
Abstract
Background: Hemoglobin A1c is an excellent population health measure for the risk of vascular complications in diabetes, while continuous glucose monitoring (CGM) is a tool to help personalize a diabetes treatment plan. The value of CGM in individuals with type 1 diabetes (T1D) has been well demonstrated when compared with utilizing self-monitoring of blood glucose (SMBG) to guide treatment decisions.
CGM is a tool for patients and clinicians to visualize the important role that diet, exercise, stress management, and the appropriate selection of diabetes medications can have in managing type 2 diabetes (T2D). Several diabetes organizations have recently reviewed the literature on the appropriate use of CGM in diabetes management and concluded CGM may be a useful educational and management tool particularly for patients on insulin therapy. The indications for using CGM either as a clinic-based loaner distribution model for intermittent use (professional CGM) or a CGM system owned by the patient and used at home with real-time glucose reading (personal CGM) are only beginning to be addressed in T2D. Most summaries of CGM studies conclude that having a standardized glucose pattern report, such as the ambulatory glucose profile (AGP) report, should help facilitate effective shared decision-making sessions.
The future of CGM indications for the use of CGM is evolving rapidly. In some instances, CGM is now approved for making medication adjustments without SMBG confirmation and it appears that some forms of CGM will be approved for use in the Medicare population in the United States in the near future. Many individuals with T1D and T2D and their care teams will come to depend on CGM as a key tool for diabetes management.
Introduction
G
While HbA1c is an established marker for the risk of vascular complications and remains the gold standard to assess glycemic control in a population of individuals with T2D, the use of CGM may be helpful for making the personalized therapy decisions desired in the era of precision medicine. 3,4 We will explore current data regarding the use of CGM in T2D and the importance of a standardized glucose report as part of a shared decision-making (SDM) encounter.
Studies of CGM Use in T2D
In recent years, there have been more CGM studies in patients with T2D, with particular interest in those on insulin-based therapy. The focus of most CGM studies in T2D is efficacy, hypoglycemia, and glucose variability. There is also a role for CGM use in special populations as well as clinical research, which has been reviewed elsewhere. 2
Studies of Efficacy and HbA1c Reduction
Vigersky et al. conducted a trial of 100 T2D patients not on prandial insulin. 6 Patients were on therapies, including diet and lifestyle only, or various other combinations of antihyperglycemic therapies, including basal insulin. Subjects were randomized to RT-CGM (real-time CGM, which measured interstitial glucose every 5 min giving a total of 288 data points over a 24-h period) used intermittently (2 weeks on, 1 week off) over 12 weeks compared to SMBG four times per day. The 12-week intervention was followed by a 40-week follow-up. 7 They showed a decrease in the RT-CGM group's mean unadjusted HbA1c of 1.0% (vs. 0.5% in the SMBG group) at week 12, with similar results sustained at week 52 (decrease of 0.8% in RT-CGM group vs. 0.2% in SMBG group). HbA1c reduction occurred in the absence of medication intensification or increased hypoglycemia, suggesting that one of the benefits of RT-CGM in T2D is behavior and lifestyle modification.
Fonda et al. showed that intermittent use of RT-CGM may be optimally suited for motivating or helping avoid burnout in T2D patients. 8 Even in patients not on insulin, there is demonstrated benefit to RT-CGM use and HbA1c reduction, presumably from improved lifestyle and behavior changes. 9 Other groups have also described a potential benefit through changing lifestyle and patient motivation to achieve glycemic goals. 10 RT-CGM also appears to be more beneficial in those with higher starting HbA1c. 8 Similar improvements in HbA1c with intermittent RT-CGM use in T2D have been seen in other studies. 11
Poolsup et al., who did a recent meta-analysis of four randomized controlled trials looking at RT-CGM in T2D, showed a pooled mean difference in HbA1c of −0.31% in T2D patients using CGM. 12
Pepper et al. in 2012 used CGM in a mixed T1D and T2D population and did not demonstrate a benefit in HbA1c reduction. 13 This retrospective analysis of 104 consecutive patients undergoing a blinded 3-day CGM study in a single center (the decision to complete the CGM study was based on an individual endocrinologist judgment) showed HbA1c did not significantly decrease (7.7% before and 7.8% up to 7 months after the CGM). Fifty-nine percent of the patients had T2D, however, no subgroup analysis between T1D/T2D was performed.
The Daily Injections and Continuous Glucose Monitoring in Diabetes (DIaMonD) study is a 6-month randomized control trial comparing the effectiveness of using RT-CGM versus SMBG to optimize glycemic control in individuals with T1D and T2D using multiple daily injections. 14,15 The data from the T1D cohort of the DIAMOND trial showed that using RT-CGM in patients with T1D significantly reduced the HbA1c compared to using standard SMBG to guide therapy decisions. The T2D cohort of DIAMOND is being analyzed separately and is expected to be submitted for publication in 2017. It will be very important to not only see if RT-CGM in patients with T2D on multiple daily injections reduces the HbA1c more than those using SMBG but to also assess the level of daily use of CGM and the degree of satisfaction with this technology in T2D.
Studies of Hypoglycemia
Zick et al. showed in a single-arm, open-label study of 367 patients that 72 h of CGM use in T2D patients on multiple daily injections of insulin can reveal more hypoglycemia (≤60 mg/dL) than by using SMBG alone, with 56.9% of patients having hypoglycemia by CGM, compared with only 26.4% of hypoglycemia detected by conventional SMBG. 16
Pazos-Couselo et al. in 2015 completed an observational, prospective study of 63 patients with T2D on insulin (basal only, premixed or basal/bolus, average age 62.7 years). 17 Patients were on a stable regimen (no significant dose adjustments in the prior 2 months) and were asked to complete two SMBG readings (pre- and post-meal) per day, rotating from breakfast, lunch, and dinner every day for 8 weeks. During the ninth week, they wore blinded CGM.
Pazos-Couselo et al. found significantly higher percentages of hyperglycemic (61.1% vs. 50.8%; P = 0.047) and hypoglycemic episodes observed by CGM rather than by SMBG (3.8% vs. 1.7%; P = 0.016). 17 More hypoglycemia was seen with CGM than by SMBG (79.2 episodes/patient/year vs. 16.6 episodes/patient/year). Moreover, 36% of hypoglycemic events detected by CGM were nocturnal, and 19% of patients had hypoglycemia detected by CGM but without any hypoglycemia by SMBG measurements. In patients with T2D treated with a variety of insulin regimens, CGM revealed a more comprehensive picture of hypoglycemia even during a period of stable therapy.
Klimontov and Myakina in 2017 used blinded CGM in 83 insulin-treated elderly inpatients (65–80 years old) to assess risk for nocturnal hypoglycemia, defined as a CGM blood glucose of ≤70 mg/dL from 00:00 to 05:59 AM. 18 Nocturnal hypoglycemia was observed in 68 of 176 twenty-four-hour recordings (39%). Lower daytime (06:00–22:59) mean glucose and higher overall mean absolute glucose corresponded with higher risk for nocturnal hypoglycemia. Interestingly, although not surprisingly, having daytime hypoglycemia was the more reliable predictor of nocturnal hypoglycemia (accuracy of 75.6%, P = 0.0004). Thus, CGM may be useful in predicting hypoglycemia in high-risk populations such as elderly patients using insulin. Furthermore, this study suggests a possible role for CGM use in the inpatient setting, which has been of increasing interest. 19
Glucose Variability
Although HbA1c has been the standard outcome measurement for most recent clinical trials, many researchers are beginning to acknowledge the importance of glucose variability, in addition to HbA1c, in T2D management. 20 CGM is the ideal tool to assess glucose variability and has recently been used in several studies to assess the effect of pharmacologic interventions on glucose control and variability in T2D.
Manski-Nankervis et al. did a post hoc analysis of patients in the INITIATION study, which tested an insulin initiation algorithm for T2D patients not at goal on maximum oral therapy (up to four oral agents). 21 Using RT-CGM in 78 subjects followed for 24 weeks, they showed that insulin initiation reduced hyperglycemia but not glucose variability. With newer noninsulin therapies available that have less risk for hypoglycemia, RT-CGM has been a useful tool to study glucose variability, in addition to HbA1c lowering, in studies evaluating SGLT2 inhibitors, GLP-1 receptor agonists, and other novel combination therapies. 21
The FLAT-SUGAR study randomized 102 patients on metformin and basal/bolus insulin therapy to 26 weeks of either maintenance on basal/bolus insulin or changing to basal insulin plus the glucagon-like peptide 1 receptor agonist (GLP1-RA) exenatide twice daily before the two largest meals of the day. 22 The mean age was 62 years, and nearly 1/3 of patients had a previous cardiovascular event. Comparing CGM at baseline to the end of the study, the exenatide group had a significant lowering in glucose variability measured by coefficient of variation (−2.4 vs. 0.4 in the basal/bolus group, P = 0.047). HbA1c did not change nor were hypoglycemia events significantly different; however, there was a non-significant trend to improvements in other glycemic variability measurements. While a relatively small and short study, this study suggests that larger, longer studies may be needed to assess correlation between glucose variability and complications, including cardiovascular outcomes. Indeed, other studies have correlated glycemic variability to risk of diabetes complications, notably neuropathy and retinopathy. 23 –25
Bajaj et al. demonstrated reduced glucose variability with basal insulin and GLP-1 RA therapy compared to other insulin-based regimens. 26 In 160 T2D patients with HbA1c ≤7.5%, using blinded CGM for 6 days, this study showed that basal insulin with GLP-1 RA therapy reduced the standard deviation of daily glucose compared to basal insulin with oral medications, basal/bolus regimen, and premixed insulin regimens (P = 0.03, P = <0.01, and P = 0.01, respectively). This observation persisted even when adjusted for HbA1c. CGM use in clinical trials will likely proliferate as our understanding of the risks of glucose variability expands. 27
Flash CGM technology has been available for personal use in adults since 2014 in Europe and is approved in the United States for professional use. 28–29 The flash CGM device includes a small, single-use sensor worn on the back of the arm that is factory calibrated (does not require patient to make finger stick calibrations) and can be worn for up to 14 days. It measures interstitial fluid glucose every 15 min and automatically stores the data, which can be retrieved and downloaded by a receiver swiped over the sensor.
Haak et al. conducted a randomized controlled trial that looked at 224 patients on intensive insulin therapy (prandial and basal insulin, prandial only, or insulin pump therapy) for T2D randomized to use the personal flash CGM (using the Abbott FreeStyle Libre system, Abbott Diabetes Care, Witney, United Kingdom) versus SMBG over a 6-month time period. 30 The HbA1c primary outcome reduction was similar in both groups (−0.29% ± 0.07% in the study group compared with −0.31% ± 0.09% in control), however, patients <65 years old did show a significant difference in HbA1c (−0.49% ± 0.13% compared with −0.05% ± 0.10%, P = 0.0081). Time in hypoglycemia in the CGM group was reduced by 43% for glucose <70 mg/dL and 53% for glucose <55 mg/dL. The number of SMBG checks for the CGM group also was reduced, from an average of 3.8 to 0.3 tests/day at the end of the study. Treatment satisfaction was higher in the CGM group, and no severe hypoglycemia episodes were seen in either the CGM or SMBG group.
Taken together, the studies have shown that CGM use in patients with T2D can not only help achieve HbA1c improvements but also identify unforeseen hypoglycemia risk and address glucose variability. CGM in clinical practice can be deployed both in the professional, clinical setting (retrospective review) and being used in the personal, at-home setting (real time).
CGM in Clinical Practice—Professional Use CGM
Professional CGM is a means for clinicians to do a glucose pattern “checkup” without requiring patients to purchase a system for personal use. Given patient insurance coverage limitations and patient preference, professional CGM is an option in addition to personal CGM. As the professional CGM systems become easier to use and less costly for the clinic, it may also be used in primary care. RT-CGM, flash CGM, or blinded CGM (no data displayed to the patient) can be worn for 3, 7, or 14 days and then downloaded in the clinic for interpretation. While most insurers require at least 72 h of monitoring for reimbursement of CGM, the current recommendation for accurate or reproducible pattern recognition is to analyze 14 days of CGM data. 31 The data then can be evaluated by the clinician, compared to the last CGM profile done and reviewed with the patient to help drive treatment changes and/or improve patient's self-management skills.
There are three systems currently available in the United States for professional CGM use (where the clinician or clinic owns the device): the Medtronic iPro2 system, 32 Dexcom Professional, 33 and the FreeStyle Libre Pro 28 (Table 1). The iPro2 system requires only a sensor with the attached data storage component, the Dexcom system includes a sensor, transmitter attached to the sensor, and a separate receiver. The FreeStyle Libre Pro system, 28 approved by the FDA in 2016, is the first flash CGM for professional use in the United States. The Freestyle Libre Pro sensor is factory calibrated and worn for up to 14 days, and does not require patients to do SMBG calibrations. The iPro2 and FreeStyle Libre Pro systems are blinded to the patient, while the Dexcom can be either blinded or unblinded to the patient.
At the end of the study period, the data can be downloaded, reviewed by the patient's diabetes healthcare provider, and shared with the patient. Some clinicians feel the blinded period is helpful to record the patients' usual habits, activities, and use of medications. Other clinicians feel the unblinded or real-time visualization of the glucose values and trends is a critical learning tool for patients to get immediate feedback on the effects of certain foods or of exercise.
The placement, education, and removal of the CGM are reimbursable by most insurance plans, as is the interpretation of the CGM data by the healthcare professional (MD, nurse practitioner, or physician assistant). Most health plans do not give specific requirements about the contents of the interpretation report and most of the time different clinicians and educators in a clinic do not have a consistent approach to SDM and the generation of an action plan. A basic interpretation report should review time in range, patterns of hypoglycemia, hyperglycemia, and prandial excursions (Table 2).
Suggest that a printed copy of the CGM report is given to the patient and file a PDF of the report in the Electronic Health Record, if possible.
CGM, continuous glucose monitoring.
Comparison to previous professional CGM reports then is facilitated by the electronic medical record. Food and activity logs kept by the patient can also be helpful when interpreting glucose excursions and time of insulin or other medication administration noted. It is ideal if the usual time for meals and medications is noted directly on a standardized glucose profile. The data from the professional CGM can expose glucose patterns and potential points for intervention that would not be seen with routine SMBG (e.g., overnight hyperglycemia). Clinicians should have methods in place to communicate recommendations to patients. Note that it may be ideal to review CGM results and recommendations with patients face-to-face in a clinic visit, but it is not mandatory for the patient to be seen in clinic to complete a professional CGM interpretation. Professional CGM is well suited to be used in SDM with patients. Indeed, SDM has been shown improve intervention effectiveness. 34 –36
With over 90% of all T2D care being provided within primary care clinics, professional CGM solutions must address the unique environment and resource limitations within primary care. 37 As more professional diabetes organizations review the current state of glucose monitoring, almost every one of them makes the recommendation and outlines the rationale for having some type of consistent or standard glucose data report. 38 –41
The ambulatory glucose profile (AGP) has been suggested as a non-industry, standard glucose report and is gaining international attention. 39,42 –47 The AGP report includes three sections: glucose statistics, the AGP graph, and a third section (daily glucose graphs in a calendar view or insulin graphs) that is variable based on the data available and the clinical/treatment needs of the individual patient (Fig. 1). The glucose statistics include measures of glucose exposure, variability, time in ranges, and data sufficiency. Newest versions of the AGP report are developed by the International Diabetes Center for the SMBG, CGM, CGM+Insulin Pump, CGM+Closed Loop Insulin delivery. Use of a standardized report allows clinicians and patients as well as the whole care team to work from the same visualization. This speeds communication between the clinicians and patients as they are seeing the same report each time the data are downloaded. The AGP report has been tested in many different clinical settings with patients of various ages, literacy, and numeracy. It was preferred by patients and providers for ease of interpretation as well as ease of identifying glucose patterns. 48
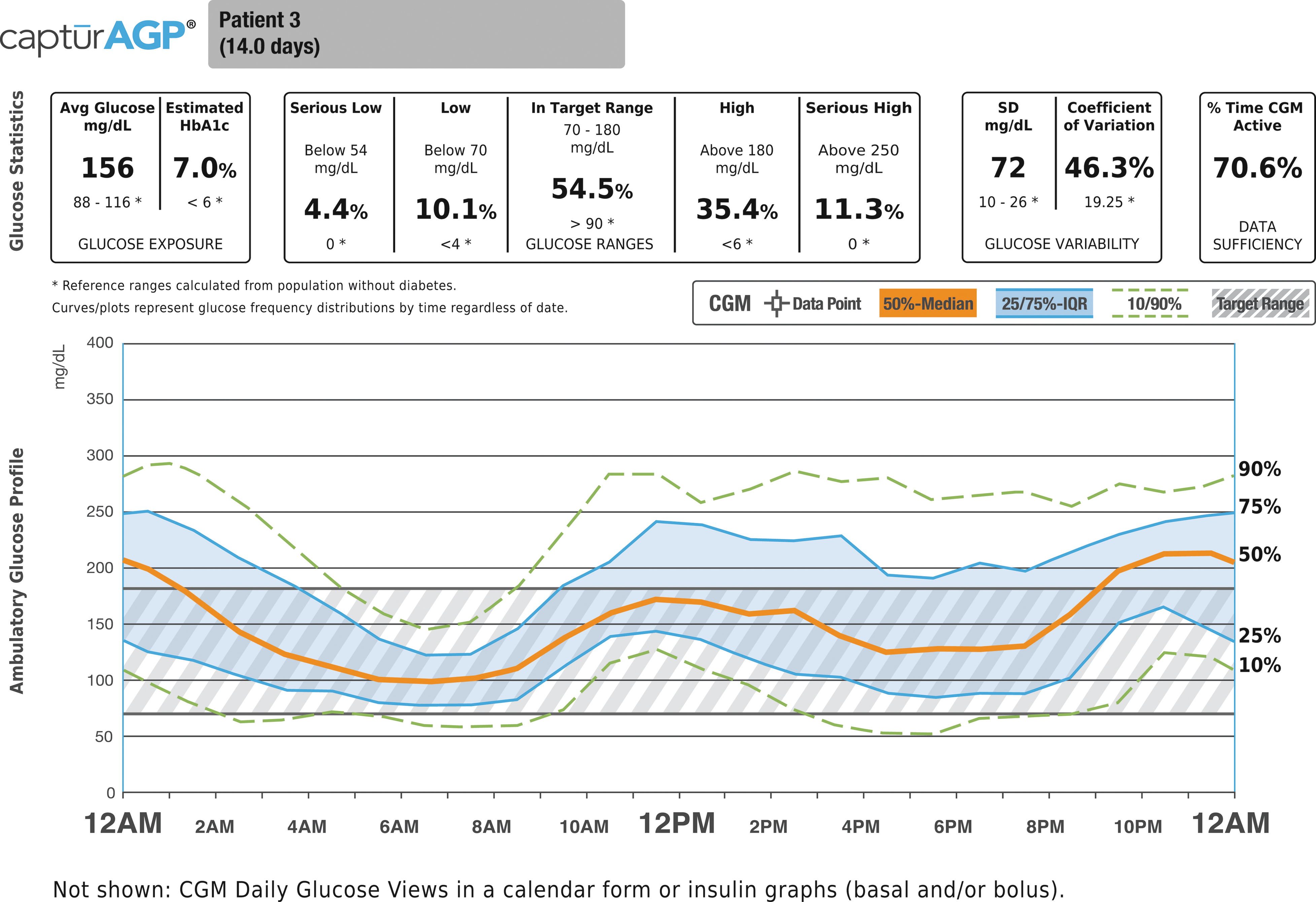
AGP CGM Report (Ambulatory Glucose Profile – Continuous Glucose Monitoring Report).
The mix of devices (SMBG, CGM, insulin pumps and pens) requires that staff are literate with many different software, processes, unique manufacturer's reports, and have the hardware to utilize all these systems, adding complexity. 28,32,33 Operationally, the downloading, cleaning, and tracking to ensure CGMs timely return required for professional CGM systems have made primary care less enthusiastic about adoption of CGM.
Indications for Personal Use of CGM
Similar to T1D, using CGM in T2D patients at high risk for hypoglycemia is understandable. Current guidelines from major endocrinology and diabetes groups have suggested use on a limited basis for CGM technology in T2D. The Endocrine Society recommends short-term, intermittent RT-CGM use in adult patients with T2D (not on prandial insulin) who have HbA1c levels ≥7% and are willing and able to use the device. 49
The results of the aforementioned DIAMOND study may lend evidence to support the use of RT-CGM in T2D patients on multiple daily injections of insulin. Furthermore, the study by Haak et al., 30 using flash CGM in T2D, is recently published and has not been incorporated into most society guidelines.
The American Association of Clinical Endocrinologists (AACE) published a consensus statement stating that CGM in T2D can be useful in patients with unappreciated hyperglycemia, hypoglycemia unawareness or those at risk for hypoglycemia, and those using intensive insulin therapy, regardless of type of diabetes. 50 AACE also calls for additional studies to evaluate the cost-effectiveness and proper clinical settings in which CGM may be most beneficial in T2D. In the 2017 Standards of Diabetes Care, the American Diabetes Association recommends CGM use for all patients with diabetes who have hypoglycemia unawareness and/or frequent hypoglycemia. 51
On December 2016, the FDA granted the Dexcom G5 system a non-adjunctive indication (“therapeutic CGM”). Therapeutic CGM is a replacement of SMBG, allowing therapy modification based solely on CGM readings and trends (the CGM device must still be calibrated using SMBG). Therapeutic CGM (dosing insulin from the sensor glucose value) was shown to as safe and efficacious as dosing insulin using SMBG values in a large multicenter RCT in T1D patients. 52 March 2017, Medicare announced therapeutic CGM coverage for patients with both T1D and T2D on intensive insulin therapy.
Another system for personal CGM use is the Eversense implantable CGM. This system is FDA approved and is a 90-day implantable CGM sensor with an external transmitter. 53
CGM Reports and Data Interpretation
The use of CGM data allows clinicians and patients to examine trends and offers more specificity for therapeutic interventions and behavioral interventions. In an age of pay for performance (P4P), most clinics have some financial risk/reward related to diabetes performance. Most diabetes P4P agreements are focused on measures of HbA1c, blood pressure, LDL cholesterol, tobacco cessation, and aspirin use for their entire patient population with diabetes. 54,55 These population health measures are meant to reflect good quality diabetes care of a population of patients, but what happens at the patient level of care delivery?
Experts have questioned over-reliance on A1c as a measure of quality care due to its tendency for regression to the mean as well as the rates' lack of hypoglycemia information. 38,56 Patient recall of hypoglycemic events is bias prone. In 15–20-min clinical encounters once every few months, it is important to quickly assess patient's glucose patterns and to act on patterns in addition to addressing any other concerns. A glance at a log book or glucose device memory, if it is brought, is prone to offering a highly selective and biased impression of glucose trends.
A better picture of the glucose trends and patterns is a picture: a glucose “EKG,” which is what the AGP report offers. Using standardized visualizations, the patient/clinician dyad can determine what medication, dosing, timing, dietary, or other interventions can be tried to impact the glucose pattern, increasing time in range (70–180 mg/dL) without increasing hypoglycemia. With both patients and clinicians wanting to avoid hypoglycemic events, AGP CGM reports can help monitor the risk for these events. 40,57 –60
The use of these individual glucose metrics, together with the patient in an SDM conversation, allows the patient and the clinician to both come to a harmonized point of not only what are the current care priorities but also why they are focused on specific issues and how the interventions are expected to change the patterns. 34 –36 The AGP then allows the clinician to focus on the individual patient while improving the population's care as a whole.
Future Directions
While more research is needed to establish the optimal frequency, timing, and duration of CGM, it seems very reasonable to consider CGM use in T2D at a minimum duration: insulin starts, increases in insulin dosage, and periods of acute diabetes problems such as increased utilization of inpatient and emergency services.
Another period where CGM is thought to be of benefit would be a therapeutic agent change. Patients at high risk for hypoglycemia and special populations such as those with chronic kidney disease may benefit from CGM analysis. When adding another medication to a patient's regimen, CGM would allow providers to see the impact or lack of impact an additional agent makes. Since many new medications are costly and often have side effects, quick feedback would allow for timely decisions about the addition or subtraction of ineffectual or not well-tolerated medications months before an HbA1c value. The benefit to both the patient and insurer would be clear; stop medications that are not effective and consider another option if necessary.
Research is yet to be completed to determine optimized T2D “checkup” schedules. It is conceivable that there would be significant benefit to SDM conversations to have at least 2 weeks of detailed glucose pattern data at specified intervals to confirm if interventions have had the expected impact, such as changes in the postprandial hours of the day, or overnight. CGM data would offer insight that even highly structured SMBG would be unable to provide due to the abundant data. Data such as fitness tracker and sleep trackers, dietary apps, insulin pens, and other patient-reported outcomes such as times of stress, anxiety, or depression will serve only to enhance the SDM conversations.
Insurers are more likely to pay for this expanded use of periodic CGM if they can be shown that the added expense for their members results in overall better health and decreased diabetes costs. Newer CGM systems are starting to incorporate external data into their reports (including the AGP).
Conclusion
CGM offers patients with T2D additional information about their glycemic control beyond the HbA1c. Data from personal use of RT or flash CGM in T2D hold great promise and we await additional data and the determination of more specific indications for use. Professional CGM use in endocrinology clinics, and eventually in primary care, is a tool to review glucose patterns and share decision-making with the patient at a clinic visit or remotely. It will be necessary to address standardization of glucose reports and interpretation, streamlining the implementation and use of CGM in clinical practice, and establish the cost–benefit ratios for both personal and professional CGM use in T2D.
Footnotes
Author Disclosure Statement
R.M.B. received research support, acted as a consultant, or served on the scientific advisory board for Abbott Diabetes Care, DexCom, Eli Lilly, Glooko, Hygieia, Johnson & Johnson, Medtronic, Novo Nordisk, Roche, and Sanofi. R.M.B.'s employer, non-profit Health Partners Institute, contracts for his services and no personal income goes to Dr. Bergenstal. He has inherited Merck stock. He is a volunteer for ADA and JDRF.