
Abstract
G
The huge range of physiological, hormonal, symptomatic, and cognitive responses triggered by the fall in blood glucose is mainly caused by elevated levels of epinephrine, but epinephrine responses to hypoglycemia might become impaired in type 1 diabetes (T1D), 3 leading to hypoglycemia unawareness. So, T1D patients can develop a high risk to fall in asymptomatic hypoglycemia, further reducing the efficacy of the counter-regulatory responses to future hypoglycemia. 4
In the literature, the alterations of cerebral functioning consequent to the hypoglycemic condition have been investigated through both qualitative and quantitative analyses of the electroencephalogram (EEG) signal. The first studies aimed to see whether cognitive dysfunction was mirrored by altered EEG activity during hypoglycemia date back to more than 60 years ago. Specifically, abnormal EEG activity defined as slow potentials was observed in ref 5 and distorted EEG waves with higher amplitude during hypoglycemia were reported in ref. 6
In the past decades, the increase in the power of low frequency bands, that is, delta and theta frequency range, during hypoglycemia in T1D patients was assessed in many studies in the literature. 7 –10 In Figure 1, it is even qualitatively observable by visual inspection that the EEG signal in the hypoglycemic condition originates from a process of higher amplitudes in the low frequency bands and reveals greater regularity. More subtle changes induced by hypoglycemia, related to the altered complexity of the overall system, have been recently revealed by the use of nonlinear methods, that is, multiscale sample entropy and fractal analyses. Indeed, during hypoglycemia, the EEG signal is more regular, more uniform, less complex than that during euglycemia. 11,12
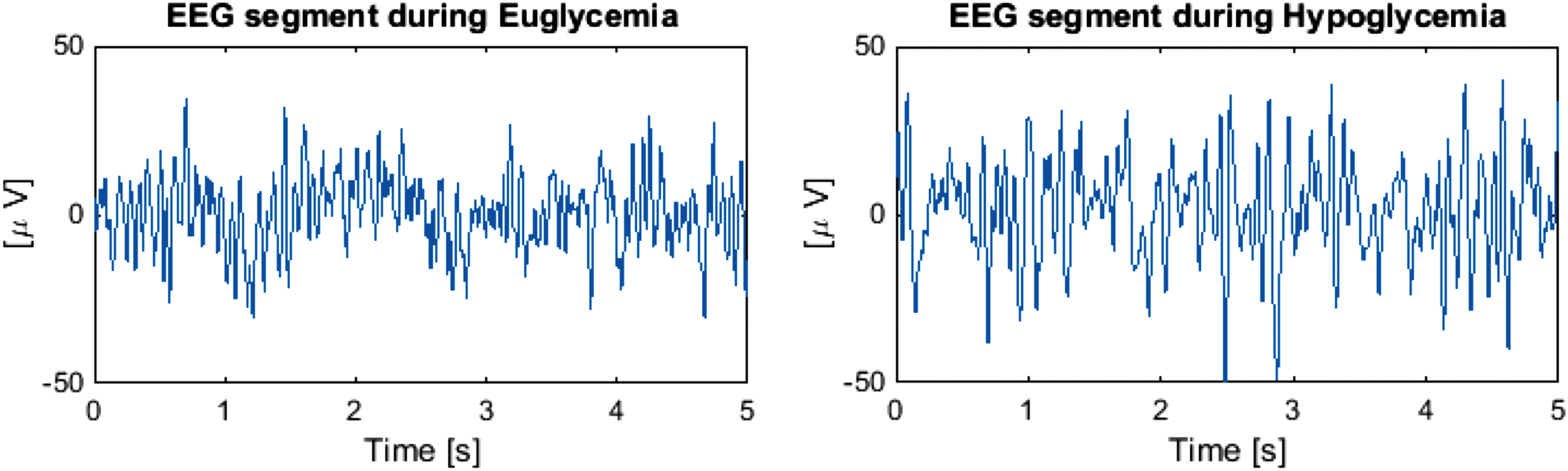
Representative electroencephalogram (EEG) signal (C4-A1A2 derivation) measured in a hospitalized type 1 diabetes patient who underwent a hyperinsulinemic–hypoglycemic clamp: 5 s interval of signal during euglycemia (left panel) and hypoglycemia (right panel). Data taken from Rubega et al. 14
Other studies exploited approaches resorting to multivariate analysis, that is, several EEG channel derivations are considered at the same time. In particular, the functional reaction of the brain to hypoglycemia also showed a decrease in connectivity by computing the networks of directional effects of one EEG recording channel over another. 13,14 Specifically in ref, 14 this decrease in the connectivity was seen in the path from the occipital lobes to the temporal and central lobes during hypoglycemia, most likely as a result of the alterations of mental and perceptual functions during this critical glycemic state.
The demonstrated EEG abnormalities in the hypoglycemic pathological condition suggested a possible use of the brain as a biosensor to detect hypoglycemia in T1D through EEG monitoring by subcutaneous electrodes and real-time data processing by means of a multiparameter algorithm. 15 A research prototype device, able to measure the EEG signal by subcutaneous electrodes and then analyze and classify it in real time, has been proposed for the detection of hypoglycemia events 16 ; however, this EEG-based hypoglycemia detection device still needs to be tested in a clinical setting.
So far, the notion that hypoglycemia affects EEG rhythms is well established, 17 –19 but the adaptation of neurological function to hypoglycemia is open to discussion in both healthy and diabetic subjects.
The article by Sejling and colleagues published in this issue of Diabetes Technology & Therapeutics assesses how hypoglycemia-associated changes are affected by an antecedent episode of hypoglycemia in T1D patients. 20 Despite subtle differences seen in cognitive function and counter-regulatory hormonal response, the study of Sejling and colleagues affirms that hypoglycemia-associated EEG changes are not affected by an antecedent episode of hypoglycemia, in both hypoglycemia aware and unaware T1D patients. This hypothesizes that there is not an immediate adaptation of the brain to acute hypoglycemia.
Sejling and colleagues underline that the effect of recurrent hypoglycemia on the brain seems controversial as reported in the literature. For instance, a single episode of mild antecedent hypoglycemia attenuated several aspects of cognitive dysfunctions during subsequent hypoglycemia in healthy subjects, 21 whereas glycemic thresholds for hypoglycemic cognitive dysfunction did not seem to shift after antecedent hypoglycemia. 22
Moreover, Sejling and colleagues find an increase in theta, alpha, and alpha–theta amplitudes during hypoglycemia than during euglycemia, and these hypoglycemia-associated EEG changes do not differ between the two groups, that is, aware and unaware subjects, and the two experimental days. This seems not in line with the study in T1D made in ref 23 in which a single episode of hypoglycemia resulted in both high glycemic thresholds for automatic and symptomatic responses to hypoglycemia and impaired physiological defense against this pathological state the next morning in T1D patients. Furthermore, an interesting finding reported in ref 24 showed an early and immediate reduction in vigilance and an early increase in EEG slow waves after even a slight lowering of blood glucose in severely hypoglycemia unaware patients than in aware patients.
In conclusion, although hypoglycemic events in patients affected by T1D were proved to be associated with measurable EEG changes, the level of adaptation of neurological function to hypoglycemia is still a debatable question. The study of Sejling and colleagues shed light on this problematic aspect, but there is room for further investigation, also using more sophisticated signal processing methodologies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.