat and/or protein content and personal glycemic index. Few apps address adjustment of insulin doses according to personal past experience or crowd wisdom instead of carb counting alone. Several of the carb counting and insulin bolus calculation apps provide no protection against, and may actively contribute to, incorrect or inappropriate dose recommendations that place patients at risk of hypoglycemia/hyperglycemia.
The Diabetes team should exercise caution in recommending unregulated insulin dose calculators to patients and address app safety as part of self-management education. The prevalence of errors attributable to incorrect estimation of carbs underlines the importance of clinical input during app design.
EPIDEMIOLOGY OF INSULIN PUMP THERAPY IN ITALY: THE IMITAS STUDIES
University of Padova, Department of Medicine- DIMED- Metabolic Diseases, Padova, Italy
University of Turin, Pediatrics, Turin, Italy
Luigi Sacco, Pediatrics, Milano, Italy
MiniMed 640G has a predictive algorythm (SmartGuard) that suspends insulin infusion when patient glucose levels are still in normal range to avoid reaching a pre-set low limit. MiniMed 640G safety and efficacy in adolescents with T1 diabetes was evaluated by analyzing CareLink data. Thirty-eight type 1 diabetes >6 months adolescents (14–20 years) on Minimed 640G, have been evaluated during a 5 days camp. Mean meter BGs, mean SGs, sensor SD, sensor MARD, % time spent in hypo (<70mg/dl), % time spent in hyper (>160mg/dl), episodes of moderate to severe hypo, episodes of hyper or DKA have been analyzed. SmartGuard has been disabled (SG-OFF) on the 2nd day from 9.30 am to 10 pm and the data have been compared with those of the 3rd day with SG-ON. The level of exercise and type of food intake was comparable between the 2 days.
During the 5 days patients carried out all activities without suffering episods of severe hypo or DKA. The average BG (Bayer Contour Next Link 2.4 meter) was 152.5 ± 25.3 mg/dl, while average SG was 147.7 ± 1.1 (Pearson = 0,75, MARD 9.2 ± 7.3%). Time spent in hypo was 0.4 ± 0.5%, while time in hyper was 17.0 ± 8.8%.
Thirty patients have turned SG off when requested and the comparison between the day SG-OFF vs day SG-ON showed comparable mean SG (149.7 ± 21.5 mg/dl vs 143.1 ± 18.0 mg/dl), while glucose variability (SD) was significantly lower with SG-ON (51.4 ± 11.9 vs 45.6 ± 10.1, p = 0.044).
No difference was observed regarding time spent in hypo (0.5 ± 0.9% vs 0.4 ± 0.4%), though with less events per day (1.9 ± 1.8 vs 1.3 ± 1.0, p = 0.084) and on average 5.0 ± 1.8 SG activations/patient/day occurred. Hyperglycemic events were 7.0 ± 3.4 vs 6.1 ± 3.3, whilst time spent in hyperglycemia was significantly reduced with SG-ON (19.2 ± 11.9% vs 13.5 ± 10.0%, p = 0.048).MiniMed 640G in adolescents with T1 diabetes was safe and effective. SmartGuard contributed to reduce both hypo events and time spent in hyper.
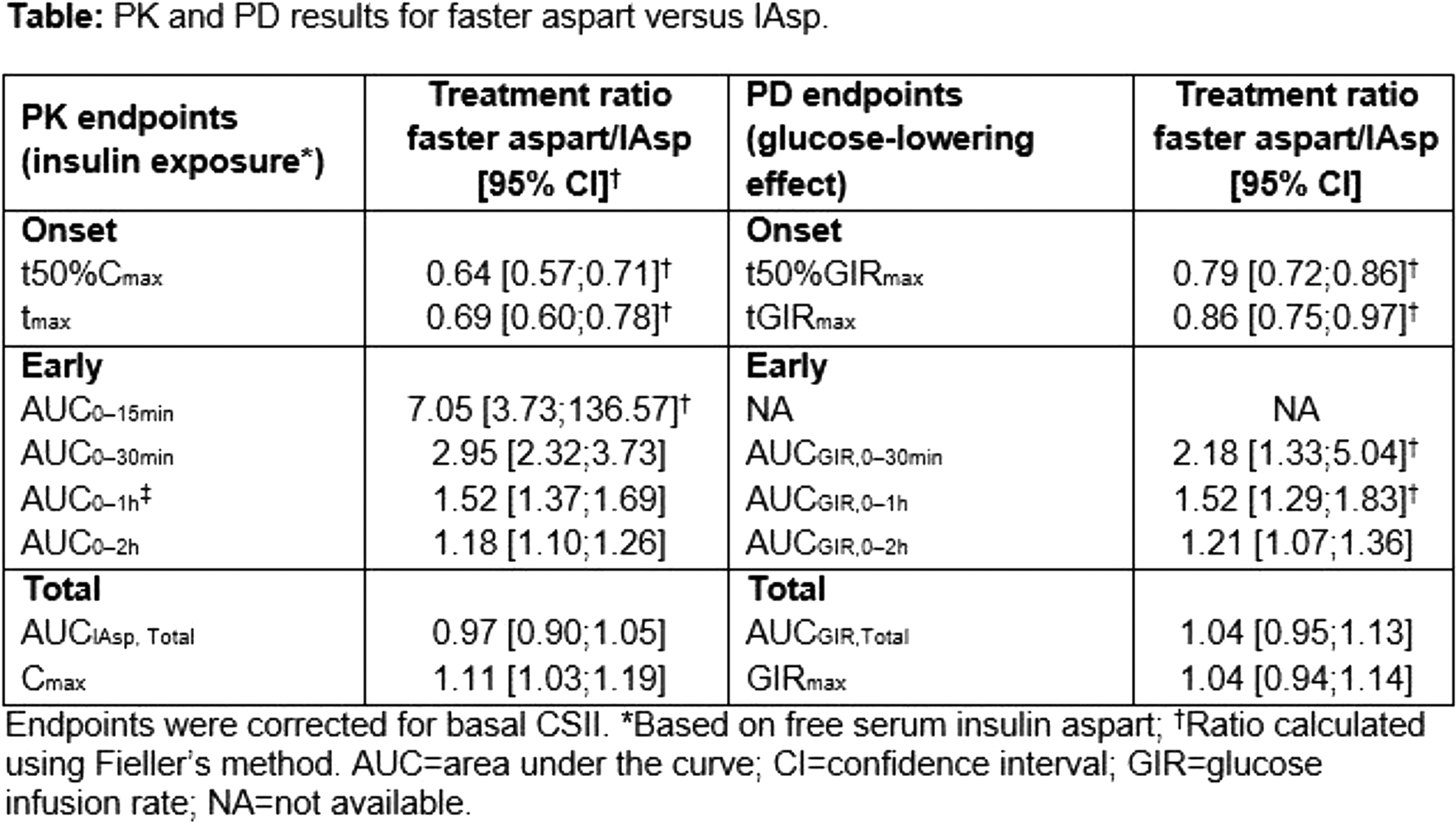
Shortening the time to peak action of fast-acting insulins may have advantages for prandial insulin coverage and may better allow postprandial insulin administration. For fast-acting insulin aspart (FiAsp, NovoNordisk) the well-characterized excipients nicotinamide and L-arginine (to stabilize the molecule) are added to the established rapid-acting insulin analog insulin aspart. The ultra-rapid effect of adding nicotinamide causes a more rapid monomer formation leading to a quick uptake into the blood stream. Studies indicated an approximately twice as fast onset of appearance in the bloodstream and 2fold higher early exposure within the first 30 minutes. We look forward to the full publication of the Phase 3 trials of this ultra-fast insulin insulin which is likely to be the first of its kind to be approved possibly as early as 2017. Also a citrate/zinc-ion chelator combination to human regular insulin employed by Biodel, Inc. showed ultra-rapid insulin properties. Issues regarding injection pain and stability of this compound are currently under investigation. Another approach to ultra-rapid mealtime insulin action is BioChaperone® Lispro, an ultra-rapid formulation of insulin lispro. BioChaperone® is a library of polysaccherides mimicking the properties of heparin. This insulin is developed in cooperation between Lilly and Adocia and is reported to have a 30 per cent earlier onset of action and a 69 per cent stronger early metabolic effect. Thus, ultra-fast acting insulins may not only been considered for use in closed-loop approaches and pump therapy but may have therapeutic advantages in the prandial insulin treatment type 1 and type 2 diabetes.
WEAK POINTS IN CLOSED-LOOP TECHNOLOGY: FAULT DETECTION AND MITIGATION
University of Colorado Denver, Barbara Davis Center for Childhood Diabetes, Aurora, USA
Current closed-loop technology combines an insulin pump, continuous glucose monitor (CGM), and an algorithm to dose insulin. Numerous weak points in the system exist. Detection and mitigation of these faults will improve the safety of artificial pancreas systems and benefit current open-loop systems.
A 4 week multicenter outpatient trial was performed in 40 patients with type 1 diabetes (age = 29 ± 8 years, 43% male, A1c = 7.3 ± 0.8%). Specific investigations targeted: 1) the effect of acetaminophen on CGM sensor glucose compared to blood glucose meter values; 2) the effect of lipohypertrophy on infusion set duration and failure, CGM sensor performance, and glucose values; 3) the effect of hyaluronidase on glucose values and infusion set failure; 4) development of algorithms to detect infusion site and CGM sensor failures in advance of hyperglycemia and DKA.
As expected, acetaminophen falsely elevated CGM sensor glucose values with implications for insulin dosing in open or closed-loop. Unexpectedly, the median ARD for CGM sensor glucose values was improved in lipohypertrophy compared to normal tissue. Hyaluronidase did not effect the duration of infusion sets, average daily glucose, or total daily insulin, however postprandial glucose levels were improved for a day after hyaluronidase infusion.
From the data generated on infusion set and sensor failures, fault detection algorithms were developed which are now being tested in real-time closed-loop studies with the goal of making open and closed-loop technology safer. More research is needed to improve the safety and performance of diabetes technology to enhance glucose control and reduce the burden for people with diabetes.
A significant challenge in the design of algorithms for the artificial pancreas is overcoming the latencies introduced by measuring glucose subcutaneously and by delivering insulin subcutaneously. These are artificial delays introduced by an external device and limit the ability of an engineered design to emulate the behavior of the natural pancreas endogenous glucose regulation including first phase insulin secretion and proximity to the portal circulatory system. These limitations are particularly challenging when one attempts to compensate for unmeasured disturbances, such as unannounced meals. In this talk, I will discuss some of the closed-loop performance measures that are impacted by delays in the feedback loop, and will review clinical work conducted in our group to address those limitations, including inhalable insulin and IP delivery of insulin. I will also introduce some of our latest work on the design of a fully implantable version of the artificial pancreas.
COMPOSITE MEASURES OF GLYCEMIC CONTROL
HbA1c is not a sufficient measure of response to therapy. One must consider other factors, especially risk of hypoglycemia and weight gain. HbA1c provides a measure of average blood glucose over the preceding 3 months, subject to inter-individual variability due to erythrocyte lifetime, hemoglobinopathies and the Hemoglobin Glycation Index. DCCT established relationships between HbA1c, risk of hypoglycemia, and risk of complications in T1DM. Based on these relationships, the present author proposed to use this relationship between risk of hypoglycemia and HbA1c to evaluate alternative forms of therapy, physicians, clinics and other interventions (1). This curvilinear relationship has subsequently been utilized by others to demonstrate superiority of glargine and detemir relative to NPH (2), and separately, superiority of other therapies (degludec, hyaluronidase pretreatment of insulin infusion sites) compared to controls. Superiority should be tested by evaluating non-identity of the relationships between risk of hypoglycemia and HbA1c for different forms of therapy, rather than by testing either HbA1c or risk of hypoglycemia alone (1,2).
I recently proposed several additional methods for simultaneous analysis of hypoglycemia and mean glucose or HbA1c: 1) Risk of Hypoglycemia vs HbA1c or change in HbA1c following intervention (1); 2) relationship between %Hyperglycemia and % Hypoglycemia (3); 3) variations of the foregoing approach, using %Time in Range combined with %Time in Hyperglycemia and/or %time in Hypoglycemia (3); 4) Relationship between ‘Change in % Hyperglycemia’ vs ‘Change in %Hypoglycemia’ (3); 5) A triangular graph showing %Hyperglycemia, % Hypoglycemia, and % Target Range simultaneously (3); 6) Display of hyper- vs. hypoglycemia (using High Blood Glucose Index (HBGI) (4), GRADE
One can avoid the need for an arbitrary choice of threshold for hypoglycemia by repeating the analyses with multiple thresholds (e.g. 40 to 80 mg/dL) and evaluating robustness of findings. A threshold of 80 mg/dL can be used as a surrogate for the much less frequent occurrence of hypoglycemia at 50 mg/dL; a threshold of 180 mg/dL can be used as a surrogate for hyperglycemia at a much higher threshold, e.g. 250 mg/dL (9). Alternatively, one can use penalty scores such as BGRI, GRADE or IGC (4–7).
Vigersky has proposed a composite analysis of HbA1c, risk of hypoglycemia and weight gain (10) and clearly elucidated the need to go beyond HbA1c. Thomas et al. proposed composite markers combining information from HbA1c, overall glycemic variability, and hyperglycemia (11–12). Augstein et al (13) proposed a Q-Score which adds measures of hypoglycemia, within-day, and between day variability (13). Augstein combined parameters using z-scores (13), an approach closely related to use of percentile scores (3,8). An Index of Glycemic Variability (IGV) has been proposed to combine results from several types of variability (total variability, within-, and between-day variability, and variability between daily means) using a weighted average of percentile scores (8).
Conclusion: Regulatory agencies should utilize multiple criteria to simultaneously evaluate safety and efficacy of therapeutic agents and devices (1–13).
1) Rodbard, D., Berger, M., and Pernick, N. Computer, networking, and information systems to facilitate delivery of health care to patients with diabetes. In: Baba, S., and Kaneko, T. (Eds.), Diabetes 1994, Proceedings of the 15th International Diabetes Federation Congress, Kobe, 6 - 11 November 1994. Elsevier, Amsterdam, pp. 800–803, 1995.
2) Little S1, Shaw J, Home P. Hypoglycemia rates with basal insulin analogs. Diabetes Technol Ther. 2011 Jun;13 Suppl 1:S53–64. doi: 10.1089/dia.2011.0022.
3) Rodbard D. Evaluating quality of glycemic control: graphical displays of hypo- and hyperglycemia, time in target range, and mean glucose. J Diabetes Sci Technol. 2015 Jan; 9(1):56–62. doi: 10.1177/1932296814551046
4) Clarke W, Kovatchev B. Statistical tools to analyze continuous glucose monitor data. Diabetes Technol Ther. 2009 Jun; 11 Suppl 1:S45–54. doi: 10.1089/dia.2008.0138
5) Hill NR, Hindmarsh PC, Stevens RJ, Stratton IM, Levy JC, Matthews DR. A method for assessing quality of control from glucose profiles. Diabet Med. 2007 Jul;24(7):753–8. Epub 2007 Apr 19.
6) Rodbard D. Interpretation of continuous glucose monitoring data: glycemic variability and quality of glycemic control. Diabetes Technol Ther. 2009 Jun;11 Suppl 1:S55–67. doi: 10.1089/dia.2008.0132
7) Rodbard D. New and improved methods to characterize glycemic variability using continuous glucose monitoring. Diabetes Technol Ther. 2009 Sep;11(9):551–65. doi: 10.1089/dia.2009.0015.
8) Rodbard D. Clinical interpretation of indices of quality of glycemic control and glycemic variability. Postgrad Med. 2011 Jul;123(4):107–18. doi: 10.3810/pgm.2011.07.2310
9) Rodbard D. Hypo- and hyperglycemia in relation to the mean, standard deviation, coefficient of variation, and nature of the glucose distribution. Diabetes Technol Ther. 2012 Oct;14(10):868–76. Epub 2012 Sep 6.
10) Vigersky RA. Escaping the Hemoglobin A1c-Centric World in Evaluating Diabetes Mellitus Interventions. J Diabetes Sci Technol. 2015 Feb 19;9(5):1148–51. doi: 10.1177/1932296815576363
11) Thomas A, Schönauer M, Achermann F, Schnell O, Hanefeld M, Ziegelasch HJ, Mastrototaro J, Heinemann L. The “glucose pentagon”: assessing glycemic control of patients with diabetes mellitus by a model integrating different parameters from glucose profiles. Diabetes Technol Ther. 2009 Jun;11(6):399–409. doi: 10.1089/dia.2008.011
12) Thomas A, Heinemann L. Prediction of the risk to develop diabetes-related late complications by means of the glucose pentagon model: analysis of data from the Juvenile Diabetes Research Foundation continuous glucose monitoring study. J Diabetes Sci Technol. 2012 May 1;6(3):572–80.
13) Augstein P, Heinke P, Vogt L, Vogt R, Rackow C, Kohnert KD, Salzsieder E. Q-Score: development of a new metric for continuous glucose monitoring that enables stratification of antihyperglycaemic therapies. BMC Endocr Disord. 2015 May 1;15:22. doi: 10.1186/s12902-015-0019-0
ESCAPING THE A1C-CENTRIC ROLE OF ASSESSING GLYCEMIC CONTROL IN DIABETES
Most diabetologists recognize the hemoglobin A1C (A1C) insufficiently captures the quality of glycemic control because it gives no information about the prevalence and severity of hypo- and hyperglycemia both of which are important for patient care and research. Indeed, both the human and financial costs of hypoglycemia (from Emergency Room visits, hospitalizations, to the induction of adverse cardiac events like ischemia and arrhythmias) provides a compelling case for finding a way to simultaneously include hypoglycemia and possibly other relevant metrics with A1C as a single composite outcome measure to assess effectiveness of a therapy whether it be pharmacologic, technologic, or educational. Such a composite metric can also be used to assess ongoing patient management. Yet, most interventions are rated by regulatory bodies, insurers, and professional organizations primarily if not exclusively on the effect on A1C. Thus, an intervention with a neutral effect on A1C but a reduction in the rate of hypoglycemia may not be considered very effective by regulatory bodies and payers. A1C, rat/severity of hypoglycemia, time-in-range, weight change, cost, patient satisfaction/quality of life, and blood pressure are among the clinically relevant variables that could be included in a composite score. To this end, there have been several attempts to devise composite endpoints and display them in graphic and/or tabular form. These include the glucose pentagon, the Q-score, and hypoglycemia-A1C score. The advantages and disadvantages of these composite metrics will be discussed.
CSII IN TYPE 1 DIABETIC PREGNANT WOMEN: ITS EFFECTIVENESS AND SAFETY DURING GESTATION AND DELIVERY
Dipartimento di Medicina Clinica e Molecolare, FACOLTÀ DI MEDICINA E PSICOLOGIA, SAPIENZA, Università di Roma
Insulin pump is a flexible option for people with diabetes.
However, CSII does not bring to a significant improvement of clinical outcome in type1 diabetic pregnant women when compared with multiple daily injections.
Timely information on how carbohydrate to insulin ratio and basal insulin infusion change throughout pregnancy, during and after delivery might lead to a more appropriate pump management particularly in women under ‘SAP therapy’.
We confirmed a progressive CHO to insulin ratio decline throughout pregnancy at each meal time with an inverse trend in very late pregnancy (after the 36th week). At breakfast, the CHO/I ratio was often lower than at lunch and/or dinner.
We also showed that insulin pump is feasible and safe during delivery when a protocol is given to selected and well educated women from the beginning of the third trimester.
This strategy obtains good and stable maternal ‘peri-partum’ capillary blood glucose profiles.
In conclusion, recommendations guiding therapeutic decisions improve patients' metabolic control and quality of life.
Angela Napoli*, Camilla Festa, Marzia Bongiovanni, Luca Mattei and Antonietta Colatrella.
Continuous Subcutaneous Insulin Infusion (CSII) in Diabetic Pregnancy:A Review.
Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2009, 31872-2148/09 2009.
Raffaella Fresa, 1Natalia Visalli, 2Vincenzo Di Blasi, 1Vincenzo Cavallaro, 1Egle Ansaldi, 3Oria Trifoglio, 4Santina Abbruzzese, 2Marzia Bongiovanni, 5Mariano Agrusta and Angela Napoli5.
Experiences of Continuous Subcutaneous Insulin Infusion in Pregnant Women with Type 1 Diabetes During Delivery from Four Italian Centers: A Retrospective Observational Study.
Diabetes technology & therapeutics volume 15, number 4,1–8, 2013.
CSII in flexible option for people with diabetes.
However, CSII does not bring a significant improvement of clinical outcome in type1 diabetic pregnant women when compared with multiple daily injections.
Timely information on how the carbohydrate to insulin ratio and basal insulin infusion change throughout pregnancy, during and after delivery might lead to a more appropriate pump management particularly in women under ‘SAP therapy’.
We observed a progressive CHO/I ratio decline throughout pregnancy at each meal time with an inverse trend in very late pregnancy (after the 36th week). At breakfast, the CHO/I ratio was often lower than at lunch and/or dinner.
We also showed that insulin pump is feasible and safe during delivery by delivering a protocol for the management of metabolic control during partum of type1 diabetic pregnant women, in selected women who have been appropriately instructed.
This strategy obtained a good and stable maternal peripartum capillary blood glucose profiles.
In conclusion, recommendations guiding therapeutic decisions could improve patients' quality of life by reducing their anxiety.
Angela Napoli*, Camilla Festa, Marzia Bongiovanni, Luca Mattei and Antonietta Colatrella.
Continuous Subcutaneous Insulin Infusion (CSII) in Diabetic Pregnancy:A Review.
Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2009, 31872-2148/09 2009.
Raffaella Fresa, 1Natalia Visalli, 2Vincenzo Di Blasi, 1Vincenzo Cavallaro, 1Egle Ansaldi, 3Oria Trifoglio, 4Santina Abbruzzese, 2Marzia Bongiovanni, 5Mariano Agrusta and Angela Napoli5.
Experiences of Continuous Subcutaneous Insulin Infusion in Pregnant Women with Type 1 Diabetes During Delivery from Four Italian Centers: A Retrospective Observational Study.
Diabetes technology & therapeutics volume 15, number 4,1–8, 2013.
GAMES FOR HEALTH
University G. d'Annunzio, Department of Medicine and Aging, Chieti, Italy
Recent studies suggest that Serious Games (SG) are interesting and innovative tools useful to influence attitudes, beliefs and behaviors. SG use entertainment technology to teach, train, or change the behavior, encouraging active engagement and processing of information from the users. Games for health are games with a focus on health care, physical and mental fitness, and their popular application areas are nutrition, physical training, education, and prevention. The game-based learning principles target intrinsic motivation, learning through fun, authenticity, self- reliance/autonomy, and experiential learning. The mechanisms adopted include rules, clear but challenging goals, fantasy, progressive levels of difficulty, interactivity, player control, uncertainty, feedback and a social element. Active videogames seem to be effective in increasing energy expenditure and promoting physical activity. It has been shown that playing video games can promote extrinsic motivation and foster positive emotion with possible very important effects on health behavior. Therefore, SG can be promising tools that seek to entertain the user while attempting to elicit some form of change in behavior. Our recent studies show that an original Web Game called “Gustavo in Gnam's Planet” increases knowledge about healthy food and improves healthy lifestyle habits; our SG “could be an important useful mean and an auspicious tool for prevention programs within a multidimensional educational program”.
Video games seem to be persuasive instruments for education in different interventions, and it is known the potential of using video games and gamification to promote healthy habits and better self-management of chronic diseases and diabetes in pregnancy.
Leeds Institute of Cardiovascular and Metabolic Medicine, Biostatistics and Epidemiology, University of Leeds Leeds, United Kingdom
It is increasingly well recognised that sleep duration and sleep quality are factors involved in glucose homeostasis. Recent technology, using continuous glucose monitoring combined with continuous actigraphy, allows us to explore the relationship between glucose and sleep in real-time, in a free-living rather than lab-based situation. This intensive longitudinal data allows us unprecedented insight into how sleep and glucose interact. Glucose control is particularly important in the context of pregnancy, where tight glucose control is associated with a significantly better outcome for mother and baby. Despite available treatments, this is often not achieved and women are particularly cautious about taking drugs during pregnancy. Understanding the relationship between sleep and glucose may enable us to develop novel lifestyle based interventions to optimise glucose control. I will present data from our recent studies of sleep in pregnant women with diabetes.
Follow me on Twitter: EleanorScott@TIME_research
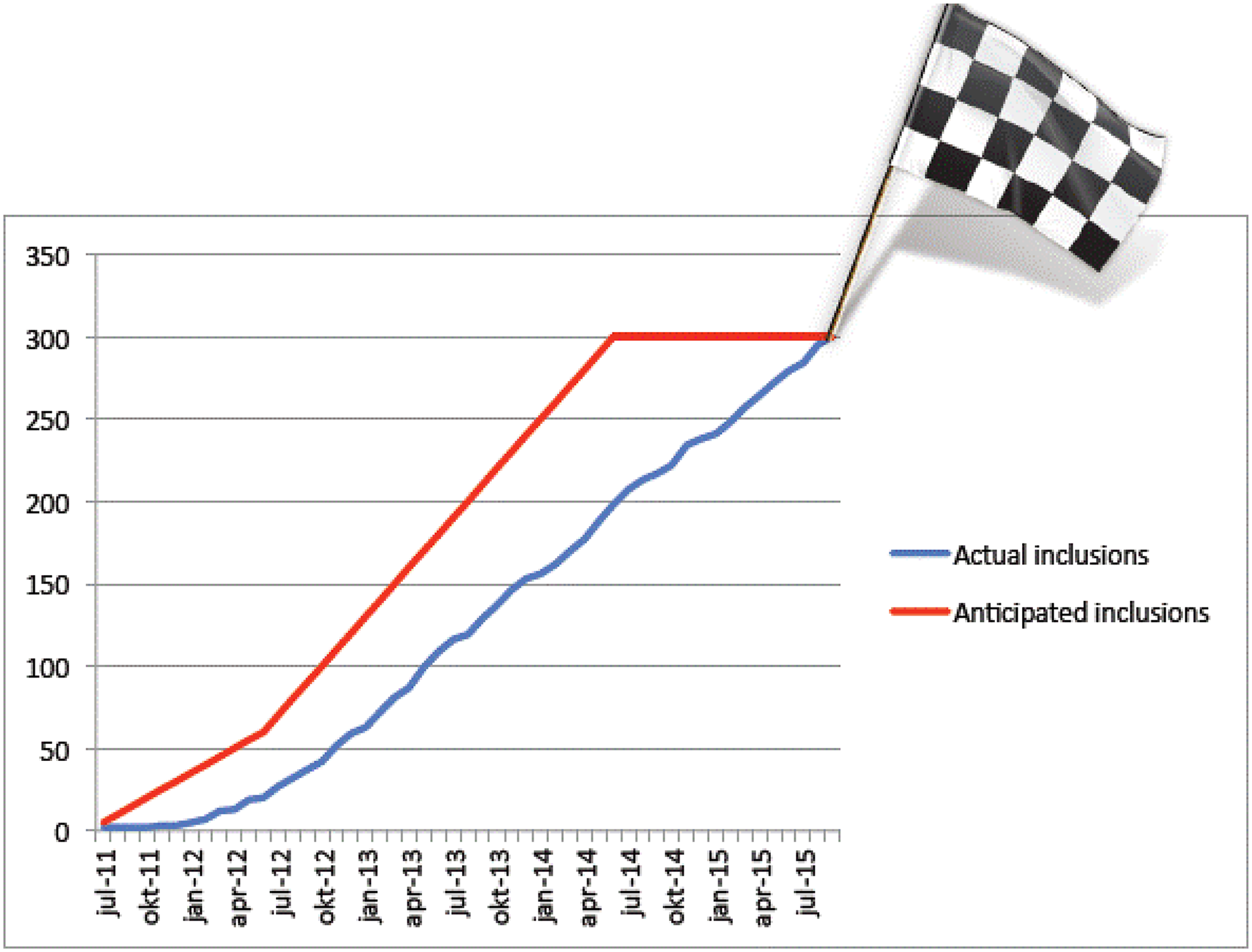
Inclusions september 2015: pregnant women n = 300
Type 1 DM n = 109
Type 2 DM n = 83
Gestational diabetes n = 108
WHO NEEDS AN ARTIFICIAL PANCREAS IN PREGNANCY?
University of East Anglia, Medicine, Norwich, United Kingdom
Continuous glucose monitoring (CGM) has highlighted the gap that exists between our expectations of tight metabolic control and the realities of actually achieving this, particularly during type 1 diabetes pregnancy. Longitudinal measurements indicate that despite overall “good” HbA1c levels, pregnant women with type 1 diabetes spend 8 hours per day with blood glucose levels above the recommended targets. New closed-loop (CL) or artificial pancreas approaches integrate insulin pump delivery (CSII) with continuous glucose monitoring (CGM) via computerized algorithms.
The vital component of a CL system for use during pregnancy is a control algorithm which can function safely despite the physiological changes in glucose turnover, endogenous glucose production and insulin kinetics. We have defined these changes in type 1 diabetes pregnancy and completed proof-of-concept studies evaluating overnight CL, in early (12–16 weeks) and late (28–32 weeks) gestation. Pilot feasibility studies demonstrated near-normal overnight glucose control (85–100% time within the target range of 3.5-7.8mmol/l), during early and late gestation. In a subsequent 24-hour crossover study comparing CL vs. conventional CSII, CL achieved excellent overnight control (95–100% time in target), with 80% overall time in target, during meals, snacks and physical activity. Home studies evaluating the feasibility, safety and efficacy of CL in real-life home settings are underway. Ongoing studies also suggest that CL can be safely used during in-patient admissions to hospital maternity units, to maintain glucose control following antenatal steroids for fetal lung maturation as well as before, during and after delivery.
Joslin Diabetes Center, Pediatrics, Boston, USA
Intensive insulin therapy and use of advanced diabetes technologies for type 1 diabetes (T1D) management place substantial burdens upon children, adolescents, and young adults. Despite these treatment tools, the majority of young patients do not achieve the recommended HbA1c targets of <7.5% (58 mmol/mol) for patients <18 years old and <7% (53 mmol/mol) for those 18 and older; only ∼1/4 youth <18 reach target and only ∼1/5 aged 18–25 achieve target. The combination of the demanding treatment program and lack of goal attainment can lead to substantial diabetes and psychosocial distress. There is likely a bidirectional interaction between psychosocial factors and CGM use as CGM adds to the burdens of care while CGM also offers opportunity to mitigate distress by providing useful real-time glucose data to guide management as well as alert patients (and family members connected remotely) of out-of-range glucose levels.
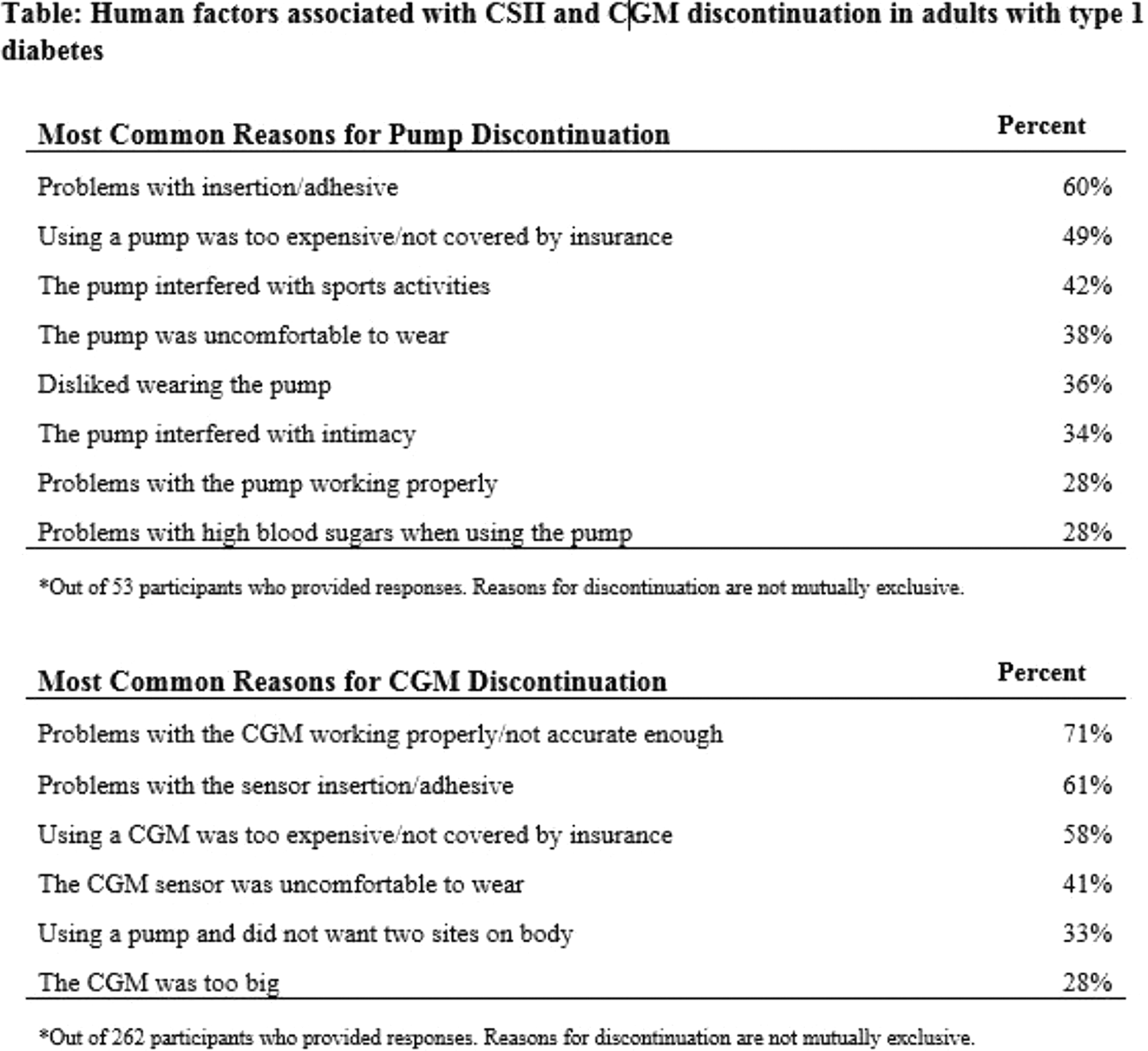
Pediatric patients are particularly burdened by CGM; although many may initiate CGM, most fail to sustain use. In turn, most of these young patients do not receive glycemic benefits from CGM. Discontinuation has been related to perceived burdens due to the device's size, pain associated with insertion, frequent alerts/alarms, and inaccuracies in early systems. Additionally, psychosocial distress has been more apparent in pediatric compared to adult patients using CGM (Diab Tech Ther 2012; 14:523-6). Youth using CGM reported more anxiety while adults reported less; youth's parents reported continued fear of hypoglycemia; youth and parents reported more negative affect around BG results; and parent-proxy report of youth depression was higher. In contrast to the youth CGM experience, adults using CGM reported less diabetes-related burden. Thus, young patients with T1D continue to demonstrate significant challenges in sustaining CGM use. Newer CGM devices with improved performance may help to overcome these behavioral barriers and improve psychosocial outcomes to sustain CGM use so that pediatric patients can achieve CGM benefits related to improved glycemic control without severe hypoglycemia.
University Medical Centre Ljubljana- University Children's Hospital, Department of Pediatric Endocrinology- Diabetes and Metabolic Diseases, Ljubljana, Slovenia
Parents have a very important role in the diabetes management and emotional coping for their child with diabetes. They become responsible for the disease management in order to avoid excursions of blood glucose and enable a better quality of their child's life. Parents often experience a great burden in their life that groves with this responsibility. Therefore, they must face their fears, sense of guilt, sadness, anger, despair and the fact that they've lost their healthy child and, consequently, the previous way of life.
On the other hand they are driven by parental instinct to protect their child with tendency to over control the child and his diabetes or the outside influences. Parents' concerns and overprotection can also be associated with the fear of hypoglycemia. This fear can create a great tension and conflicts in family relationships. In 2013–2014 a study was performed at University Children's Hospital. A group of 231 parents (140 mothers and 91 fathers) participated. The results showed that mothers were experiencing greater stress, fear of hypoglycemia, feelings of anxiety, and had worse subjective well-being, whereas fathers were generally less functionally involved in the diabetes management. Parents have a central role in coping with the child's illness and its management. They are not only important as a child's health experts, but they have an important role in the regulation of child's and their own emotions created by the new life with diabetes. Therefore it is important to help and assist parents to recognize and identify emotions and debilitating affects that will likely influence family, their child and themselves.
AUF DER BULT- Kinder- und Jugendkrankenhaus, Diabetes Centre for Children and Adolescents, Hannover, Germany
Canary Health, Medical, Los Angeles, USA
Digital health self-management is a new category of behavior change interventions, designed to improve health and reduce costs of care for individuals with one or more chronic conditions. Patients with diabetes must master a myriad of behaviors to improve their outcomes. In addition to the medical aspects of diabetes management they need to master, they also need to be able to live their lives while managing their disease. This is made all the more difficult since nearly all patients with type 2 diabetes have one of more other chronic conditions requiring attention. Putting the patient in the center of their diabetes journey requires a consumer-centric approach to education and support.
One proven-effective approach to this requirement is the peer-to-peer Chronic Disease Self-management Program (CDSMP). Developed in 1992 and continuously updated by Dr. Kate Lorig and her colleagues at Stanford University, CDSMP, and its digital transformation (Better Choices Better Health (BCBH)) teach participants how to manage their chronic conditions, adhere to medication regimens, and maintain functional ability. CDSMP is premised on certain assumptions: that patients can learn to take responsibility for the day-to-day management of their conditions; that knowledgeable patients who practice self-management can improve their health status and use fewer health care resources; and that patient self-management programs should be inexpensive and widely available. In numerous published studies of CDSMP and BCBH, participants were shown to have improved their health behavior, such as exercise, symptom management, medication adherence and communication with physicians, and maintained or improved their perception of their health status. Participation in CDSMP was also shown to reduce AIC, hospitalizations and hospital days.
This presentation will focus on the digital version of the CDSMP by giving an overview of the program and a summary of the outcomes which have been demonstrated in patients with diabetes.
Department of Surgery, Brody School of Medicine, East Carolina University, Greenville, NC, USA
• it is unigender even though there are sharp differences in fat distribution between men and women;
• it does not account for fitness and would, for example, accept one of our recent subjects for bariatric surgery at a weight of 307 lbs., 5′8″ and a BMI of 47 even though he was our fastest running back at our university;
• it does not allow for the changes with aging and the fat infiltration of muscle and
• most seriously, it prevents access to bariatric surgery to African Americans and Asians who develop diabetes and other co-morbidities of the metabolic syndrome. Three-dimensional scanning with white light or infra-red technology, finally offers an approach to quantify the dimensions of the human body with the potential to measure and predict physical performance and health. The technology, similar to but far more accurate than that used daily at airports for the screening of travelers, is rapid, safe and inexpensive.
Note that the two individuals are the same height and weight, yet an adiposity index, calculated from the derived measurements of surface area, trunk volume and sagittal measure at levels of the pelvis can sort patient physiques into “apple” vs.”pears” and allow prediction of the likelihood of the metabolic syndrome.

University Children's Hospital- University Medical Centre Ljubljana, Department of Endocrinology- Diabetes and Metabolism, Ljubljana, Slovenia
A robust literature has demonstrated that hyperglycemia, hypoglycemia and increased glucose variability are independently associated with mortality in diverse cohorts of critically ill patients, and that diabetic status modulates these relationships. Time in targeted blood glucose range (TIR) may be a suitable descriptor of the overall efficacy and safety of glycemic control, and could be considered as marker of the severity of dysglycemia and as an index of the quality of care. Moreover, high TIR may be the key element of glycemic control needed to effect optimal outcome and may, in fact, blunt the deleterious impact of transient excursions into the hypoglycemic and hyperglycemic ranges.
A retrospective study involving a cohort of 3,297 patients with intensive care unit (ICU) length of stay (LOS) at least 1.0 day admitted between 2009–2013 to a single mixed medical surgical ICU demonstrated that TIR 70-140 mg/dL >80% was independently associated with survival in critically ill non-diabetic patients, independently of ICU LOS and severity of illness (Crit Care 2015; 19:179). For non-diabetic patients, the observed:expected mortality ratios for TIR above and below the median value of 80.6%, using Acute Physiology and Chronic Health Evaluation IV methodology, were 0.53 and 0.78. In contrast, among DM there was no clear relationship between TIR 70-140 mg/dL and survival. A growing literature corroborates the significance of TIR as a “unifying” metric of glycemic control in the critically ill and has important implications for the design of clinical protocols for glycemic control in the critically ill as well for the design of future interventional trials of intensive insulin therapy.
PREVENTING READMISSIONS IN HIGH RISK DIABETES PATIENTS: PLANNING & IMPLEMENTING A TRANSITIONAL CARE PROGRAM
New York Presbyterian Hospital/ Weill Cornell Medicine, Division of Endocrinology- Diabetes & Metabolism, New York, USA

High quality evidence is crucial for establishing the clinical benefit of new technologies, which patient groups benefit the most, cost-effectiveness, short and long-term safety, and patient usability. But often diabetes technology is introduced into practice before all but the slimmest evidence base has been established.
Often there is a paucity of evidence in diabetes technology because many studies are inappropriately designed, e.g. inadequately powered or involve the wrong patient groups.
Although meta-analysis of randomized controlled trials is considered the cornerstone methodology for evidence-based medicine, it is frequently misused and quoted inappropriately, with misleading conclusions for decision-making. Examples include selecting trials that do not match intended use (e.g. in CSII vs. MDI trials, subjects have only modestly elevated HbA1c at baseline, or subjects with severe hypoglycaemia have been excluded); including short-duration trials where outcome cannot be accurately assessed (e.g. trials <6 months when measuring severe hypoglycaemia); and including trials using obsolete technology (e.g. first-generation insulin pumps). Individual patient data meta-analysis, linking patient-level characteristics to outcome, is useful for establishing those likely to benefit most from technologies.
Guidelines and consensus statements can be surprisingly lacking in evidence and, based usually on average trial responses without context and clinical judgement, can ill-serve the individual patient.
Stakeholders - clinicians, manufacturers, patients, funders, regulators, publishers - need to cooperate in setting, regulating, monitoring and interpreting best evidence for diabetes technology, be it garnered from trials, registers, surveys, expert opinion, patient responses or other means.
ATTD 2016 Oral Presentations
ELASTARGENE 3C HELPS TO IMPROVE GLYCATED HAEMOGLOBIN IN CHILDREN AND ADOLESCENTS WITH TYPE 1 DIABETES USING INSULIN PUMP THERAPY
Luigi Sacco, Pediatrics, Milano, Italy
Barbara Davis Center for Diabetes, University of Colorado, Aurora, USA
Center for Diabetes and Vascular Disease, 48145, Muenster, Germany
Study sponsored by Sanofi (NCT02227212)
HEVA HEOR, Health economics, Lyon, France
Medical University of Graz, Internal Medicine, Graz, Austria
Profil, Neuss, Germany
A.O. Ospedale Niguarda Ca' Granda, Interdisciplinary Diabetes and Pregnancy Center, Milano, Italy
Hospital Universitario San Ignacio, Endocrinology, Bogotá D.C, Colombia
Children's Hospital of Eastern Ontario, Endocrinology and Metabolism, Ottawa, Canada
To compare the effect of the Trend Arrow Adjustment Tool (TAAT), JDRF CGM Study Group 10/20% adjustment tool, and no adjustment for arrows, on postprandial glucose.
University of Cambridge Metabolic Research Laboratories, Institute of Metabolic Science, Cambridge, United Kingdom
St Vincent's Hospital, Department of Endocrinology and Diabetes, Melbourne, Australia
Yale School of Medicine, Pediatric Endocrinology, New Haven, USA
Profil, Medical Technology, Neuss, Germany
Rensselaer Polytechnic Institute, Chemical and Biological Engineering, Troy, USA

University of California Santa Barbara, Department of Chemical Engineering, Santa Barbara- CA, USA
AMCR Institute- Inc., Diabetes, Escondido, USA

Academic Medical Center at the University of Amsterdam, Endocrinology, Amsterdam, Netherlands

Montreal Institute of Clinical Research, Montreal, Canada
Academic Medical Center - University of Amsterdam, Department of Endocrinology, Amsterdam, Netherlands
Dexcom Inc., San Diego, USA
Jaeb Center for Health Research, T1D Exchange Clinic Network, Tampa, USA

Medisch Centrum Haaglanden, Interal Medicine, Den Haag, Netherlands
Children's Hospital AUF DER BULT, Diabetes Centre for Children and Adolescents, Hannover, Germany
Joanneum Research Forschungsgesellschaft mbH, HEALTH –Institute for Biomedicine and Health Sciences, Graz, Austria
Twelve T1D patients (5 females, 7 males, age 33.0 ± 10.4, diabetes duration 15.7 ± 11.8 yrs) attended a clinical trial in a clinical research center for 12 hours. Two single-port systems were placed 24 hours prior to the trial. Patients' blood glucose dynamics was induced with high glycemic index meals followed by delayed, overdosed insulin boluses.
Medtronic, Inc., Diabetes, Northridge, USA
Diabetes Zentrum Mergentheim, Diabetes Klinik, Bad Mergentheim, Germany
The primary outcome measure was difference in HbA1c between two study groups at day 194. Pre-specified secondary outcome measures included time in hypoglycaemia and subgroup analysis by age.
Time in hypoglycaemia, defined as glucose <3.9 mmol/L, was reduced in the intervention group compared with control at study end (-0.47 ± 0.134 hrs/day (mean±SE); p < 0.001). Time in hypoglycaemia (<3.9 mmol/L) was reduced both during daytime and at night with nocturnal hypoglycaemia (<3.9 mmol/L, 11pm-6am) cut by 1.01 ± 0.26 hrs/night (mean±SE); p < 0.001) compared with the control group.
Leeds Children's Hospital, Paediatrics, Leeds- West Yorkshire, United Kingdom
Xeris Pharmaceuticals, R&D, Austin, USA
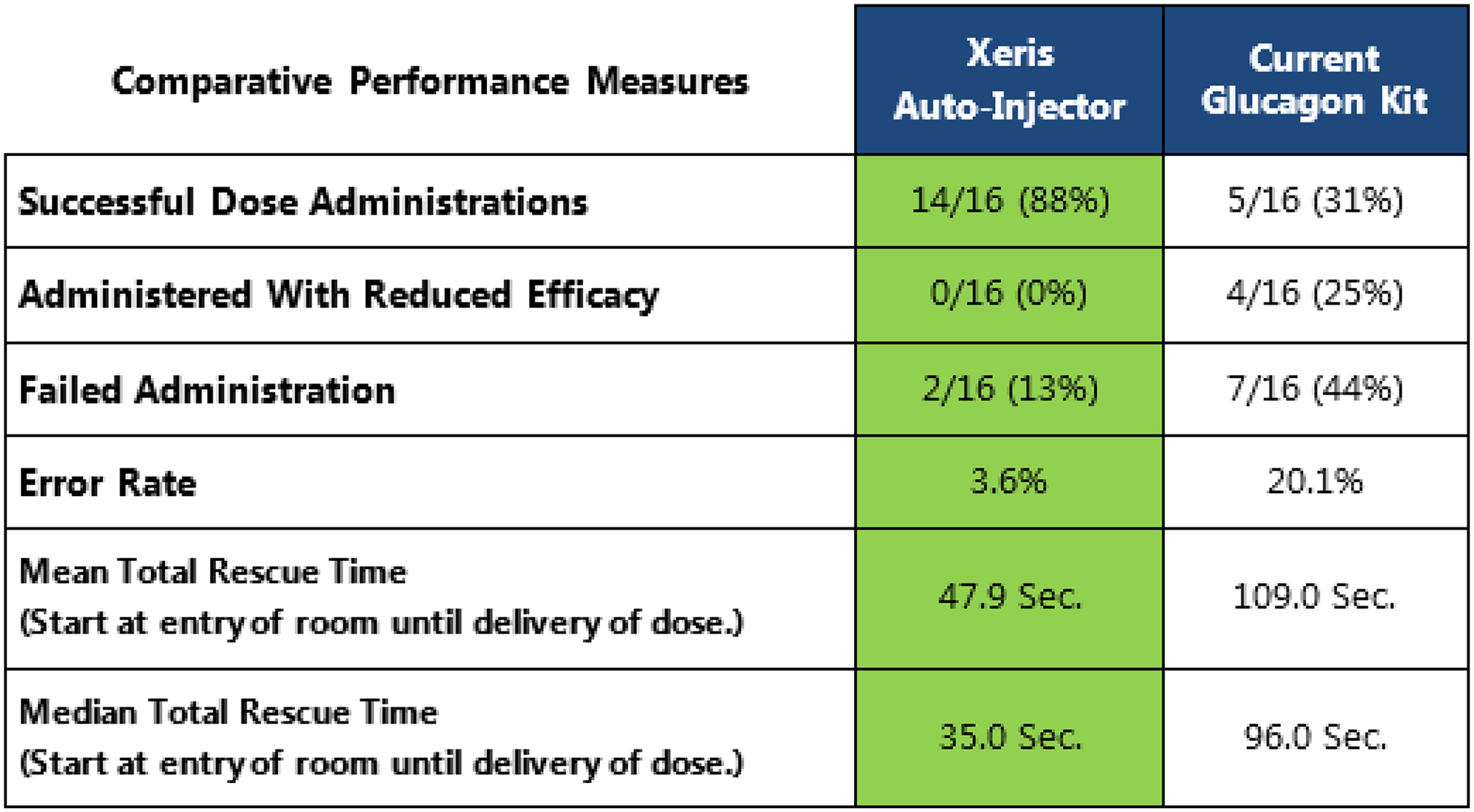
Faculty of Medicine, Pharmacology, Galle, Sri Lanka
This study was conducted to examine the effects of vitamin D therapy on renal functions of patients with diabetic nephropathy (DN).
Kohnodai Hospital - National Center for Global Health and Medicine, Department of Internal Medicine, Ichikawa, Japan
‘Auf der Bult’, Diabetes Centre for Children and Adolescents, Hannover, Germany
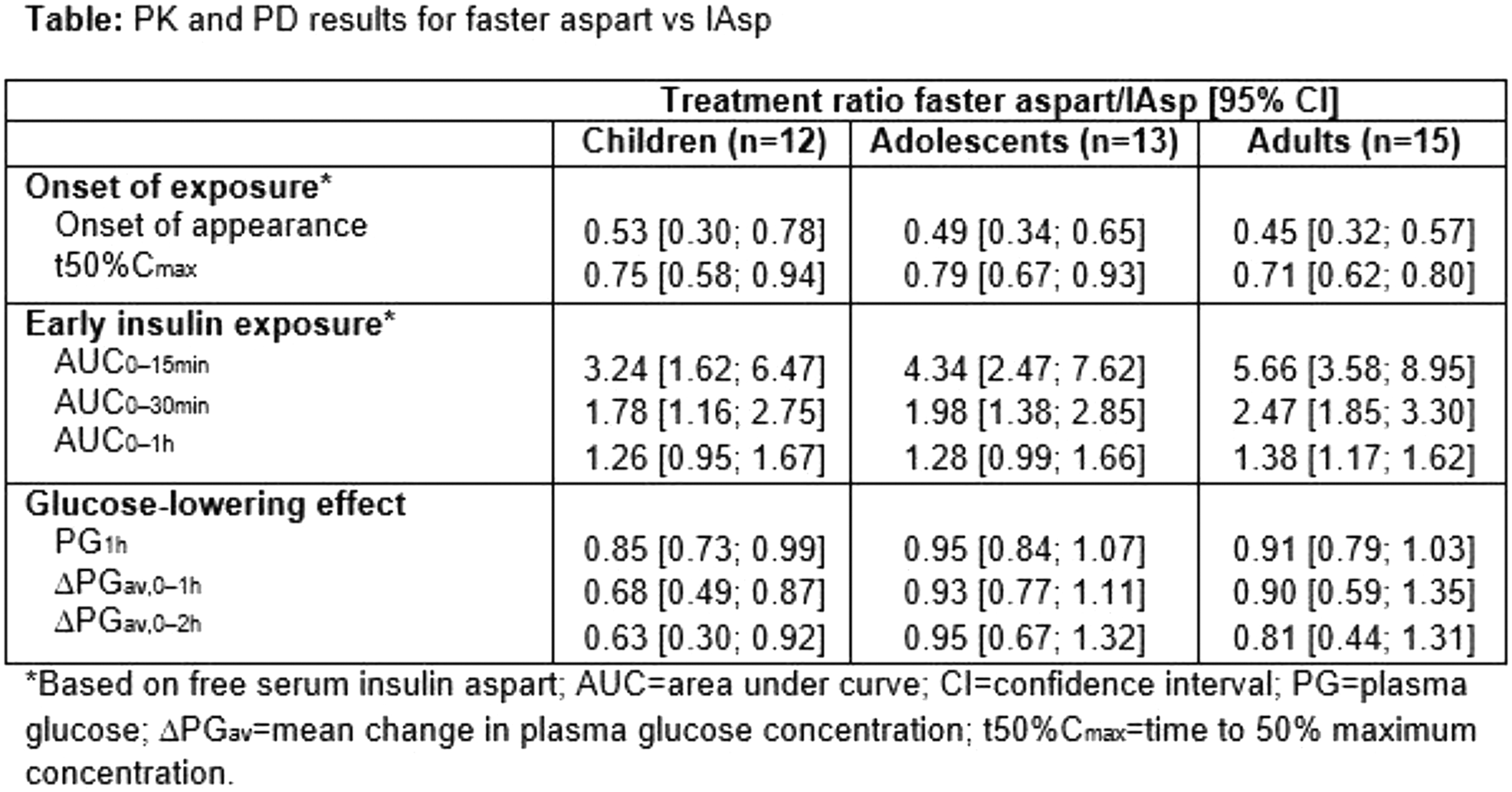
University of Parma, Department of Clinical and Experimental Medicine, Parma, Italy
Studies sponsored by Sanofi (NCT01499082, NCT01499095)
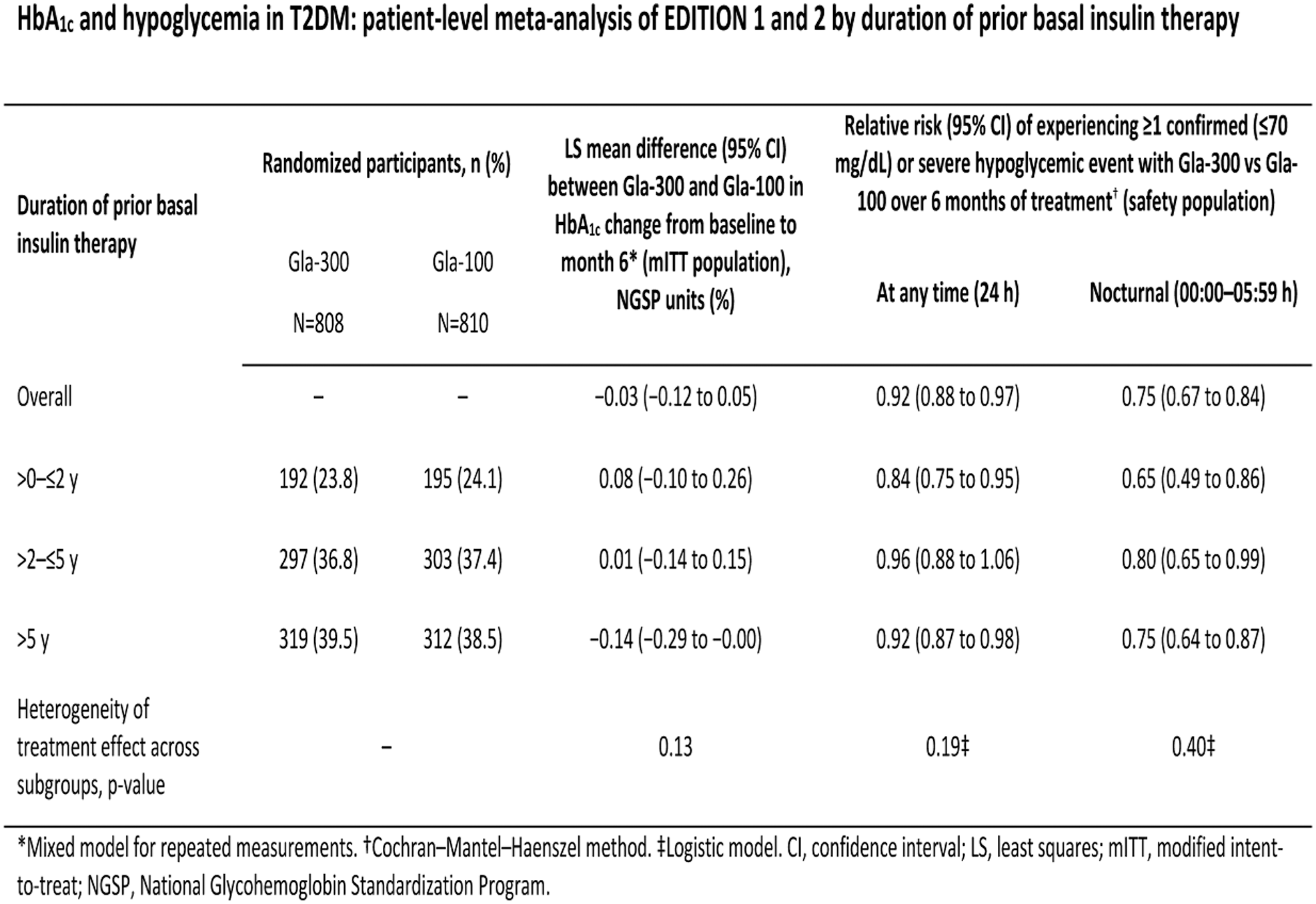
Stevens Institute of Technology, Hoboken, USA
We aim to develop a fully automated dietary monitoring system that can identify meal times, amounts, and food type, based on data continuously collected from unobtrusive, body-worn sensors. To address this, we first aim to determine the timing of eating events (such as food intake and chewing) from which other activities can be inferred.
USA
The emergence of artificial pancreas (AP)-type devices in clinical practice necessitates novel tools for understanding precisely what the device does on behalf of the patient. In particular, for a predictive AP algorithm which autonomously modulates insulin delivery relative to the prescribed basal rate, it is helpful to develop a simple metric capturing, quantitatively, instances when the algorithm took significant insulin-modulating action to mitigate, if not avoid, potential hypo- and hyperglycemic excursions. The benefits of such a metric are twofold:
1) By design, the metric will capture instances when the algorithm successfully averted situations in which the patient would have been alarmed (e.g., via CGM threshold alarms), and thus had to intervene him- or herself – which will help instill confidence in the system; and
2) Proper, guided analyses of such metrics can help patients and/or HCPs fine-tune the patient's pump settings, like basal rates, to further improve glucose control.
Animas Corporation has developed and evaluated such a metric, called the Artificial Pancreas Activity Event (APAE). This metric has two analogous variations: APAE-Hypo and APAE-Hyper, which capture instances when the algorithm took significant action to mitigate, if not avoid, hypo- and hyperglycemic excursions, respectively. The metric is based both on the duration of algorithm activity and the magnitude of its insulin modulation relative to the basal rate.
Evaluation of the metric via an in-depth in silico trial using the FDA-accepted UVA/Padova Simulator demonstrated promise in enabling patients/HCPs to better understand the system's overall therapeutic value. The figure shows a representative example of the APAEs recorded for one virtual patient using Animas' Hypoglycemia-Hyperglycemia Minimizer (HHM) algorithm.
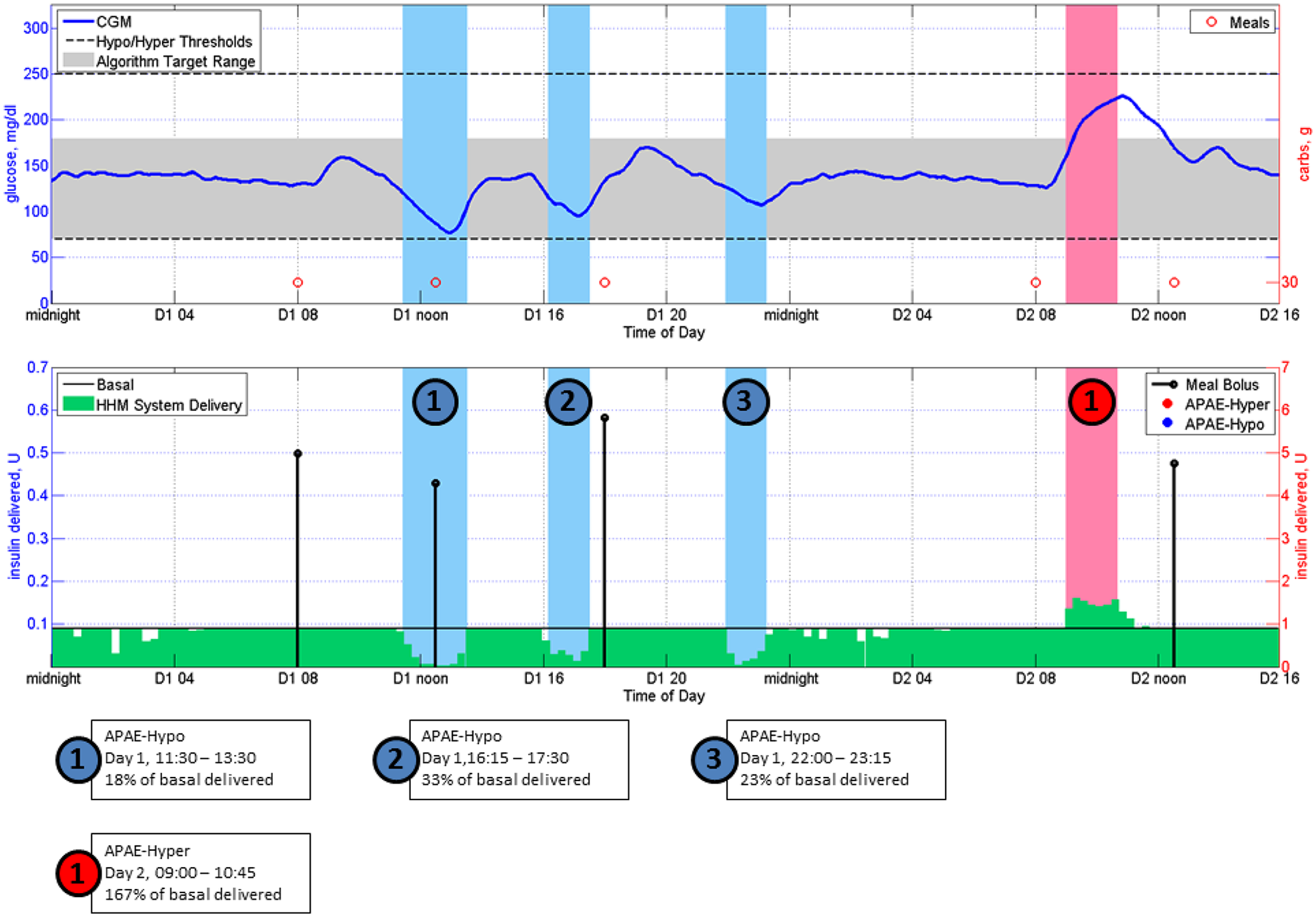
Department of Medicine, University of Perugia School of Medicine, Perugia, Italy
Beverley Balkau: has served on advisory boards for AstraZeneca, BMS, Novo Nordisk, and Sanofi.
Soazig Chevalier: is an employee of Sanofi.
Jeremy Pettus: has served on advisory boards for Sanofi, Tandem, and Novo Nordisk.
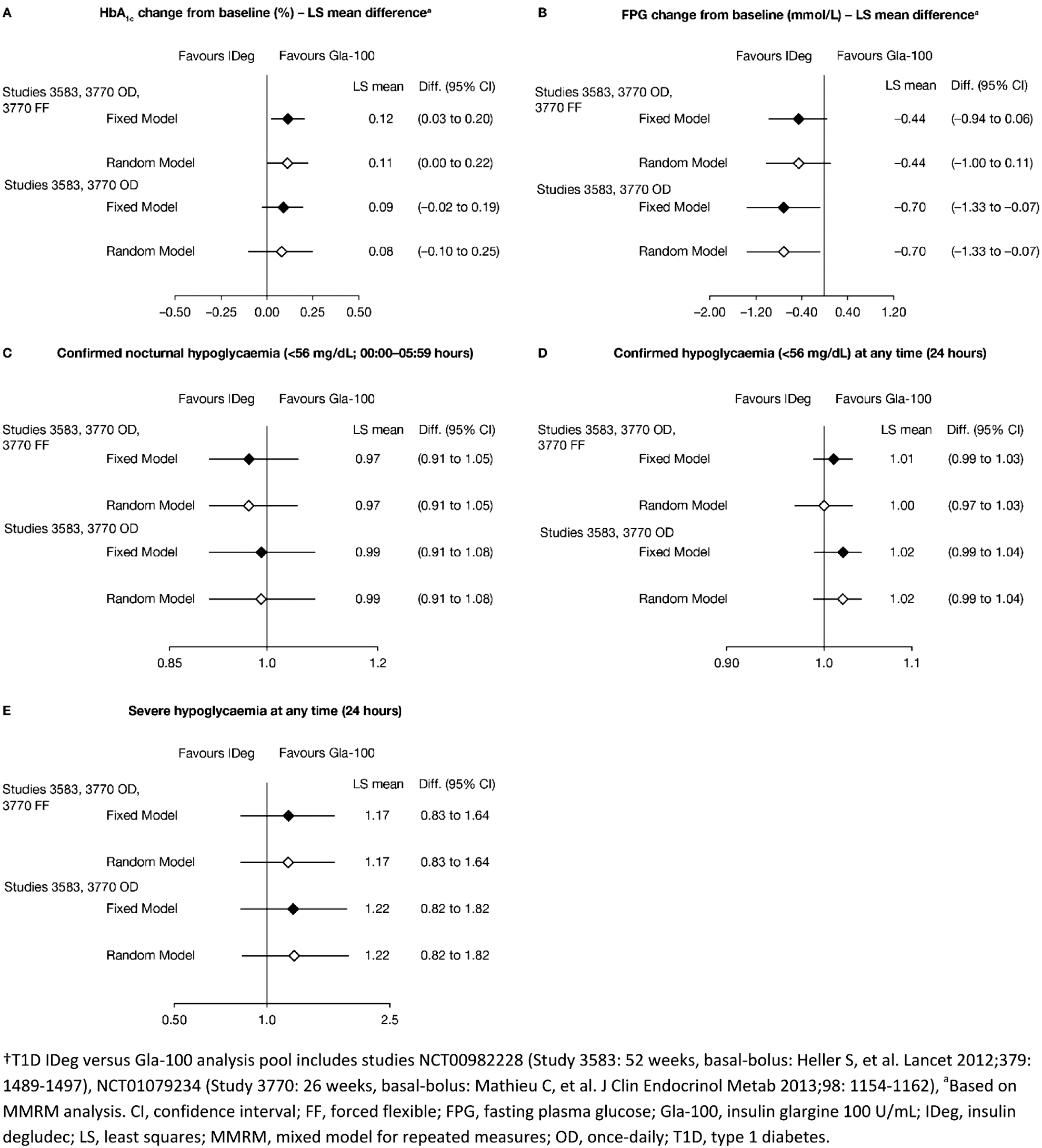
Faculty of Health Sciences and Medicine, örebro University Hospital, Örebro, Sweden
University Hospital of North Norway, Norwegian Centre for Integrated Care and Telemedicine, Tromsø, Norway
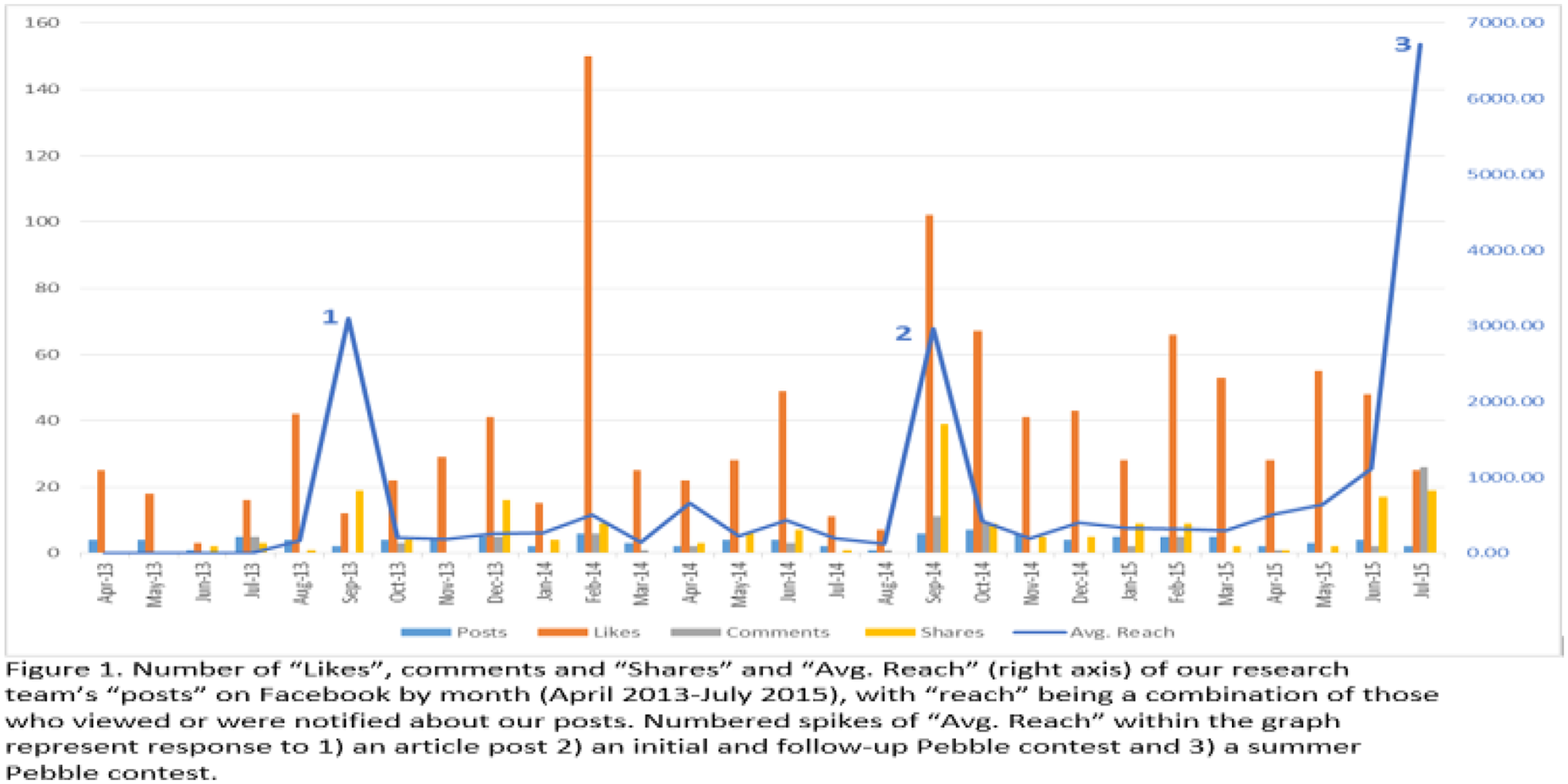
University of Pavia, Department of Electrical- Computer and Biomedical Engineering, Pavia, Italy
Imperial College London, Division of diabetes- endocrinology and metabolism, London, United Kingdom
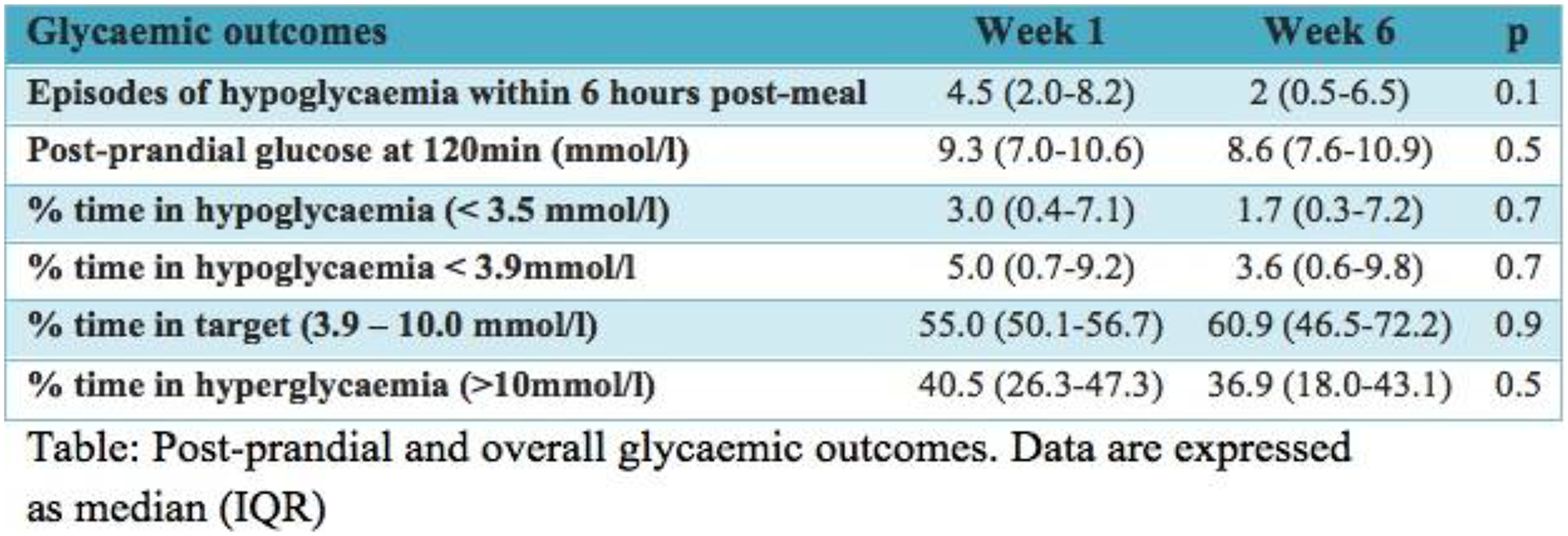
Sutter Medical Center and Center of Excellence in Diabetes and Endocrinology, USA
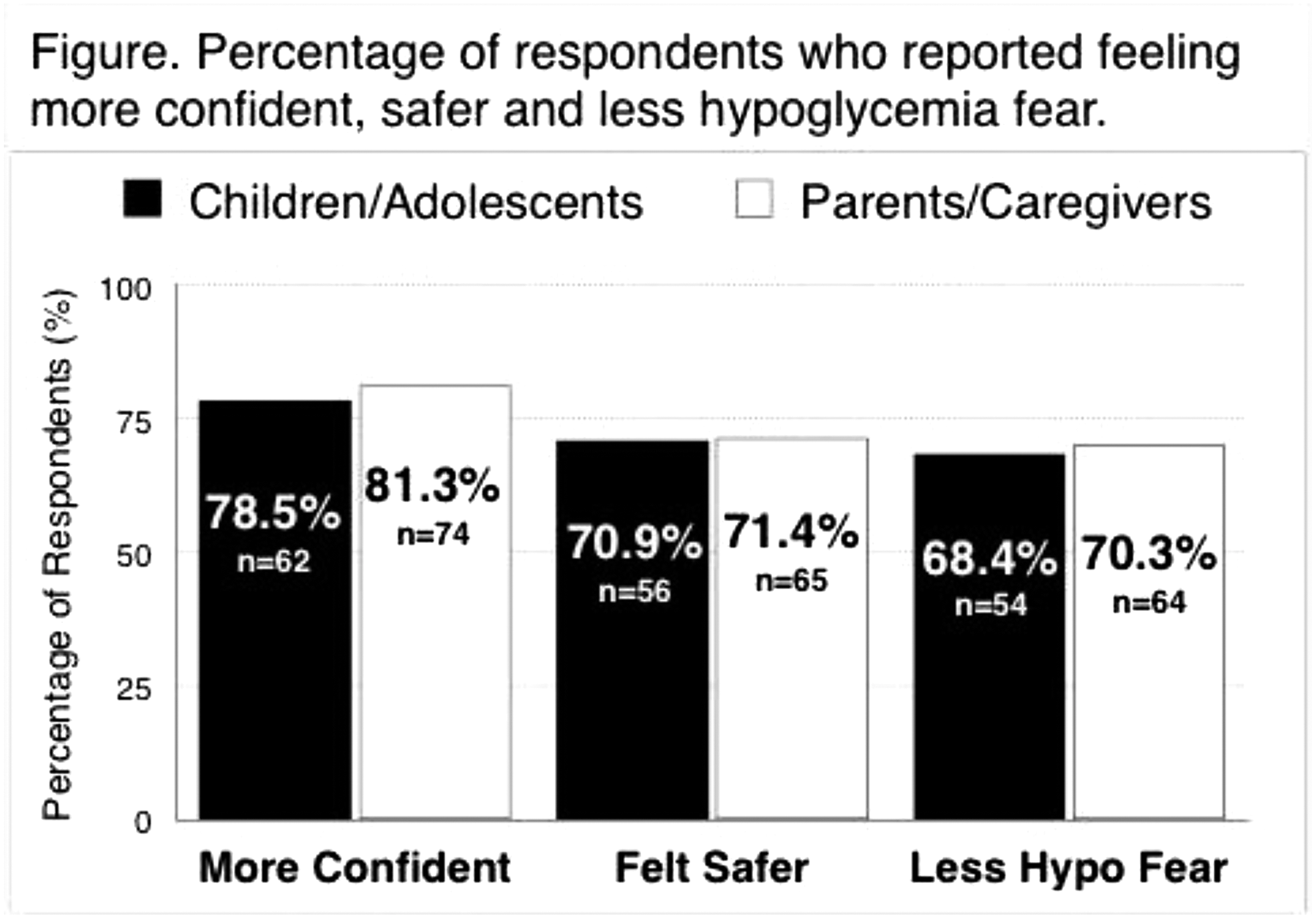
Roche Diabetes Care- Inc., Medical Affairs Department, Indianapolis, USA
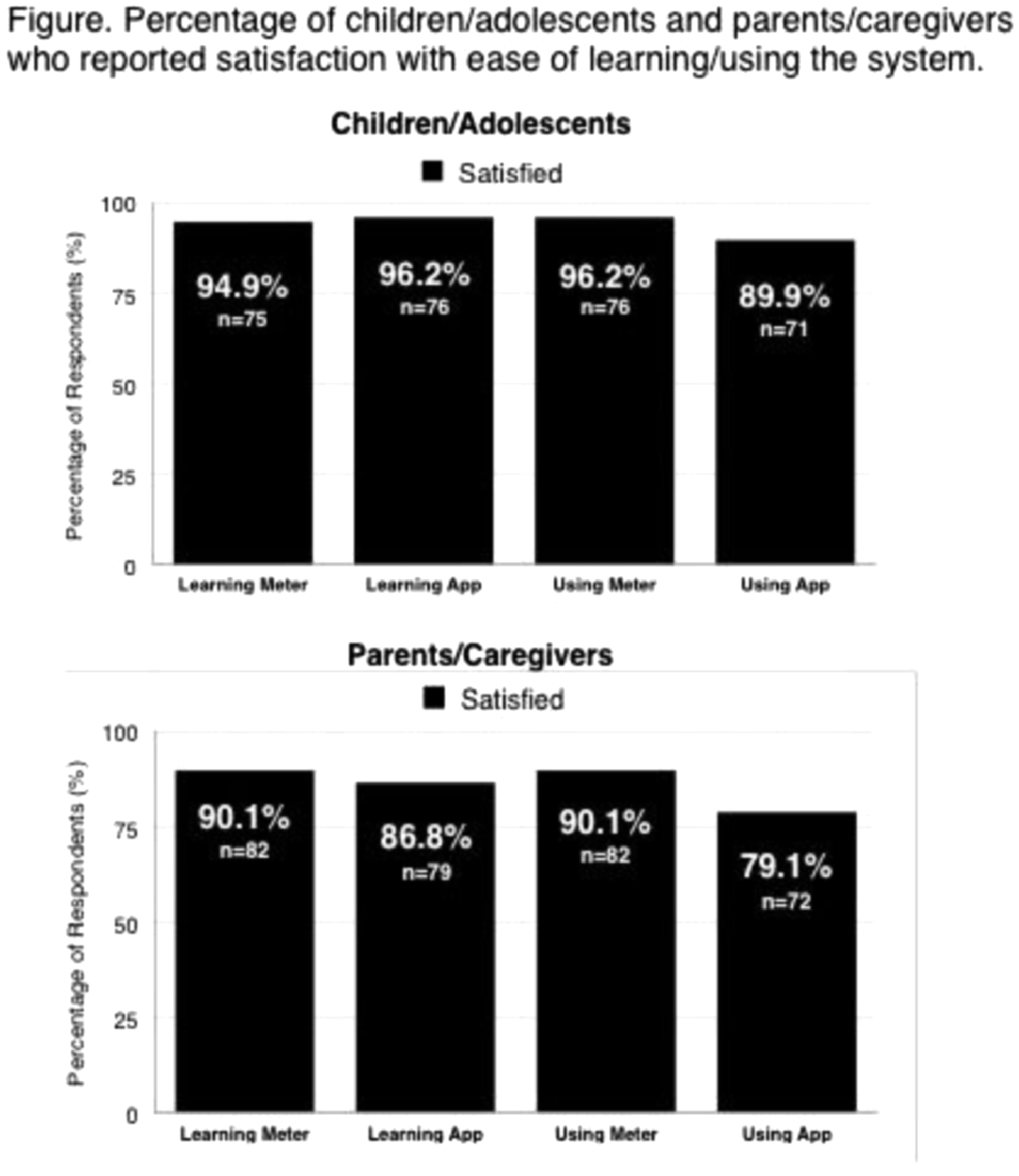
Olgahospital - Klinikum Stuttgart, Pediatric Endocrinology and Diabetology, Stuttgart, Germany
Canary Health, Medical, Los Angeles, USA
Institute of Child Health- University College London, Genetics and Epigenetics in Health and Disease, London, United Kingdom
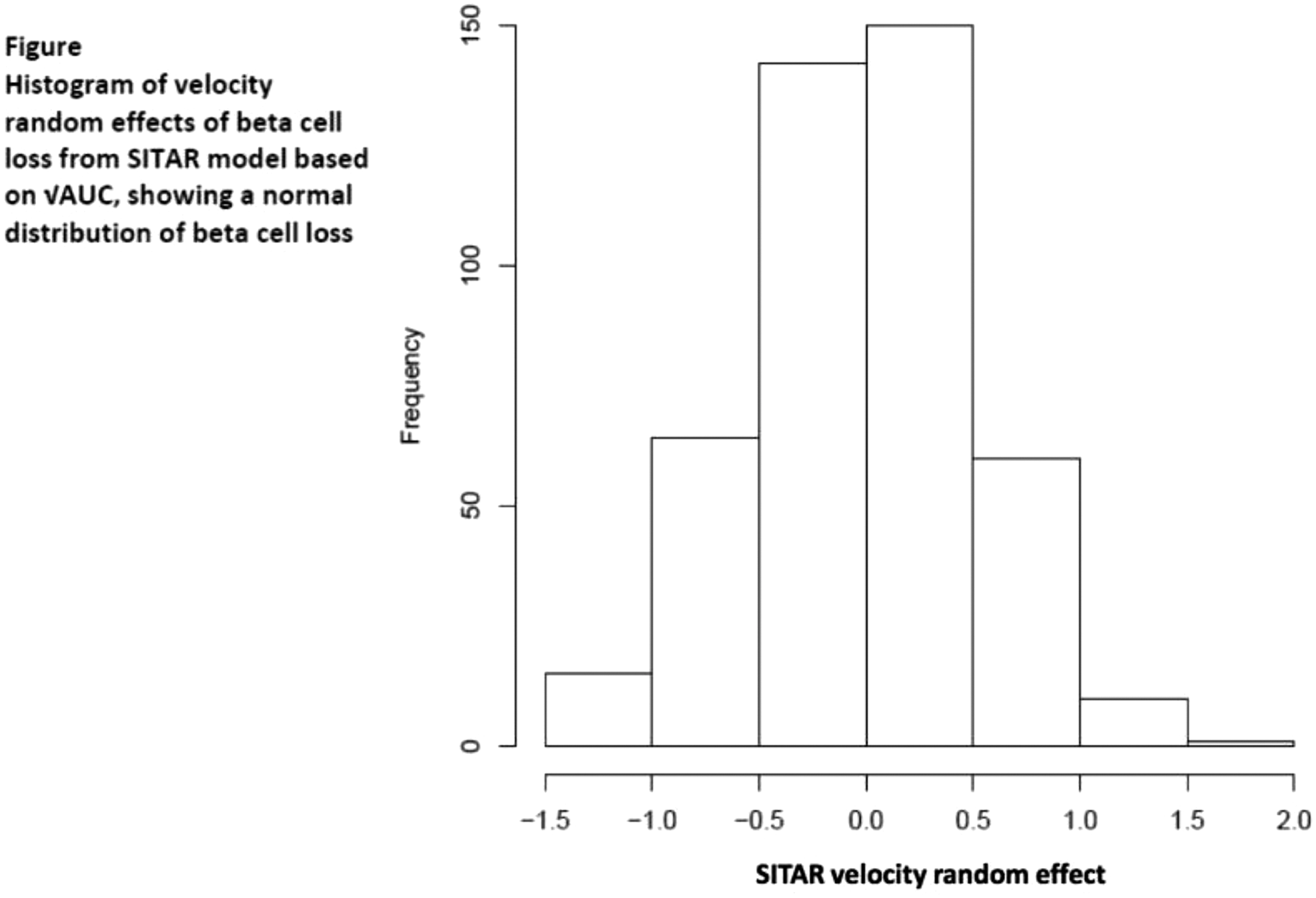
Nizhny Novgorod State Medical Academy, Endocrinology and Internal Medicine, Nizhny Novgorod, Russia
Antwerp University Hospital, Endocrinology- Diabetology- Metabolism, Edegem, Belgium
Ipswich Hospital NHS Trust, Diabetes & Endocrine Centre, Suffolk, United Kingdom
Mayo Clinic, Endocrinology, Rochester, USA

Centro Hospitalar e Universitário de Coimbra, Department of Endocrinology, Diabetes and Metabolism, Coimbra, Portugal
John Hunter Children's Hospital, Newcastle, Australia
A significant dose-dependent response was seen with increasing grams of protein from 180–300min (p < 0.001)
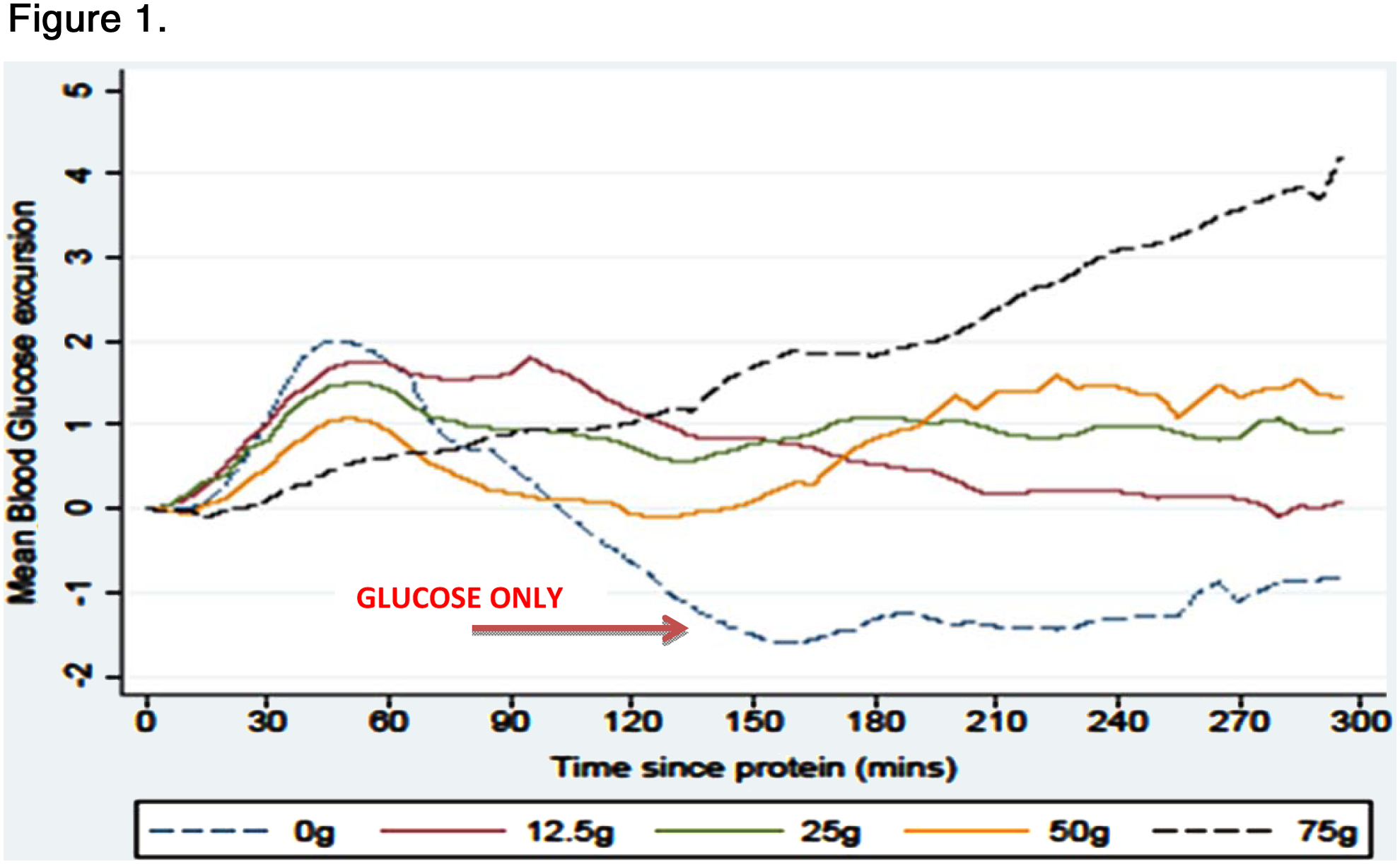
Assuta Medical Center - Maccabi Health Fund, Institute of Endocrinology and Diabetes, Tel-Aviv, Israel
Objectives
Clinical, biochemical and anthropometrical parameters during intervention were analyzed. Our Compliance and Hypoglycemia assessments were also applied.
These findings are proof- of- concept of our Gravicentric theory.
Atlanta Diabetes Associates, Atlanta, USA
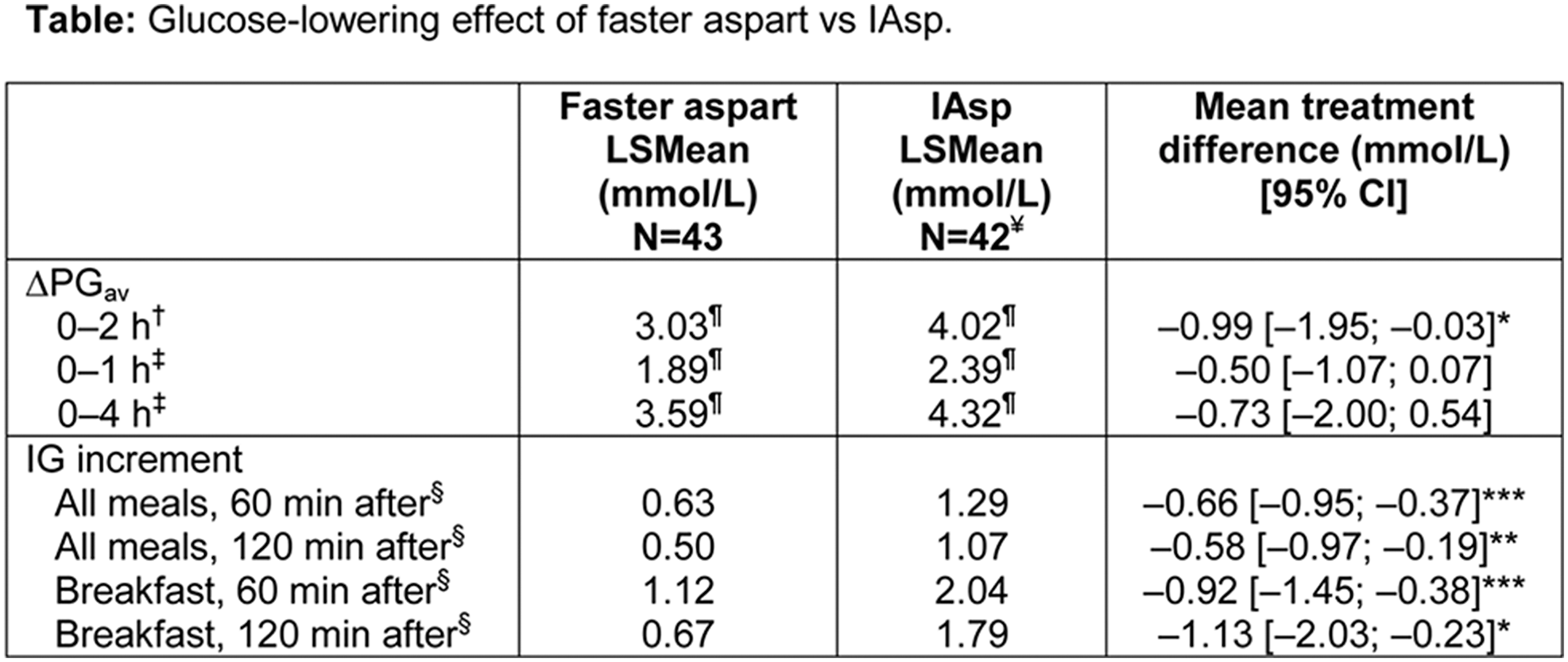
Institute for Materials Research, School of Chemical and Process Engineering- University of Leeds, Leeds, United Kingdom
ATTD 2016 E-Poster Presentations
LMC Diabetes and Endocrinology, LMC Diabetes and Endocrinology, Toronto, Canada
At 6 months, CSII subjects had achieved significantly greater A1C reduction (-1.1 + 1.2% vs -0.4 + 1.1%, p < 0.001) - maintained at 12 months. MDI subjects crossing to CSII showed -0.8% A1C reduction, with final A1C identical in both arms. SP response rate (A1C < 8.0%) was higher in the CSII arm (CSII 55% vs. MDI 28%) but by end of the CP, both groups had achieved similar response rates of 57%.
CSII total daily dose (TDD) was 520.4% lower in the SP; in the CP, MDI subjects crossing to CSII showed a 19.0% TDD reduction; final TDD was equivalent in both groups. There was no difference between groups in weight gain nor ketoacidosis. In each group, 1 patient experienced severe hypoglycemia.
HEVA HEOR, Health Economics, Lyon, France
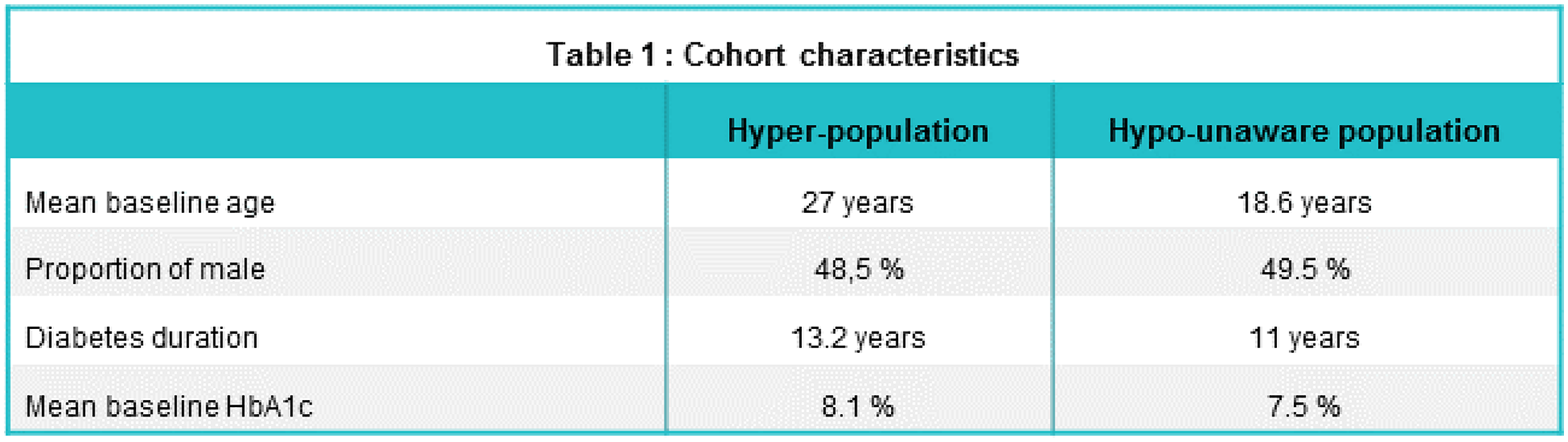
Roche Diagnostics S.L., Medical Affairs, Sant Cugat del Vallès, Spain
To reach consensus of the default values and ranges of the eDetecta alerts and define specific profiles of alerts depending on patient age, treatment and situation.

Abbott Diabetes Care, Research and Development, Alameda, USA
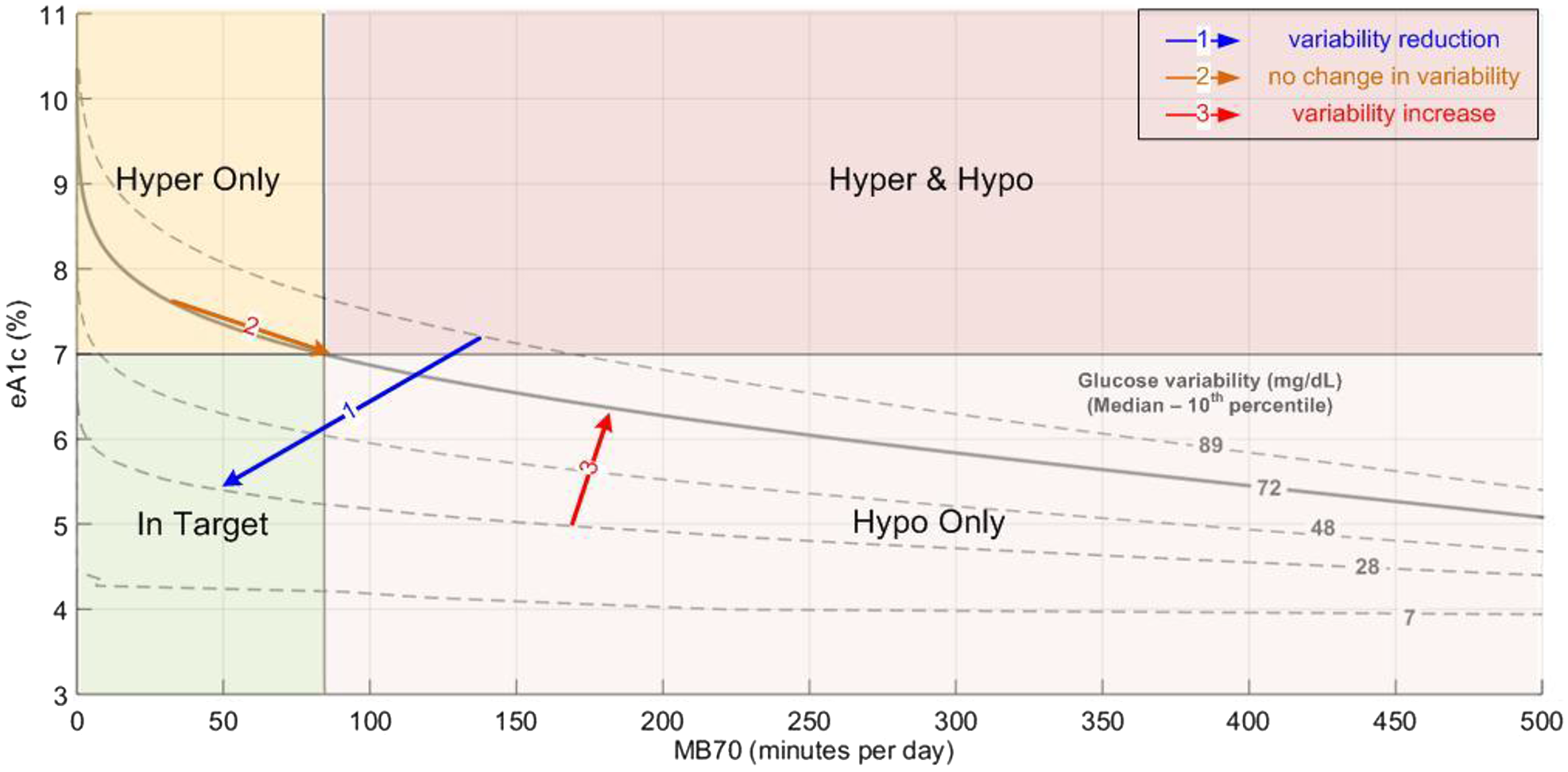
Comenius University in Bratislava- Jessenius Faculty of Medicine and University Hospital Martin, Department of Pediatrics, Martin, Slovakia
Supported by grant VEGA1/0262/14
Paris, France
• ulcers: follow-up visit in the two years preceding onset of first ulcer, • no ulcers: less than two years between last two follow-up visits.
Ulcer onset was predicted via monofilament and GTF (0-8) tests, with predictive accuracy being analysed using the AUC of ROC curves. Screening of predictive factors for ulcer onset was then performed using multivariate logistic regression.
King's College London, Diabete Research Group, London, United Kingdom
Università Vita-Salute San Raffaele, Department of Internal Medicine, Milan, Italy
Data are median and interquartile range (IQR). *In a subset of n = 15 patients, glucometers were downloaded during outpatient visits and SMBG values in the prior 3 months were analyzed.
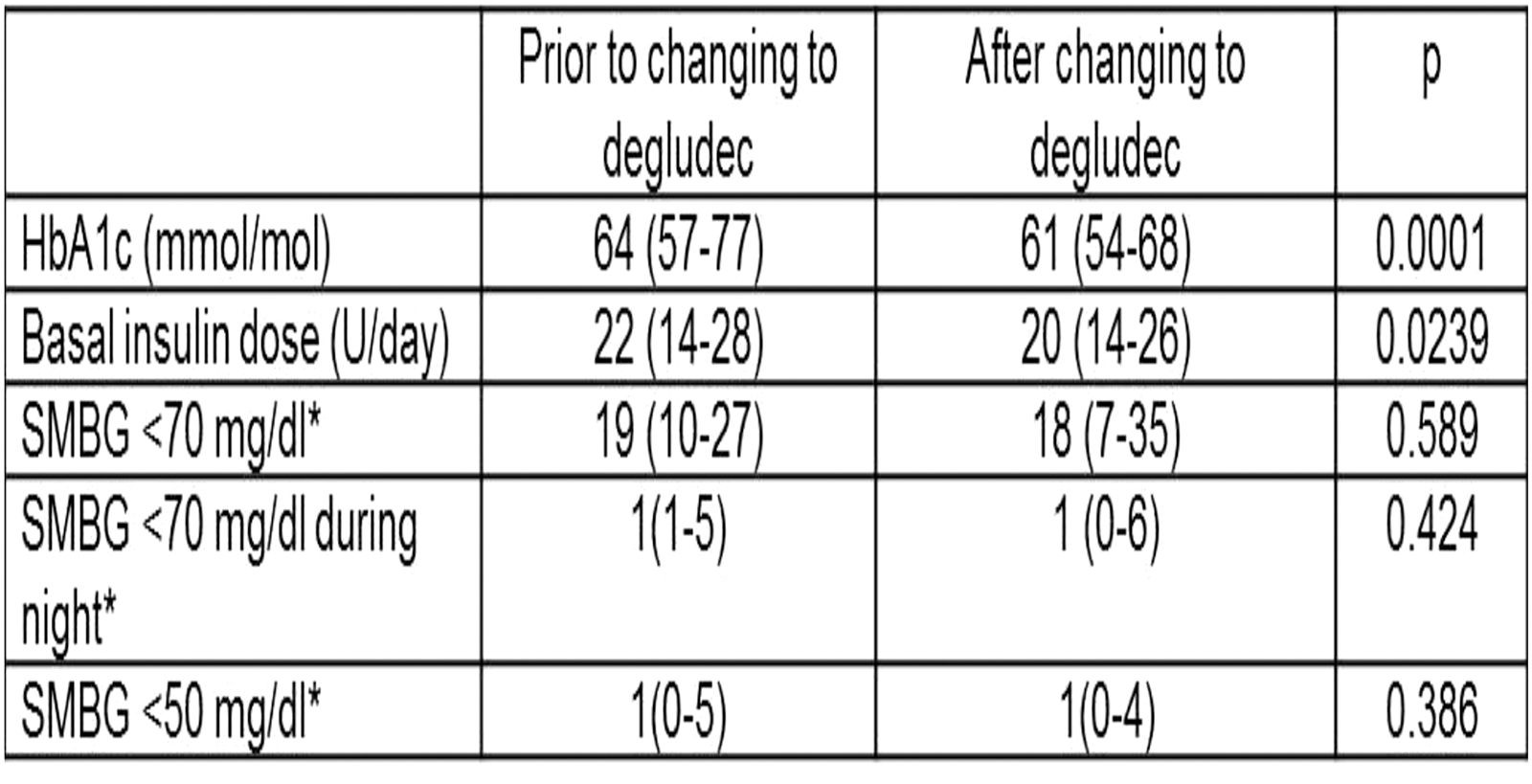
Profil, Neuss, Germany
Faster aspart demonstrated a greater early glucose-lowering effect within 2h post-dose than IAsp (Table); the greatest (2-fold) difference was within the first 30 min (LSmean, mg/kg: elderly 44.7 vs 21.4; younger adults 42.8 vs 20.5). PK/PD effects did not differ significantly between groups. Treatments were well tolerated; no safety issues were identified.
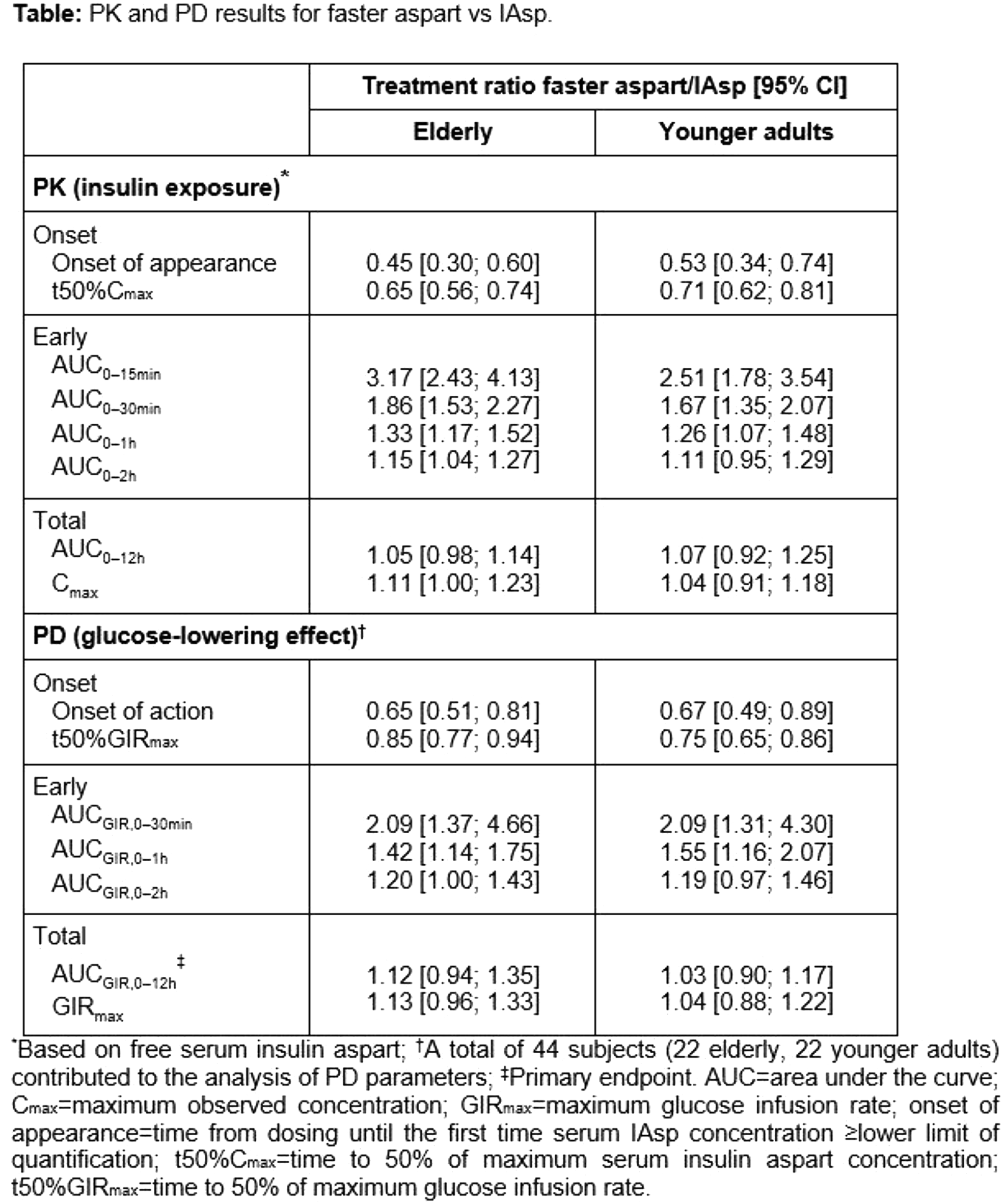
University of Sydney, Sydney Medical School, Sydney, Australia
Studies sponsored by Sanofi (NCT01499082, NCT01499095, NCT01676220)
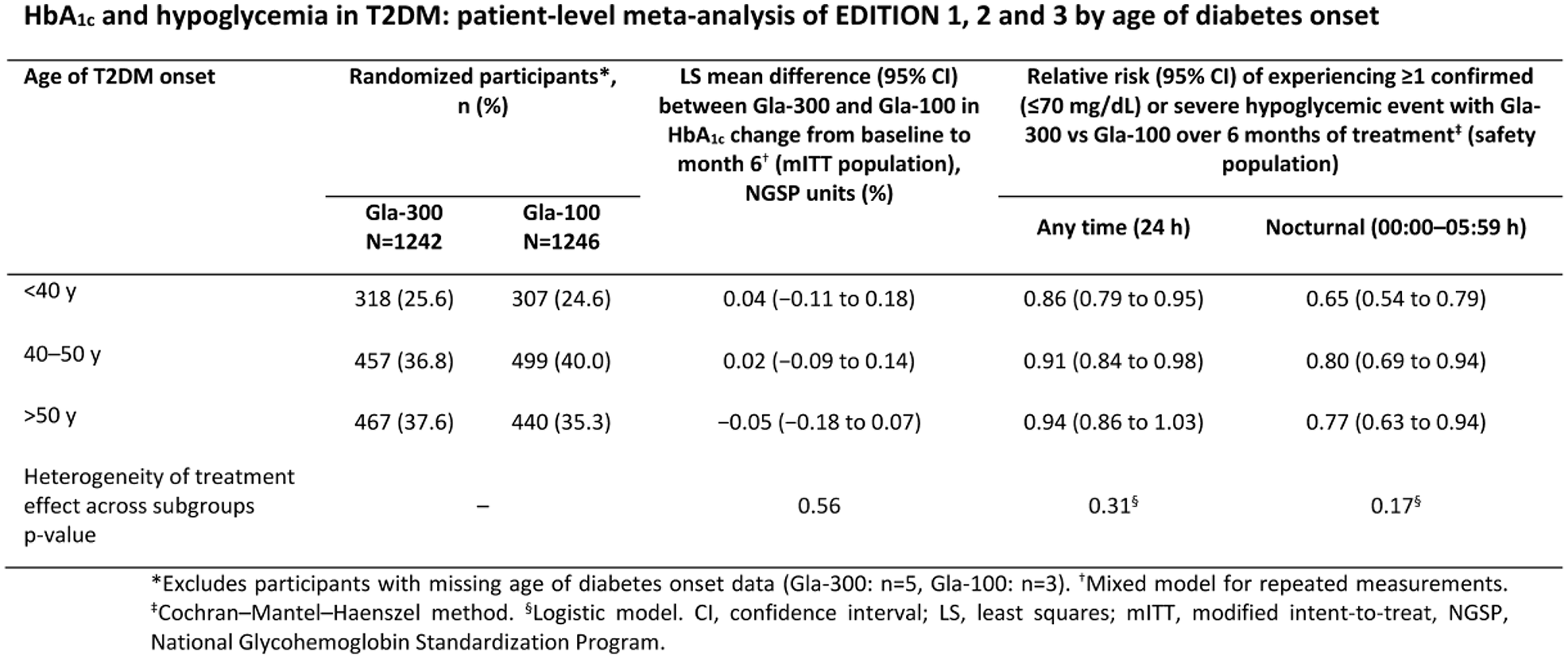
Oregon Health & Science University, Department of Medicine, Portland, USA
Studies sponsored by Sanofi (NCT01499082, NCT01499095, NCT01676220)

York University, School of Kinesiology and Health Science - Faculty of Health, Toronto, Canada

Second University of Naples, Department of Psychology, Caserta, Italy
IRCM Institut de recherches Cliniques de Montréal, Metabolic Diseases, Montréal, Canada
University of Colorado Anschutz, Barbara Davis Center for Diabetes, Aurora- CO, USA
During the subsequent 42 night RCT phase, we analyzed sensor use, skin reactions, errors, and why the experimental system was not used.
During the RCT, subjects 4-6 yo experienced more frequent and severe skin reactions (P = 0.02), while adult subjects (26-45 yo) wore individual sensors a median of 26 hours longer than the youngest subjects (P < 0.001). Technical problems with the sensor (errors, miscalibrations, etc.), traveling, and BG levels >270 at bedtime (study requirement) were primary contributors to non-system use.
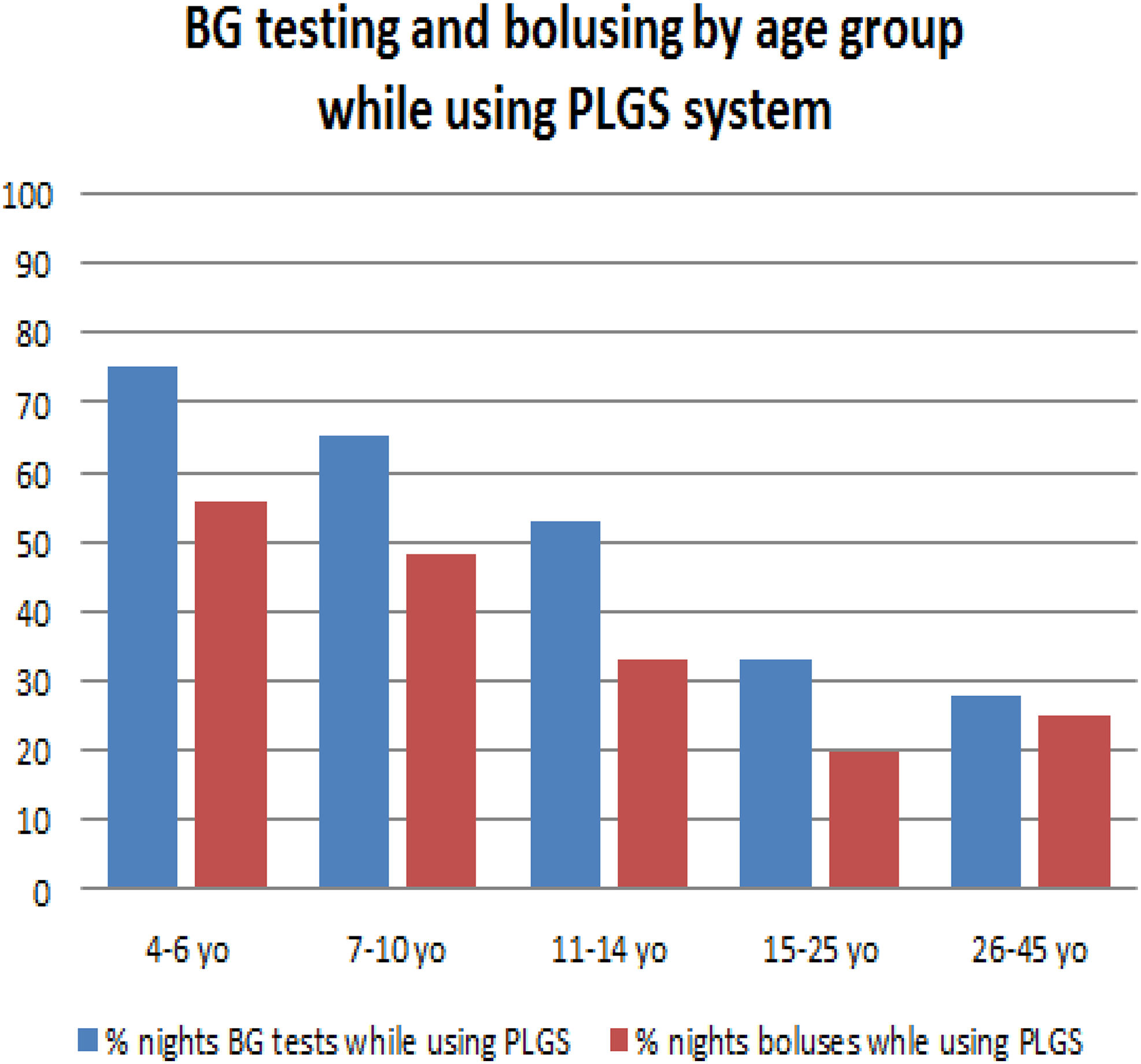
University of Cambridge Metabolic Research Laboratories, Institute of Metabolic Science, Cambridge, United Kingdom
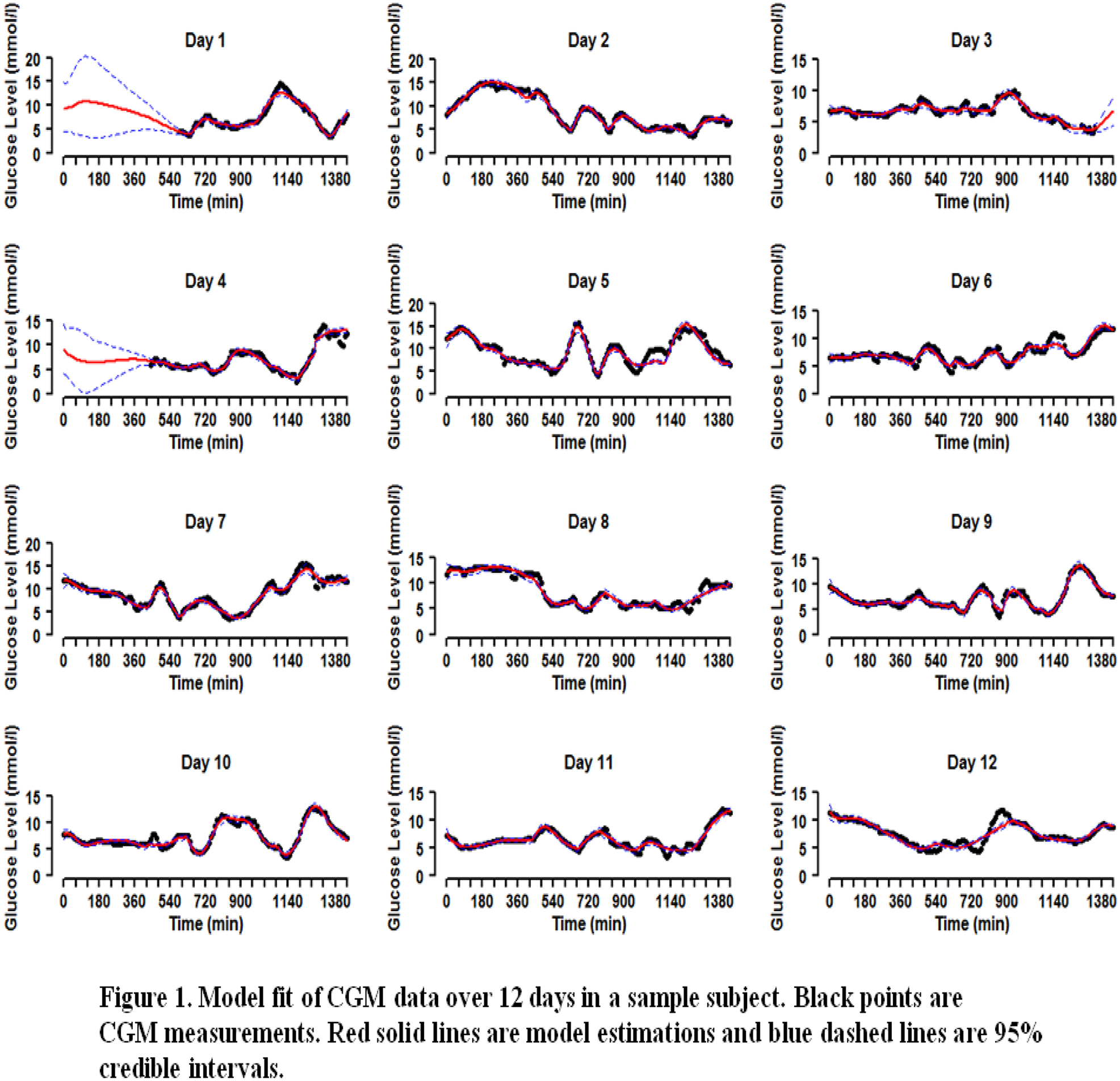
University of Virginia, Psychiatry and NB Sciences, Charlottesville, USA
Policlinico Universitario Gaetano Martino, Department of Clinical and Experimental Medicine, Messina, Italy
Diabetech- LP, Research & Development, Sausalito, USA
Academic Medical Center - University of Amsterdam, Department of Endocrinology, Amsterdam, Netherlands
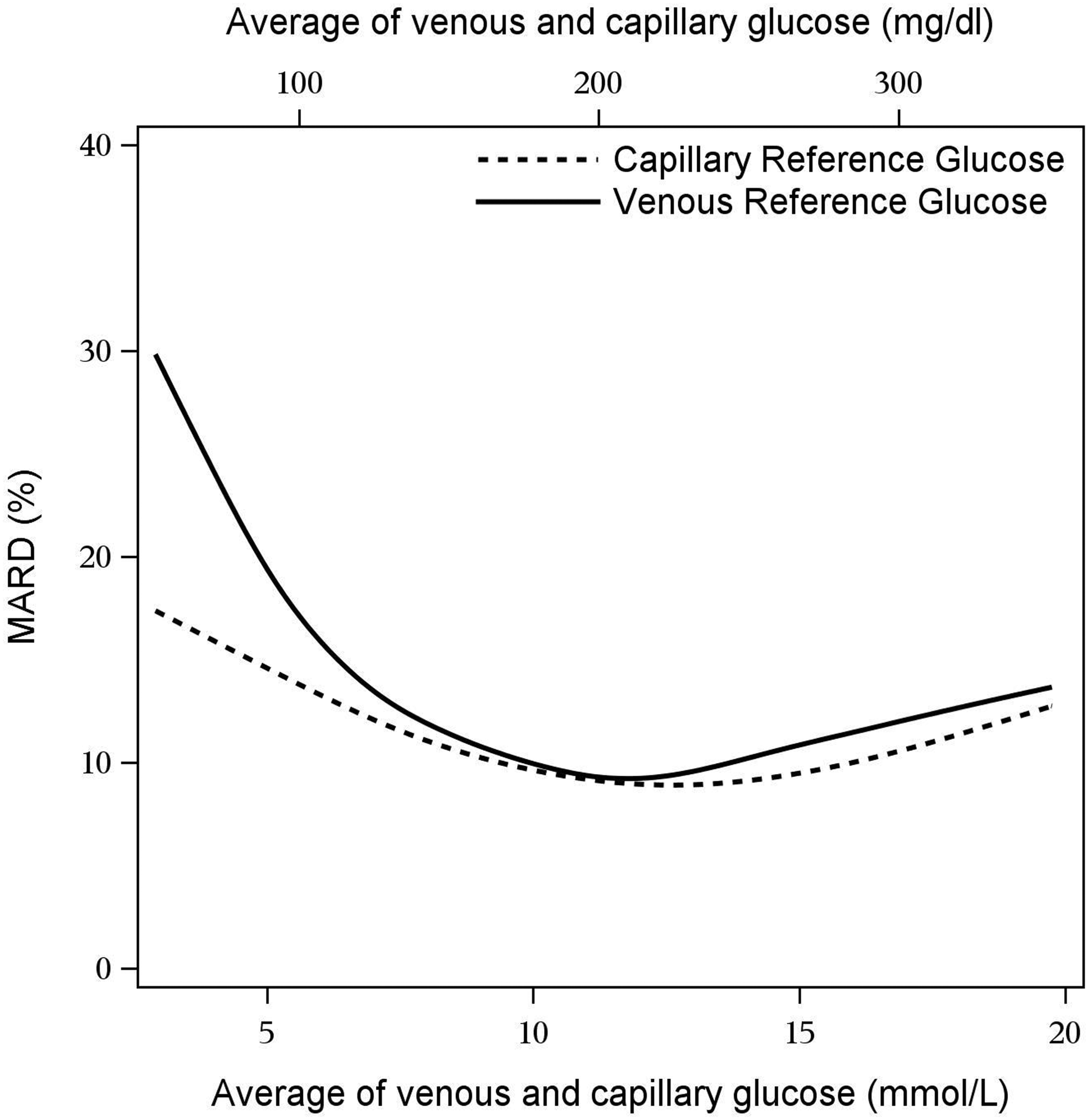
Dexcom Inc., San Diego, USA
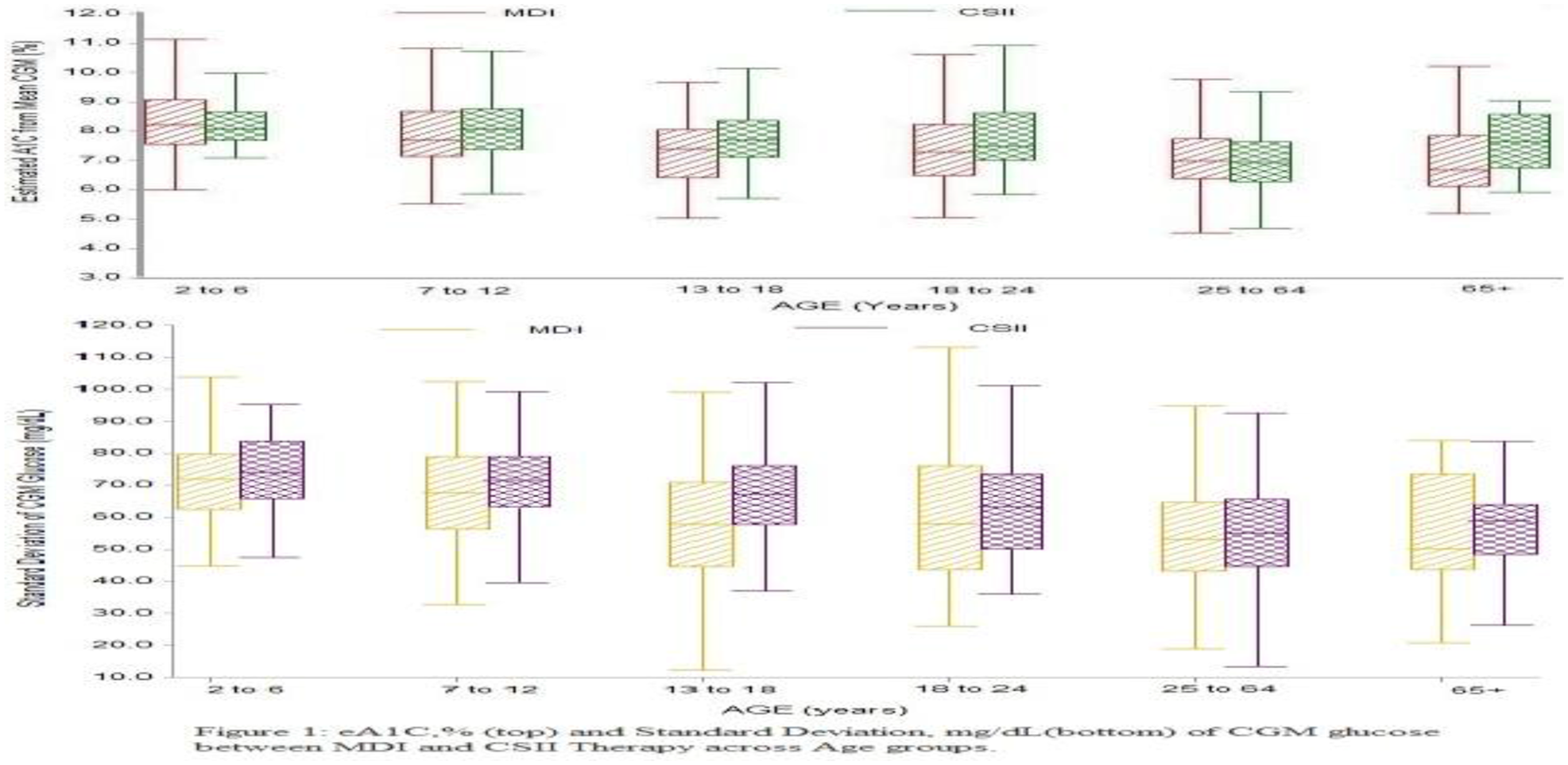
AMCR Institute Inc., Escondido CA, USA
AMCR Institute- Inc., Diabetes, Escondido, USA
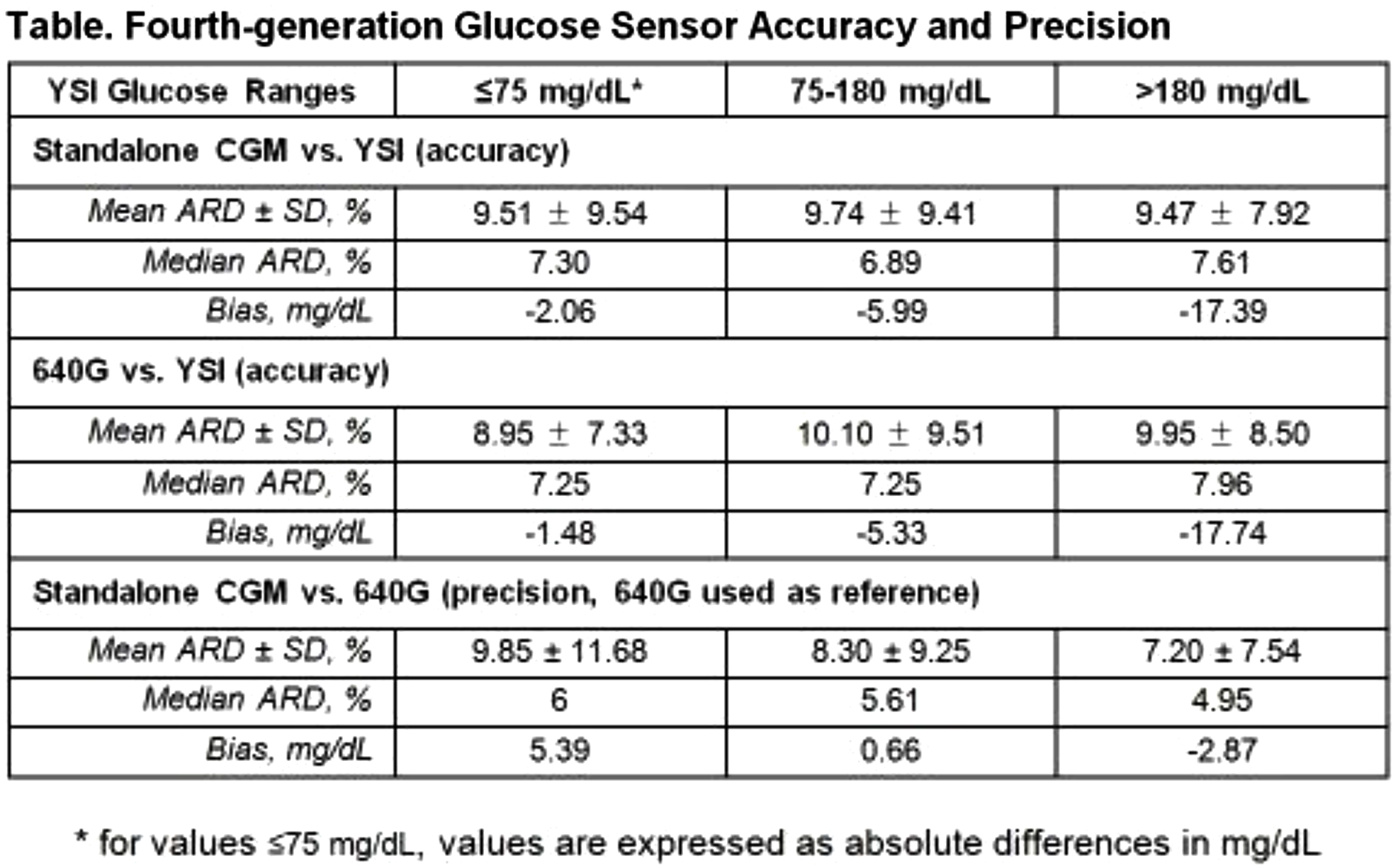
Medtronic, Diabetes, Northridge, USA
2nd School of Medicine - Charles University and University Hospital Motol, Department of Internal Medicine, Prague, Czech Republic
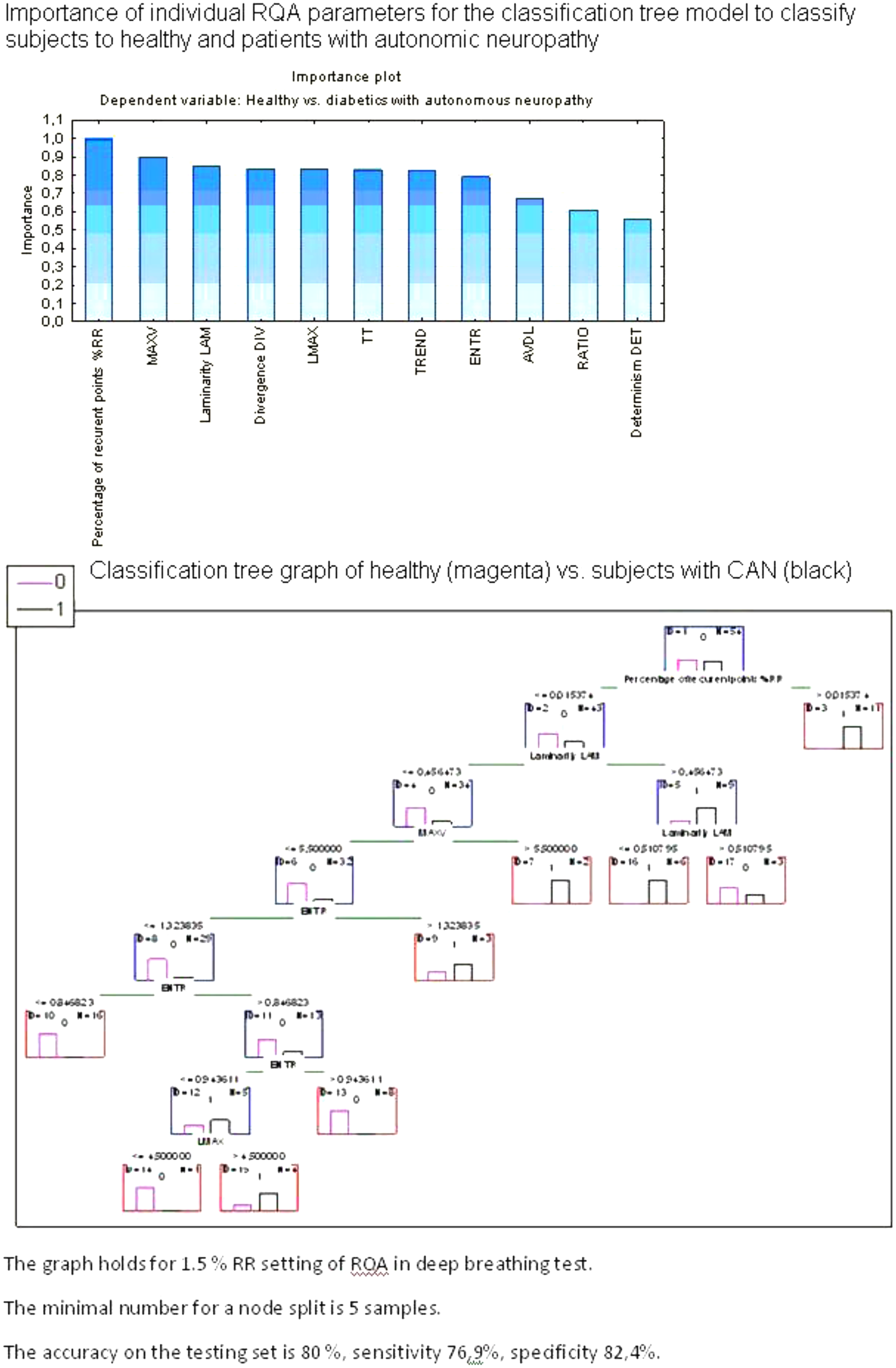
Hôpital Européen de Paris GVM Care Research, Seine St Denis, Aubervilliers, France
We gained success in these patients with GIBP with prolonged selected intra venous (IV) rather than enteral antibiotherapy
Patients (n = 75), aged 44 to 92, were included from october 2013 to april 2015
PEDIS 3 to 4 - IDSA moderate to severe - UT 3C 3D
All had a deficient bone structure on clinical (probe bone test) or imaging basis (Xr, CTscan, MRI).
Loco regional anesthesia (n = 43) or none (n = 32) were proposed.
Patients had GIPB (n = 3) being still diabetic.
We had no complication and 100 % success in bacterial retrieval.
Gram +68% gram – 28% anaerobie 4%.
IV broad spectrum antiobiotherapy was given in first intention.
Selected enteral antibiotherapy after bacterial identification were prescribed afterwards.
Follow up was done at one, three and six months.
Soft tissu infection and biological degradation were patent.
As the same antibiotherapy was effective with IV, it was prolonged 4 to 6 weeks.
Long term IV antibiotherapy should be discussed for patient with GIBP.
Yeungnam University School of Medicine, Department of Internal Medicine, Daegu, Republic of Korea
Endocrinology Research Center, Diabetic Foot Clinic, Moscow, Russia
Illinois Institute of Technology, Chemical and Biological Engineering and Biomedical Engineering, Chicago, USA
Imperial College London, EEE, London, United Kingdom
Centre Hospitalier Sud-Francilien, Essonnes, Corbeil-Essonnes, France
The aim was to determine how many patients would wish to have an AP after receiving detailed system information.
Most of the patients expressed a desire to have an AP. following this information, their desire was greater, and with the number of patients feeling it was extremely likely that they would have an AP in place of their insulin-pump rising from 24% to 41%.
Logistical-regression-analysis suggests that the desire to have an AP is determined by 2 factors: the recency of onset of T1D(OR = 0.94/year of duration; p = 0.014) and ongoing treatment with pump therapy vs. multiple daily injections (OR = 0.26;p = 0.058). Dissatisfaction with current therapy, the hope of improved HbA1c-levels or decreased-risk-of-hypoglycaemia or associated complications, the hope of improved freedom or comfort, and the length of time needed to develop the device did not appear to be significantly correlated with hopes about AP.
Montreal Institute of Clinical Research, Diabetes, Montreal, Canada
National Chung Cheng University, Department of Chemical Engineering, Chiayi, Taiwan
University of Twente, NIKOS, Enschede, Netherlands
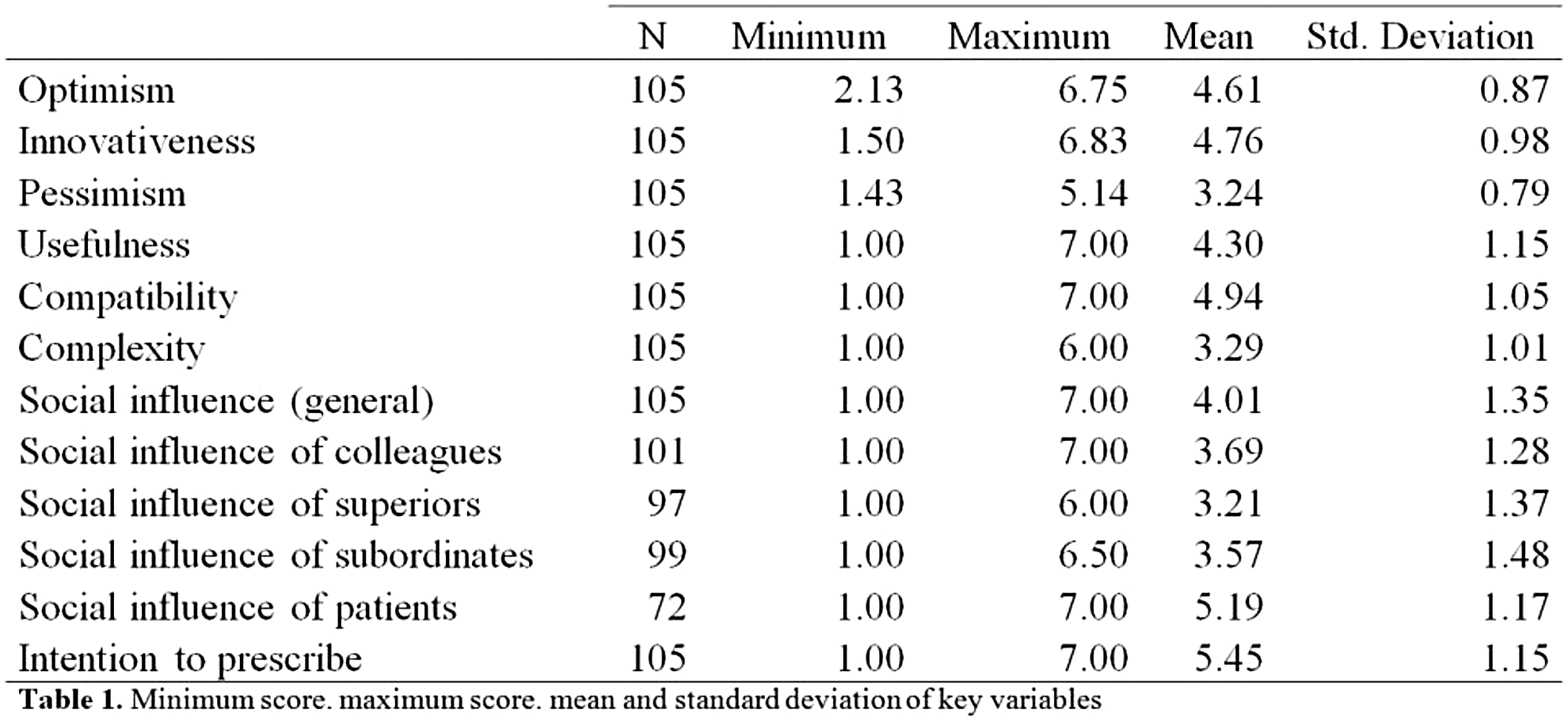
Institut d'Informàtica i Aplicacions, Universitat de Girona, Girona, Spain
This work aims to develop a new methodology for automatically detecting exercise that only requires data from a continuous glucose monitor (CGM) and the insulin delivered to the subject.
University of Padova, Department of Information Engineering, Padova, Italy
The aim of this work is to use CGM and subcutaneous insulin delivery (CSII) to adapt patient CR to follow physiological and/or behavioral changes.
National YunLin University of Science and Technology, Information Management, Douliu, Taiwan
University-Hospital of Padua, Department of Woman's and Child's Health - Neonatal Intensive Care Unit, Padova, Italy
Endocrinology Research Center, Epidemiology, Moscow, Russia
Determination of the correlation between average daily blood glucose excursion and manifestation/progression of DR during 20 year period.
Imperial College London, Electrical and Electronic Engineering, London, United Kingdom
The UVa-Padova T1DM Simulator v3.2 was used to validate the proposed technique. The 10 adult virtual subjects over a 1-week scenario were used for testing purposes. The proposed coordinated strategy was evaluated against an uncoordinated version of the same controller. Results are expressed as mean ± SD.
Sheba medical center, Institute of Endocrinology, Ramat Gan, Israel
Mehr Medical Group, Internal Medicine/Gynecology, Tehran, Iran
In contrast to conventional practice where insulin is delivered whenever it is needed (high BS), we deliver insulin whenever it is most effective (when the first derivative changes its slop direction) so that very low doses can accomplish huge jobs.
Mehr Medical Group, Internal Medicine/Gynecology, Tehran, Iran
Mason Clinic, Seattle, USA
Forty (40) system incidents, resulting in missed automated insulin doses, occurred in 17 Daily Living clinical studies in the CRC. In each case, because the ADMC was not yet implemented, the on site engineer had to intervene and manually restore closed-loop dosing.
Port of Spain, Trinidad and Tobago
It has been shown that an exogenous bolus of adrenaline causes increased plasma glucose levels mainly due to gluconeogenesis, a compensatory increase in insulin secretion, and a counterintuitive reduction in glucose uptake by body cells.
Johannes Kepler University of Linz, Institute for Design and Control of Mechatronical Systems, Linz, Austria
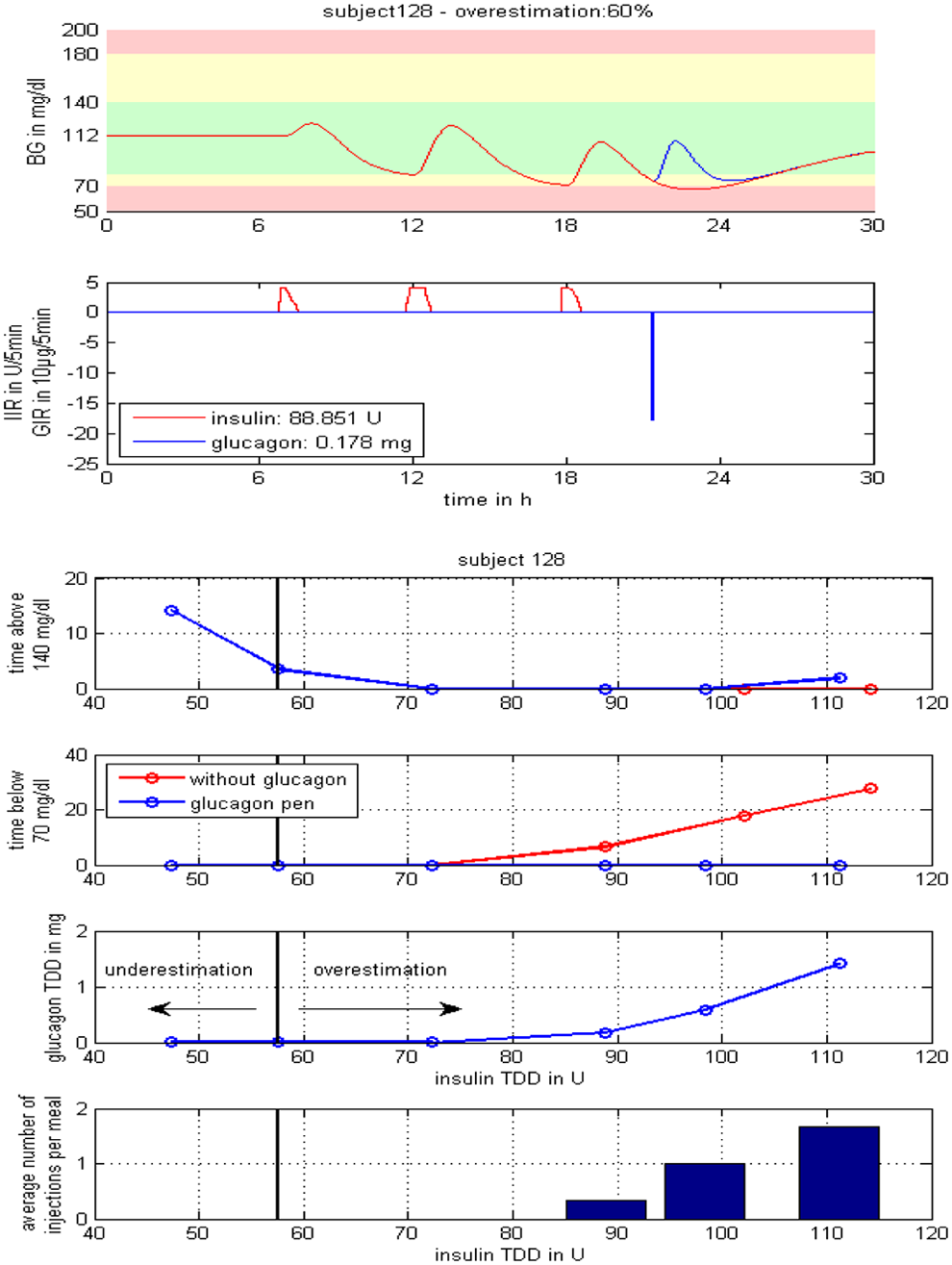
Medtronic, Inc., R&D, Northridge, USA
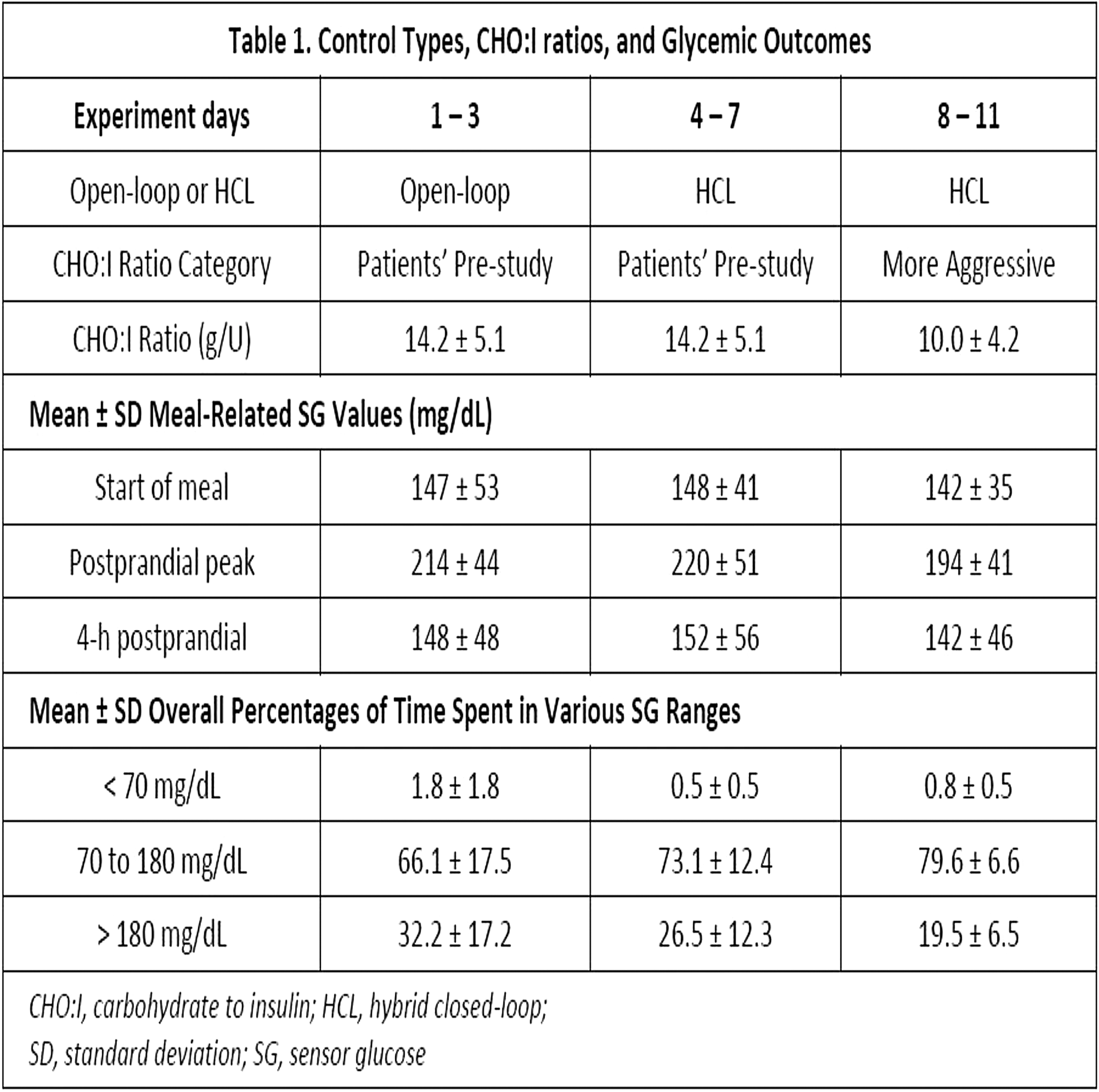
Imperial College, Department of Diabetes, Endocrinology & Metabolism, London, United Kingdom
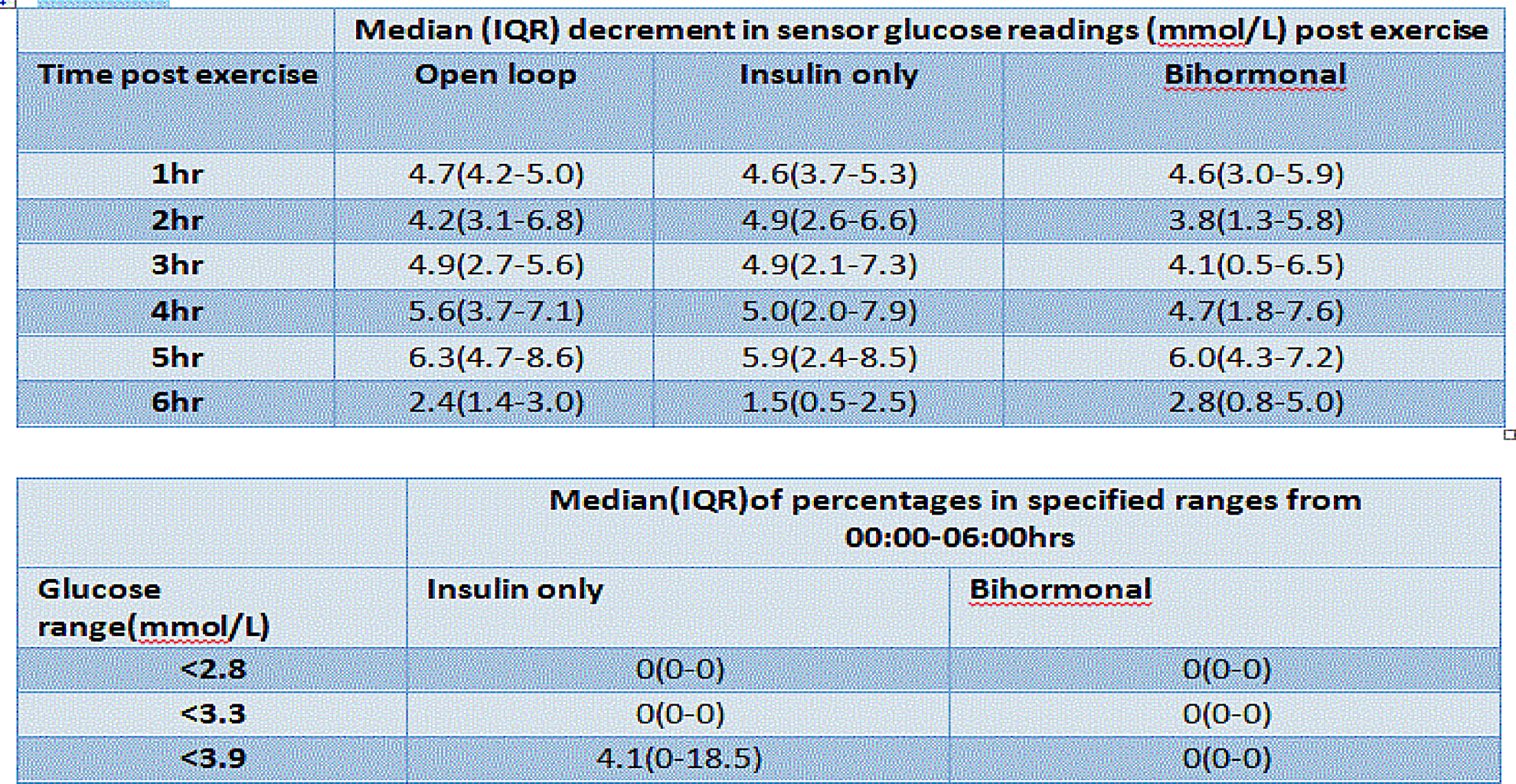
Imperial College, Department of Diabetes, Endocrinology & Metabolism, London, United Kingdom
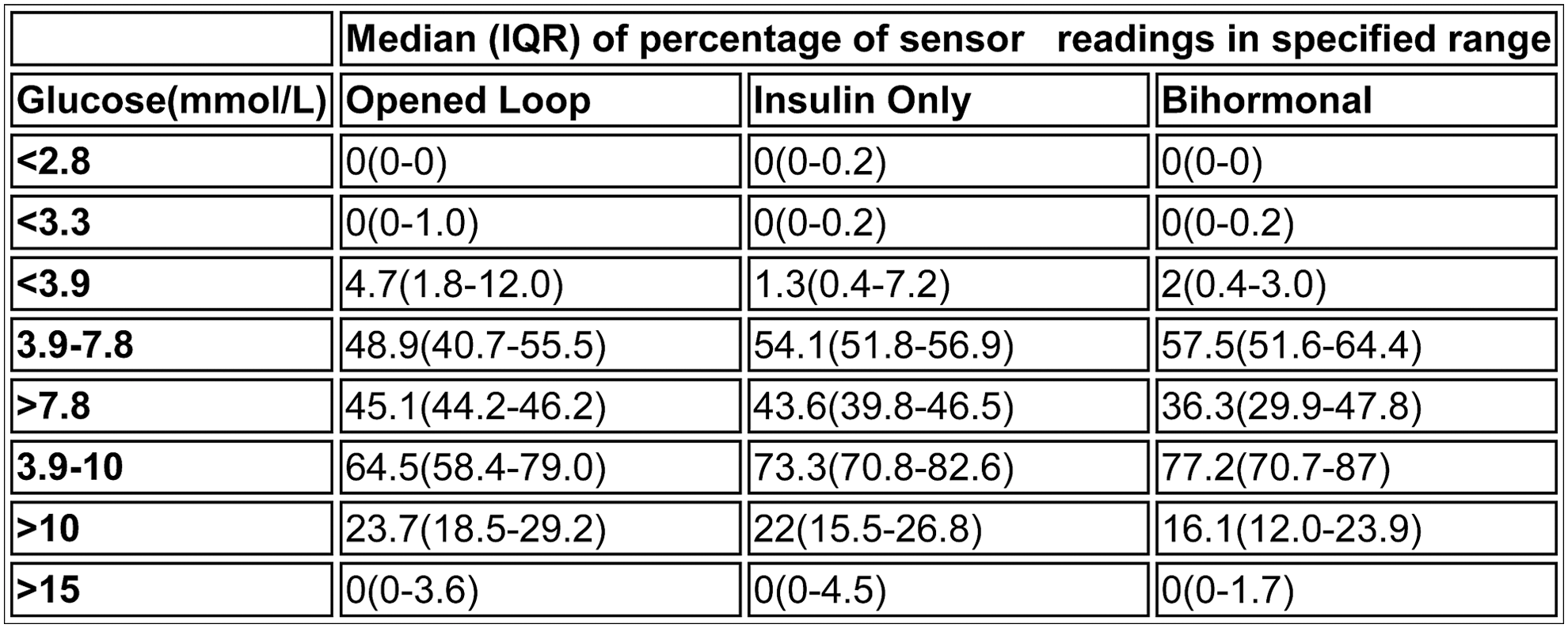
Lund University, Department of Automatic Control, Lund, Sweden
A nonparametric modeling approach using a combined pharmacokinetic/pharmacodynamics model was used to estimate the insulin action of the rapid-acting insulin and the IR for each patient. The IR estimate was allowed to change in-between days.
University of Cambridge Metabolic Research Laboratories, Institute of Metabolic Science, Cambridge, United Kingdom
Medtronic - Inc., Diabetes, Northridge, USA
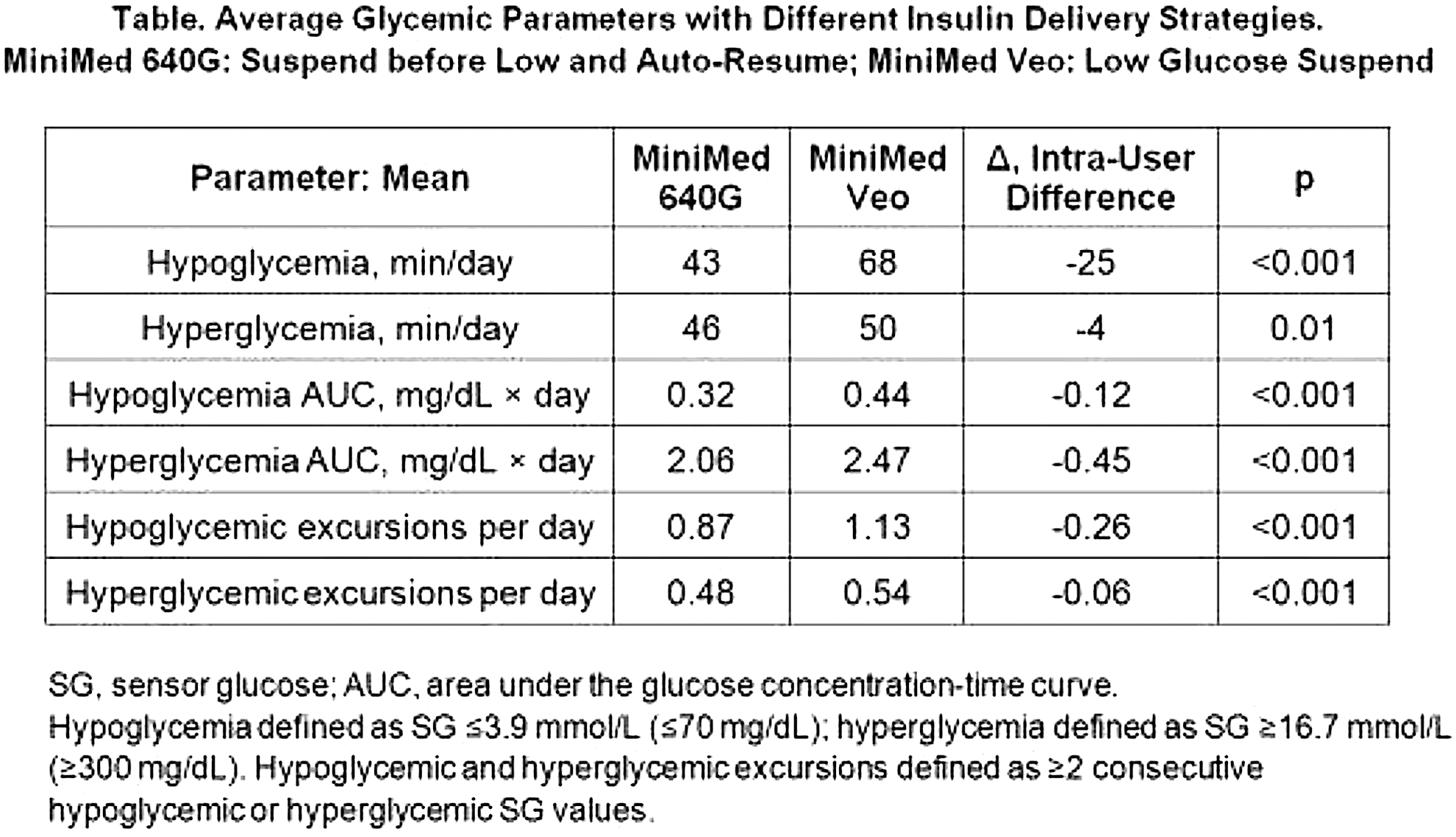
Medtronic - Inc., Diabetes, Northridge, USA
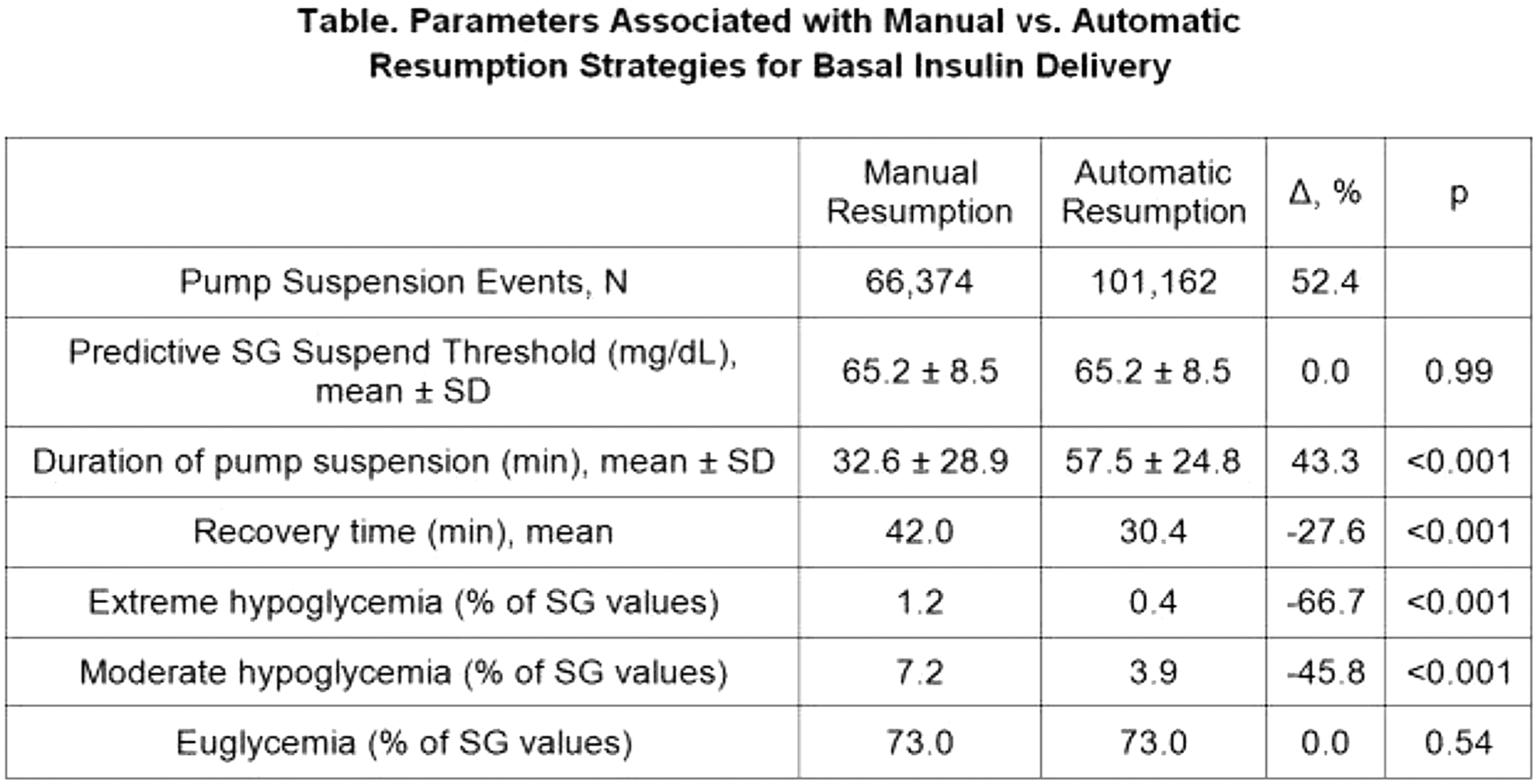
Medtronic - Inc., Diabetes, Northridge, USA
Polytechnic Institute of Viseu, Health School, Viseu, Portugal
To identify feelings experienced by parents after the child diagnosis and reflect on the influence of care provided by health professionals in the acceptance and adaptation to diabetes.
University Hospital of North Norway, Norwegian Centre for Interated Care and Telemedicine, Tromsø, Norway
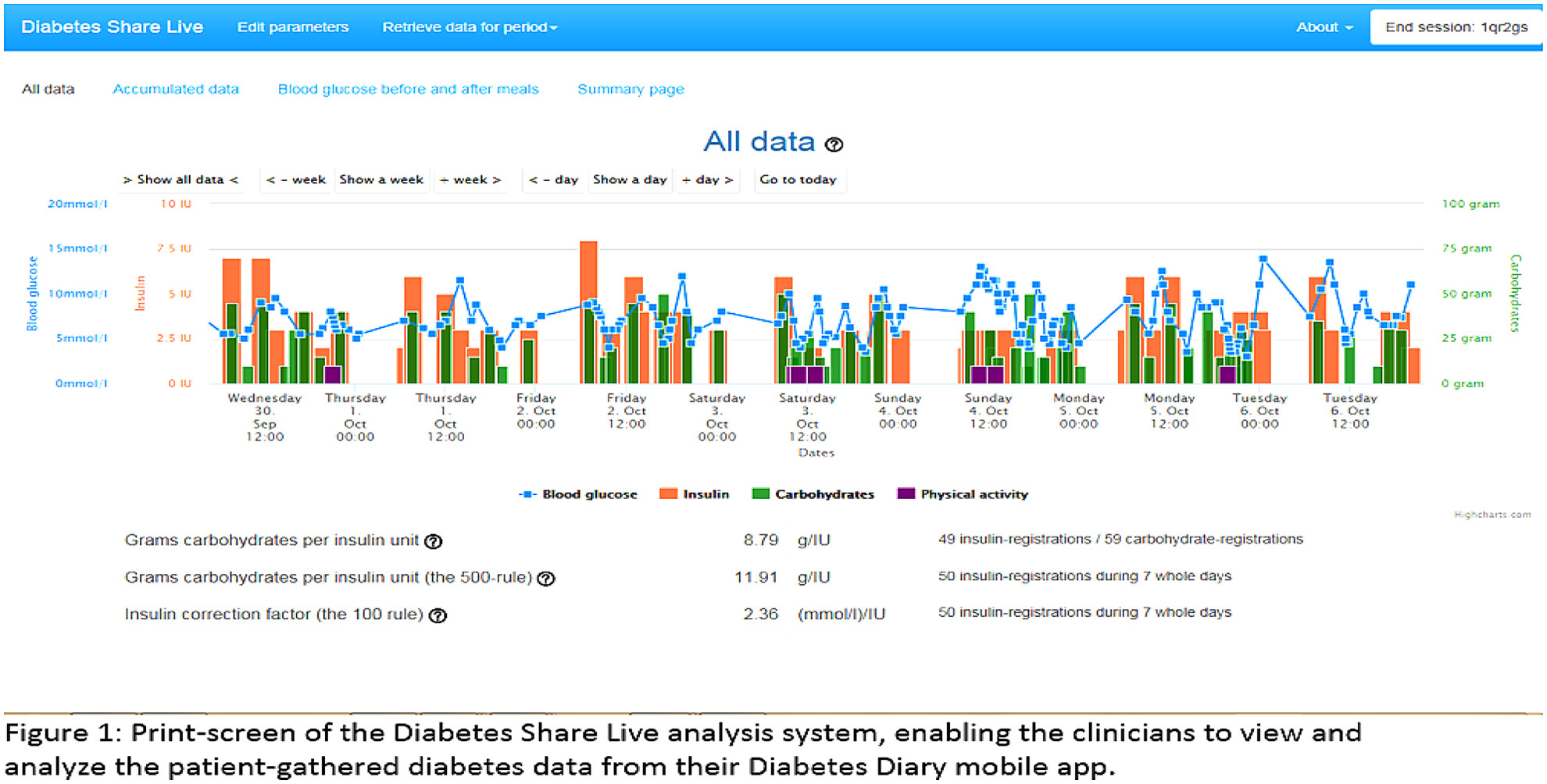
Moscow Regional Research and Clinical Institute MONIKI, Endocrinology department, Moscow, Russia
The aim of this research is to develop methods for assessment of cutaneous blood microcirculation in patients with type 2 diabetes (DM) using LDF. The best way of doing this is reducing the variability of measurements and increasing the difference between healthy and ill individuals.
Institute of Public Health, Research Unit of general practice, Odense, Denmark
The aim of this study is to describe and analyze the variation in use of POCT of HbA1c among diabetes patients in Danish general practice and municipalities.
Riga East Clinical University Hospital, Clinic of cardiovascular diseases, Riga, Latvia
Aim: to compare twenty-four hours HRV parameters in patients with T2DM and without and with CARTs in DM patients.
UERN, INFORMATIC, Mossoró, Brazil
Kazan State Medical University, Therapy, Kazan, Russia
Institute of Clinical Research Center- NHO Kyoto Medical Center, Department of Preventive Medicine, Kyoto, Japan
Seoul National University, College of Pharmacy, Seoul, Republic of Korea
Comenius University and University Hospital, 2nd Department of Internal Medicine, Bratislava, Slovakia
To retrospectively assess the association of the orthostatic hypotension (OH) with macrovascular and microvascular complications of diabetes mellitus and to determine its effect on mortality.
Samara Children's Hospital 1, Endocrinology, Samara, Russia
Thammasat University, Preclinical Science, Pathumthani, Thailand
After 6 weeks of treatments, the fasting blood glucose, serum insulin, serum leptin, intraperitoneal glucose tolerance test (IPGTT), serum lipid profile, hepatic glycogen content, and hepatic lipogenic genes and gluconeogenic enzyme protein expression were determined.
Pirogov National Medical University, Internal Medicine, Vinnitysa, Ukraine
Institute of Nutrition of Russian Academy of Sciences, Department of Metabolic Diseases, Moscow, Russia
University of Padova, Information Engineering, Padova, Italy
Prince Sultan Military Medical City, Diabetes Treatment Center- Department of Endocrinoloy and Diabetes, Riyadh, Kingdom of Saudi Arabia

Bournemouth University, Faculty of Health & Social Sciences, Bournemouth, United Kingdom
Bournemouth University, Faculty of Health & Social Sciences, Bournemouth, United Kingdom
CGM Impact Scale results show 86%(n = 44) of participants reported feeling better (14% neutral) about their diabetes control with 90% CGM naïve participants and 81% experienced CGM users reporting increased confidence about their diabetes. As well as 73% (n = 37) feel more safe (27% neutral) while sleeping and 78% (n = 39) are confident (22% neutral) about avoiding serious hypoglycemia. Previous CGM users showed the same results as first time CGM users (p = 0.45). Responses correspond with an average improvement in HbA1c from 7.51 to 7.05 (p < .0001) over the 90 days use of the CGM. Eighty-four percent (84%) would choose to be inserted again.
Diabetes related distress data was comparable for all participants with no deterioration associated with implantable CGM use. 93% of first time users and 77% experienced CGM users would like to continue using the system to help manage their diabetes more effectively.
Hospital Clínic, Laboratorio Core, Barcelona, Spain
a) ≥95% of the results must be within ±15% of the analyzer results (entire range).
b) ≥99% of the results must be within ±20% (entire range).
a) ≥95% of the results must be within either ±12 mg/dL of the analyzer result, for samples <100 mg/dL, or ±12.5% for samples ≥100 mg/dL.
b) ≥2% of results present differences >20% when glucose is ≥75 mg/dL or >15mg/dL when glucose is <75 mg/dL.
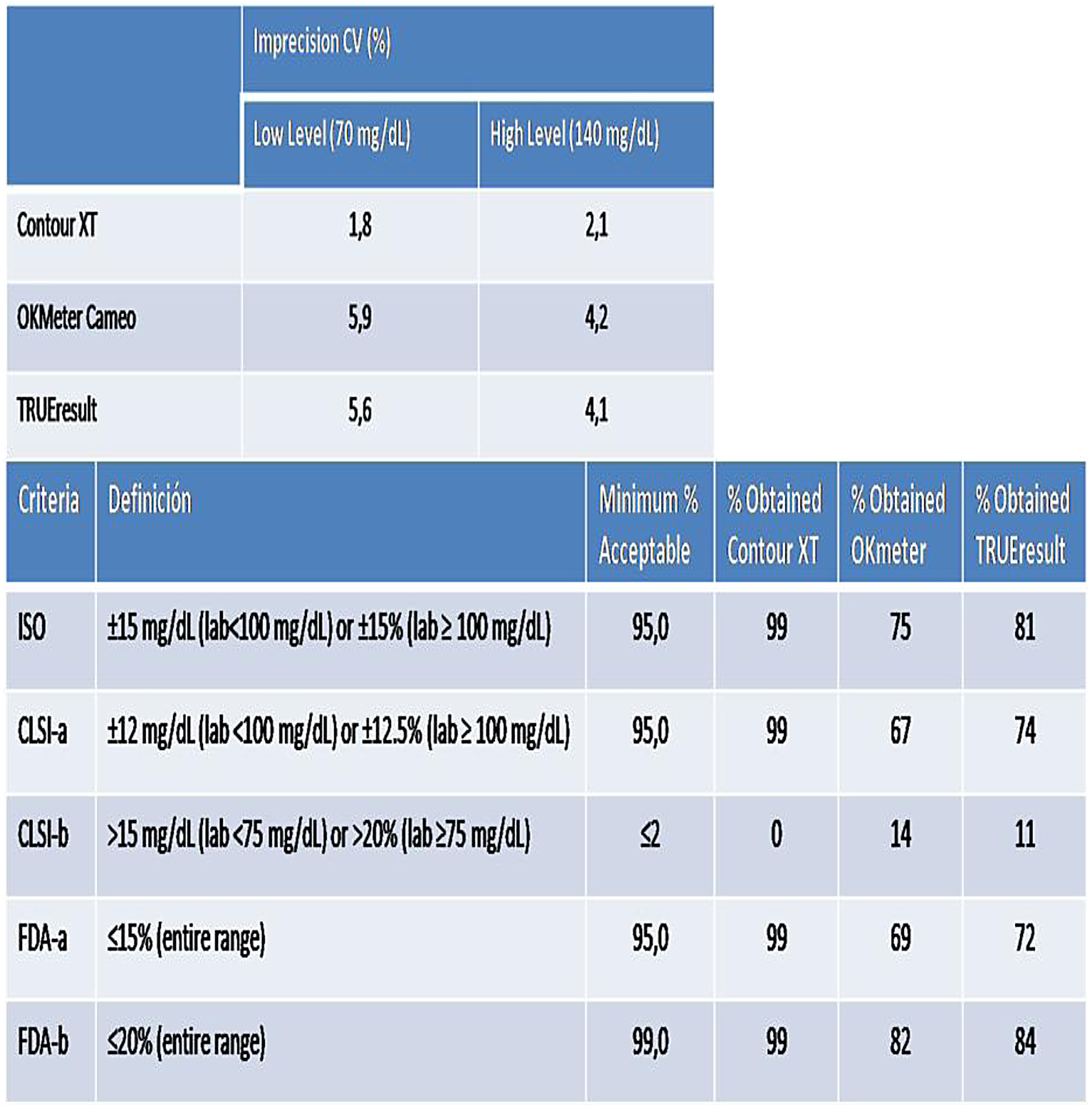
Second Medical Faculty- Charles University, Department of Internal Medicine, Prague, Czech Republic
Abbott Diabetes Care, Alameda, USA
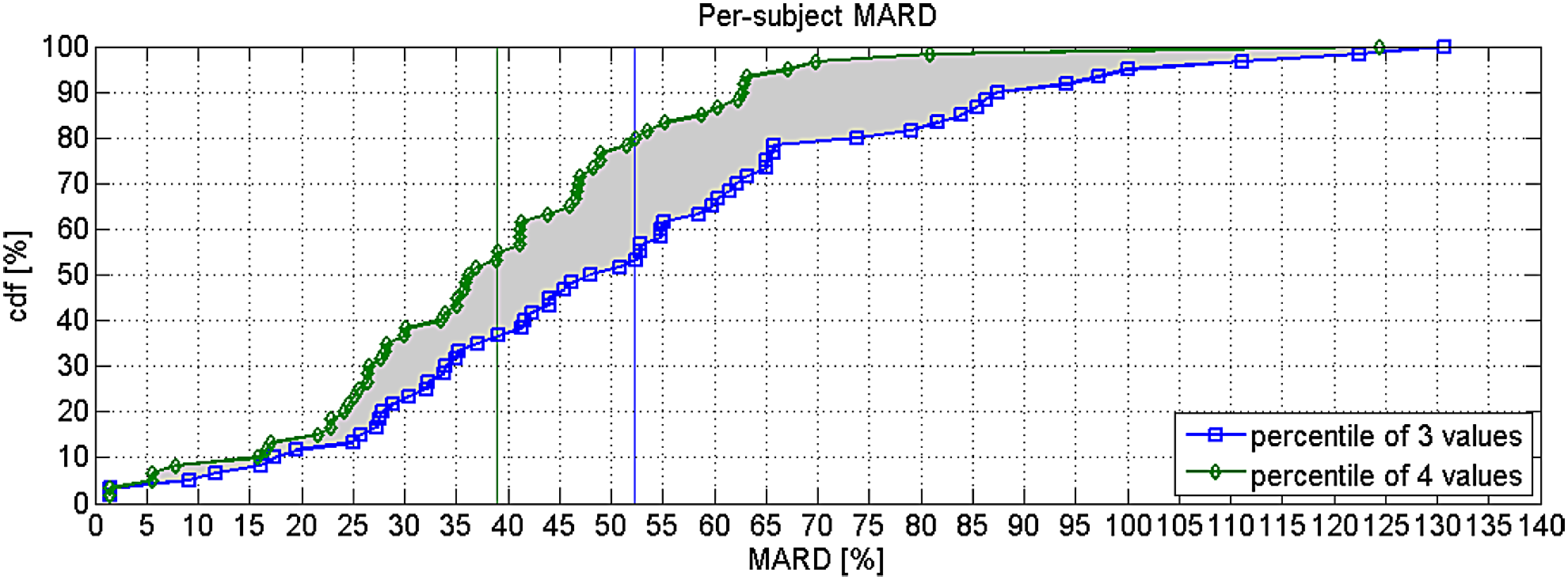
Trondheim University Hospital, Dept of Endocrinology, Trondheim, Norway
Hospital Regional Universitario, Endocrinología, Málaga, Spain
Our objective was to evaluate metabolic control and adherence to SAP therapy 7 years after initiation of SAP in a clinical trial.
Imperial College London, Diabetes- Endocrinology & Metabolic Medicine, London, United Kingdom
The majority of adult patients with current or previous experience in CGM (64%) ranked cost as the top limitation to CGM use. This was followed by lack of accuracy (21%). This order was reversed for the children group, where CGM inaccuracy was ranked as the most important limitation (43%) followed by cost (28%) (Figure 1). Further analysis revealed that 33.3% of adult respondents from North America ranked cost as the top limitation compared to 67.7% in UK.
These findings were confirmed by qualitative data analysis.
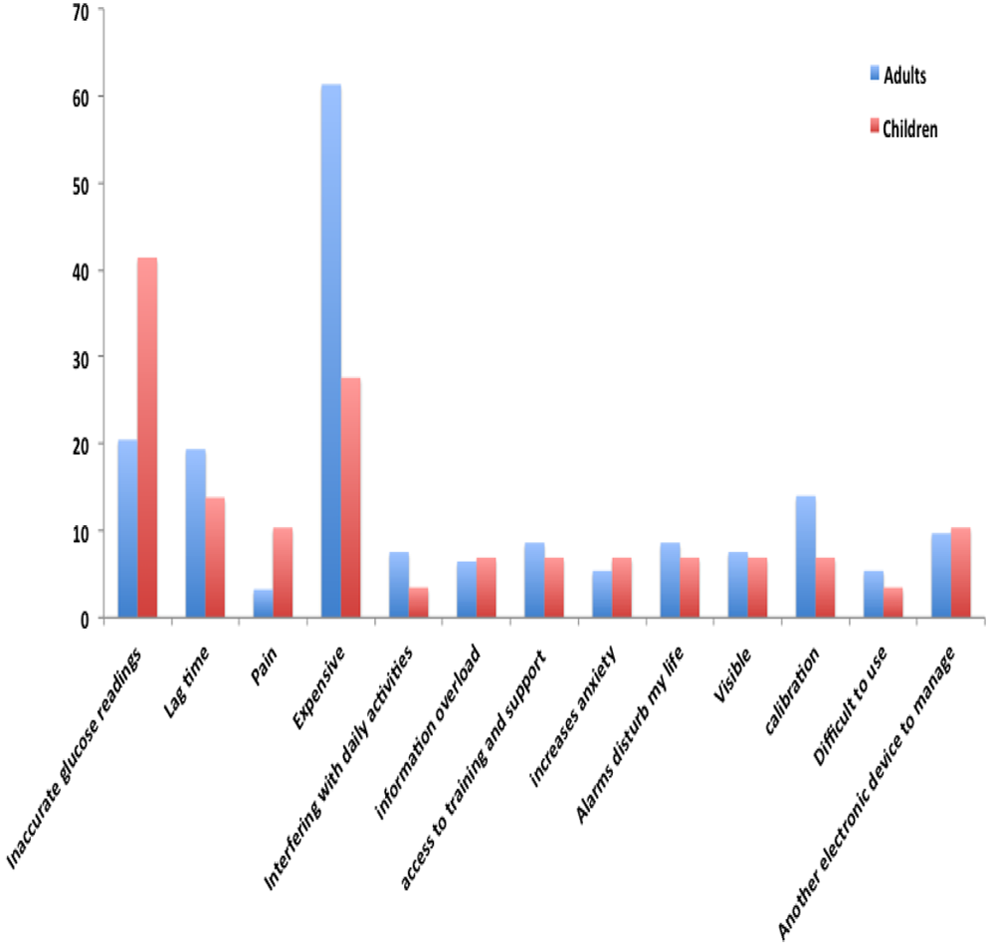
University of Colorado Denver, Barbara Davis Center, Aurora, USA

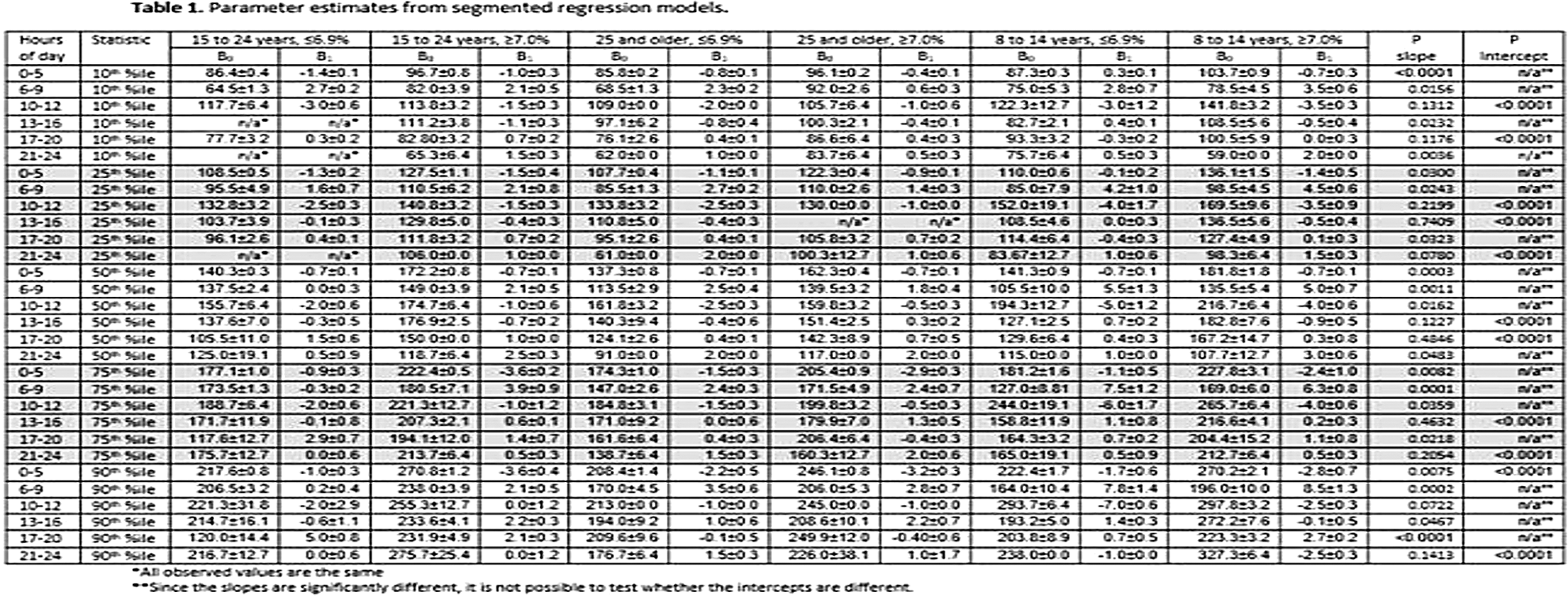
University of Virginia, Psychiatry and NB Sciences, Charlottesville, USA
Diabetes Zentrum Mergentheim, Diabetes Klinik, Bad Mergentheim, Germany
Pre-specified secondary outcome measures included; SMBG frequency, quality of life measurements and safety analysis.
Diabetes-Treatment-Satisfaction Questionnaire (DTSQ) showed increased overall treatment satisfaction for intervention vs. control (13.1 ± 0.50 (adjusted mean±SE) vs. 9.0 ± 0.72 (p < 0.001)). Diabetes Quality of Life (DQoL) also showed increased treatment satisfaction for intervention vs. control (-0.2 ± 0.04 (adjusted mean±SE) vs. 0.0 ± 0.06 (p = 0.0259)).
During FreeStyle Libre wear (intervention (6 months) and control group (4 weeks, masked)) there were; 158 occurrences of skin symptoms/sensor-insertion events (e.g. mild pain, bruising, itching, erythema), normally expected with device use. There were 9 instances of device-related adverse events (e.g. infection, allergy) from 6 subjects. No device-related serious adverse events were reported.
Integrity Applications Ltd., R&D, Ashkelon, Israel
Dexcom, R&D, San Diego, USA
Jothydev's Diabetes Research Centre, Diabetes, Thiruvanathapuram, India
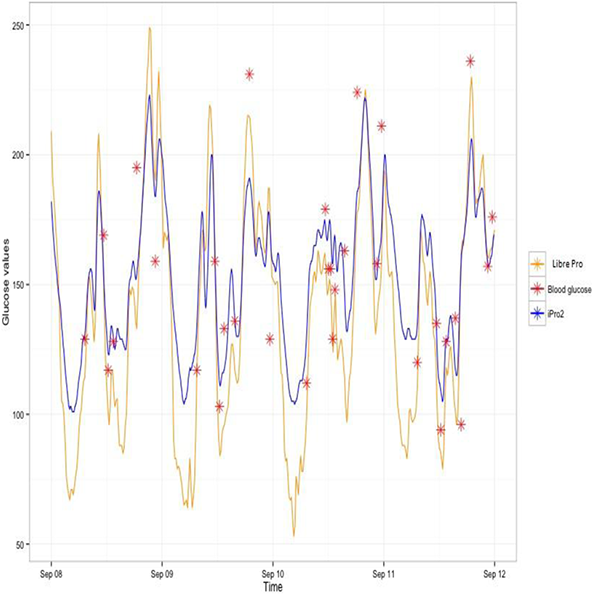
University Children's Hospital, Endocrinology & Genetics, Skopje, FYR Macedonia
Continuous glucose monitoring system (CGMS) might help in defining the daily glucose profile in children with IGT detected on OGTT. It might also be a useful tool for follow up of children and adolescents with IGT.
Body mass index correlated well with insulinemia (p < 0.001), but not with the peak glycemia (p = 2.1). Peak glycemia was in correlation with the HOMA index (p = 0.03). Four children (14.3%) developed overt DM2 within five years of follow up, all at the age >12 years. Repeated CGMS profiles were predictive of worsened metabolic control.
Academic Medical Center - University of Amsterdam, Department of Endocrinology, Amsterdam, Netherlands
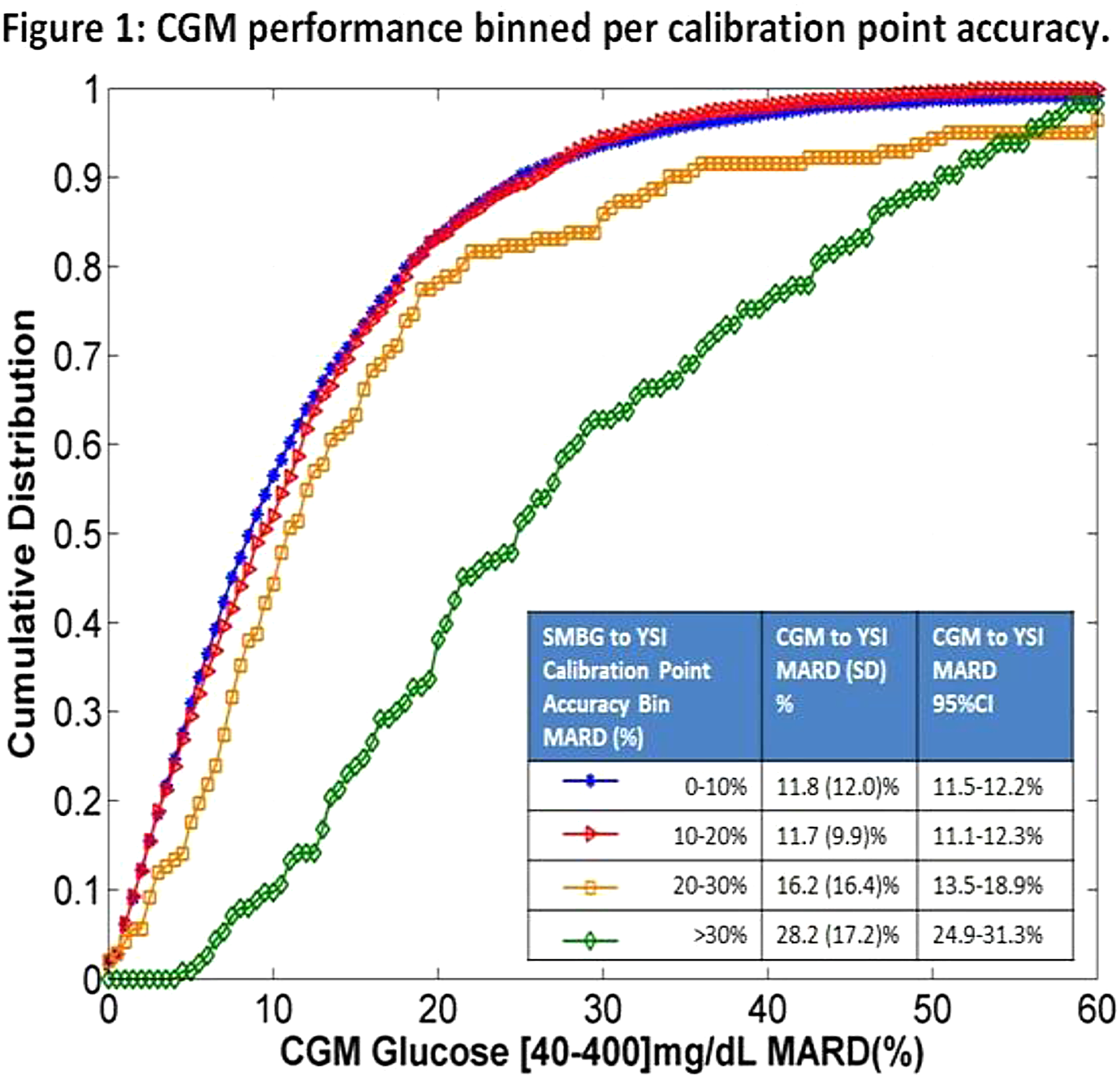
The University of Tokushima, Diabetes Therapeutics and Research Center, Tokushima, Japan
To investigate accuracy and time delay of CGM and AP in comparison with PG during hyperglycemic and euglycemic glucose clamp conditions.
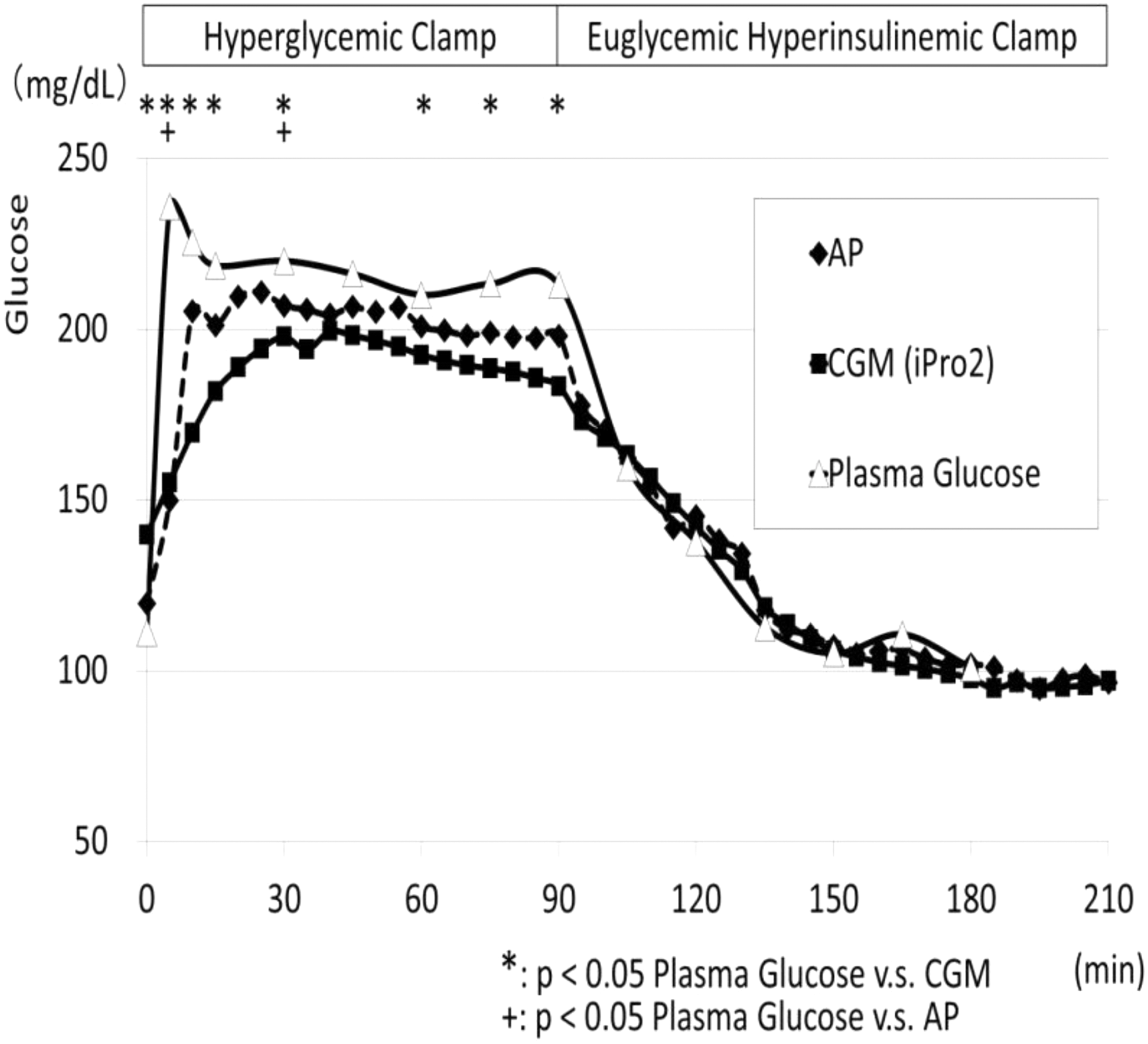
University of Padova, Department of Information Engineering, Padova, Italy
Centro Hospitalar e Universitário de Coimbra, Serviço de Endocrinologia- Diabetes e Metabolismo, Coimbra, Portugal
MIMOS Berhad, Photonics R&D, Kuala Lumpur, Malaysia
Diablo Clinical Research, Walnut Creek CA, USA
Pediatric Hospital “Giovanni XXIII”, Metabolic Diseases- Clinical Genetics and Diabetology, Bari, Italy
Universitary Hospital Santiago de Compostela, Endocrinology and Nutrition Service, Santiago de Compostela, Spain
The inclusion criteria to start SAP therapy were high glycemic variability (GV) or at least 1 episode of several hypoglycemia (SH) in the year before the initiation of treatment with sensor in real time.
We analyzed glycemic control and hypoglycemia events at baseline and after 1 year of follow up in the whole sample and separated by inclusion criteria (GV and SH). Furthermore we evaluated the use of the sensor.
Glycemic control data, hypoglycemic events and use of sensor are shown in Table 1.
The main cause of disruption of the monitoring was the unavailability of the sensors (hypoglycemia group) and patient's decision (glycemic varibility group).
In patients with high glycemic variability SAP therapy improved the metabolic control with a significant decrease of SD.
Patients of the SH group used the sensor more than the GV group.
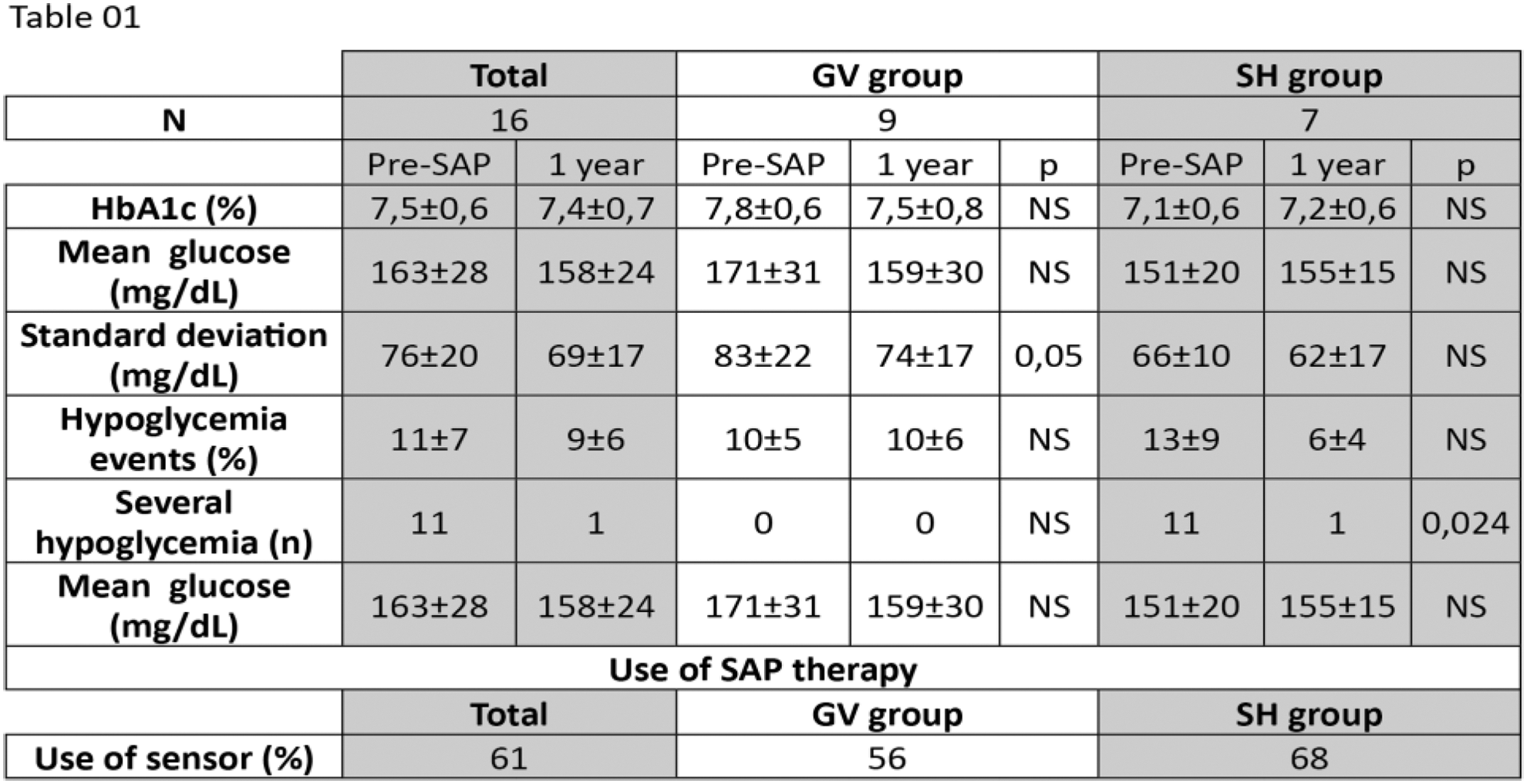
Pfützner Science & Health Institute, Diabetes Center and Practice, Mainz, Germany
Ascilion AB, R&D, KISTA, Sweden
The sensing method is based on radio frequency (RF) spectroscopy where the complex permittivity changes are measured using a resonant cavity sensor. The concept of glucose measuring using RF spectroscopy was proven both on macroscopic prototypes (cm-scale) and on a miniaturised low-cost MEMS chip.
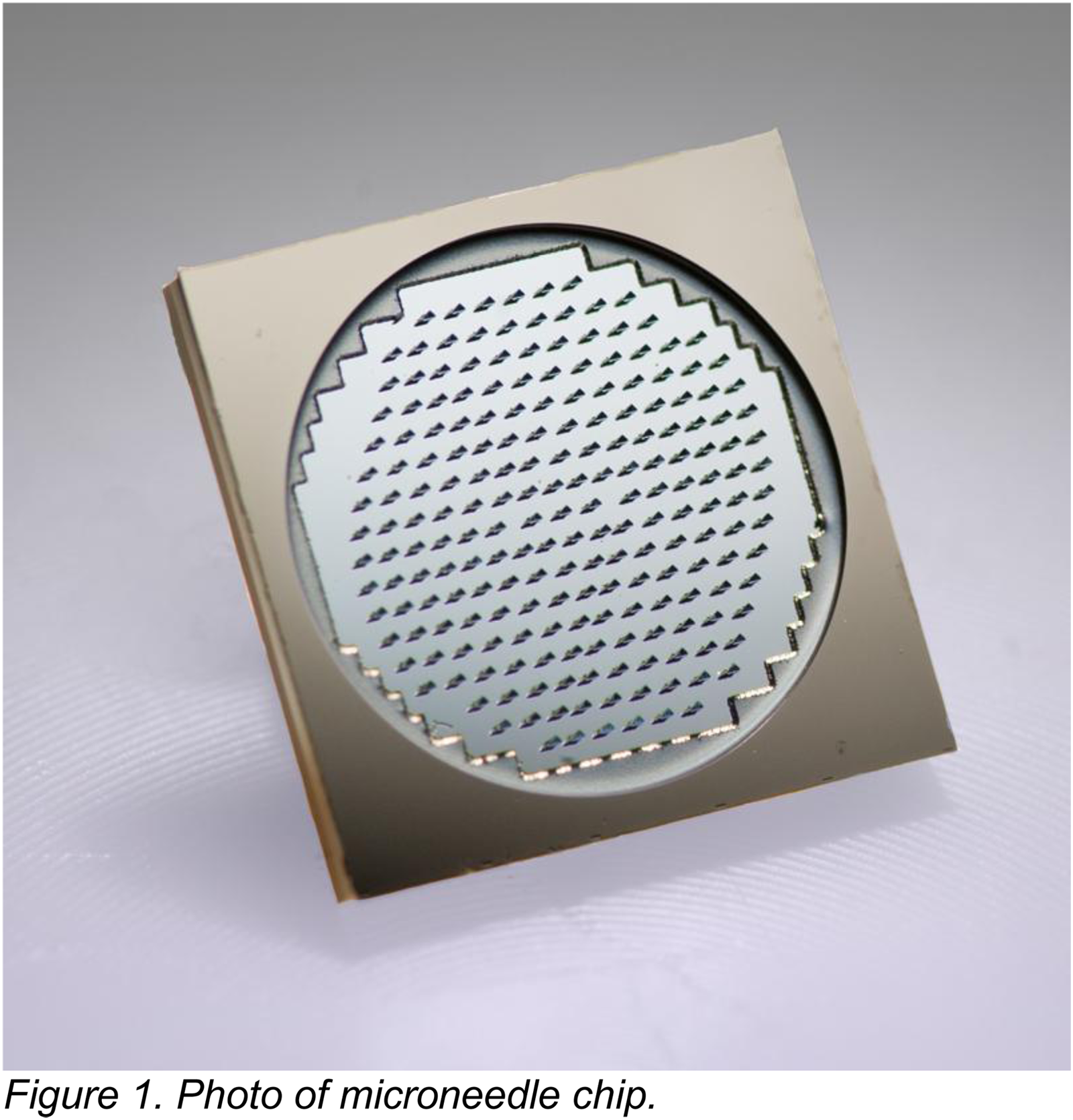
“Elias” Emergency University, Department of Endocrinology- Diabetes and Metabolic Diseases, Bucharest, Romania
HEVA HEOR, Health Economics, Lyon, France

Zagazig University- Faculty of Medicine, Internal Medicine, Zagazig, Egypt
Charles University - 2nd Faculty of Medicine and University Hospital Motol, Dpt.of Internal Medicine, Prague, Czech Republic
Supported by the Czech Ministry of Health Project No.15-25710A(P08 panel).
CHRU Brest, Endocrinology-Diabetology, Brest, France
CHRU Brest, Endocrinology-Diabetology, Brest, France
National Scientific Medical Research Center, Endocrinology Department, Astana, Kazakhstan
University of Padova, Department of Information Engineering, Padova, Italy
Chaim Sheba Medical Center, Diabetes, Ramat Gan, Israel
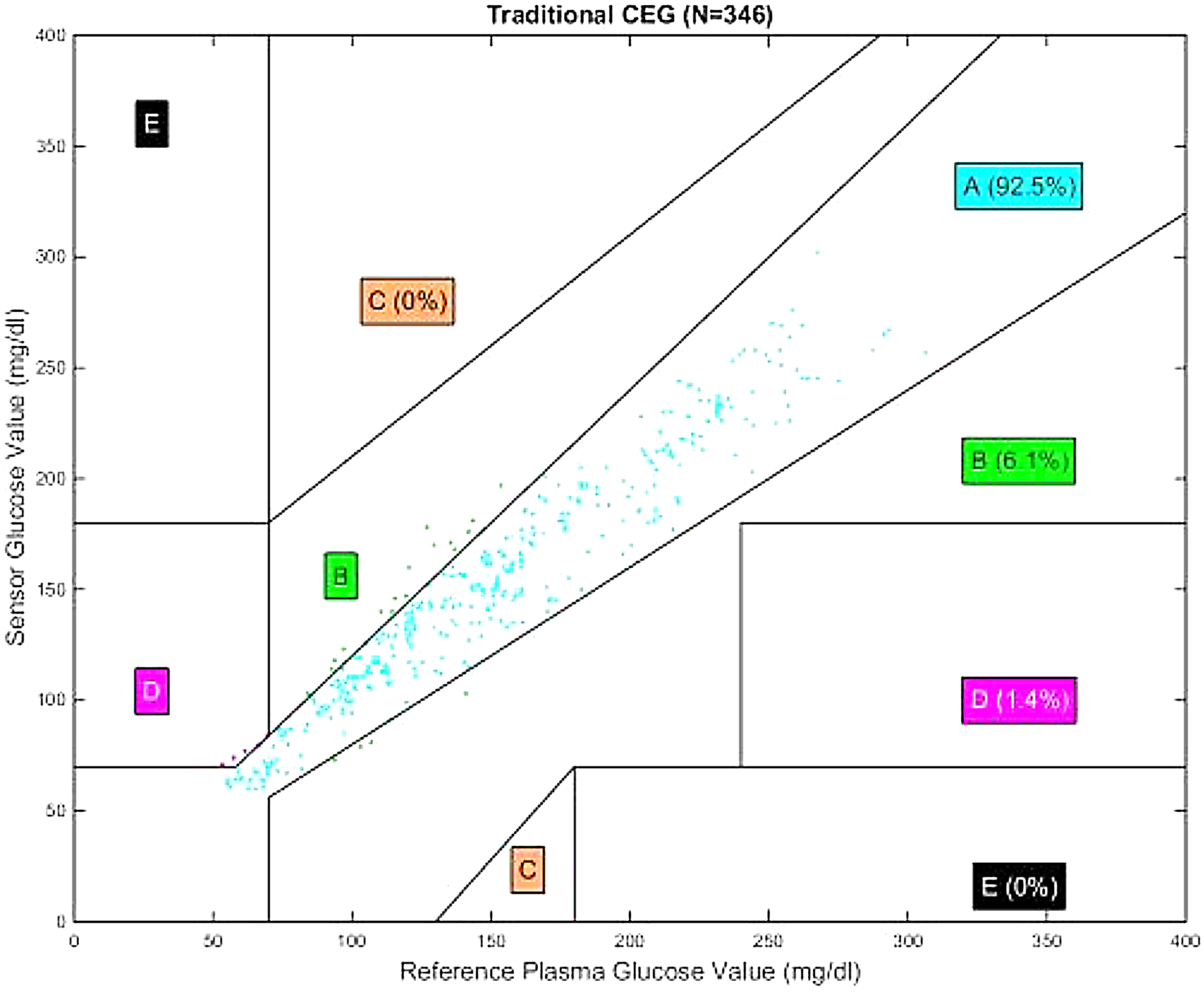
University of Texas at Houston Health Science Center, Pediatric Endocrinology, Houston, USA
• 16 yrs female T1DM
• HbA1C 12.8%
• Reported FBSs: 100-200 mg/dl
The patient admitted using the control solution provided with her home blood glucose meter to do the tests, instead of using her own blood.
• 18 yrs female T1DM
• HbA1C 13.2%
• Download of glucometer normal FBSs below 110 mg/dl
Her boyfriend admitted “offering himself” to use his blood test on the glucometer to make her feel better about diabetes.
1- Technology/device: Evaluate malfunction
2- Human aspect/persons involved or witnessing testing: Perform testing under the supervision of the healthcare provider and explore the possibility of false testing.
Hvidovre University Hospital, Department of Endocrinology, Hvidovre, Denmark
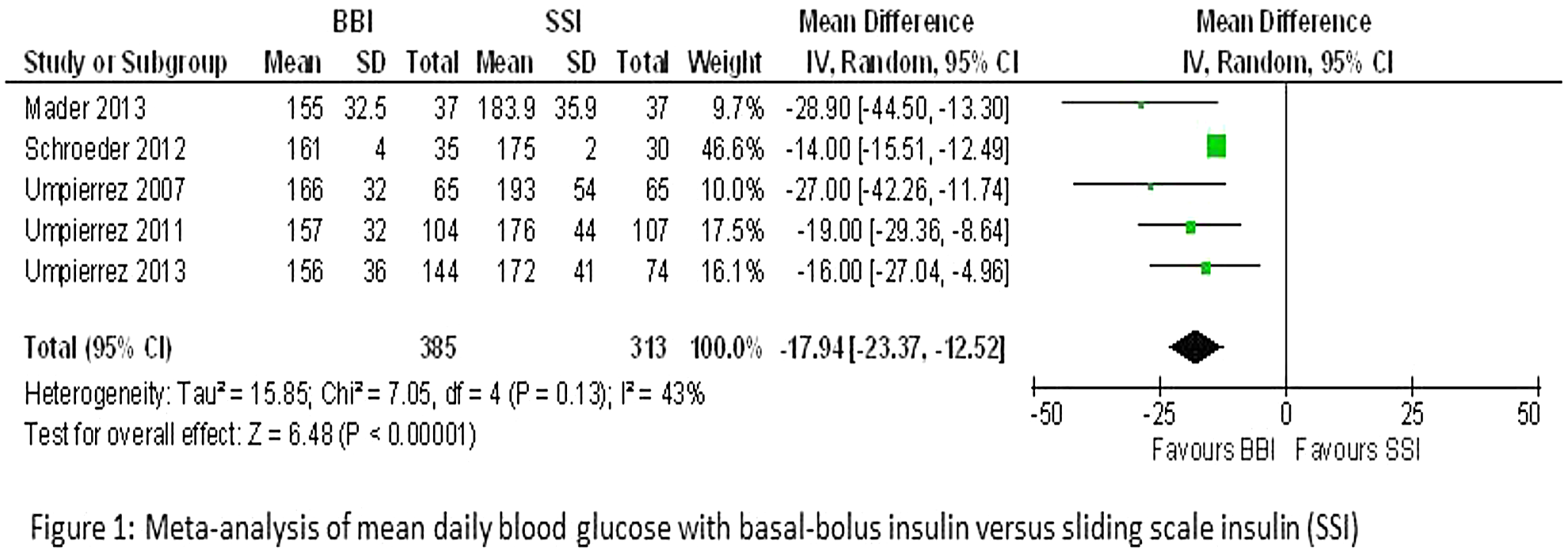
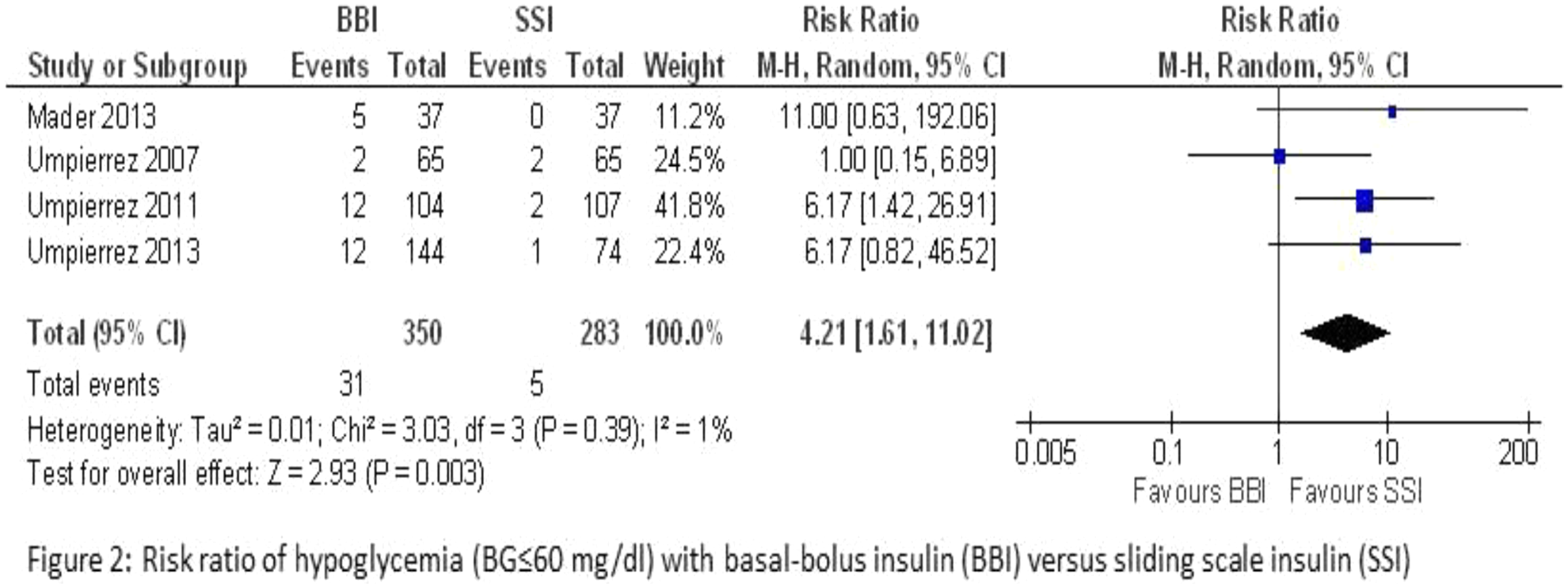
Kinderkrankenhaus auf der Bult, Janusz- Korczak-Allee 12, D-30173 Hannover, Germany
Sensor-augmented insulin pump (SAP) with the “MiniMed®640G” system features the PLGM algorithm (predictive low glucose management = “SmartGuard”) which stops insulin pump delivery based on predicted sensor glucose levels. This may offer advanced protection against hypoglycaemia.
The present study with pediatric patients in Germany had 3 phases: phase 1 – CSII with MM640G (4 weeks), phase 2 – SAP with MM640G without SmartGuard (2 weeks), phase 3 - MM640G with SmartGuard (6 weeks). Following settings for SmartGuart were applied in the study: switch off before Low: 70 mg/dL, threshold for hypoglycemia: 70 mg/dL. Primary outcome was the potential reduction in the frequency of hypoglycemic episodes and hypoglycemic intensity (AUC and time <70 mg/dl).
The interim analysis of 18 patients (age 9.9 ± 3.8years, diabetes duration 7.3 ± 3.0years, CSII experience 6.6 ± 1.7years) showed 2.64 ± 0.54 “interruptions before Low” per day and patient with SmartGuard. The total pump stoppage time was 149 ± 36 min per day. The pump stoppage time per event was 62.1 min. On average, the lowest glucose value during insulin shutdown was observed after 75.1 min. In 10% of cases the glucose values were lower than 55 mg/dL. The predictive low glucose shutdown of insulin delivery occurred at a glucose level of 107.5 mg/dL, and the average level at resumption was 108.0 mg/dL. Comparing phase of SAP with/without SmartGuard, decreased hypoglycemia events and intensity by using SmartGuard (table).
The present study provides evidence for further reducing the risk for hypoglycemia with SmartGuard without compromising the safety of SAP therapy.
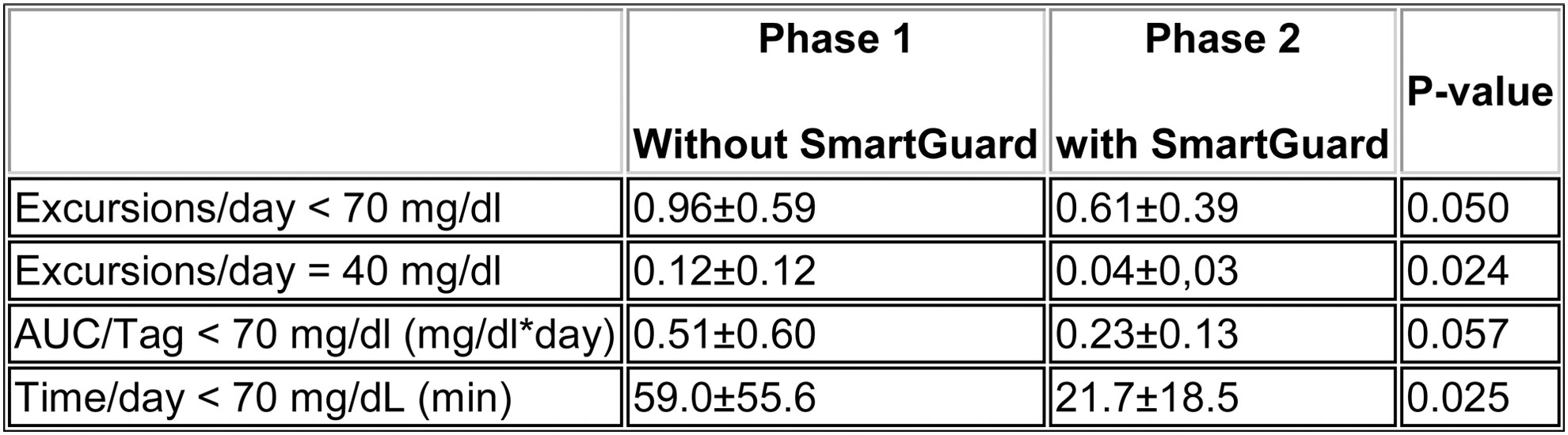
Badalona Serveis Assistencials, Dirección de Planificación, Badalona- Barcelona, Spain

University of Colorado Denver, Barbara Davis Center, Aurora, USA
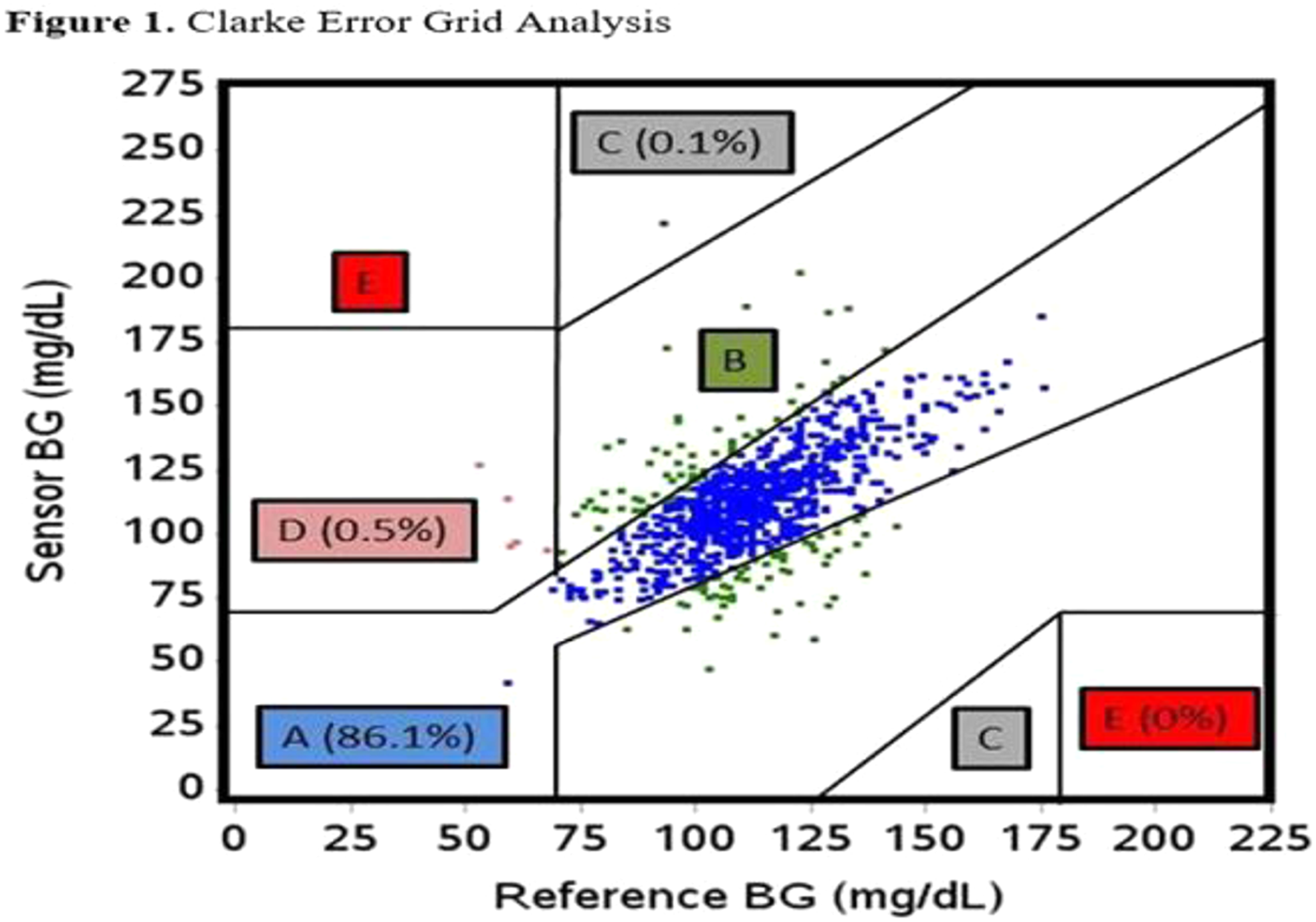
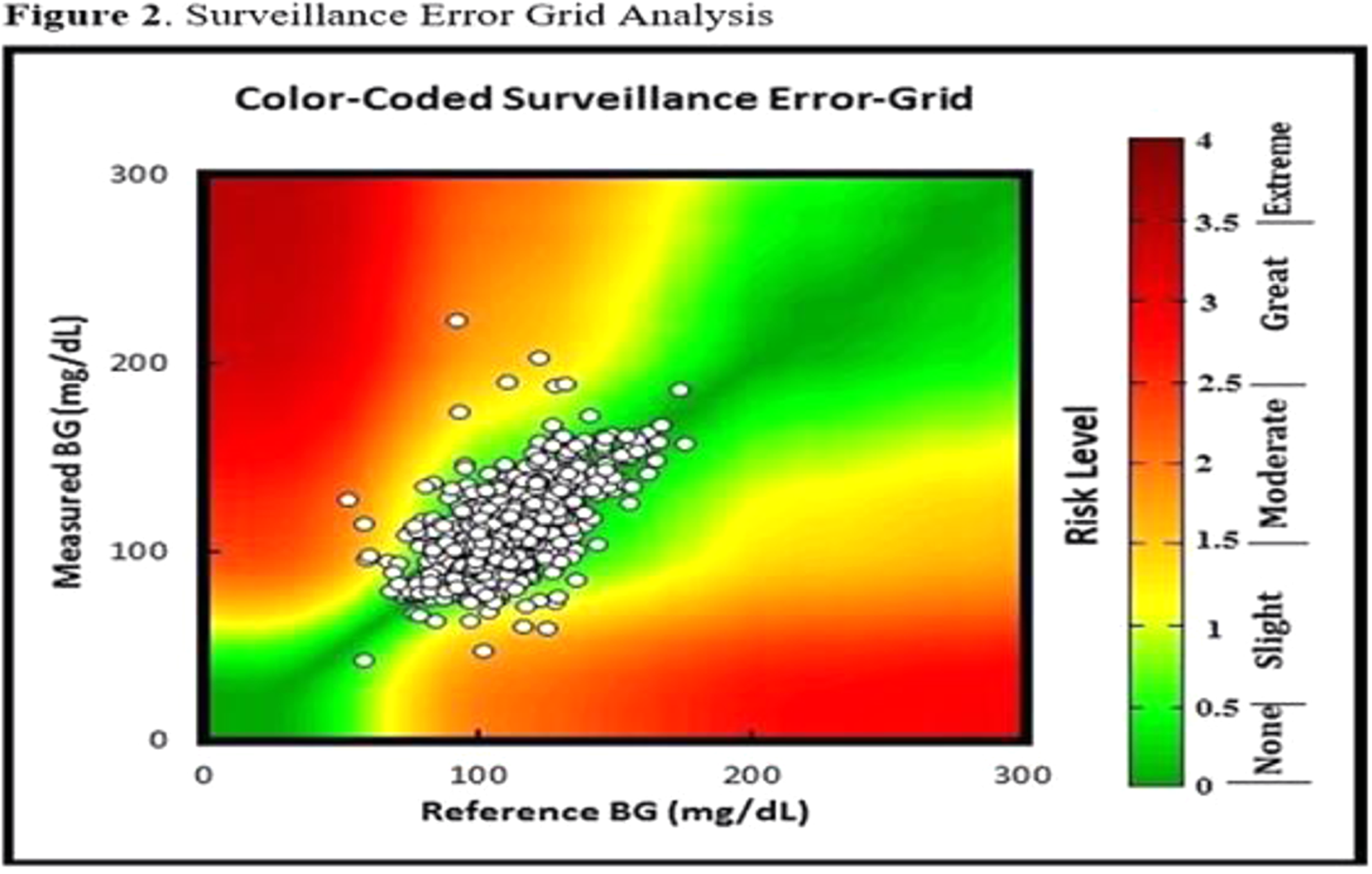

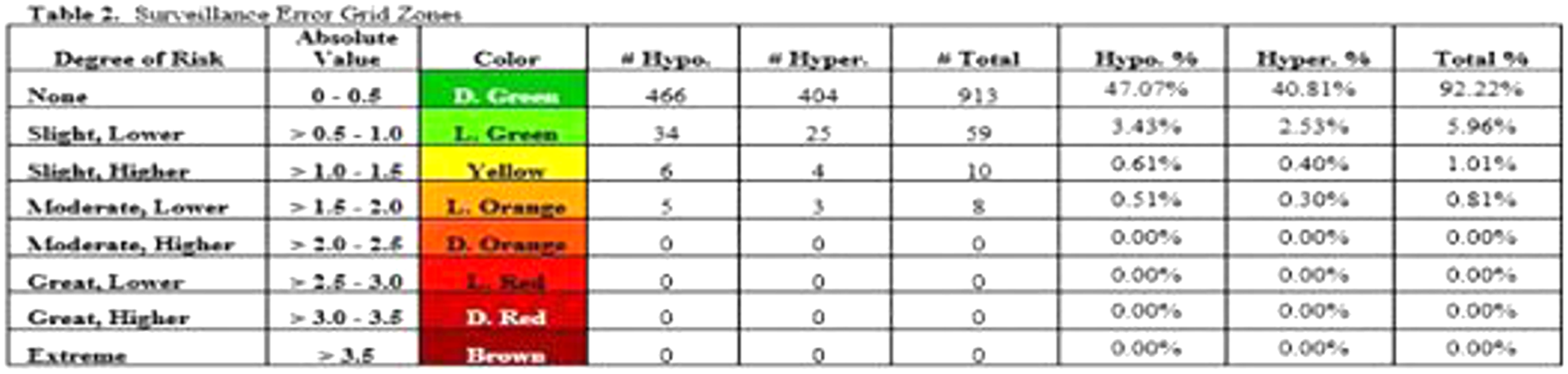
Ivano-Frankivsk National Medical University, Endocrinology, Ivano-Frankivsk, Ukraine
Croydon University Hospital, Diabetes & Endocrine/Obstetrics & Gynaecology, London, United Kingdom
The aim was to assess whether pregnant diabetic women were seen in clinic as per guidelines and to determine the outcome of all diabetic pregnancies in line with the below audit standards.
All diabetic women seen in the multidisciplinary antenatal clinic -100%
Care plan documented -100%
Of the 257 women, 99 had a caesarean section (38.5%). 26 /257 (10%) babies required admission to the neonatal unit. 3% (8/257) of all diabetic women had babies who needed admission for neonatal hypoglycaemia. 88% of all babies born had a normal weight.
University of Tsukuba, Graduate School of Comprehensive Human Science, Tsukuba, Japan
Hospital, Endocrinology- Diabetology and Metabolic Diseases, Dijon, France
University Hospital of North Norway, Norwegian Centre for Integrated Care and Telemedicine, Tromsø, Norway
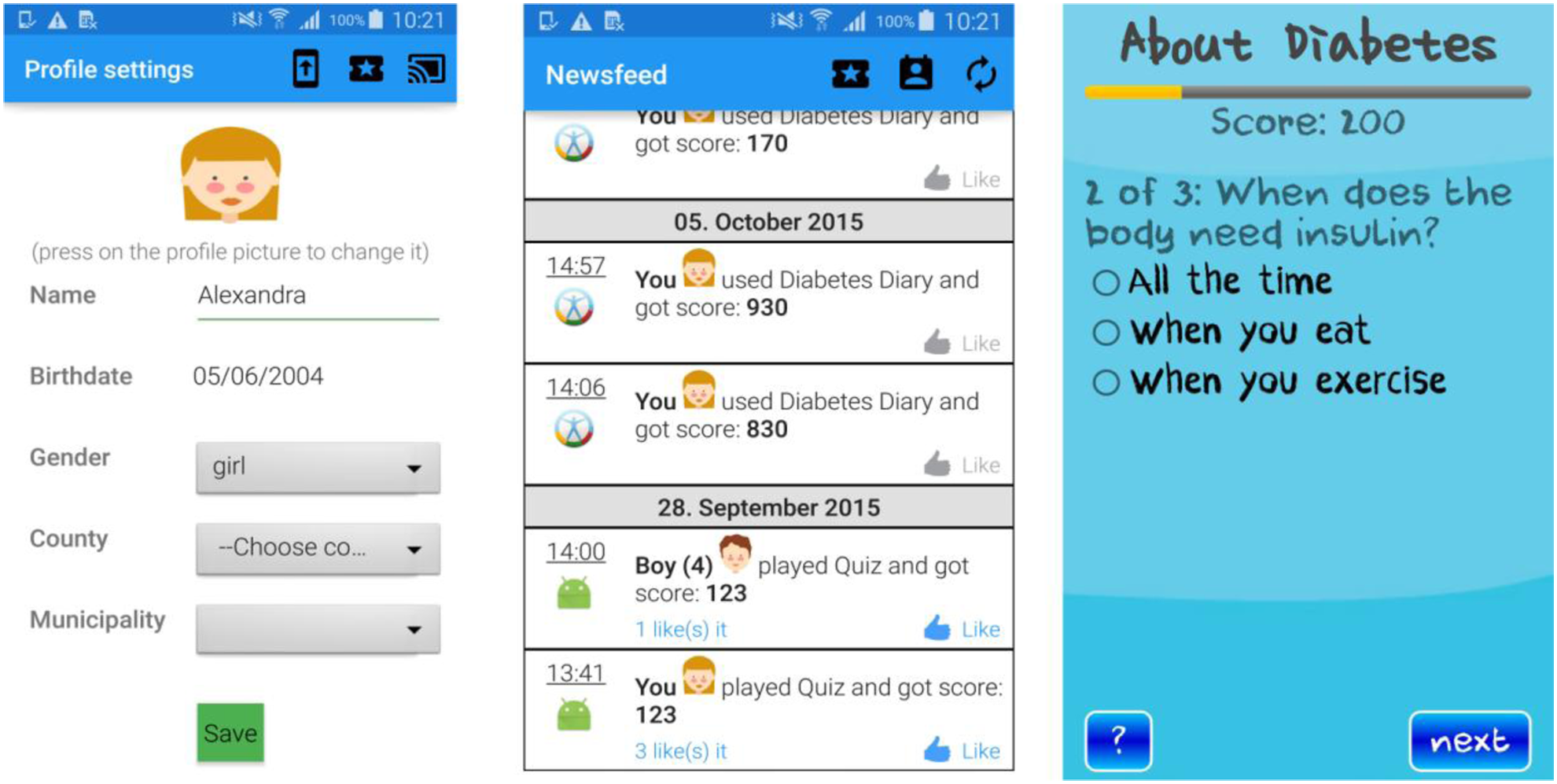
LMC Diabetes & Endocrinology, Diabetes, Toronto, Canada
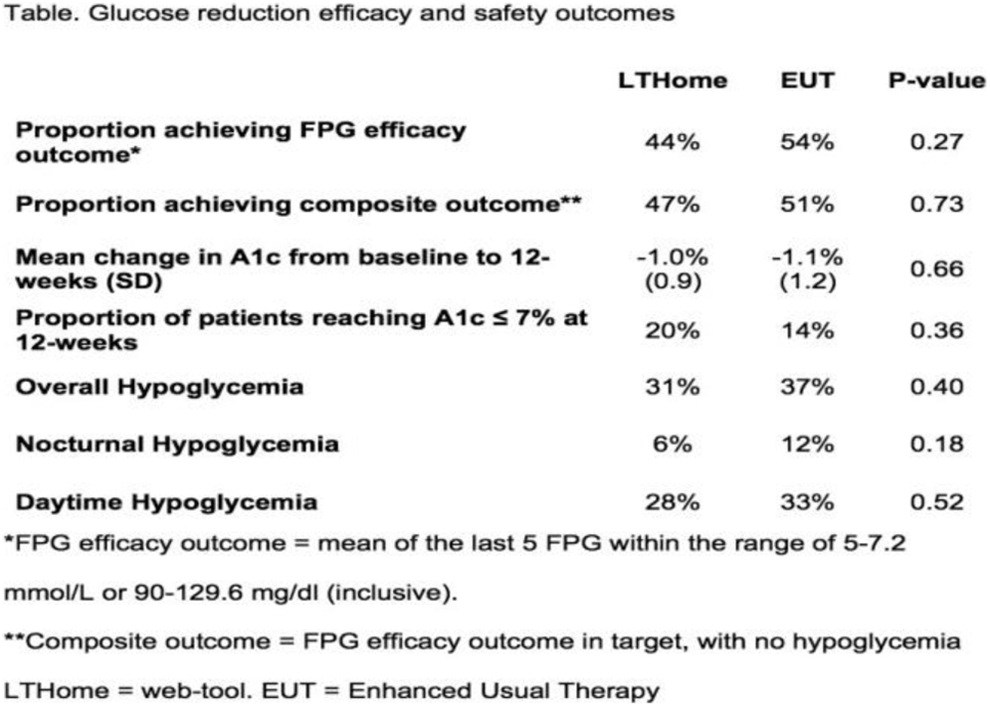
LMC Diabetes & Endocrinology, Diabetes, Toronto, Canada

Croydon University Hospital, Paediatrics, London, United Kingdom
1. Reviewing blood glucose levels on the computer screen with a clinician to discuss during clinic visits (
2. Increased awareness of complications of diabetes (
3. Increased blood glucose test frequency (
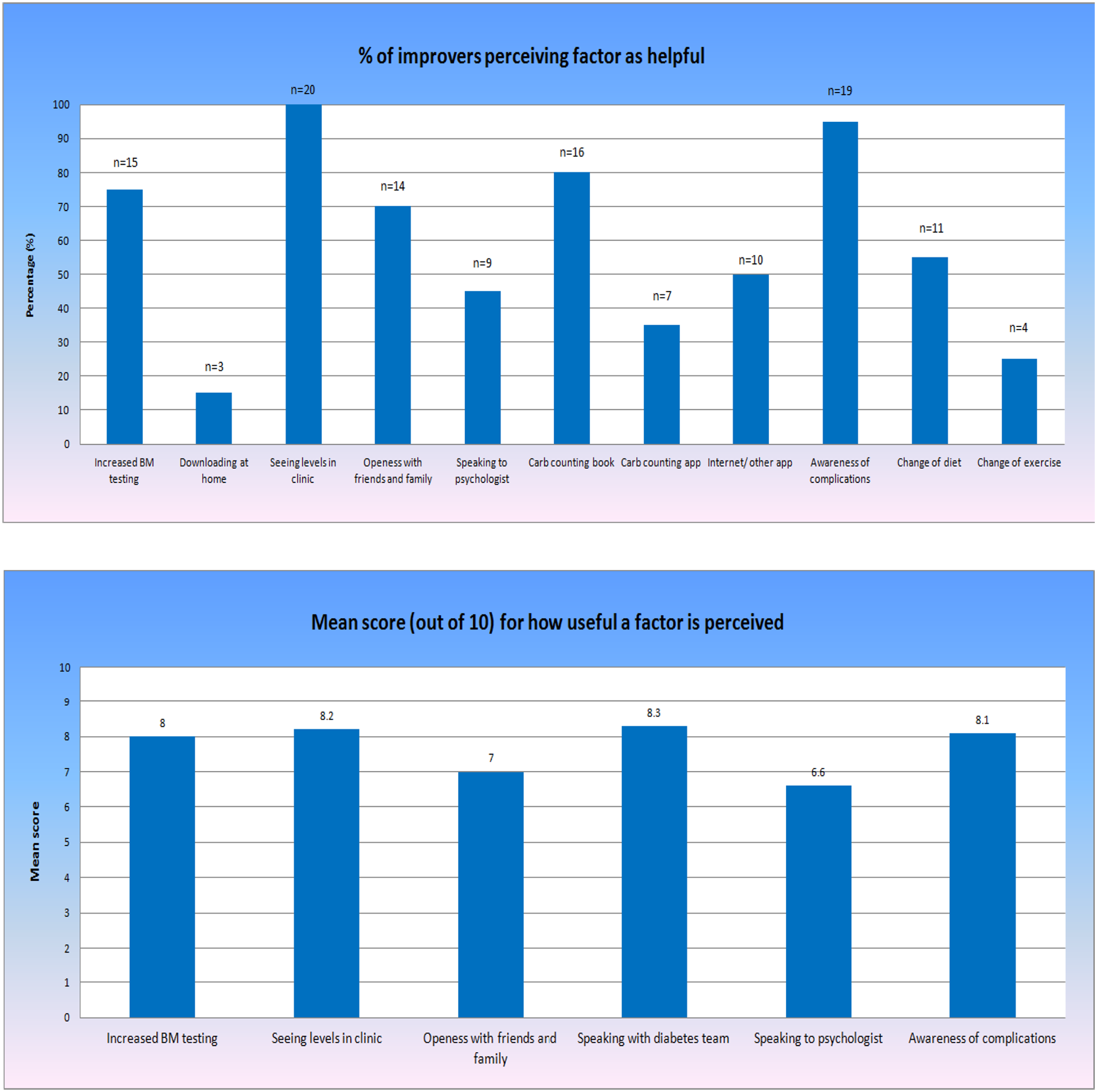
University Hospital of North Norway, NST, Tromsø, Norway
University of Pavia, Dipartimento di Ingegneria Industriale e dell'Informazione, Pavia, Italy
Diabetes Glandular Disease Clinic, Endocrinology, San Antonio, USA

A.O. Ospedale Niguarda, SSD Diabetologia, Milano, Italy
The “DSA box” consists in blood tests, ECG, eyes examination, carotid doppler ultrasound and, if necessary, specific evaluations and finally diabetologic visit. The other patients “not DSA” are followed according to the usual standard outpatient care.
Our preliminary data highlights the difficulties of aligning the hospital digital systems, the modalities to collect medical records and the different clinical reality.
University Children's Hospital, Department of Endocrinology- Diabetes and Metabolism, Ljubljana, Slovenia
Main feature of this application is that it calculates carbohydrates, fats, proteins and other nutrient values from weight of consumed food. It uses well-edited database consisting of local finished meals and also local and international food products available. It also features easy selection with multiple portion-size pictures (according to children age groups) of selected food items to simplify weight input. As food is added into the application, sums of all nutrient values are calculated and displayed. User can also save typical complete meals as templates to speed up the input process.
Application will be developed in three phases. First we will build a dynamic webpage with database of foods nutrients and individualised according to age portions. In the second phase we will build “web-view application” and publish it on Google Play store. In the last phase, the web page will be reproduced as “native application” with complete nutrients database and images, so it will work on mobile phones without internet connection, allowing users to use it everywhere on the go.
Imperial College London, Diabetes- Endocrinology & Metabolic Medicine, London, United Kingdom
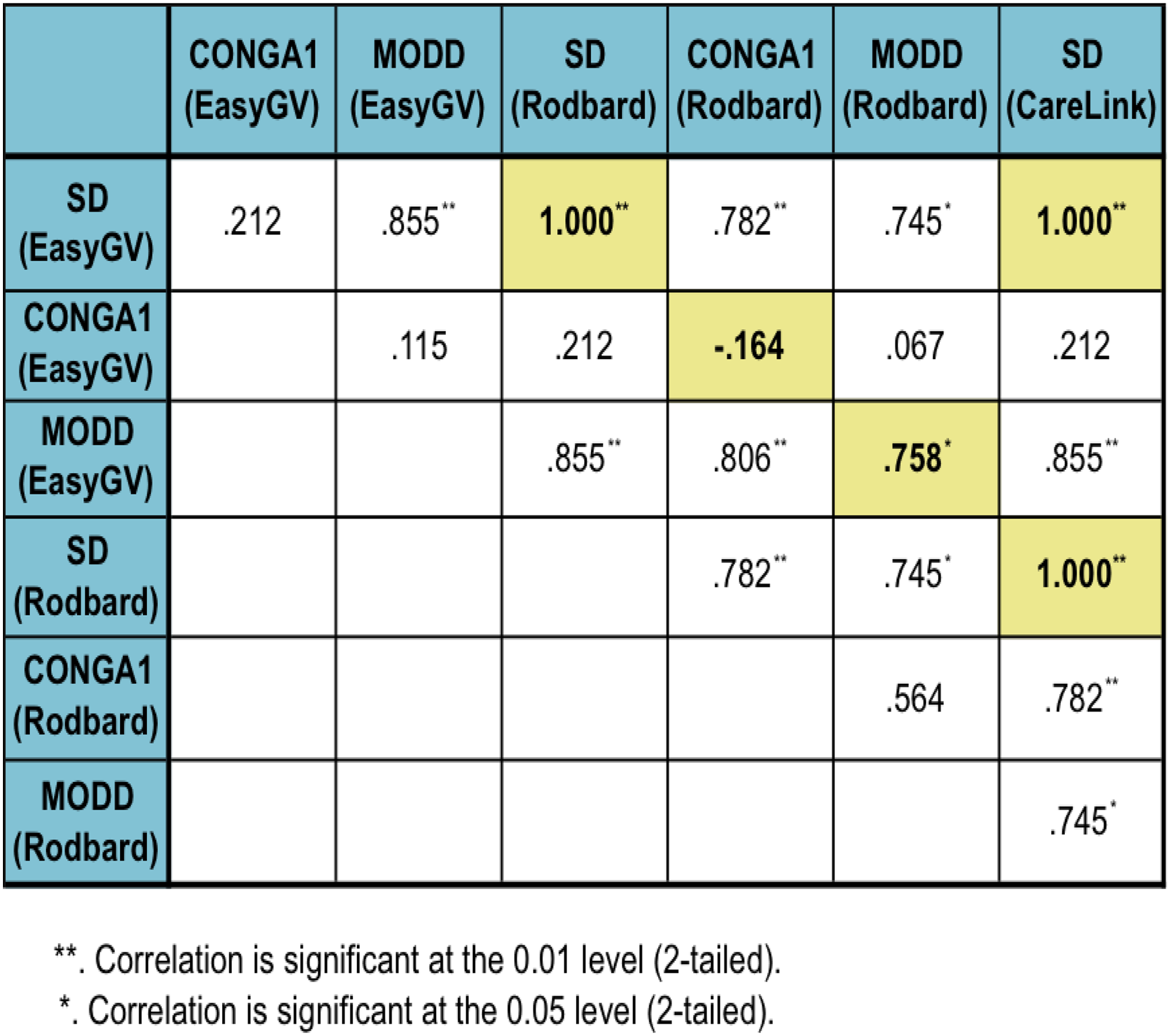
“Magna Græcia” University, Department of Clinical and Experimental Medicine, Catanzaro, Italy
University of Tromsø - The Arctic University of Norway, Department of Computer Science, Tromsø, Norway
• Colour signalization: Automatically adjusted lamp in the family's home indicates how the child is doing by changing colours and blinking. Similarly, colour can be displayed on walls, smartwatches, smartphones, pads and computers. • Info panel: Smart panel running Nightscout application at home plays an alarm and displays updated information received from the Diabetes Diary independently of where the child is located. • Smartwatch: Alarms and vital information from the child is available on a Pebble that communicates with the smartphone-based diary. • Radio: Through transferring BG-values as radio signals, the FM-RDS radio announces and displays incoming BG-values. • SMS: The diary app sends an SMS to the child's parents' phone(s) every time updates are made to the diary.
Czech Technical University in Prague, Faculty of Biomedical Engineering, Kladno, Czech Republic
Regarding the approach applied in the system presented, our aim is to find the best possible combination of reminders and alerts and implement these processes as fully automatic.
The system has been already tested by diabetic patients.

Brazilian Juvenile Diabetes Association ADJ Diabetes Brasil, Brazilian Young Leaders Training, São Paulo, Brazil
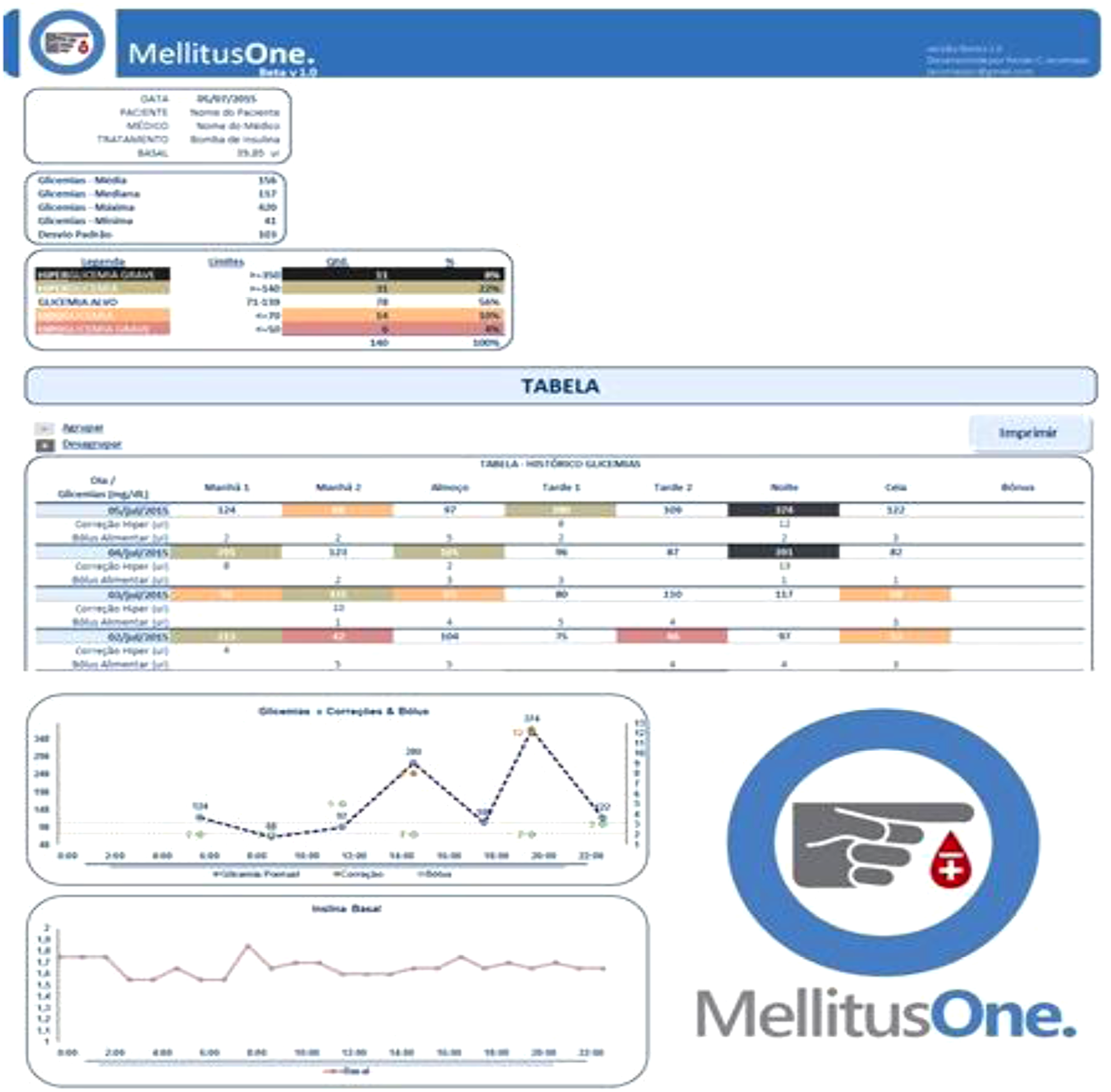
The Arctic University of Norway, Department of Computer Science- UiT, Tromsø, Norway
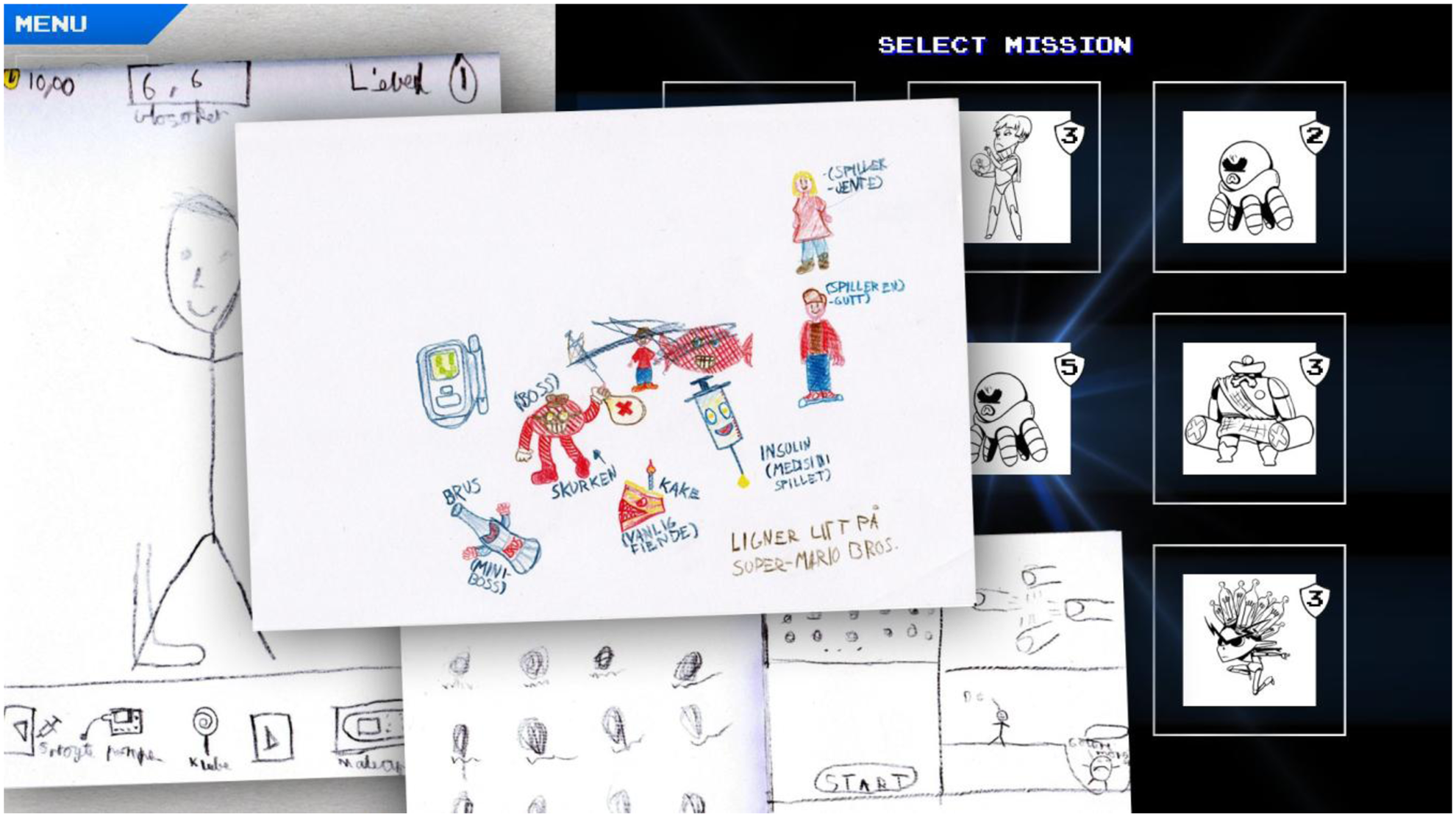
Jothydev's Diabetes Research Centre, Diabetes, Thiruvanathapuram, India
University of Ulsan College of Medicine/Asan Medical Center, Department of Physiology, Seoul, Republic of Korea
IRCCyN, Commande, Nantes, France
The objective is to validate this model using clinical data of a larger number of patients and to prove its ability to predict the behavior of glycemia and insulinemia dynamics.
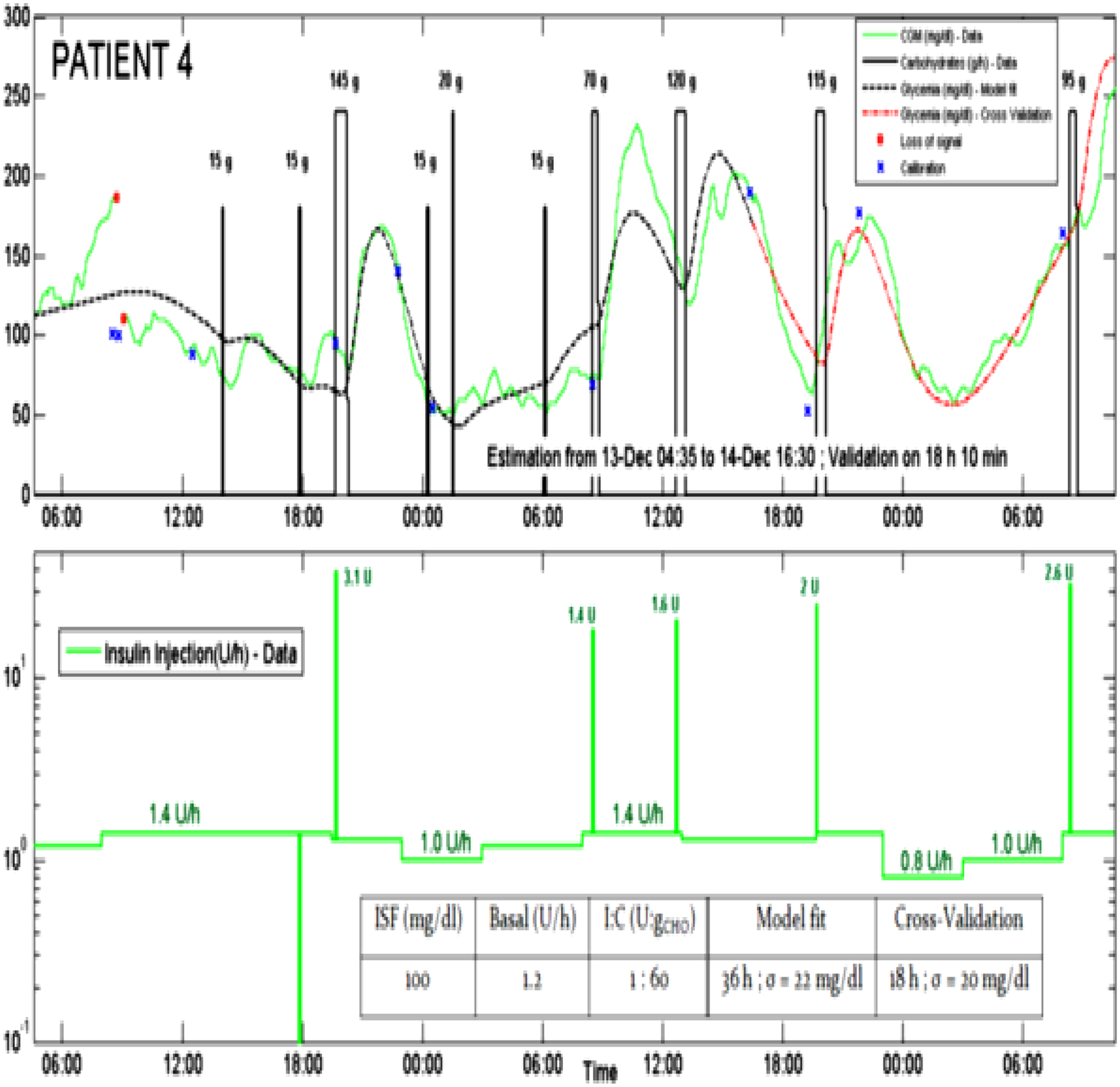
Diabetech- LP, Research & Development, Sausalito, USA
Diabetech- LP, Research & Development, Sausalito, USA
Statistics Table 3 – Change in A1c – Control vs. Treatment “Group C: baseline A1c 7-8.9”

International Diabetes Center, HealthPartners Institute, Minneapolis, USA
1. Evaluate streamlined, standardized cloud-based glucose reporting using CaptūrAGP™ software and report
2. Assess patient and clinician preferences regarding the AGP report including presentation of glucose data, standardized terminology and utility in diabetes management
Clinicians reported that the AGP report when compared to other data sources was best at helping educate patients about glucose patterns (89%) and for helping the clinicians see patterns 84%.
Spin-off Application Centre, First Medical Faculty of Charles University, Prague, Czech Republic
University College London, UCL Interaction Centre, London, United Kingdom
Pediatric Hospital “Giovanni XXIII”, Metabolic Diseases- Clinical Genetics and Diabetology, Bari, Italy
Saint-Petersburg Medical University, Endocrinology, Saint-Petersburg, Russia
The Center of Family Planning and Reproduction, Endocrinology, Saint-Petersburg, Russia
Both T1D patients and doctors found useful information in topics #diascience, #diagadgets, #diadoctortalk. Patients with T1D were also interested in #diapregnancy. Statistically significant difference between 2 groups was only in topic #translationofdiaarticles.
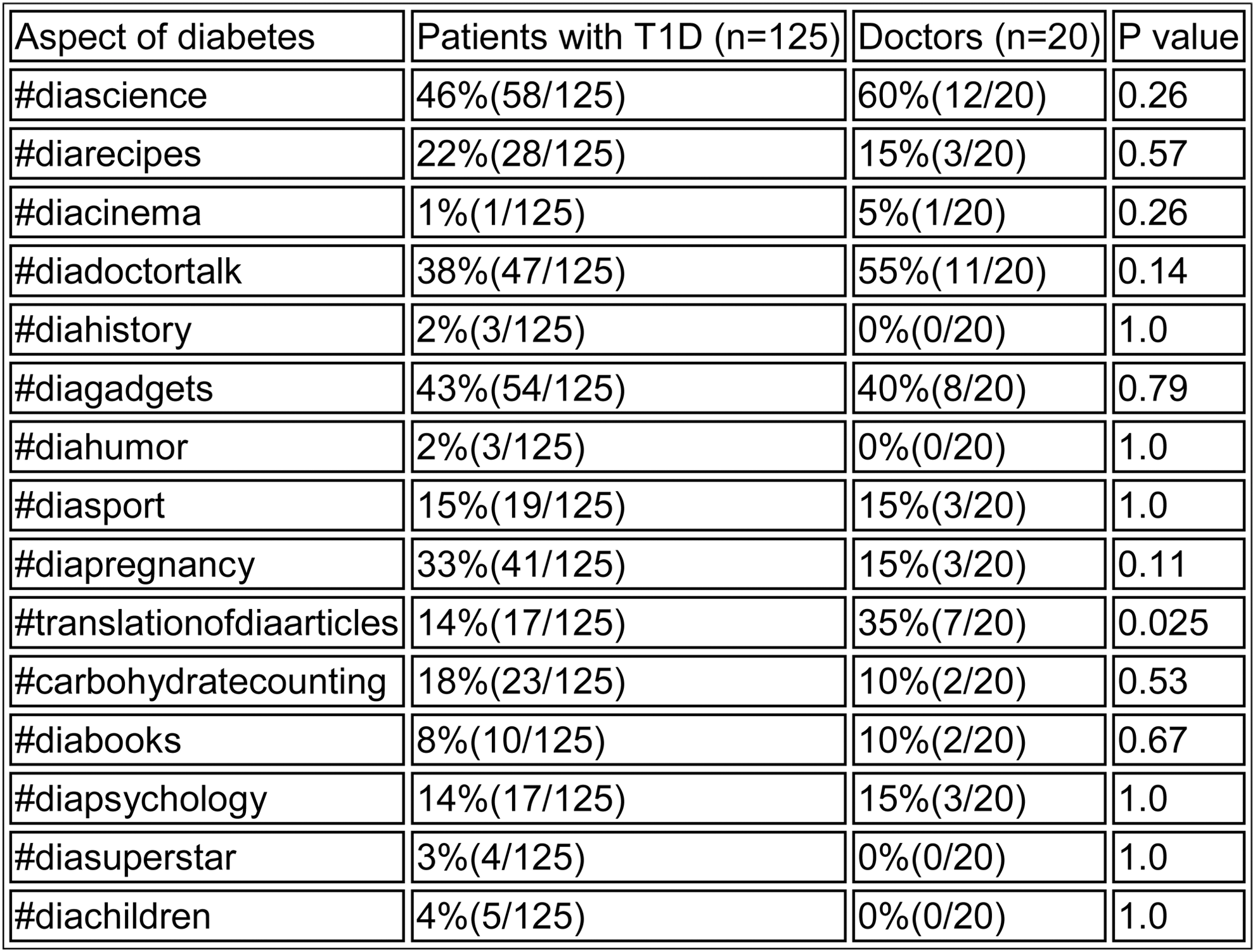
Imperial College London, Centre for Bio-Inspired Technology, London, United Kingdom
Imperial College London, Centre for Bio-Inspired Technology, London, United Kingdom
University Clinic of Endocrinology, Center for Insulin Pump, Skopje, Macedonia
Patients were able to ask questions and open discussion on different topics about their diabetes management, where other patients could respond and comment. Advice was given by doctor/educator and educated patient according to the group.
Hba1c was performed baseline, three and six months after the study. Patient should have at least 3 communications per week to be eligible for evaluation.
Endocrinology Research Centre, Diabetes Institution, Moscow, Russia
Scripps Health, Scripps Whittier Diabetes Institute, San Diego, USA
CRF Health, Product & Services Management, London, United Kingdom
CNR Institute of Neuroscience, Metabolic Unit, Padova, Italy

CNR Institute of Neuroscience, Metabolic Unit, Padova, Italy
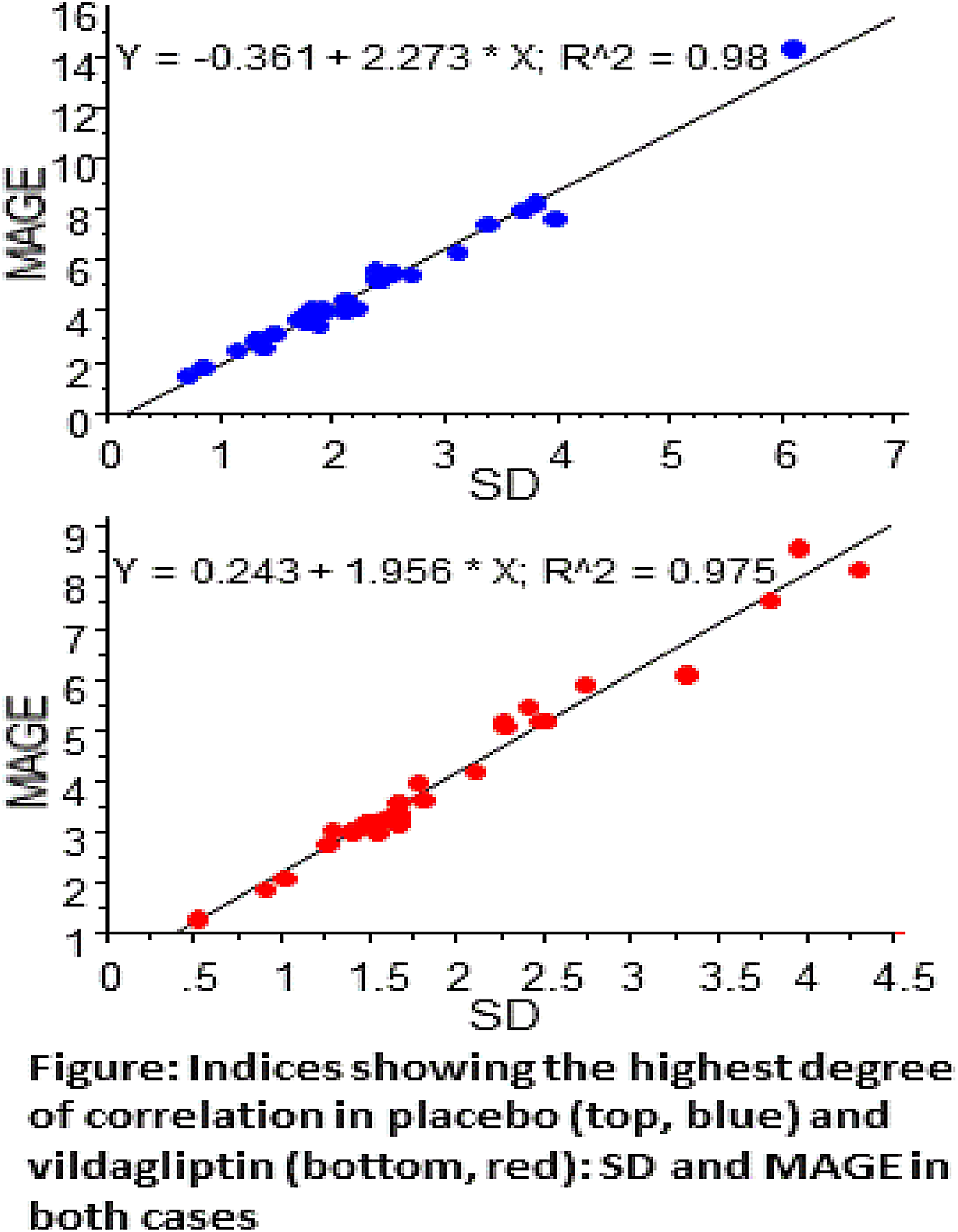
Quattro Folia Oy, Research, Espoo, Finland
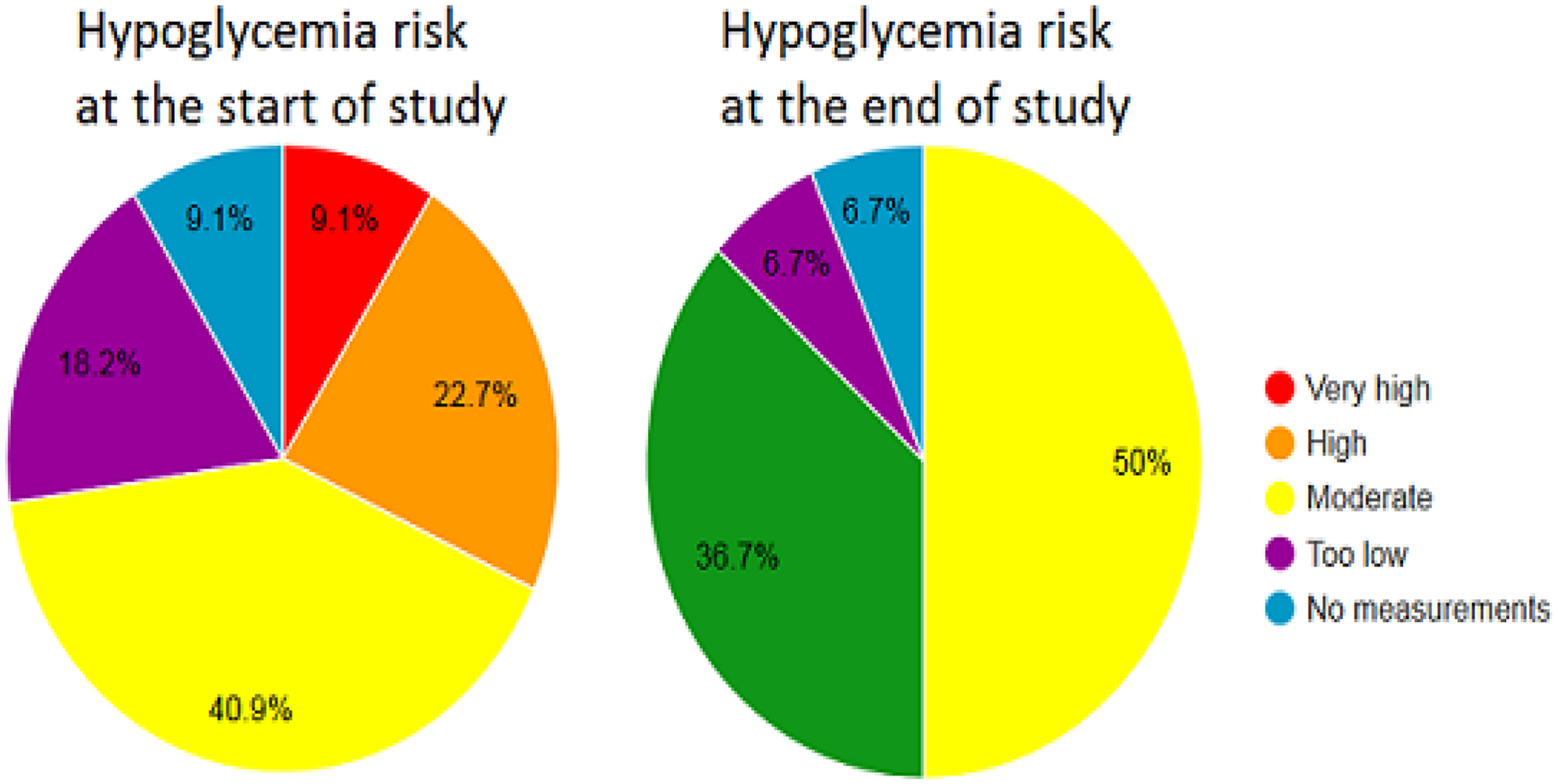
Medtronic, Inc., Diabetes, Northridge, USA
UCL- School of Pharmacy, Research Department of Pharmacy Practice, London, United Kingdom
43 patients were asked about their beliefs, views and experiences regarding their medicines/devices used and lifestyle. This was followed by conducting interviews with healthcare professionals, in order to propose for service development.
University of Western Australia, School of Population Health, Perth, Australia
Centre Hospitalier Hôtel Dieu, Le Creusot, France
The proportion of patients in every HbA1c class was as follows.
HbA1c evolution according to terciles at T0, showed a better improvement for the highest initial levels.
Weight remained stable : 95.9-96.9-95.1kg - ΔT0-T12 : - 0.8 kg – NS ; BMI : 33.8-34-33.7 kg/m2 - Δ : -0.1 kg/m2- NS.
Insulin doses decreased : 1.28/0.97/1 - ΔT0-T12 : - 0.28 U/kg/j (-22% – p < 0.001).
No severe hypoglycemia has been reported, 6 patients stopped the treatment by AIP (4 infections/catheter).
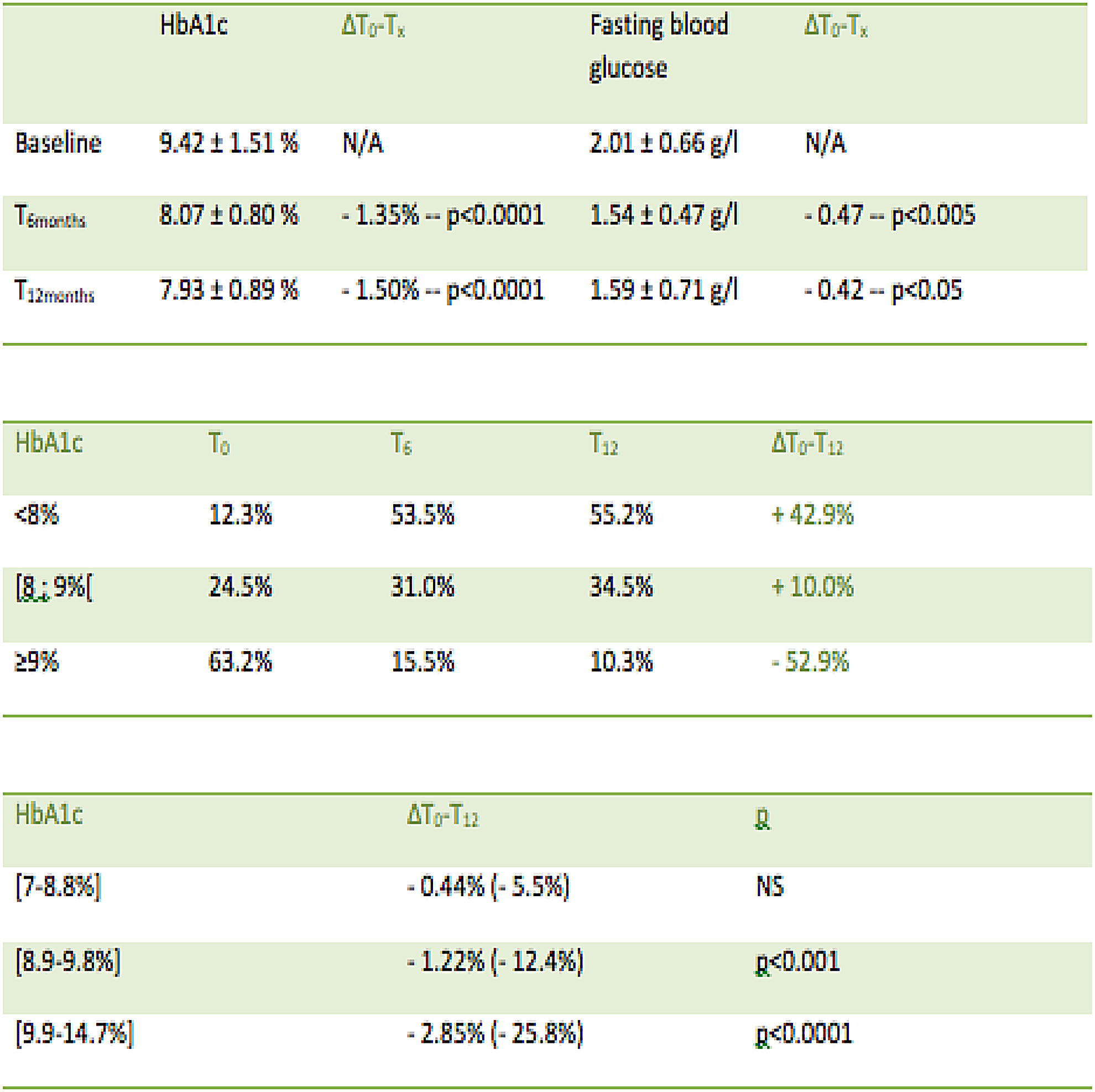
Hôpital Saint Joseph, Endocrinology and Diabetology, Paris, France
No specific technical problem was reported in terms of pump or catheter.
At T12months, insulin total dose decreased by 22% and flows number was limited (n = 2.45 and basal/bolus ratio = 1.23).
We assessed hypoglycemia frequency with MI vs. AIP : 3.3 in the last 12 months (0.13 severe/yr) vs. 2.3 in the last 3 months (not severe).
Hospitalizations comparative analysis before and 12 months after AIP treatment showed a global improvement especially for uncontrolled diabetes causes (66 vs. 28%; p < 0.05).
Cardiovascular risk factors remain the same: weight (Δ =-0.9 kg), BMI (Δ = - 0.1 kg/m2), blood pressure and lipid status are not different.

Medical University Varna, Department of Pediatrics and Medical Genetics, Varna, Bulgaria
Badajoz University Hospital, Department of Endocrinology, Badajoz, Spain
Medical University, Dept. Pediatric Endocrinology and Diabetology, Lublin, Poland
Ospedale Civico di Partinico, Internal Medicine - Regional Reference Center for Diabetology and Insulin Pumps, Partinico, Italy
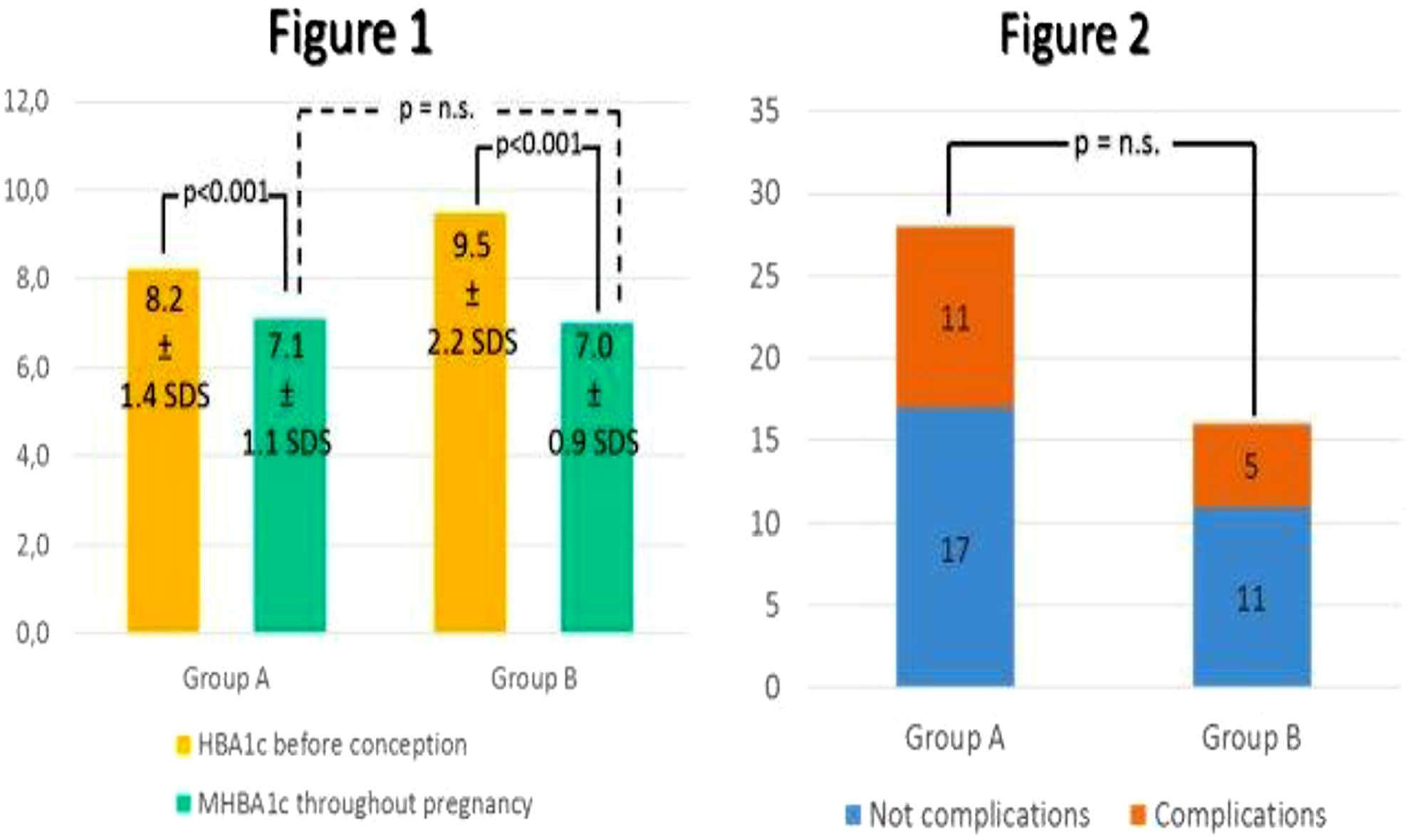
Karolinska Institute, Department of Women's and Children's Health, Stockholm, Sweden
The aim was to evaluate whether an intervention with GSD-Y in groups of adolescents starting on CSII and their parents leads to decreased HbA1c and fewer diabetes-related family conflicts.
DFCS correlated with HbA1c. The intervention group perceived a lower degree of conflicts after GSD-Y education.
Animas Corporation, Wayne, PA, USA
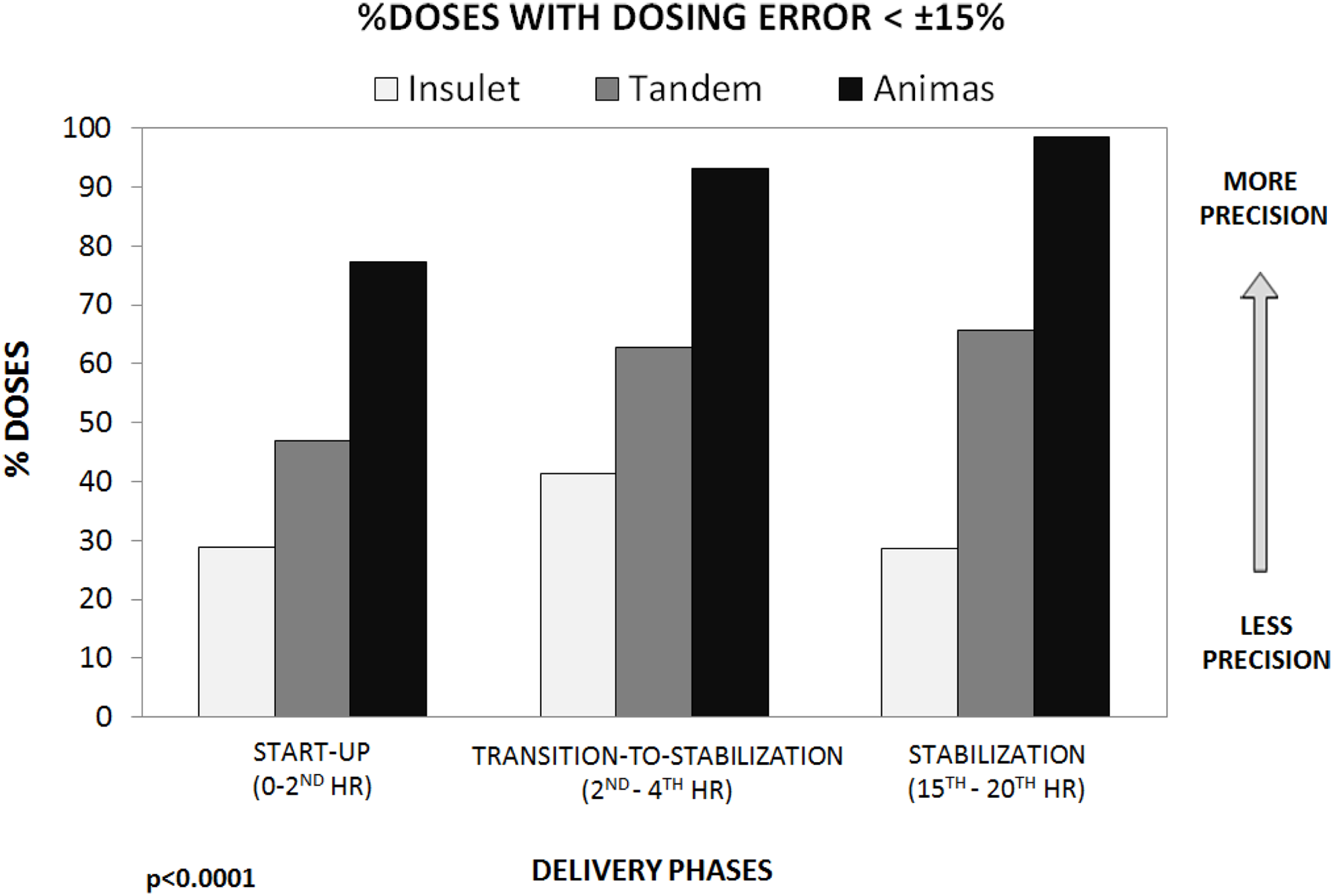
Department of Personality- Assessment and Psychological Treatment., Instituto de Investigación Biomédica de Málaga IBIMA. Universidad de Málaga, Málaga, Spain
University Clinical Centre Maribor, Department of Endocrinology and Diabetology, Internal Clinic, Maribor, Slovenia
Medical University of Lodz, Department of Internal Medicine and Diabetology, Lodz, Poland
Hospital de Cabueñes, Endocrinology, Gijon, Spain
Of these, 71% were women, with a mean age of 36 years (SD 13) and a mean diabetes evolution of 16 years (SD 10). Mean time with CSII was 6 years (SD 4).
The most common reason for pump treatment was brittle diabetes (43%), followed by pregnancy planning (22%), severe hypoglycemia or hypoglycemia unawareness (21%) and inadequate metabolic control (12%).
Baseline HbA1c was 7.6% (SD 1) and fell by 0.1% at the end of follow-up. HbA1c reduction was higher in patients with CSII use <2 years (-0.85% vs +0.1%; p < 0.05) and in those with a baseline HbA1c >8% (-0.9% vs +0.3%; p < 0.05).
13 pumps were withdrawn (11%), mainly for psychological pump intolerance. Safety was good, with a hospitalization rate of 1.2 patients/year.
In terms of HbAc1 reduction, CSII therapy was more effective in the short-term use and in patients with a higher baseline HbA1c.
University of Virginia, Center for Diabetes Technology, Charlottesville, USA
Endocrinology Research Centre, Institution of Diabetes, Moscow, Russia
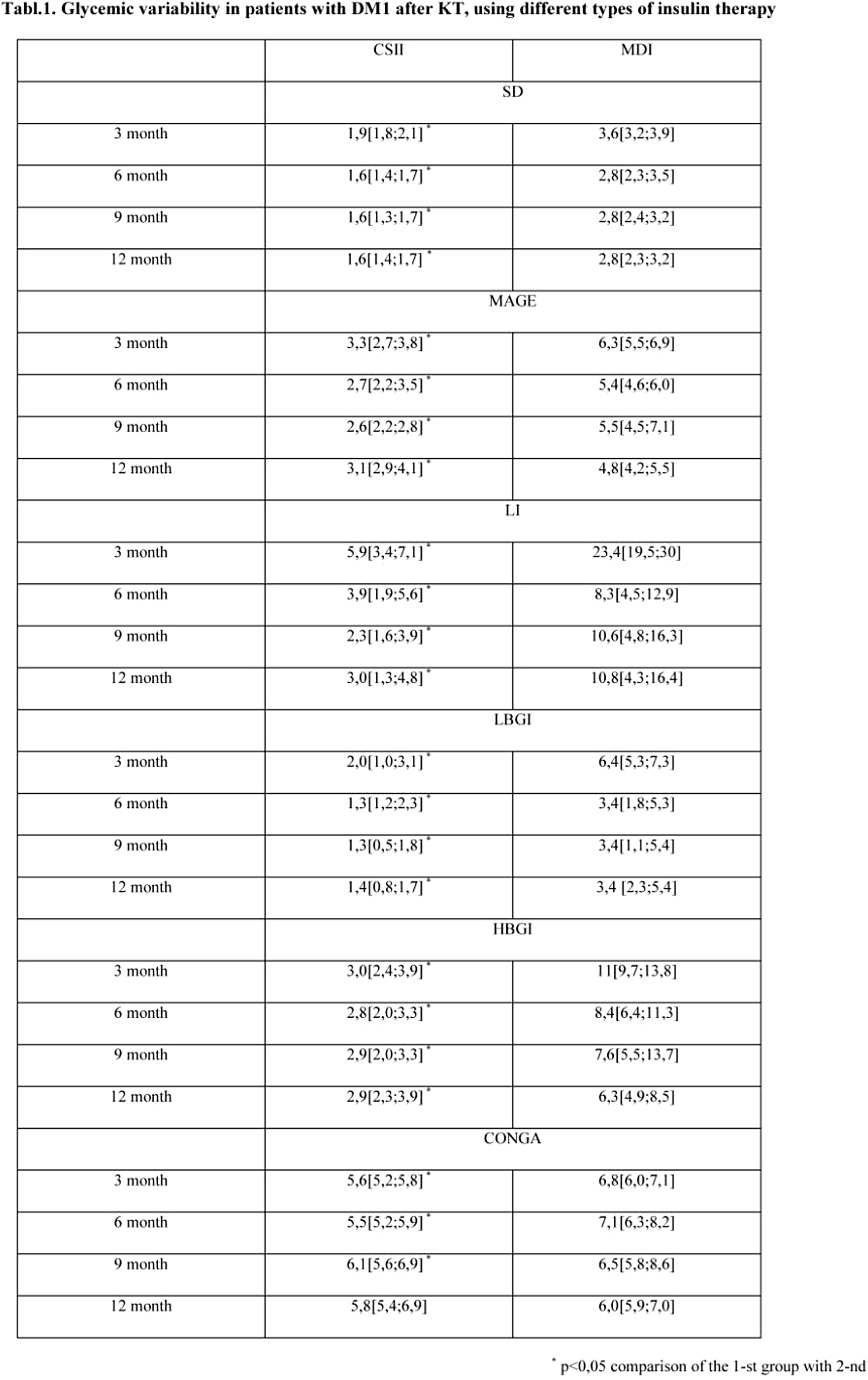
Hospital Universitario San Ignacio, Endocrinology, Bogotá D.C., Colombia
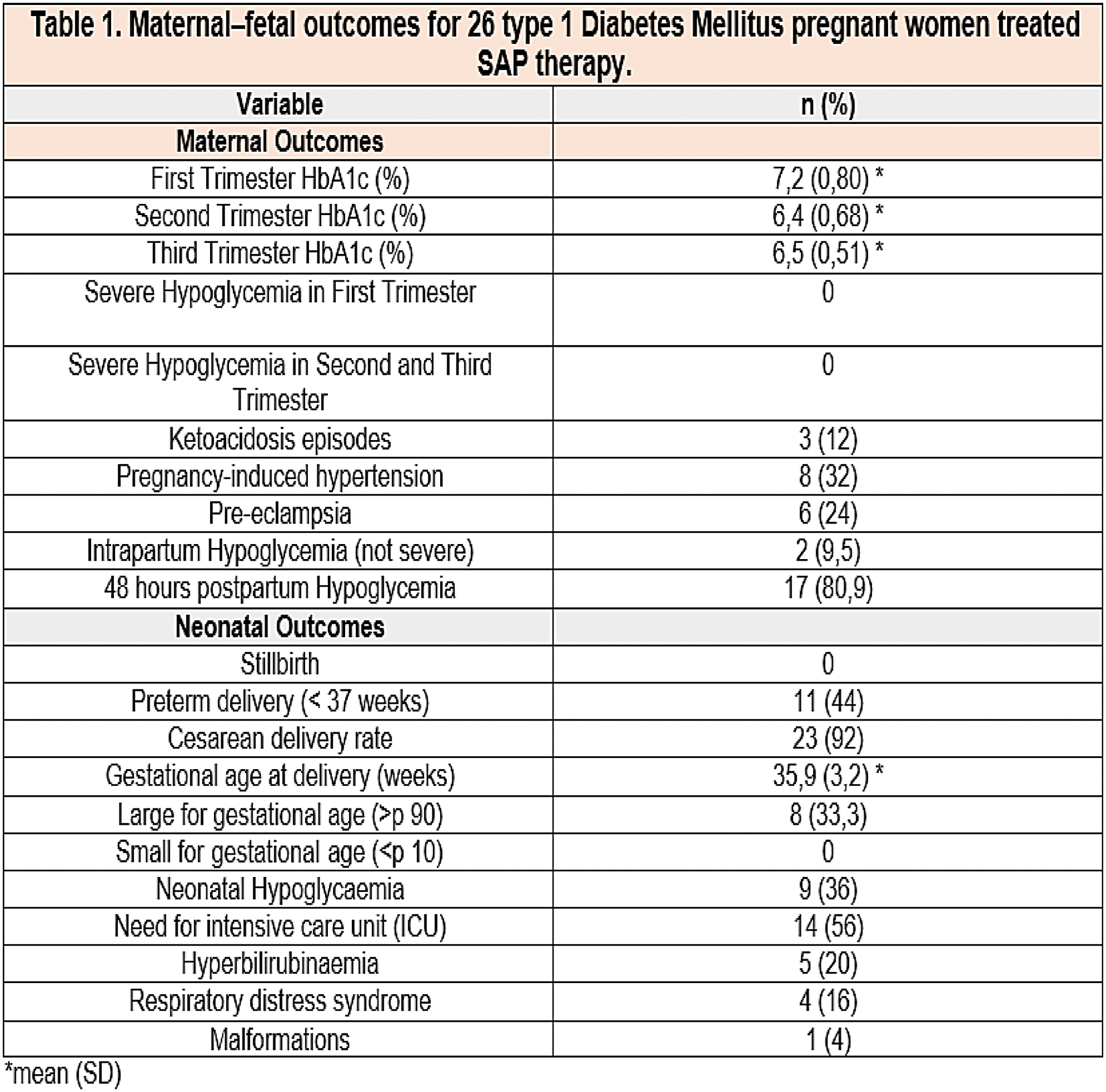
University of Verona and AOUI Verona, Department of Medicine, Verona, Italy
San Raffaele Scientific Institute, Diabetes Research Institute, Milan, Italy
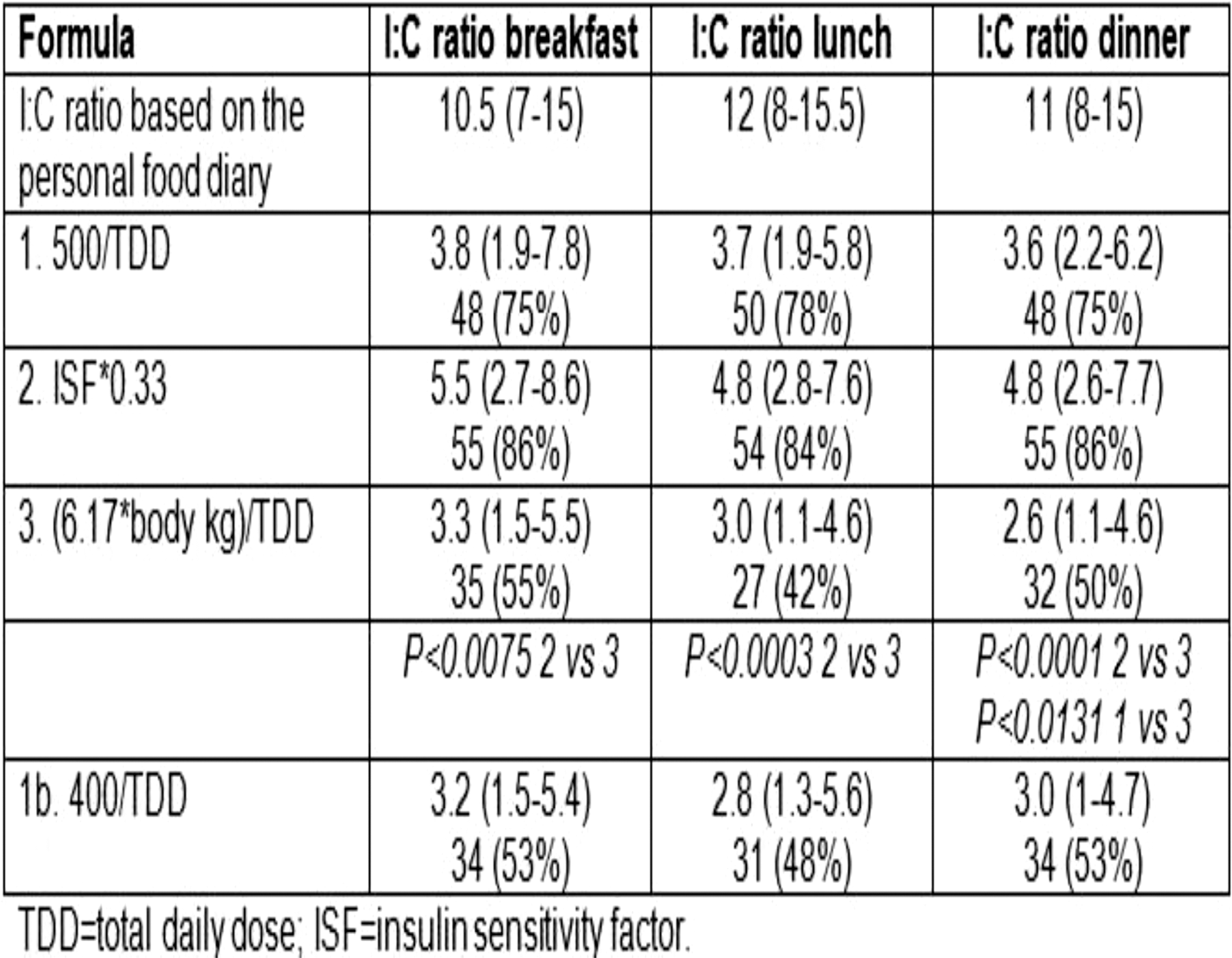
CeQur, Clinical Research, Marlborough, USA
Medical University of Graz, Endocrinology and Metabolism, Graz, Austria
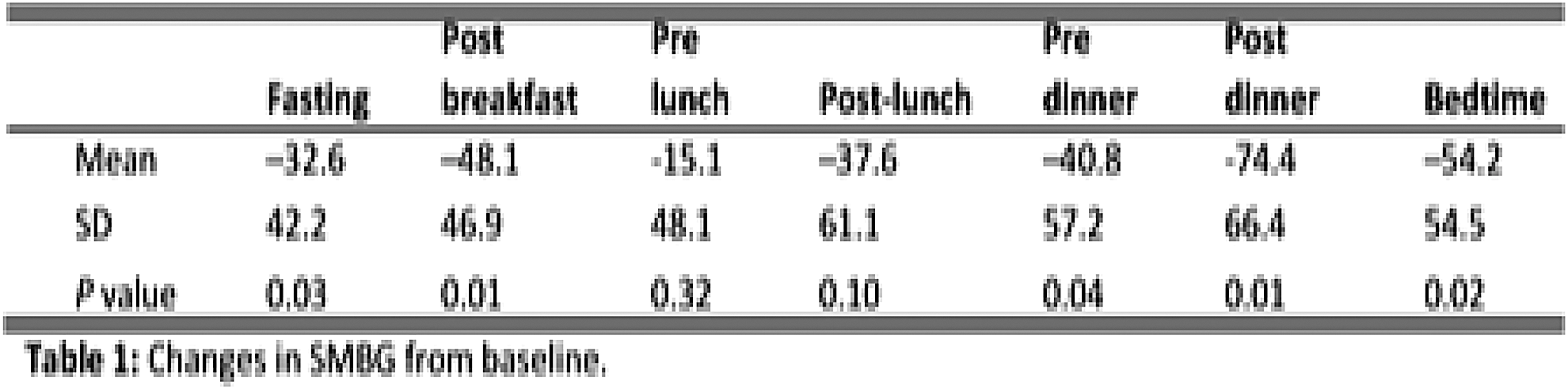
Second University of Naples, Department of Medical- Surgical- Neurological-Metabolic Diseases and Aging, Naples, Italy
Vita-Salute San Raffaele University, School of Diabetology and Endocrinology, Milan, Italy
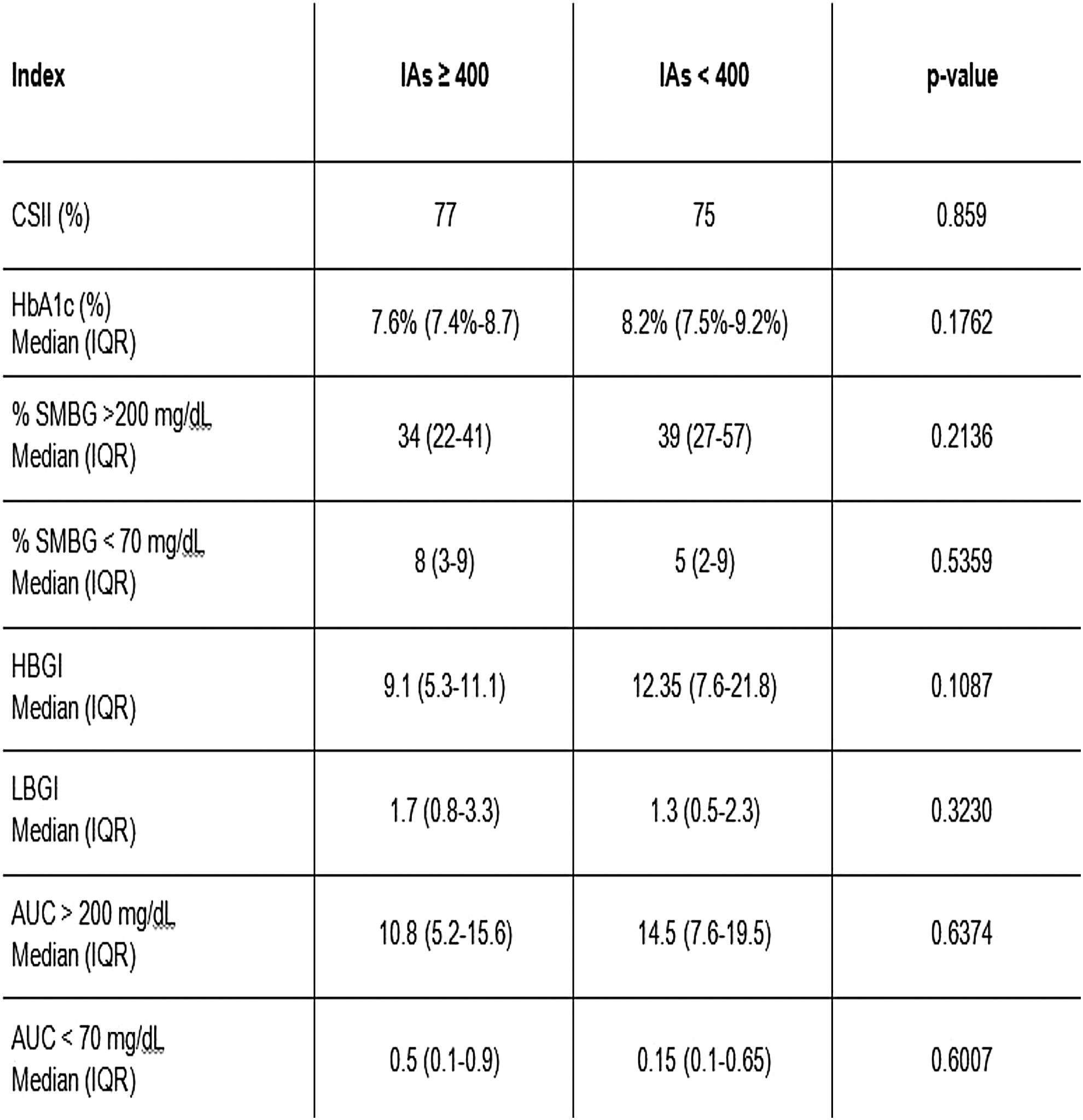
Vienna, Austria
The CGM values and trends were used to calculate the prandial insulin and to correct higher glucose levels by the bolus calculator. In addition the patients received an algorithm to respond to rising and falling trends shown on the CGM. If the CGM trends were rising, patients had to receive a supplement insulin dose; if the trends were falling the insulin pump was stopped and sometimes carbohydrates were given.
NHO Kyoto Medical Center, Diabetes Center, Kyoto, Japan
Animas Corp, Quality Engineering, Wayne, USA
Saint-Petersburg Medical University, Endocrinology, Saint-Petersburg, Russia
The rating of problems was made separately for two groups. Using the Pirson's method we also explored correlations between patient's HbA1c level, income level and level of education.
Patients both on CSII and MDI have some similar problems (mainly with supplies for diabetes, fear of pregnancy problems, CHO counting and frequent glycemia control). Patients on MDI are anxious about psychological moments, reaching normoglycemia, lack of information about diabetes and hypoglycemia; patients on CSII have difficulties with pregnancy planning, sex and social opinion about their illness and more problems with diabetes supplies.
Section Endocrinology-Garibaldi Nesima Hospita, Clinical and Experimental Medicine, Catania, Italy
Institut für Diabetes-Technologie Forschungs- und Entwicklungsgesellschaft, an der Universität Ulm, Ulm, Germany
Mazara del Vallo, Italy
However additional determinations should be made within postprandial states, particularly when rapid insulin analogues or pump-treatments are used. There is a need for patients to be able to adjust their insulin doses accurately and independently during continuous subcutaneous insulin infusion (CSII) therapy in order to improve glycemic control. To assess the relationship between HbA1c and frequency of SMBG in a group of type 1 diabetes CSII users, compared with MDI.
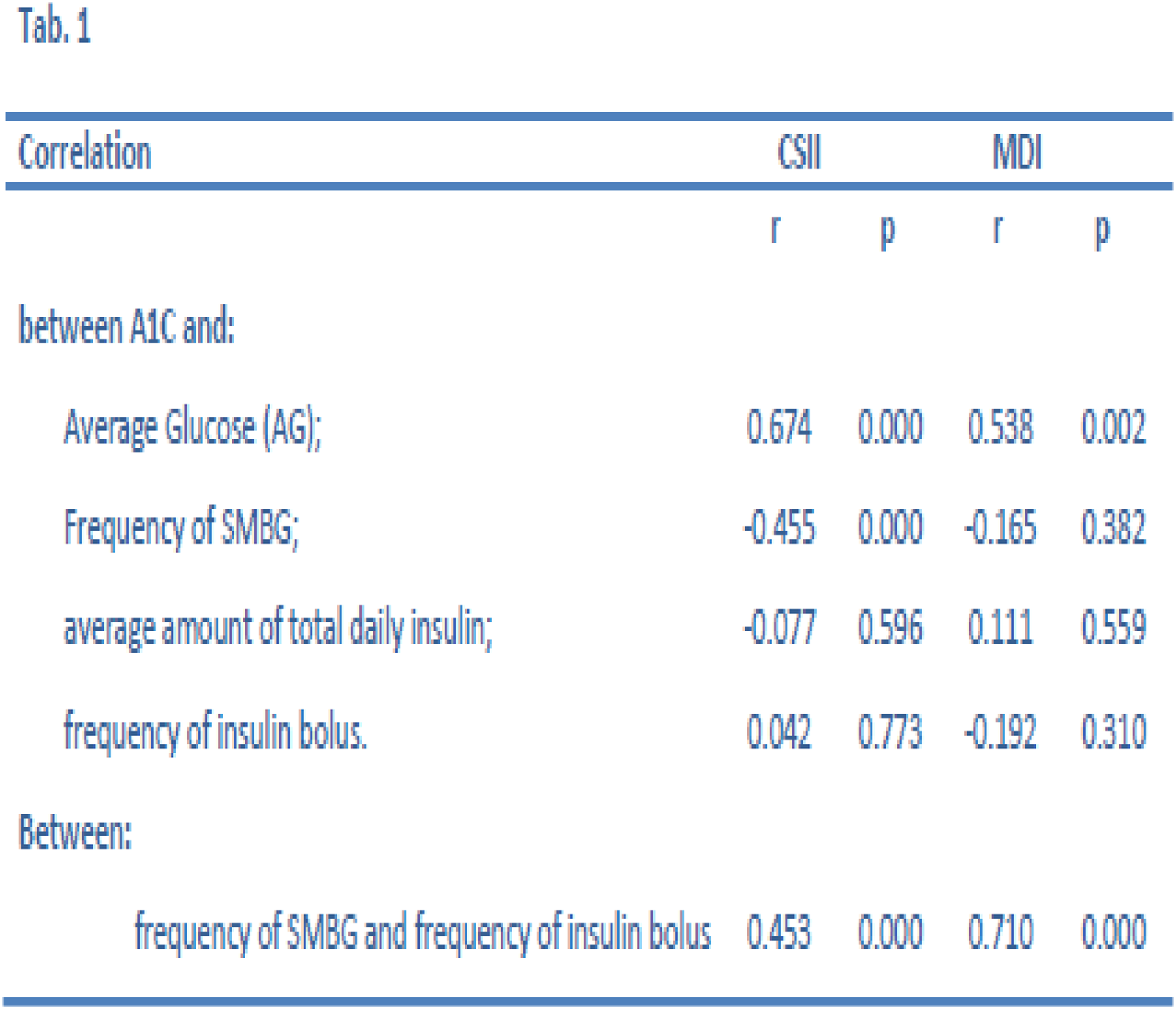
ASP 6 Palermo Ospedale Civico Partinico, Regional Reference Centre for Diabetology and Insulin Pumps, Partinico, Italy
ASP 6 Palermo Ospedale Civico Partinico, Reference Centre for Diabetology and Insulin Pumps, Partinico, Italy
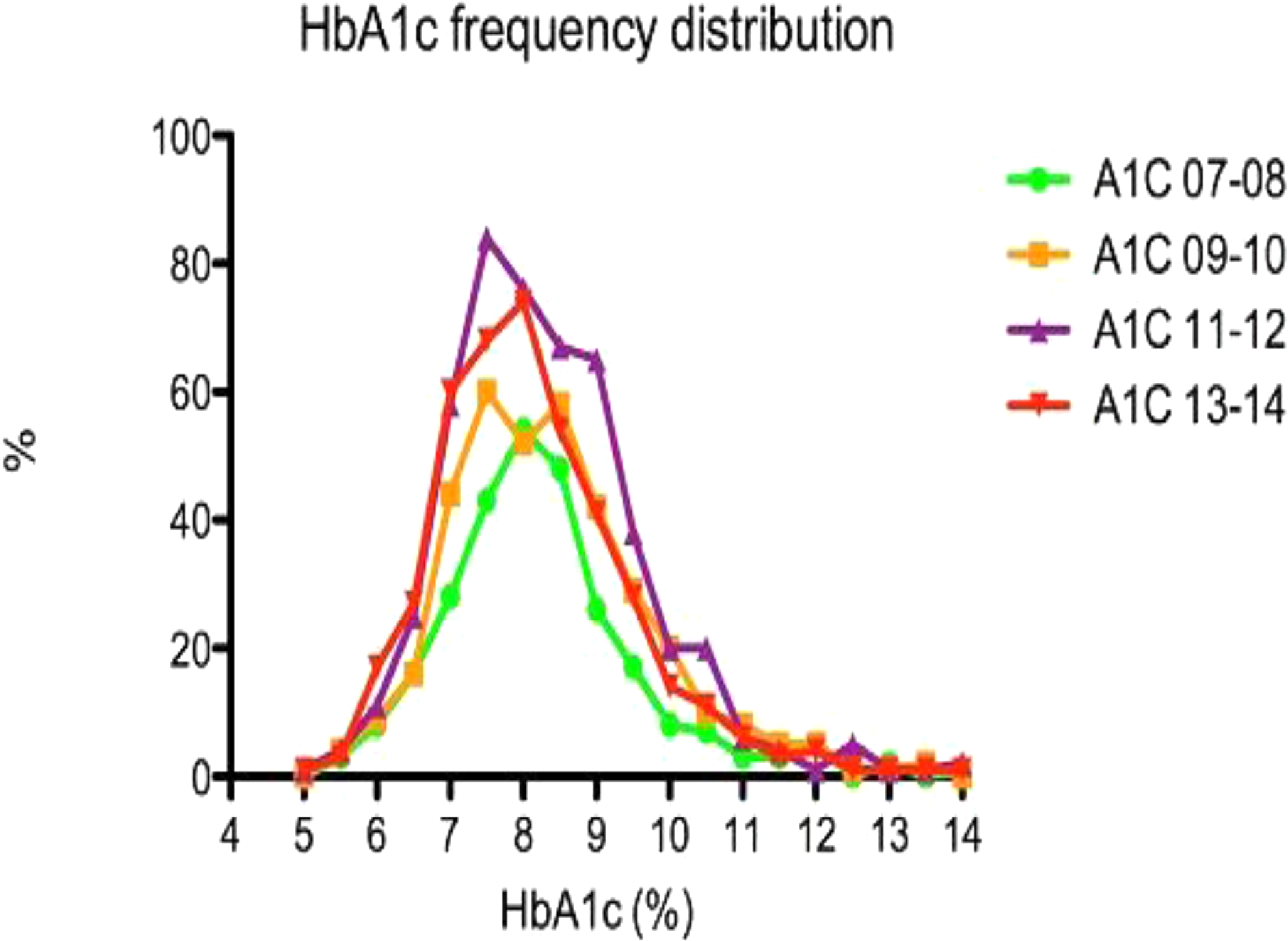
Coimbra Pediatric Hospital, Centro Hospitalar e Universitário de Coimbra (CHUC), Endocrinology and Diabetology Unit, Coimbra, Portugal
Hygeia, Diabetes Center and Clinic, Athens, Greece
Garibaldi-Nesima Hospital- Endocrinology Section, Clinical and Experimental Medicine, Catania, Italy
Kazan State Medical University, endocrinology, Kazan, Russia
Kazan State Medical University, Endocrinology, Kazan, Russia
Kazan State Medical University, Endocrinology, Kazan, Russia
Chinese PLA General Hospital, Diabetes, Beijing, China
BD Technologies, Parenteral Sciences, Research Triangle Park, USA
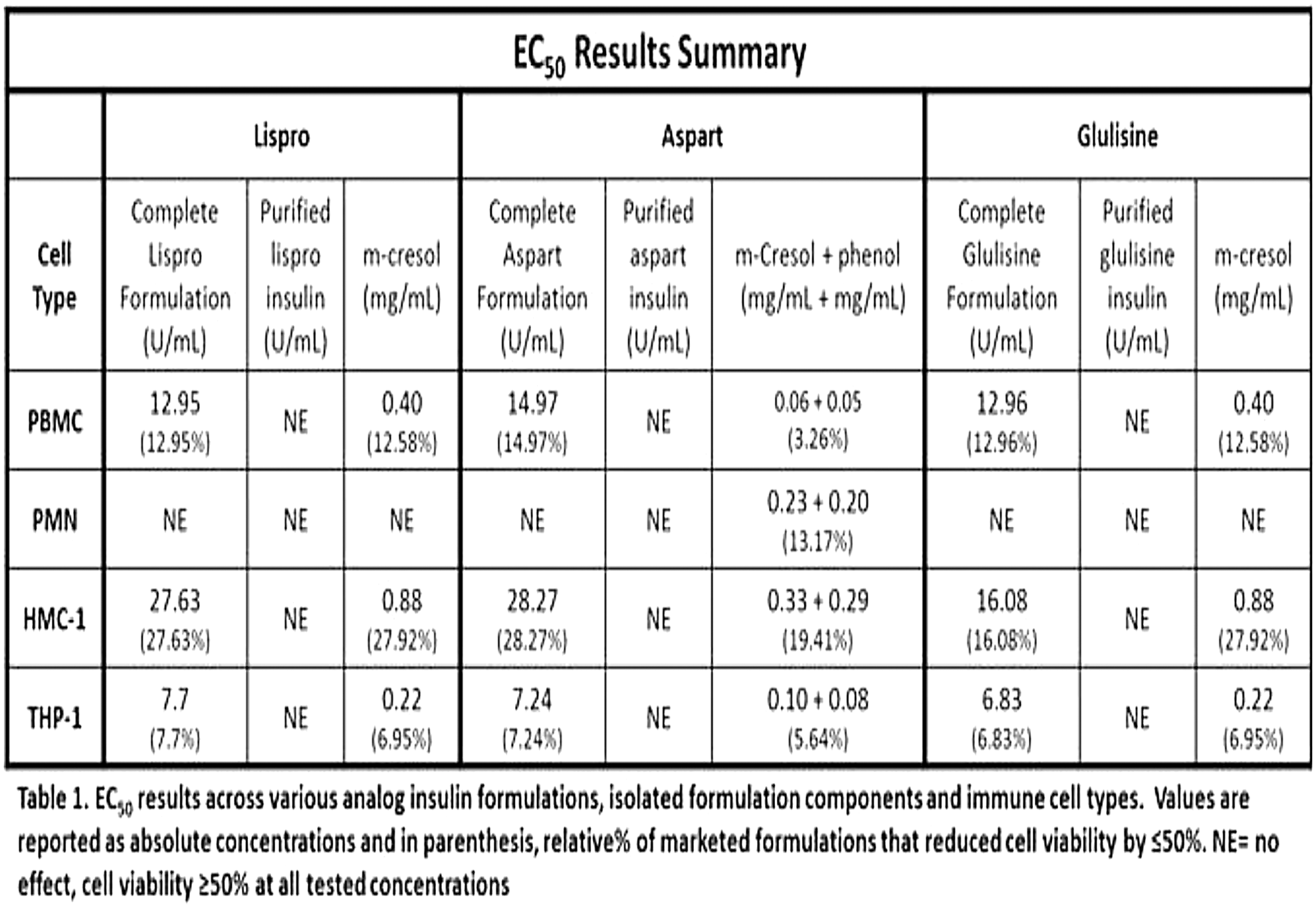
McGill University, Department of Medicine, Montreal, Canada
Studies sponsored by Sanofi (NCT01499082, NCT01499095, NCT01676220)
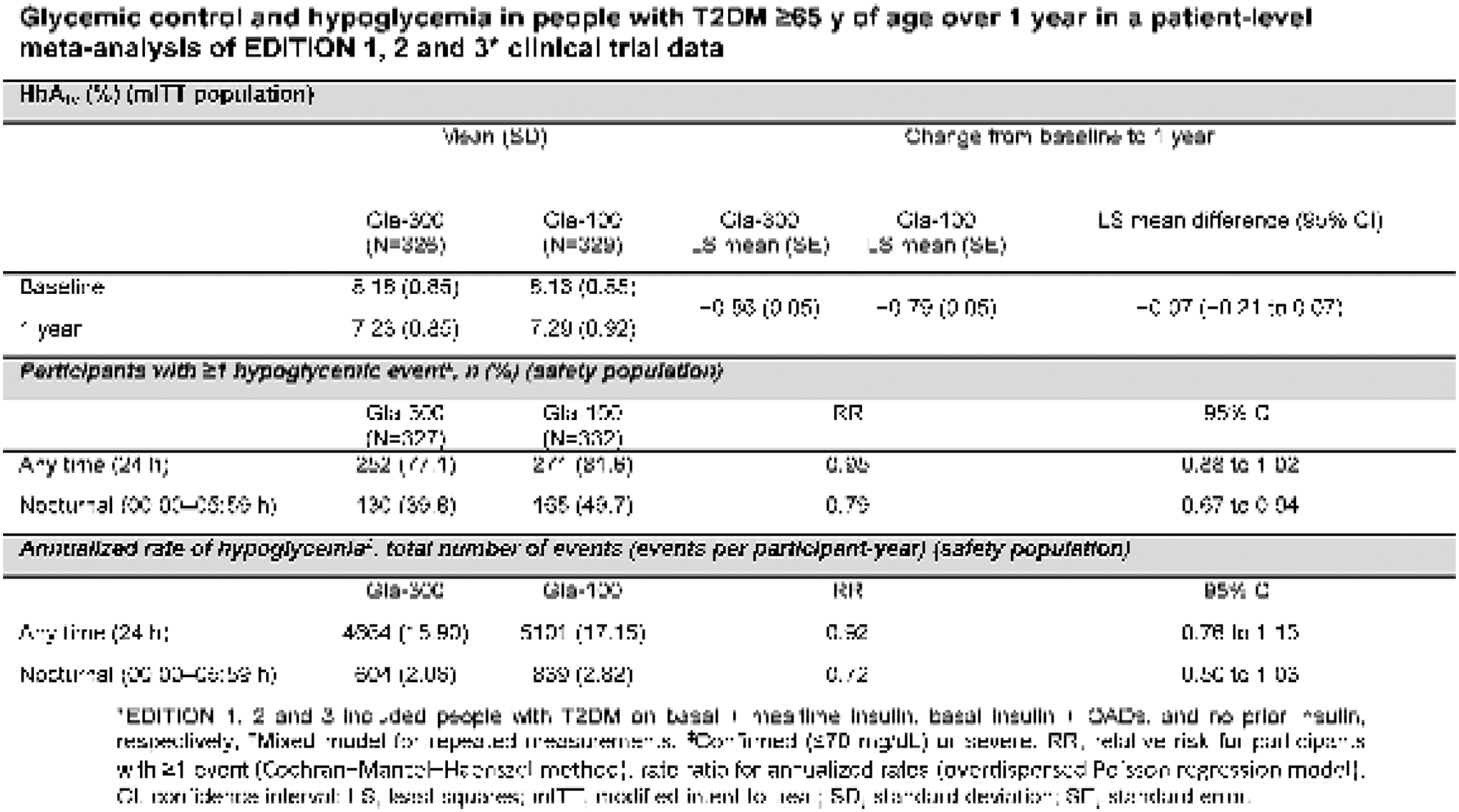
Novo Nordisk A/S, Global Research, Måløv, Denmark
Assistance Publique Hôpitaux de Paris, Bichat Hospital, Paris, France
Studies sponsored by Sanofi (NCT01499082, NCT01499095).
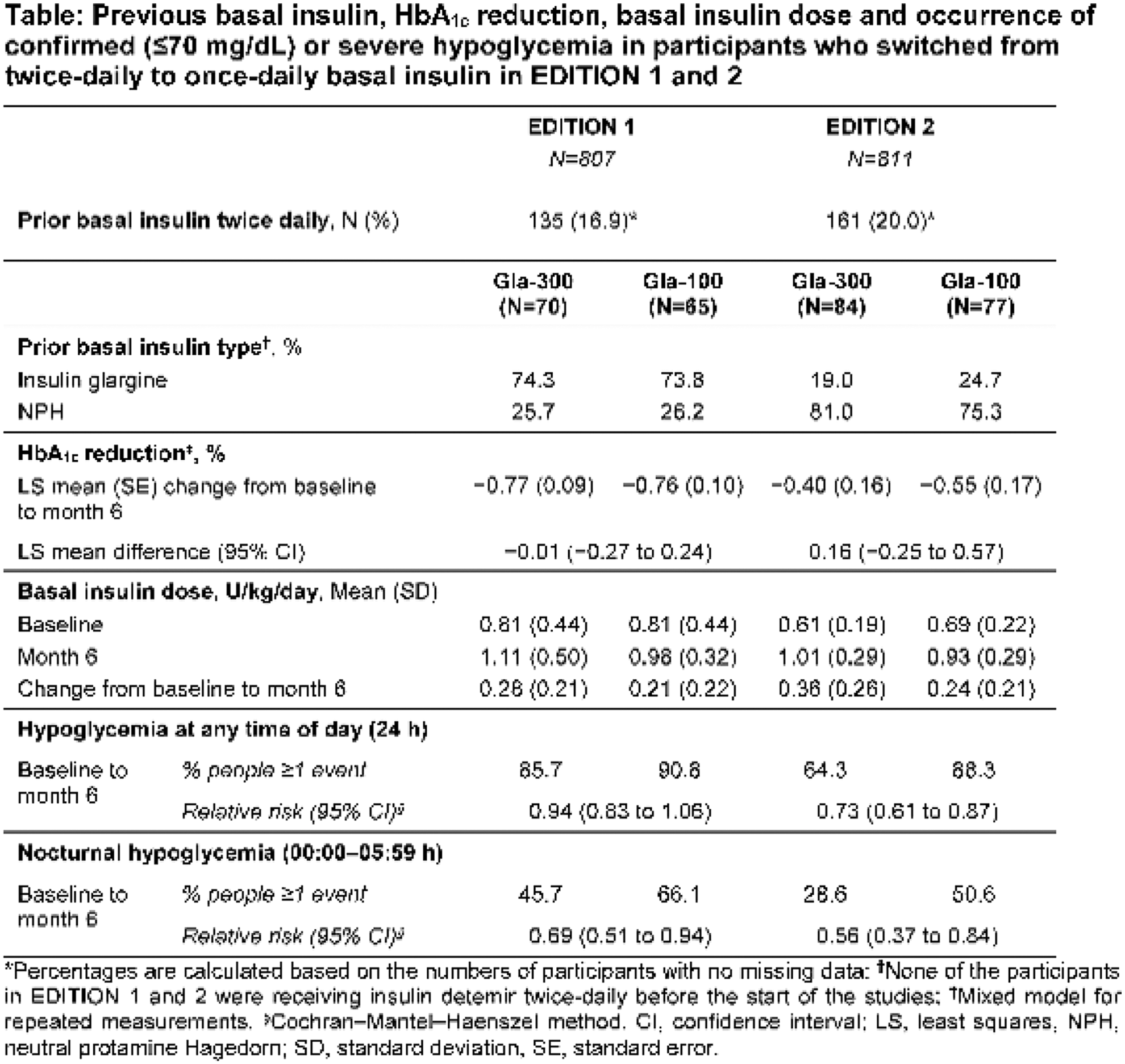
University Military Hospital, Internal Medicine Department, Prague, Czech Republic
Städtisches Klinikum München GmbH-Klinikum Schwabing, Division of Endocrinology and Diabetes, Munich, Germany
Studies sponsored by Sanofi (NCT01499082, NCT01499095, NCT01676220)
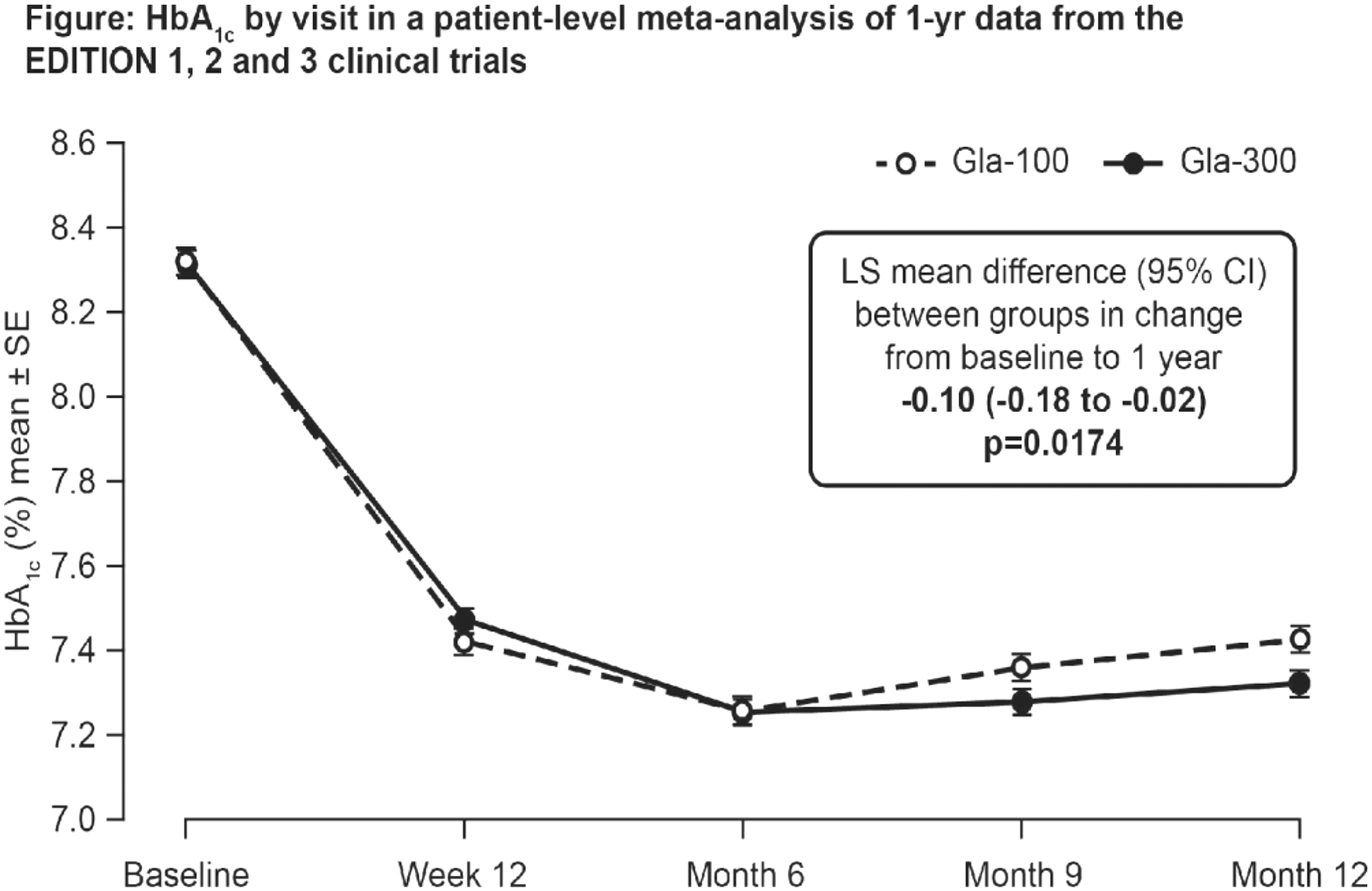
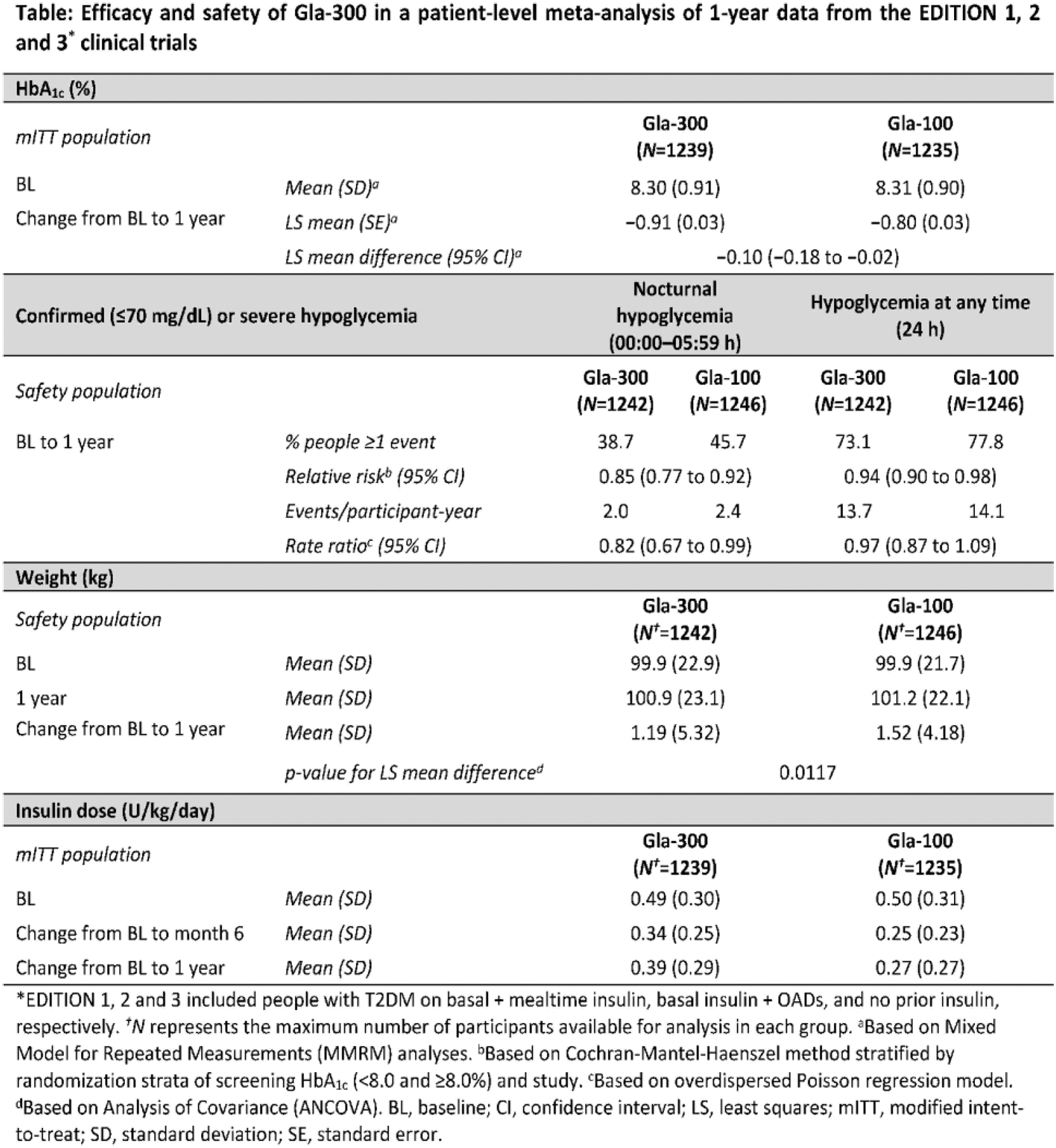
SOUSEIKAI Hakata Clinic, Fukuoka, Japan
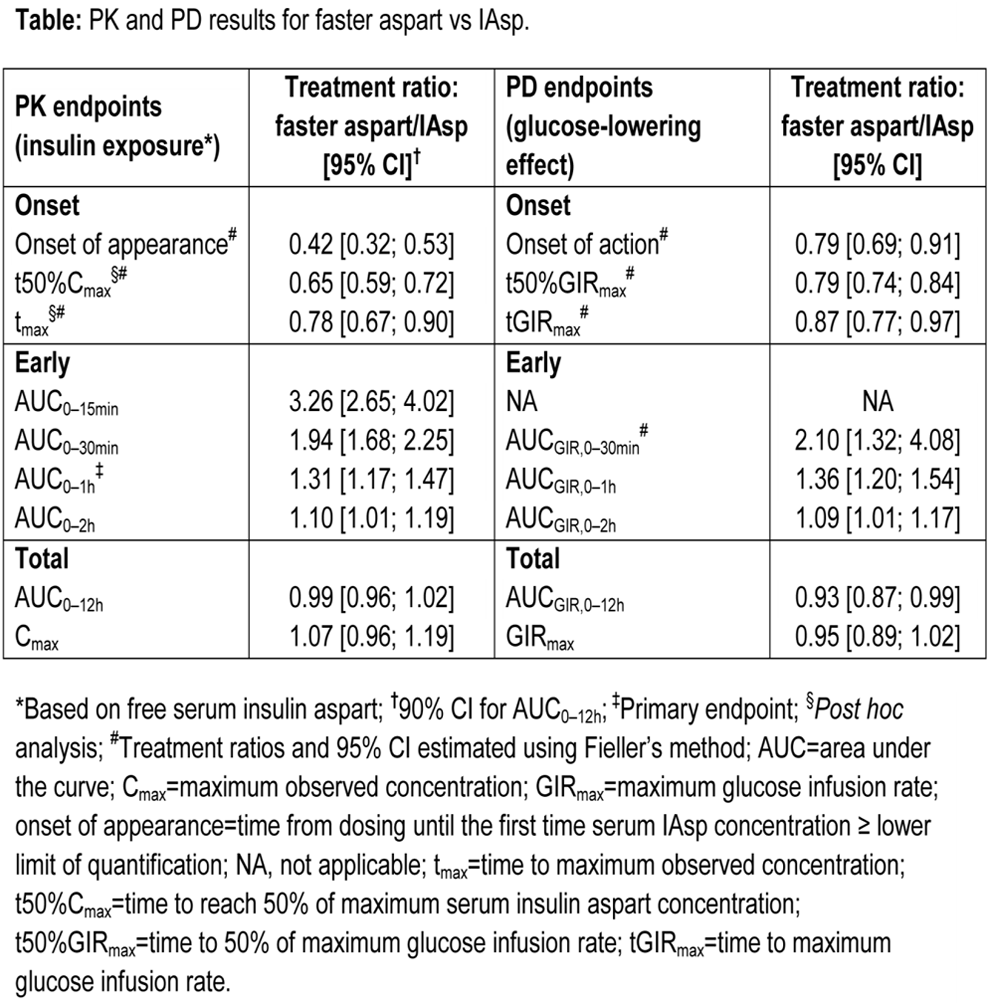
Sanofi, Diabetes Division, Frankfurt, Germany
Study sponsored by Sanofi
University of Perugia, Perugia, Italy
Study was sponsored by Sanofi.
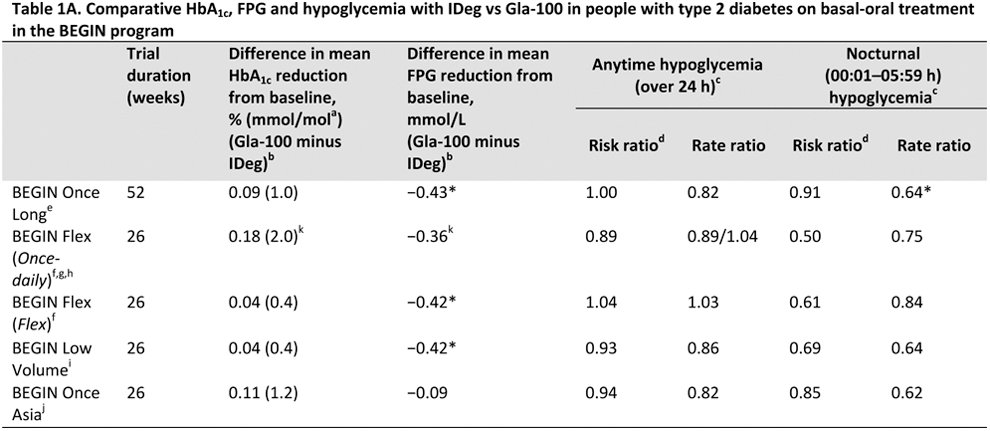

Winnipeg Regional Health Authority Health Sciences Centre, Winnipeg, Canada
An online survey of 386 HCPs and 318 patients with type 2 diabetes on long-acting BI for 6–36 months (BI users: current n = 243; discontinued n = 75) evaluated HCP/patient communication on BI titration in the USA, France and Germany.
The majority of surveyed HCPs agreed that communicating the need for optimal BI titration to patients is important, with >75% of these reporting doing so at the initiation visit (Table). However, only 16–28% of patients recalled discussing titration at their initiation visit and many (32–42%) were unaware of the need to increase the dose over time. While 28–39% of patients recalled discussing the time needed to reach goal with their HCP at the initiation visit, 22–36% felt that additional information on this topic would improve their confidence in self-titrating their BI. Most patients and HCPs agreed that more effective support tools to assist with BI initiation/titration are needed; patients reported that their willingness to self-titrate and confidence in self-management success would be increased by these tools.
In conclusion, the survey showed a marked disconnect in communication between HCPs and patients. Communication could be enhanced by providing effective support and educational tools, which would in turn improve patient understanding of and self-confidence in timely and effective titration and optimal BI use.
This market survey project was conducted by Hall & Partners US LLC and funded by Sanofi.
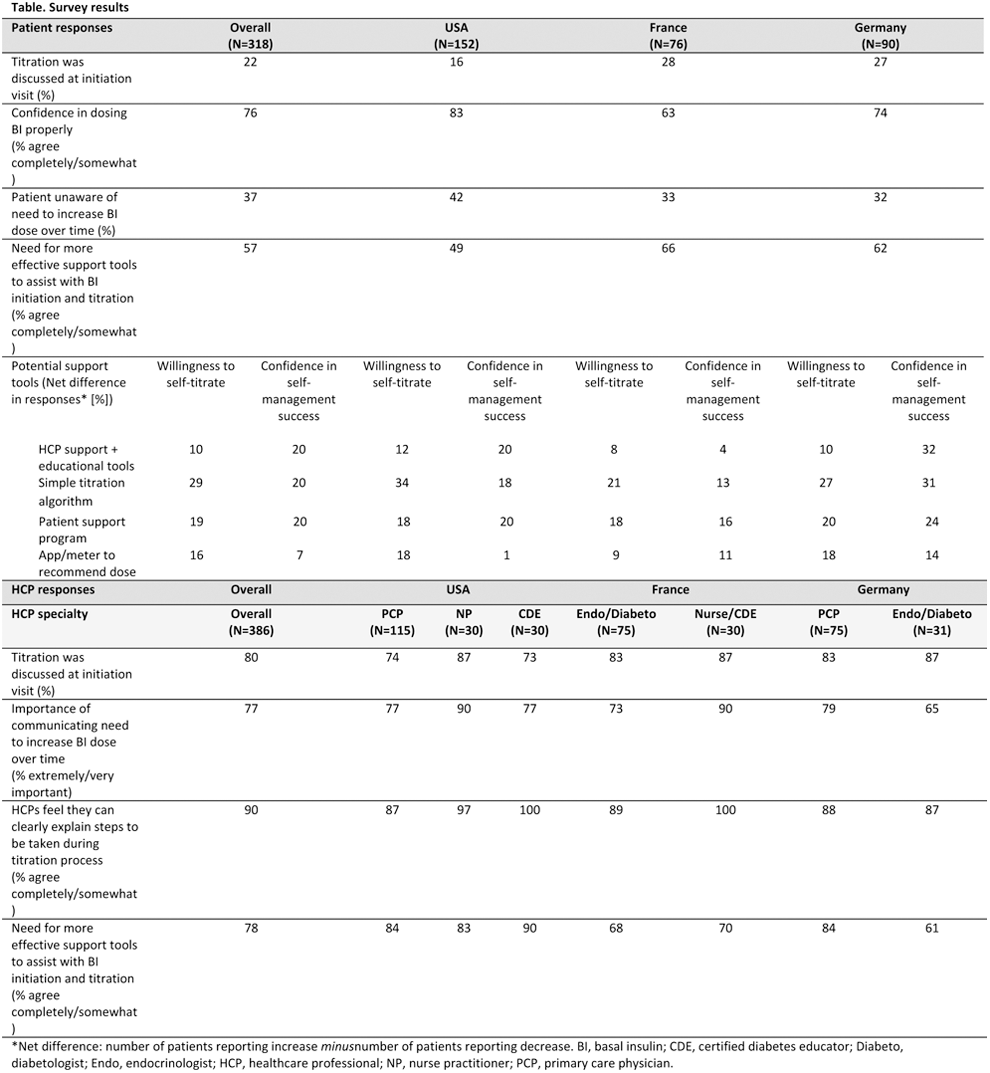
InsuLine Medical, R&D, Petach-Tikva, Israel
Park Nicollet, International Diabetes Center, Minneapolis, USA
Mehr Medical Group, Internal Medicine/Gynecology, Tehran, Iran
Mehr Medical Group, Internal Medicine/Gynecology, Tehran, Iran
Last Mile P/S, Copenhagen, Denmark
Last Mille P/S, Copenhagen, Denmark
CeQur Corporation, Marlborough, USA
Pfützner Science & Health Institute, Diabetes Center and Practice, Mainz, Germany
Pfützner Science & Health Institute, Diabetes Center and Practice, Mainz, Germany
Pfützner Science & Health Institute, Diabetes Center and Practice, Mainz, Germany
Second University of Naples, Department of Pediatrics, Naples, Italy
We evaluated the effects of an indwelling catheter on metabolic control and quality of life in children and adolescents with type 1 diabetes and in their mothers.
The percentage of mothers with distress when giving injections was high (43.5%). Most improved over time (at 1 year only 8%).
Before the starting of the study, 53% of children did not cooperate during insulin injections. At 1 year only 3% of children showed stress for injections.
Profil, Neuss, Neuss, Germany
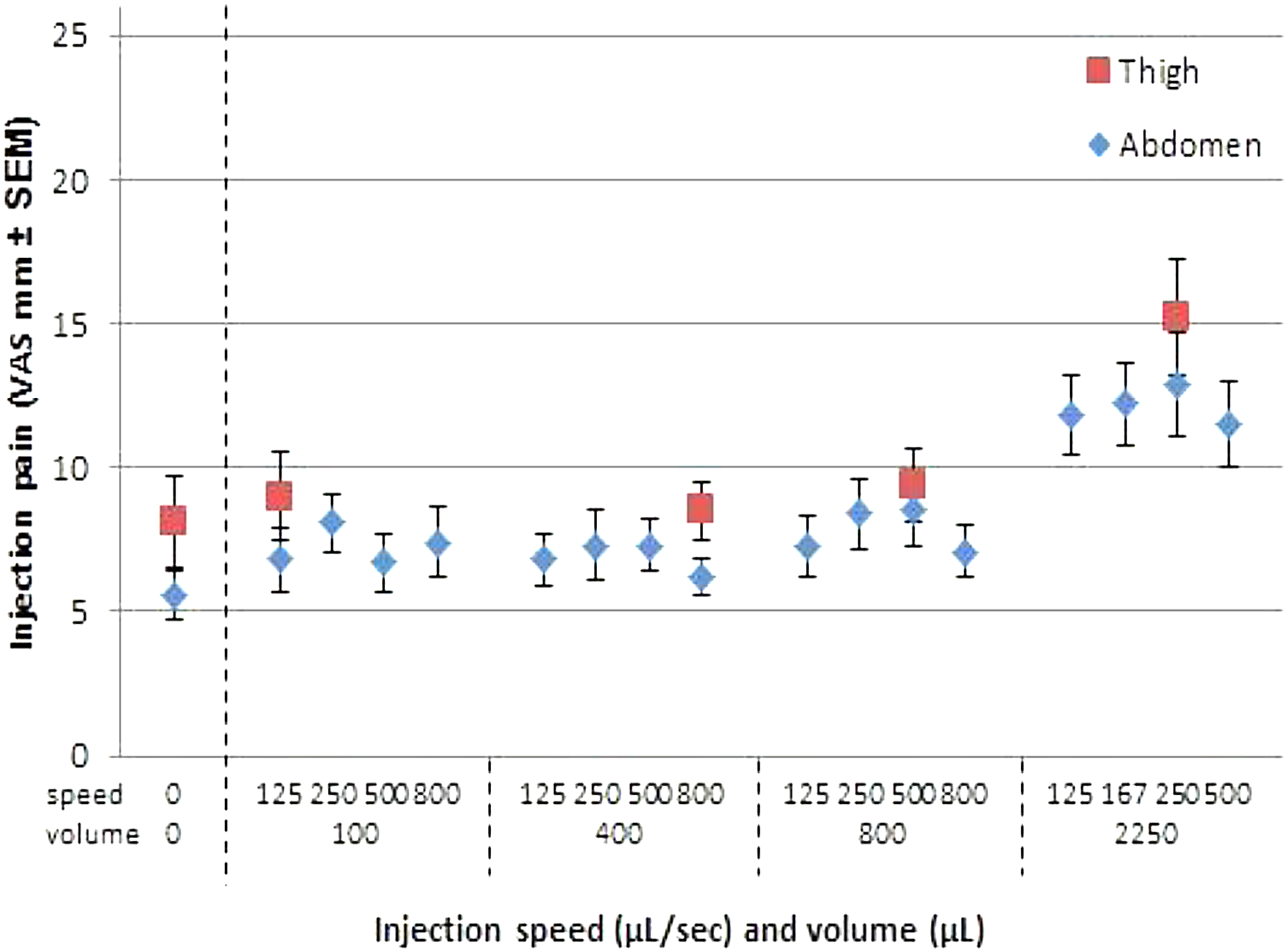
Profil, Neuss, Neuss, Germany
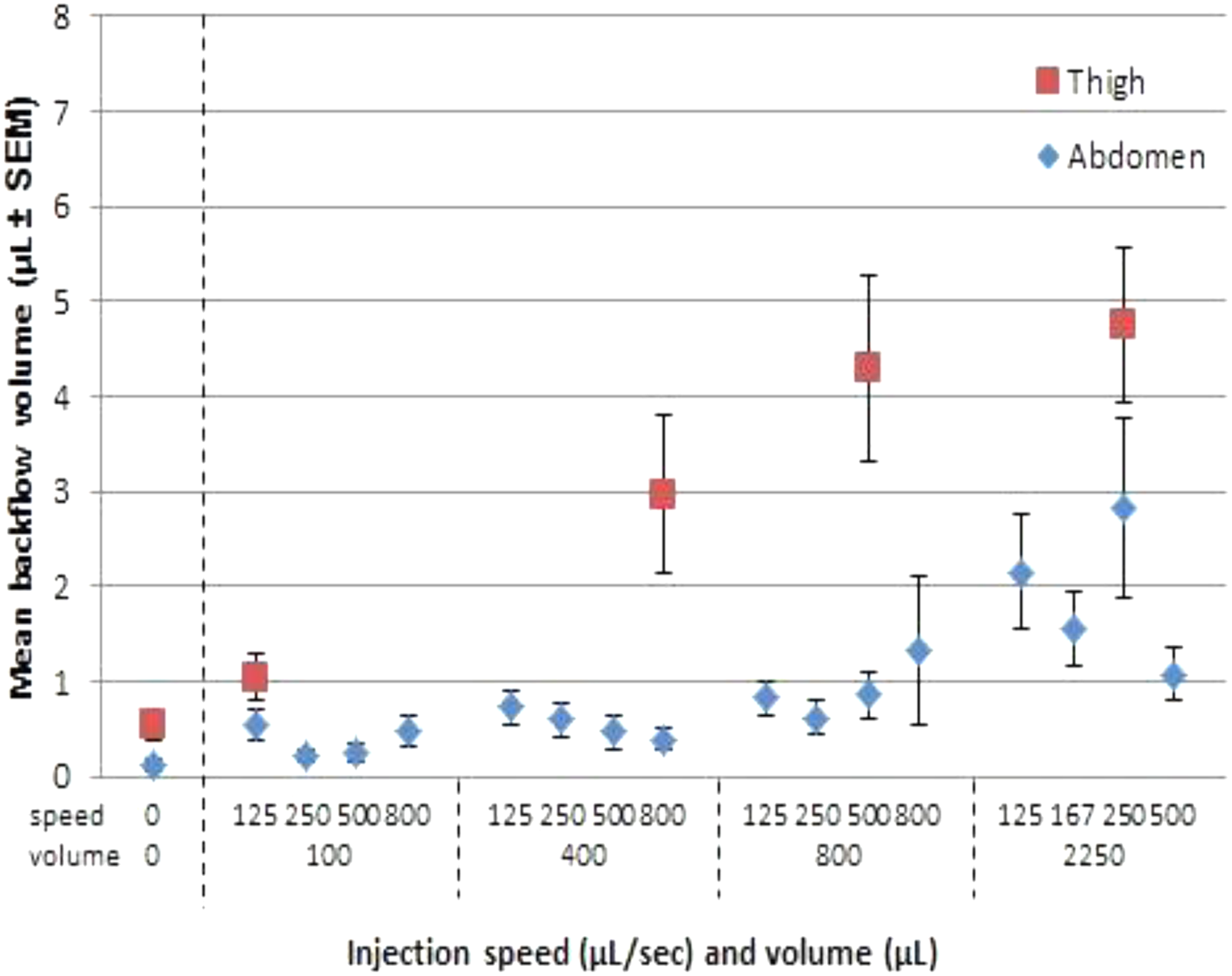
National Cheng Kung University, Pharmacology, Tainan, Taiwan
Chinese University of Hong Kong, School of Life Sciences, Hong Kong, China
Tbilisi, Georgia
Hospital de la Santa Creu i Sant Pau, Endocrinology- EDUAB-HSP- CIBER-BBN, Barcelona, Spain
Federal University Dutse, Biochemistry, Dutse, Nigeria
Seoul National University, Pharmacy, Seoul, Republic of Korea
M.M.University, M.M.College of Pharmacy, ambala cantt, India
Scientific Centre for Family Health and Human Reproduction Problems, Department of Pathophysiology, Irkutsk, Russia
Scientific Centre for Family Health and Human Reproduction Problems, Department of Pathophysiology, Irkutsk, Russia
Chang Gung Memorial Hospital, Endocrinology and Metabolism, Keelung City, Taiwan
SK Chemicals, Life Science R&D Center, Seongnam, Korea
Copenhagen University Hospital Hvidovre, Department of Endocrinology- Research Unit, Hvidovre, Denmark
Mayo Clinic, Ophthalmology, Jacksonville, USA
University of Padova, Department of Information Engineering, Padova, Italy
Artificial pancreas studies in children are increasing and the T1DMS could play an important role in algorithmic development.
The aim of this study is to assess and, if necessary, to update the in silico children included into the T1DMS.

University of Padova, Department of Information Engineering, Padova, Italy
University of Padova, Department of Information Engineering, Padova, Italy
Sir Gangaram Hospital, Endocrinology, Delhi, India
Medtronic, Health Economics and Reimbursement, Northridge, USA
Shanghai Changhai Hospital, Endocrinology, Shanghai, China
Institut für Präventive Medizin IPM, Freiburg, Germany
6 Clinical Hospital, Minsk, Belarus
ATTD 2016 Read By Title
Clinical Hospital No1, Dept. of Pediatric Gastroenterology and Hepatology, Zabrze, Poland
Medical Faculty Comenius University and University Hospital, 2nd Department of Internal Medicine, Bratislava, Slovakia
CNR Institute of Neuroscience, Metabolic Unit, Padova, Italy
NTNU, Department of Engineering Cybernetics, Trondheim, Norway
McGill University, Computer Science, Montreal, Canada
UNQui, Depto. Ciencia y Tecnología, Quilmes, Argentina
University Complutense of Madrid, Computer Architecture Depatment, Madrid, Spain
University of Bern, ARTORG Center for Biomedical Engineering Research, Bern, Switzerland
Mehr Medical Group, Internal Medicine/Gynecology, Tehran, Iran
University Hospital Motol and 2nd Faculty of Medicine- Charles University in Prague- Czech Republic, Department of Paediatrics, Prague, Czech Republic
Montreal Institute of Clinical Research, Research Platform on Obesity Metabolism and Diabetes, Montreal, Canada
Zealand Pharma A/S, Bioanalysis and Pharmacokinetics, Glostrup, Denmark
Instituto Politécnico de Viseu, Escola Superior de Saúde, Viseu, Portugal
National Cheng Kung University, Department of Pharmacology, Tainan, Taiwan
King Faisal Medical City, Family Medicine, ABHA, Kingdom of Saudi Arabia
1. Sinha Institute of Medical Science & Technology- 2. Vidyasagar University, Biochemistry & Diabetology, Kolkata, India
Immanuel Kant Baltic Federal University, Laboratory of Immunology and Cell Biotechnologies, Kaliningrad, Russia
Universidad Católica de Santiago de Guayaquil, Medical School, Guayaquil, Ecuador
Gangnam Severance Hospital - Yonsei University College of Medicine, Internal Medicine, Seoul, Korea
Nizhny Novgorod State Medical Academy, Endocrinology and Internal Medicine, Nizhny Novgorod, Russia
School of Public Health- Tehran University of Medical Sciences, Department of Health Education and Promotion, Tehran, Iran
University of Naples SUN, Department of Woman, Child and of General and Specialized Surgery, Naples, Italy
ENGAIN, Central Research Laboratories, Sungnam-si, Republic of Korea
Hamad General Hospital, Pediatric Endocrine and Diabetes Unit, Doha, Qatar
Endocrinology Research Centre, The Institute of Pediatric Endocrinology, Moscow, Russia
Tianjin Univeristy, Tianjin, China
Centro Hospitalar e Universitário de Coimbra, Serviço de Endocrinologia- Diabetes e Metabolismo, Coimbra, Portugal
University Clinic of Endocrinology, Center for Insulin Pump, Skopje, Macedonia
Pfützner Science & Health Institute, Diabetes Center and Practice, Mainz, Germany
Pfützner Science & Health Institute, Diabetes Center and Practice, Mainz, Germany
Endocrinology Research Centre, Diabetes Institution, Moscow, Russia
DirectSens GmbH, Kolsterneuburg, Austria
Hospital Italiano de Buenos Aires - Argentina, Endocrinologist, CABA, Argentina
Hospital Italiano de Buenos Aires - Argentina, Endocrinología, CABA, Argentina
Institut für Diabetes-Technolgie Forschungs- und Entwicklungsgesellschaft mbH, an der Universität Ulm, Ulm, Germany
ARKRAY-Inc, R&D, Kyoto, Japan
Imperial College, Department of Chemistry & Institute of Biomedical Engineering, London, United Kingdom
University Medical Center Ljubljana, Department of Endocrinology- Diabetes and Metabolic Diseases, Ljubljana, Slovenia
Shanghai Jiao Tong University Affiliated Sixth People's Hospital Shanghai Diabetes Institute, Endocrinology, Shanghai, China
Hamad General Hospital, Pediatric Endocrine and Diabetes Unit, Doha, Qatar
“P&A Kyriakou” Children's Hospital- Athens- Greece, Diabetic Clinic- 2nd Deparment of Pediatrics- University of Athens, Goodi- Athens, Greece
Graduate School of Medicine- Kyoto University, Department of Human Health Sciences, Kyoto, Japan
Arabian Gulf University, Physiology, Manama, Bahrain
University Hospital of North Norway, Norwegian Centre for Integrated Care and Telemedicine, Tromsø, Norway
Centro Hospitalar e Universitário de Coimbra, Endocrinology- Diabetes and Metabolism, Coimbra, Portugal
University of Brasilia, Biomedical Engineering, Brasilia, Brazil
University of Colorado- Boulder CO, Language- Development and Cognition Lab, Randolph, USA
The University of Dąbrowa Górnicza, Department of Computer Science, Dąbrowa Górnicza, Poland
Moscow Regional Scientific Research Clinical Institute, Moscow, Russia
Moscow Regional Scientific Research Clinical Institute, Moscow, Russia
University of Brasília, Doce Desafio Program, Brasília, Brazil
Arabian Gulf University, College of Medicine, Manama, Bahrain
Wolfson Medical Center, Department of Acute Care, Holon, Israel
STU Faculty of Electrical Engineering and Information Technology, URK, Bratislava, Slovakia
IRCCyN, Commande, Nantes, France
University of Newcastle, Electrical Engineering and Computer Science, Newcastle, Australia
Arabian Gulf University, Physiology, Manama, Bahrain
Czech Technical University in Prague, Faculty of Biomedical Engineering, Prague, Czech Republic
Saint-Petersburg Medical University, Endocrinology, Saint-Petersburg, Russia
Saint-Petersburg Medical University, Endocrinology, Saint-Petersburg, Russia
Saint-Petersburg Medical University, Endocrinology, Saint-Petersburg, Russia
University of Pavia, Department of Electrical- Computer and Biomedical Engineering, Pavia, Italy
School of Public Health- Tehran University of Medical Sciences, Department of Health Education & Promotion, Tehran, Iran
School of Public Health- Tehran University of Medical Sciences, Department of Health Education & Promotion, Tehran, Iran
Hamad General Hospital, Pediatric Endocrinology/Diabetes, Doha, Qatar
Hôpital Bichat, Diabetology, Paris, France
A.O. Ospedale Niguarda Ca' Granda, Diabetes Unit, Milano, Italy
AHEPA University General Hospital, Department of Nutrition and Dietetics, Thessaloniki, Greece
AHEPA University General Hospital of Thessaloniki, 1Department of Nutrition and Dietetics, Thessaloniki, Greece
São João Hospital, Pediatrics, Porto, Portugal
Federal Almazov North-West Medical Research Centre, Endocrinology, Saint-Petersburg, Russia
Federal Almazov North-West Medical Research Centre, Endocrinology, Saint-Petersburg, Russia
University Clinic of Endocrinology, National Center for Insulin Pump, Skopje, Macedonia
CeQur, Marlborough, USA
University of Hanyang, Pharmacy, Ansan, Republic of Korea
Cairo University, Faculty of Medicine, Cairo, Egypt
Sapienza University of Rome, Rome, Italy
Euromedica General Clinic, Endocrinology- Metabolism and Diabetes, Thessaloniki, Greece
Dongguk University-Seoul, College of Pharmacy, Goyang, Republic of Korea
Uimyung Research Institute for Neuroscience, Sahmyook University, Seoul, Republic of Korea
Late Breaking Abstract
Studies sponsored by Sanofi (NCT01499082, NCT01499095, NCT01676220).
