
Abstract
Background:
Artificial pancreas (AP) systems have initially been designed for and tested in teens and adults, but there is evidence that an AP system with additional support and safety systems could greatly benefit younger children with type 1 diabetes (T1D).
Subjects and Methods:
Five pediatric endocrinologists and 15 parents of children aged 5–8 years with T1D participated in a total of four focus groups. Focus groups investigated current diabetes technology use and acceptance, as well as possible modifications to the current adult AP system, which would allow for safe and successful use in younger children. Modifications discussed include child-specific functionality for input tasks, safety features, and monitoring capabilities.
Results:
Participant suggestions included the following: passcodes for differential access to AP features by parents, ancillary caregivers, and the child; preset early, intermediate, and advanced child access categories; maximal customization for general and alarm settings; simplified meal screens utilizing the AP’ corrective blood glucose (BG) ability; automated exercise mode; spoken and dictated messaging capabilities; emergency contacts; treatment instructions for the child and caregiver; remote monitoring website and application; animated continuous glucose monitor BG trace; gamification, such as rewarding diabetes-friendly behaviors; and comprehensive training of all individuals involved in the child's diabetes care.
Conclusion:
Parents and physicians were eager for AP applications to be available for younger children, but stressed that a modified system could better serve this group's needs for safety and improved diabetes-related communication. The diverse and emerging needs of 5–8-year olds require flexible and customizable systems for T1D management.
Introduction
Y

Current tools for diabetes care compared to AP-based diabetes care. Current care involves the option of using some tools (such as CGM and insulin pumps) that an AP system relies on. While current care relies on direct entry by parents, children, and other care givers, for the majority of the day and night, the AP system determines insulin delivery from preprogrammed data and CGM tracings, requiring only carbohydrate entry for food. In both cases, the child may not be at a mature enough state to enter data leading to insulin delivery. AP, artificial pancreas; CGM, continuous glucose monitor.
An important goal in the development of AP technology is to provide effective treatment that is adoptable by users of all ages. The Diabetes Assistant (DiAs) was the first ambulatory AP system, developed by the University of Virginia (UVa). The DiAs has been extensively tested in outpatient settings over more than 200,000 h of use in both adults and adolescents. 10,11 However, a user interface such as DiAs, while designed to facilitate BG management tasks in adults, 12 may be too advanced and even dangerous when used by younger children. Inadequate oversight, understanding, and training, and purposeful misuse significantly contribute to reported adverse events with pediatric use of insulin pumps. 13,14 Applying this information to the adoption of a pediatric AP system, it is possible that younger children will benefit most from a system that provides them with modified access to some features but reserves access to advanced features to caregivers. For instance, the younger-child AP system may be adapted to more team-centered rather than patient-centered care by including thorough training of all caregivers and promoting involvement for optimal diabetes management and patient outcomes. 15,16
Other challenges when considering pediatric use of closed-loop technology include the following: unpredictable eating and exercise, significant hypoglycemia, low insulin doses, high insulin sensitivity, and the usability of closed-loop components 15,17 ; the complexity of the closed-loop components is further tempered by this population's variant levels of comfort and maturity with technology use and the intimate involvement of various caregivers (i.e., parents and school staff) in many management tasks. This study employed focus groups of pediatric endocrinologists and parents of younger children with T1D to assess factors associated with diabetes technology adoption in children aged 5–8 and discuss adaptations to the DiAs user interface to promote successful and safe use in this age range. The 5–8-year age range was chosen to capture the prepubertal, early elementary population who are less likely to have developed skills to independently manage T1D and therefore rely on diverse, potentially inconsistent aid between home and school. Safety modifications and support systems facilitating continuous and involved care would greatly benefit this age range in particular, whereas older adolescents may take more responsibility for their disease management.
Methods
Study design and analysis
This study uses a phenomenological framework to explore how the experience of caring for younger children with T1D shapes needs and desires for AP modifications. Four, 2-h-long focus groups, that is, guided discussions, were conducted at UVa. One focus group consisted of pediatric endocrinologists, who were recruited for their knowledge of current diabetes technology as well as safety risks and benefits of diabetes technology use in younger children, while the latter three focus groups consisted of parents of children aged 5–8 with T1D. The focus group technique was chosen for the following reasons: (1) the interactive dynamic effect within a group is more than the sum of independent interviews, (2) participants could provide context and qualification to their statements, and (3) the fact that the moderator has the opportunity to ask relevant follow-up questions.
18
Throughout the focus groups, broad, predetermined questions (outlined in Supplementary Materials 3; Supplementary Data are available online at
Focus groups were audio recorded, transcribed, and coded in accordance with thematic analysis 19 and analyst triangulation. 20 This included the following steps: (1) two researchers (R.G. and S.L.R.) coded the entire transcript into inclusive categories and (2) a third researcher and subject matter expert (M.D.D.) reviewed the coded data and synthesized the themes within the predetermined categories of the following: current technology use, AP input tasks, AP safety features, and individuals involved in diabetes management. The goal of this analysis was to include all participant viewpoints, while organizing them into meaningful categories as characterized by multiple analyzers. While it was determined that there was a high degree of similarity between the primary raters' output, analyst triangulation improved diversity of perspective on the final coded categories and contributed to a richer synthesis.
Results
Participants
Each 2-h-long focus group was attended by three to six participants. The researchers attempted to achieve data saturation by initially recruiting five participants per focus group, a number chosen to promote diversity of experience, while allowing ample opportunity for each participant to talk; five recruited parents did not attend the focus groups due to last-minute conflicts, so spouses were allowed to participate to reach the recruitment goal. Five pediatric endocrinologists and 15 parents of 11 children aged 5–8 with T1D participated in separate focus groups. Pediatric endocrinologists were recruited from around the state and had a median of 21 years' (range 2–36 years) experience in treating pediatric diabetes in practices with extensive pump and CGM use. One of the pediatric endocrinologists had been the study physician for an AP trial; the others did not have experience with the AP.
Parents were recruited by flyers placed in the waiting area of UVa's Pediatric Diabetes Clinic or referred by physicians at additional pediatric endocrinology clinics and asked to contact the Center for Diabetes Technology (CDT) by phone or e-mail. Local clinics were chosen to increase the likelihood that families could participate in the focus groups in person. In addition, families with pump and/or CGM experience were recruited for their familiarity with these AP system components. The range in duration of diabetes was 2–7 years. No parent had experience in using a research closed-loop system, but one had an older child who had participated in an AP clinical study. Additional participant characteristics are available in Table 1.
Pediatric endocrinologists and parents of 5–8-year-old children with T1D participated in 2-h focus groups at the University of Virginia. Focus groups examined improvements to safety features and the user interface of the AP for use in young children.
AP, artificial pancreas; CGM, continuous glucose monitor; SD, standard deviation; T1D, type 1 diabetes.
Topics
Parents and physicians were given a description of the current AP system (Fig. 1). As this system relies largely on existing technologies, participants were initially asked to report their experiences with current CGM and insulin pump management. Using technology for the management of T1D in younger children depends on the patients, the parents, and ancillary caregivers; participants were asked to provide their input on necessary characteristics of persons involved in AP diabetes management. A summary of these discussions is provided in the Supplementary Materials 1 and 2, respectively. Participants were then asked about the settings and data input for the AP. Common themes across focus groups are discussed in the body, while a comprehensive list of suggested functionalities and supporting quotations are available in the corresponding Tables 2 –4.
BG, blood glucose; CDT, Center for Diabetes Technology.
AP Technology: Input Tasks
Settings
Insulin settings
AP insulin settings, prescribed by endocrinologists and sometimes adjusted by parents between appointments, are entered into the system like an insulin pump (Table 2). All participants agreed that insulin settings should be changed only by the physician or parents, but disagreed about whether they needed to be locked. Considering the user-friendly interface of the AP's phone platform, the majority (87%) of parents believed entering settings should require a passcode.
Security and general settings
Parents recommended maximizing the ability to customize settings (e.g., alerts/alarms, remote monitoring, and user interface). Research has shown that adding more options can decrease the likelihood of a person choosing anything; however, more knowledge and organization of the options into categories diminish this effect. 21 Participants supported default settings, which could be further customized by the parent based on the child's developmental level and autonomy in diabetes management.
Meals
Physicians expressed confidence in the AP’s closed-loop capabilities with regard to meals and suggested simplifying the meal screen using loose estimation of carbohydrates and subsequent AP compensation. Based on experiences with their own children, parents believed that 5–8-year olds should be involved in entering meal information. Most parents agreed it would be appropriate to lock insulin delivery capabilities for this age range, while other parents believed passcodes would make ancillary diabetes care more difficult. Many parents supported measures to aid parental involvement in school meals.
Exercise
Indicating exercise within the DiAs sets a temporary low BG target of 140 mg/dL (compared to the default 110 mg/dL) and may provisionally suspend basal insulin. 22,23 When used during exercise, this allows the system to prevent exercise-induced hypoglycemia; when used during rest, this feature may not allow for as tight a control as otherwise possible. Because this function is not a major safety hazard, physicians and parents were only concerned with whether a 5–8-year-old would remember to use the function. Participants suggested automatizing the exercise function or utilizing it all day to prevent dangerous lows when outside the house.
Messaging
Because the AP uses a mobile platform, text or wireless messaging could be enabled for child-caregiver communication. 24 Parents agreed that written and audio messaging should be enabled and would be especially helpful for substitute nurses; during field-trips; and at friends' and families' houses.
Parents' and physicians' further experience with and suggestions for current diabetes technology is shown in Supplementary Table 1. Thoughts regarding creating a successful care team for their child's diabetes is shown in Supplementary Table 2. (Supplementary tables [Supplementary Data] are available at
AP Technology: Safety Features
Passcodes
The focus groups discussed the viability of a password to block features that may not be safe for 5–8-year olds when unsupervised (i.e., Fig. 2 and Table 3). Participants unanimously agreed that current pump/iPhone passwords do not keep children out and increase the difficulty of diabetes management for adult caregivers. All but one parent, whose child had intentionally delivered insulin to induce need for hypoglycemia treatment, agreed that children with diabetes generally respect their pump as a medical device. However, participants perceived that the AP’s phone platform may be more enticing to children and could pose more risk than current diabetes technology. Participants wanted flexibility with setting passcodes so that families may decide together which features need to be initially blocked and which may be freely accessed as their child's autonomy increases. Customizable passcode formats to support different family and school preferences and the ability to set passcodes for certain times of day were also supported.
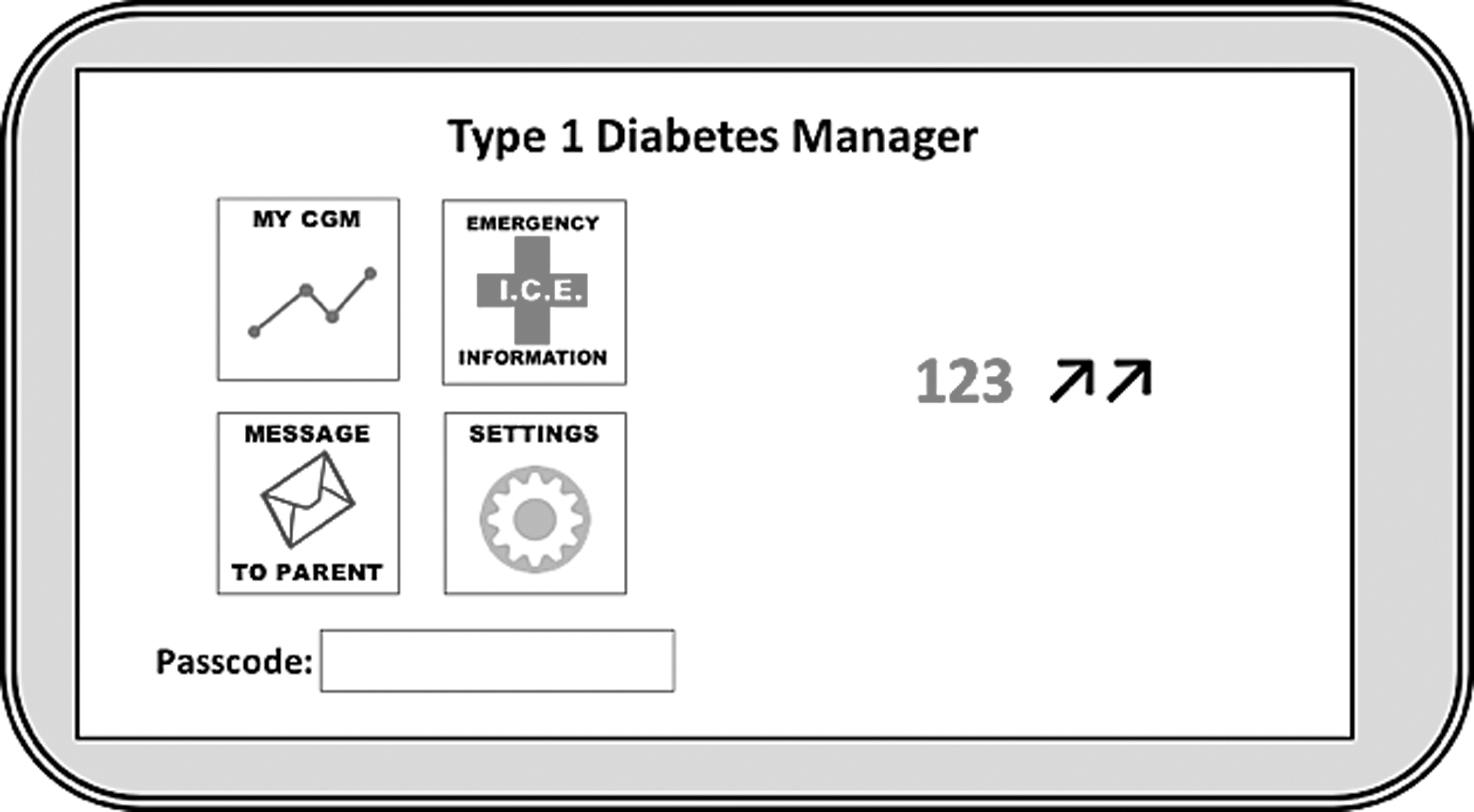
Prototype of AP-modified access screen, with buttons leading to further screens with specific utility. Parents posited that some screens (such as CGM tracings, emergency contact information, and message communication with parents) could have open-access, where other screens (such as insulin settings or carbohydrate information) require passcode access.
Emergency contacts/phone call
Focus groups considered emergency situations in which the child, adult caregiver, or diabetes-unfamiliar person would want to contact the parent. Participants supported listing emergency contacts either on a strip across the top of the home or lock screen, or within a button. Parents showed mixed support for enabling buttons that could directly contact caregivers, the physician, and 911, but most participants would like the AP to automatically call an emergency contact if the data indicated a dangerous low or prolonged high blood sugar.
Alerts and alarms
Alert and alarm preferences varied across families, and participants believed the ability to customize based on their needs would increase their likelihood of adopting the technology. Parents agreed on the following default alarm settings: noticeable low alarms that persist until acknowledged and treated; an alert for a caregiver to check the pump site when high BG persists (longer than 2 h) despite AP action; a loud alarm and accompanying caregiver alert for a sharp BG spike without an insulin bolus, indicating carbohydrate consumption without accompanying insulin; loud nighttime alarms accompanied by automated phone calls; a parent/supervisor passcode to silence alarms and ensure timely treatment; and alarms that increase in intensity, culminating in a voice readout of treatment instructions, when alarms are ignored and/or proper treatment is not initiated.
Instructions for child and caregivers
Participants unanimously supported simple, written, and pictorial instructions accompanying alarms to help children and other care providers with treatment decisions and alleviate alarm-induced anxiety among school staff. For hypoglycemia, a banner with, “Blood sugar is low. Treat with fast-acting carbs.” and pictures of appropriate treatment could help those unfamiliar with diabetes care. More in-depth information about diabetes, treatment, and AP technology should also be available.
Monitoring
CGM trace and history
Some parents believed that a CGM BG tracing should be accessible on the home screen of the AP, whereas others were not sure how their child would benefit from this information (Table 4). Current CGM users and physicians believed that a CGM trace is an important visual that helps younger children understand their BG. Investigators presented prototypes of an animated CGM screen; an airplane and its contrail mark the BG trace, while a blue sky indicates a safe BG range, clouds a high BG range, and trees a low BG range (Fig. 3). Parents thought that animation could be a great teaching tool and motivator. However, they also worried that children may get upset when having out-of-range BG, such as during an illness or other uncontrollable circumstances, or the animation could negatively motivate children to push their BG high or low and explore what happens to the screen. Animation should be an available, but not mandatory feature.
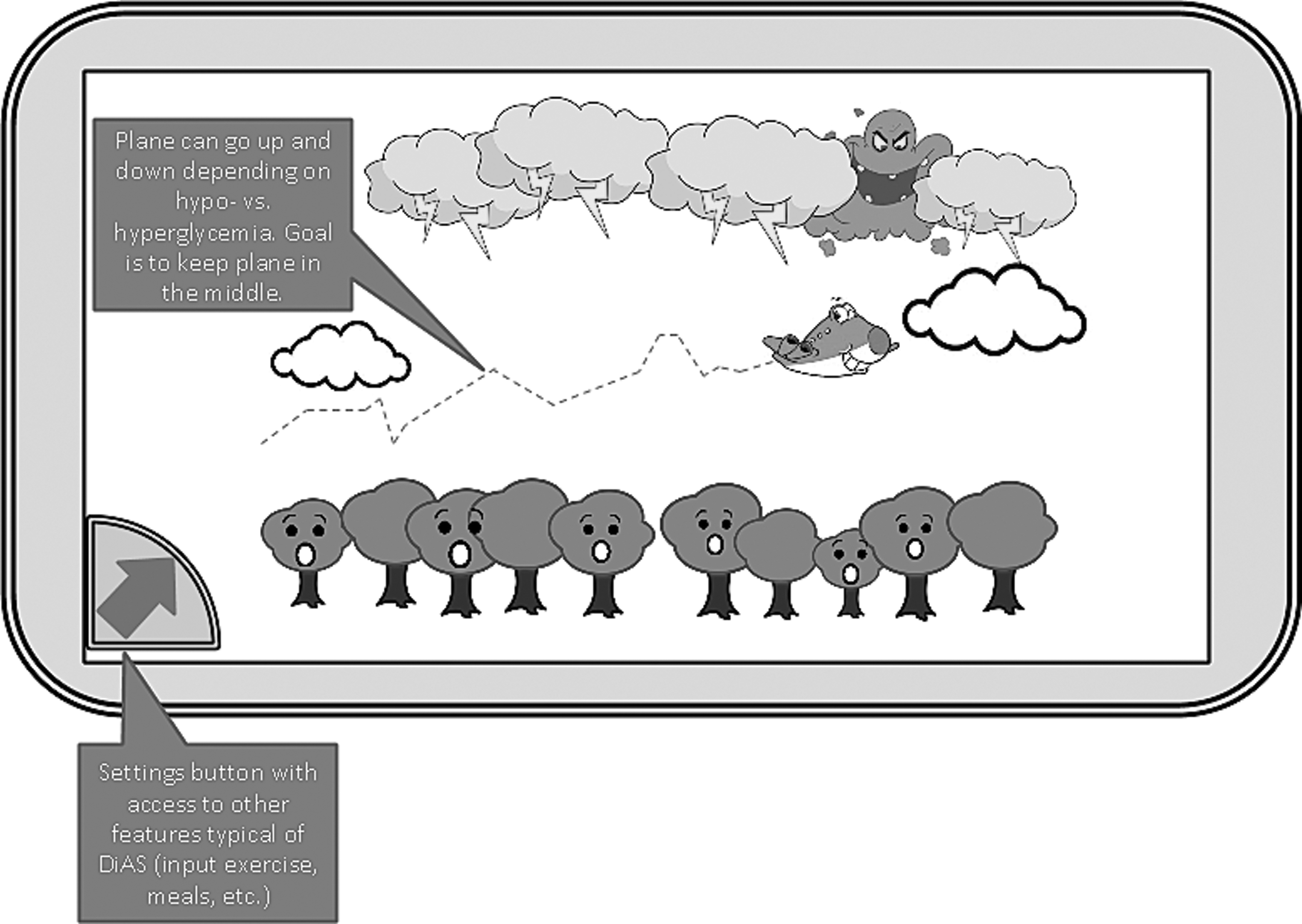
Prototype of animated CGM trace. A modifiable screen such as this could provide a visual cue for children to understand their current blood glucose level that is best when not too low (in the trees) and not too high (in the stormy clouds).
Gamification
Investigators introduced the possibility of AP gamification based on evidence of diverse mHealth apps for improving health outcomes, including an increased frequency of BG monitoring in adolescents with T1D. 25,26 Participants agreed that children would be motivated by earning points for good diabetes management such as responsible bolusing, entering finger sticks, calibrating the CGM, making healthy food choices, promptly acknowledging alarms, and treating lows quickly. Parents did not want rewards to be based on average BG or time in range since these are not in the child's direct control. Points could be rewarded by an online system or by the parents, and this feature could be turned off if desired.
Remote monitoring
Current CGM users reported relying on remote monitoring daily. Participants in each focus group expressed interest in both remote monitoring through the AP and proposed the ability to remotely bolus insulin. Parents wanted a corresponding website and phone application that could be accessed by care providers.
Discussion
Across focus groups, suggestions for AP modifications followed two major themes: (1) creating a modified and flexible AP system to help a child assume more responsibility for their diabetes management and (2) creating a system that can facilitate the involvement of and communication between various care providers. Prior research and results from these focus groups emphasize that both self-efficacy and a team-centered approach are positive for diabetes management in younger children. 27 The ability of the AP to integrate diverse diabetes tools (e.g., pump and CGM, meal and exercise assistant, text messaging, phone calls, diabetes care websites and social media, diabetes care information, and AP training) into one device simplifies and expedites their multipurpose use to involve parents while bolstering child problem-solving and self-management skills. 24
Involving the children in their care at this age is critical because it can set the stage for effective diabetes management for their entire lives. Self-management skills deemed appropriate for this age group based on the focus groups included the following: inputting exercise, monitoring their CGM trace, and knowing where/when to get help. Focus groups supported modifications to incentivize children to participate in positive diabetes management activities (e.g., animation of the CGM trace and a points system). Focus groups strongly endorsed flexible AP settings that allow responsibilities to be tailored to the individual child. It is important to note that (1) children go through many changes between the ages of 5–8, which necessitate adjustments in AP settings, and (2) improvements in quality of life (QoL) are dependent on having appropriate expectations for the technology based on the maturity of the patient. 28
Care teams must understand the capabilities of and sustained involvement necessary for successful AP use in younger children. As previous studies have shown, maintaining parent involvement at this age is critical to adherence to BG monitoring and glycemic control, and sustaining a higher QoL. 27,28 The AP also has the potential to alleviate parental/child stress related to diabetes when the adopters are willing to participate in a care team and the technology is adopted with realistic expectations. Features of the AP that could reduce parental/child stress and were well received during the focus groups include the following: passcodes to block insulin delivery (as the CDT recently tested in younger children 9 ); customizable alerts to the child/caregivers to ensure appropriate treatment and discourage covert snacking; and easily accessible resources and incentives through animation and gamification.
Focus groups also stressed the importance of improving ancillary caregiver involvement in young children's T1D management. Participants cited poor training as a barrier, while good training was considered imperative to successful technology adoption. With the complex AP system, training is even more critical for all parties involved in diabetes management. Parents from the focus groups were overwhelmingly unsatisfied with their children's current diabetes management at school, consistent with previous published literature, 29 concluding that school nurses and primary teachers need enhanced training on T1D and how to reliably manage BG events. Psychoeducational factors could be included in training to help children, parents, and ancillary caregivers deal with the pressures of T1D management. 30 In addition, focus groups supported features to help ancillary caregivers including the following: text messaging, instructions paired with alarms, straightforward input screens (e.g., carbohydrate entry, exercise indicator, and treatment screen), and diverse remote monitoring capabilities.
Finally, the adoption of AP technology also needs to take into account barriers, stigmas, and preconceived notions associated with the hardware (i.e., insulin pump and CGM). A study assessing patients' future acceptance of closed-loop technology found that pump users who read a description of an AP system were highly trusting the system's accuracy and usefulness, 31 whereas a study with CGM users were more concerned with the system's accuracy. 32 These results were mirrored in our focus groups in that, the parent's attitude toward the AP system was dependent on current CGM use/expertise. Parents with CGM experience understood the benefits/limitations and the need for continued treatment involvement (i.e., fingersticks, calibrations, and interpreting BG trends/history). Parents with intermittent CGM experience conveyed greater dissatisfaction with sensor inaccuracy, consistent with data that nonregular CGM users have less valuable experiences with the technology. 33 Finally, parents with no CGM experience were the least aware of the potential value and limitations of CGM technology. Again, future AP users must be fully aware of the technology's capabilities, requirements, and limitations.
This study sought to move away from what engineers or adults find easy to use and toward what children aged 5–8, parents, and potentially diabetes-unfamiliar care providers can utilize as a team. A direction for future research would be to explore other perspectives (e.g., school staff, family members, certified diabetes educators, the children themselves, and a larger child age range) on proposed modifications to the AP system for children. One limitation of this study is the limited sample size; while the targeted population further limited generalizability, the researchers thought it was critical to recruit participants with children using AP components (i.e., insulin pump and CGM technology). A more diverse sample in the future could include children who do not use these components (i.e., use multiple daily injections and no CGM) to represent the larger diabetes population. The authors sought to quantify the focus group data by tracking percent support per functionality discussed, but this has limited accuracy as the open-ended format allowed focus groups to generate different ideas. While equal contribution was encouraged, there is always the potential for domination by one or several speakers as well as groupthink with the focus group format. Surveys could be used along with focus groups to increase generalizability. Focus groups and surveys specific to user interface and AP features could be administered to children and family members after experience with closed-loop systems in a clinical trial, as is being done with teen and adult populations. 34,35
Footnotes
Acknowledgment
Funding source: UVa internal Launchpad Grant Program.
Authors' Contributions
S.L.R., PhD in industrial engineering (with a focus on cognitive human factors) and professor at Clemson University, conducted the focus groups. This researcher has had 8+ years of experience conducting experimental studies and running focus groups, but had little bias or knowledge specific to the AP before this project. M.D. DeBoer, pediatric endocrinologist and researcher at the UVa CDT, and Daniel Cherñavvsky, researcher at the CDT and Chief Medical Officer at TypeZero Technologies, Inc., helped introduce the AP system and ask/answer questions requiring detailed knowledge of the AP. R.G., psychology BA and research technician at the CDT, was present at the focus groups and managed participant recruitment and consent, transcription, coding, and writing. M.D. DeBoer and S.L.R. participated in coding and critical revising as well. No relationship was established between the researchers and the participants before the focus groups, at which time the researchers gave short, professional introductions.
Author Disclosure Statement
D.R.C. is CMO of TypeZero Technologies, Inc., a company currently testing an inControl AP system purchased from the UVa Center for Diabetes Technology with the aim of marketing the product once approved. M.D. Breton is a founder and equity holder of TypeZero Technologies, Inc. He has received research support from Dexcom, Tandem, Roche, Senseonics, Sanofi, and Ascensia. M.D.B. has received consulting fees and honorarium from Sanofi, Ascensia, Dexcom, and Roche. All other authors have no competing financial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.