
Abstract
Objectives:
The study assessed the psychosocial impact of the bihormonal bionic pancreas (BP) on adults in a real-world outpatient setting.
Research Design and Methods:
Thirty-nine adults with type 1 diabetes at four study centers across the U.S. participated in a two-arm, random-order, crossover design study: 11 days with the BP and 11 days with their usual care (UC). Psychosocial questionnaires were administered before the first study arm, at the end of the first study arm, and at the end of the second study arm.
Results:
The mean age of participants was 33 years; mean diabetes duration was 17 years; and 84% were non-Hispanic Caucasian. Significantly greater improvements in psychosocial outcomes were found following the use of BP versus UC; these included reductions in diabetes-related distress (P < 0.001) with the greatest drops in distress related to hypoglycemia and to eating constraints, and greater treatment satisfaction (P < 0.05). The majority of BP users described their experience as positive with a reduction in worrying about low (72%) and high (69%) blood sugars. The majority reported trusting the device (69%) and feeling less burdened by the BP than their usual method of diabetes care (64%). Concerns about the burden of the BP were also expressed, with >75% of users highlighting the burden of carrying around the equipment and the need to change glucagon daily, and more than half of the participants reporting concerns about wearability, discomfort, the time it took to correct out-of-range numbers, and “glitches” in the system.
Conclusions:
Overall, participants report substantial psychosocial benefits accruing from the BP relative to their usual method of diabetes care. However, participants also reported a number of burdens associated with the system. Future versions of the BP device should be designed with the goal of addressing these concerns, and studies with larger, more diverse samples, and with more technology-naive participants are needed.
Introduction
T
New technologies are being developed to make glycemic control easier, safer, and less burdensome for patients. A class of technologies, referred to as artificial pancreas, closed-loop, automated insulin delivery, or bionic pancreas (BP) systems, can automatically monitor blood glucose levels and suspend insulin delivery to reduce the risk of hypoglycemia without patient action. Most of these systems can also increase insulin delivery to prevent and treat hyperglycemia. Typically, such systems consist of three parts: a continuous glucose monitor (CGM), a control algorithm that makes automated dosing decisions about when and how much insulin to administer, and a drug infusion system for delivery of the insulin. Studies offer promising results, showing superiority of automated systems over standard pump therapy with increased time spent within glucose targets and/or reduced hypoglycemia. 4 –10
Unfortunately, single-hormone systems cannot “take back” insulin once it has been administered, so the risk of hypoglycemia remains, especially in postexercise and late postprandial settings. 11 One automated system, the bihormonal BP, in addition to automatically delivering insulin, can also administer glucagon, which is used to automatically raise blood glucose. 12 –17 Therefore, it may be able to more effectively prevent hypoglycemia and decrease patient burden. For example, delivery of glucagon can prevent nocturnal hypoglycemia without the need for a patient to wake at night and can prevent hypoglycemia associated with exercise without carbohydrate treatment. Other features of the BP may make diabetes management easier for patients. For instance, meal announcements are optional and when meals are announced there is no need to count carbohydrates. All of these features may contribute to improved patient quality of life and clinical outcomes. The BP has been shown to improve glycemic management relatively to usual care (UC) in outpatient settings in preadolescent children, adolescents, and adults. 12 –16
While the technological accomplishments of the BP system are impressive, the impact of the BP on patient burden (e.g., alarms, rashes, hassles, and discomfort) and emotional well-being (e.g., worry, burden, and quality of life) have not been assessed. The success of any technology is contingent upon the patient's perception that the technology is safe, reliable, and effective. It must be able to adapt to real-life experiences and events without increasing the burden of caring for the disease. Data regarding both the Continuous Subcutaneous Insulin Infusion (CSII) and CGM technologies suggest that a patient's body image, comfort in being public about having diabetes, burden with the daily demands of the regimen, willingness to rotate sites, expectations regarding glycemic variability, and comfort with large amounts of data are all factors that affect a patient's willingness to engage with these technologies. 18 –24 While researchers have studied the human factors inherent in CSII and CGM individually, very little is known about these issues in systems that combine these two elements with algorithms that automate glycemic management.
The purpose of the present study is to assess the psychosocial experience associated with using the BP in adults with T1D. Specifically, we focused on assessing emotional wellbeing, ease of use, confidence, trust in the accuracy of the system, and barriers impacting optimal engagement compared with UC. Assessing the psychosocial impact of the BP's daily use can help identify potentially modifiable barriers to adopting and using the technology effectively. It will also enable the medical team to better prepare patients and their family members about what to expect and how to respond to the new experiences that this technology provides.
Methods
Participants
Thirty-nine adults ≥18 years of age with T1D participated in this study. 17 All had T1D for ≥1 year, were on insulin pump therapy for ≥6 months, and worked or studied during the day within one mile of one of the four study centers (Massachusetts General Hospital, University of Massachusetts Medical School, University of North Carolina Chapel Hill, and Stanford University). Participants were required to live within a 30-min drive of the study center and had to be willing to remain within a 60-min drive of the study center for the duration of the study. Each participant was required to have a designated contact ≥18 years of age that lived with them and was willing to receive calls from the study staff to check on their welfare if necessary. Exclusion criteria included inability to safely adhere to the study procedures, hepatic failure or renal failure on dialysis, known coronary disease or an abnormal electrocardiogram suggesting coronary disease, congestive heart failure, history of transient ischemic attack or stroke in the last year, and hypoglycemic seizure in the last year.
BP system
Insulin and glucagon were automatically administered by a fully integrated bihormonal BP, as previously described. 17 Briefly, a G4 Platinum CGM (Dexcom) was connected through a custom hardware interface to an iPhone 4S (Apple), which ran the control algorithm. Two t:slim infusion pumps (Tandem Diabetes Care) were controlled through Bluetooth to deliver subcutaneous doses of insulin and/or glucagon up to every 5 min through commercially available insulin infusion sets. The only information used by the system to start operation was the body mass, with no information provided to the algorithm about the participant's usual insulin regimen. The BP automatically adapted insulin dosing to each participant's needs. Routine CGM calibrations were performed twice per day. The user interface showed the CGM glucose data and insulin and glucagon doses, and allowed for optional meal input by the patient. Subjects chose the meal type (breakfast, lunch, or dinner) and the meal size (typical, more than usual, less than typical, or a small bite) without counting carbohydrates. If subjects used this feature, they were instructed to use it immediately before eating. The BP then gave a partial meal-priming bolus that was automatically adapted toward 75% of the insulin need over the 4 hours following announced meals of that type and size.
Study design overview
The present study was part of a larger randomized crossover trial. 17 Participants were treated for 11 days with the BP and 11 days with their UC practices in random order. The co-primary outcomes of the trial were average CGM glucose level and the percentage of time a patient's CGM glucose was below 60 mg/dL. Participants had no restrictions on their activities or food intake during both study periods. Participants carried the CGM and iPhone portion of the BP during the UC arm, but the user interface on the iPhone and the Dexcom G4 display were blinded. Each participant used their own insulin pump and their own CGM (if they had one) during the UC arm. Questionnaires were administered three times: on the first day of each study arm and within 1 h of the end of the study.
Measures
Quality of life
The 5-item World Health Organization Well-Being Index (WHO-5) 25,26 is a brief, generic global rating scale measuring subjective wellbeing. All items are positively phrased, and respondents rate how well each of the five statements applies to him or her when considering the last 14 days. Each of the 5 items is scored from 0 (none of the time) to 5 (all of the time).
Diabetes-specific emotional distress
The Type 1 Diabetes Distress Scale (T1-DDS) is a validated scale developed specifically for adults living with T1D. 27,28 The scale yields a total distress score (alpha = 0.91) and subscale scores that assess seven specific areas of distress. The current study excluded physician distress (given the potential bias due to study design), and included the remaining six subscales (24 items), including: powerlessness, negative social perceptions, friend/family distress, hypoglycemia distress, management distress, and eating distress (subscale alpha range = 0.76–0.87). Items are rated on a 6-point scale from “not a problem” to “a very serious problem.”
Treatment satisfaction
The Diabetes Treatment Satisfaction Questionnaire-satisfaction (DTSQs) 29,30 is a validated, 6-item scale developed to assess a patient's level of satisfaction with their current treatment regimen, and was administered at baseline. The scale is rated on a 7-point scale, ranging from “0” to “6” with higher scores indicating higher satisfaction. In addition, two items assess the frequency of unacceptably high or low blood sugar levels, respectively. The Diabetes Treatment Satisfaction Questionnaire-change (DTSQc) assesses response to a change in treatment. 29,30 Therefore, it was administered at the end of each study arm. The item content is identical to the DTSQs, but responses are rated on a 7-point scale ranging from 3 to −3. For treatment satisfaction, higher positive scores are indicative of improved treatment satisfaction; negative scores indicate a worsening of treatment satisfaction. For frequency of low and high blood sugar levels, greater negative scores indicate a decrease in unacceptably low or high blood sugar levels, whereas positive scores indicate an increase. A “0” is indicative of no change.
Experience with the BP
The authors created a 38-item descriptive measure that assessed different aspects of a patient's experience with the BP. Items were developed from interviews with both adults and adolescents who participated in trials with earlier versions of the BP device. Items asked about both positive and negative experiences related to the use of this technology, for example, blood glucose management, device burden, and overall satisfaction. Items were rated on a 5-point scale (1 = strongly disagree to 5 = strongly agree). This questionnaire was administered only once, immediately after the patient completed the BP arm of the trial. Because of the descriptive nature of this instrument and the large number of original items, we report data only from items on which at least 50% of patients reported positive or negative experiences.
Data analysis
Independent t-tests and chi-square analyses were used to examine potential differences between groups based on which arm was experienced first (BP/UC vs. UC/BP). Repeated Measures ANCOVA models were employed to examine differences in the psychosocial measures between BP and UC, collapsed across order of presentation. Participant age and gender were included as covariates, given their established associations with key variables in the current study. To better understand baseline predictors of change we conducted exploratory analyses of associations between participant age, gender, baseline HbA1c, and CGM use with the psychosocial outcomes, as well as the interaction between these key participant characteristics and the intervention period.
Results
Participants were on average 33.3 years of age and had lived with diabetes for an average of 16.8 years (Table 1). Approximately half (53.8%) of the sample was female. Eighty-four percent of participants were Non-Hispanic White, 7.7% identified as Hispanic, and the remaining participants identified as Asian, African American, or multiracial. There were no group differences at baseline, except that those randomized to the BP arm first reported significantly higher scores on the DDS at baseline than those randomized to the UC arm first.
BMI, body mass index; BP, bionic pancreas; UC, usual care.
Changes in psychosocial measures
Significantly greater improvements compared with baseline were found across all psychosocial measures after the BP arm compared with the UC arm (Table 2). Participants reported a significantly greater reduction in total diabetes-related distress during their time in the BP arm relative to their time in the UC arm, with a mean (SE) between-group difference of −0.33 ± 0.10 (P = 0.001). There was also a significantly greater decrease in diabetes-related distress following use of the BP for five of the six T1-DDS subscale scores, including distress related to hypoglycemia (−0.55 ± 0.15, P = 0.007), eating (−0.43 ± 0.12, P = 0.004), diabetes management (−0.39 ± 0.12, P = 0.003), powerlessness (−0.22 ± 0.15, P = 0.01), and concerns related to family and friends (−0.22 ± 0.10, P = 0.05). Although participants randomly assigned to the BP arm first reported overall higher distress at baseline than those assigned to the UC arm first (P = 0.03), the interaction between distress and ordering of study arm did not reach significance (F = 3.28; ns), indicating that change in total distress was not different for those receiving BP first versus UC first.
Raw DTSQc scales represent change with negative scores indicative of greater improvement, thus mean scores are presented to identify level of change from baseline to UC/the BP period; however, a statistical test was only performed on the difference between these two scores.
P < 0.05.
P < 0.01.
P < 0.001.
DTSQc, Diabetes Treatment Satisfaction Questionnaire-change.
Significant between-group differences were also found for general quality of life relative to baseline (Fig. 1, WHO-5), with greater improvement following use of the BP compared with UC (0.27 ± 0.12, P = 0.03). Furthermore, improvements in treatment satisfaction (Fig. 2) versus baseline were larger in the BP arm compared with UC arm (0.35 ± 0.13, P = 0.01), with greater decreases in both the reported frequency of unacceptably low blood sugars (−1.74 ± 0.35, P < 0.001) and unacceptably high blood sugars (−1.70 ± 0.35, P < 0.001) in the BP arm versus the UC arm.
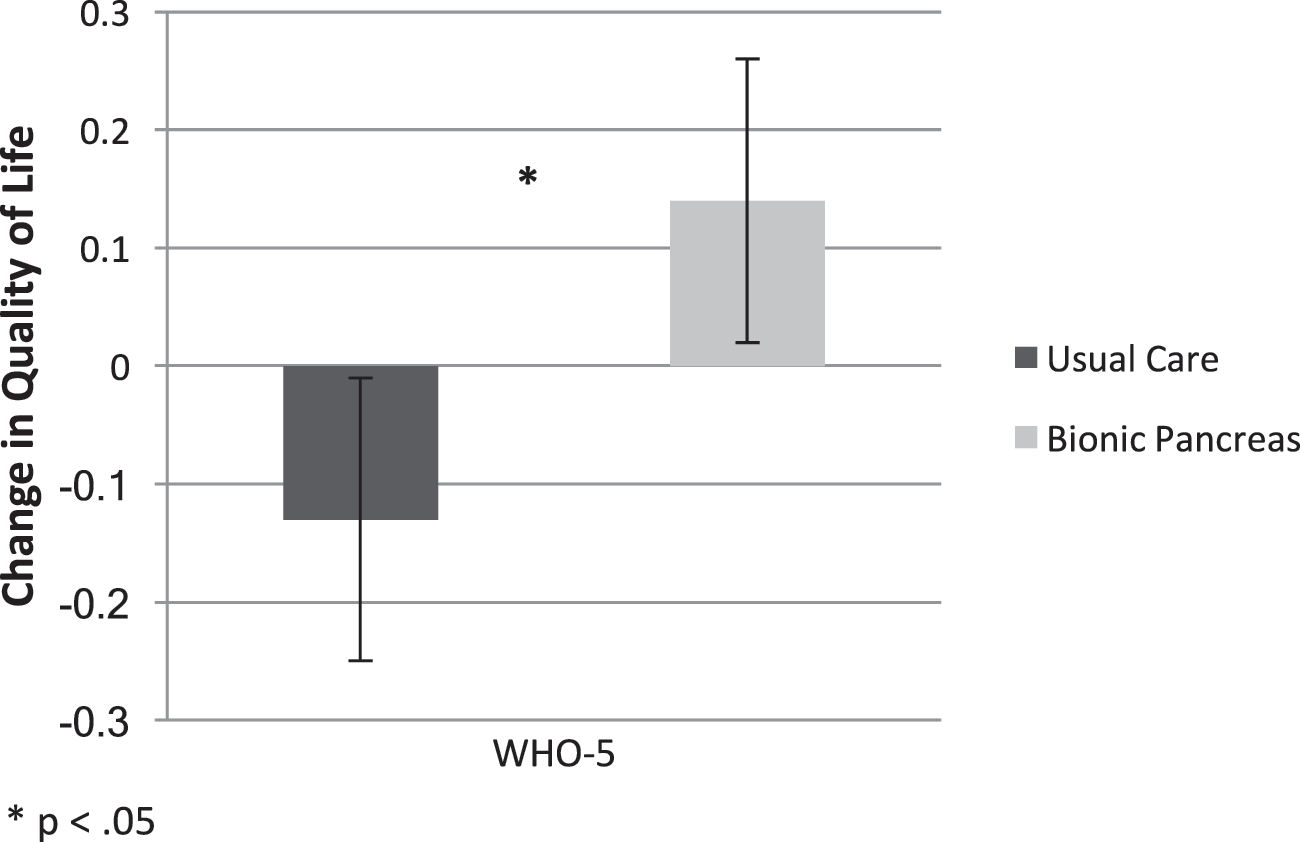
Quality of life (WHO-5).

Diabetes treatment satisfaction.
In exploratory analyses we examined the interaction between patient demographic factors (age, gender, baseline HbA1c) on the differences in psychosocial outcomes between treatment arms. No interactions among these variables reached significance. Furthermore, main and interaction effects of intervention group by CGM use (sensor-augmented pump) during the UC period were not significant.
Experience with the BP
The majority of participants described the BP experience as positive: 72% reported that it helped them to worry less about low blood sugars, 77% noted that it helped them to worry less about low blood sugars while sleeping, and 69% felt that it helped them to worry less about high blood sugars. Furthermore, 69% trusted the device to manage their blood glucose and 64% reported they felt less burdened by the BP than their usual method of diabetes care. Approximately half (54%) of participants reported it would be difficult to give up the device when the study ended.
Significant concerns regarding the BP were also expressed. About three-quarters of participants felt that carrying around all of the equipment was burdensome (77%) and that it was a big bother to have to change the glucagon each day (80%). More than half of participants reported that it was uncomfortable to wear all of the necessary equipment (67%), the BP was more intrusive than their typical method of diabetes care (56%), they were bothered by how long the device took to respond to high blood sugars (54%), or that the BP had too many glitches or bugs (54%). Importantly, in an overall rating, 31% of respondents expressed that “the bionic pancreas was more trouble than it was worth.”
Discussion
This study compared the social and emotional response of adults with T1D to using the BP, compared with UC in the context of a multisite, randomized, crossover study in a real-world outpatient setting. Participants report improvements in many psychosocial variables associated with using this technology relative to self-management of diabetes using their own insulin pump, either alone or with a CGM in the context of sensor-augmented pump therapy. Specifically, participants reported significantly greater reductions in diabetes-specific distress during the BP arm of the trial, with notable reductions in distress related to hypoglycemia and eating, relative to UC. While those randomized to the BP arm first had higher baseline distress, it is notable that greater reductions in distress during the BP arm persisted after controlling for ordering. During the BP arm, participants also reported greater improvements in treatment satisfaction and fewer concerns about out-of-range blood glucose numbers than during the UC arm. The majority of participants also reported positive experiences using the BP, specifically citing significantly fewer worries about low blood sugars. Concerns about the burden associated with the BP were also raised. Specifically, concerns were expressed related to the amount of equipment required and discomfort associated with carrying around the necessary equipment. Concerns were also raised regarding the need to change glucagon daily, feeling as if the BP was more intrusive than their typical method of insulin delivery, feeling as if the system did not respond to out-of-range glucose levels quickly enough, and dealing with system glitches.
Our moderator analysis demonstrated that no measured baseline patient characteristic differentially affected the findings. Thus, the psychosocial effects of the BP were relatively uniform across patients, increasing the potential generalizability of these findings to the T1D community at large. Even with the lack of variability in patient response, some patients felt that BP was worth the effort and others did not. As found in other research, not everyone has a positive response to the use of advanced technologies. Once the safety and efficacy of the BP has been demonstrated in larger trials, it will be important to document which kinds of patients can make the best use of the system, and what can be done to streamline BP use to make it accessible to a wider range of patient preferences and styles.
A limitation of the current study was the small study sample size, with limited statistical power for moderator analyses. Second, there was a significant ordering effect for diabetes distress that could have impacted the results. A further limitation was the lack of technology-naive participants; all participants in the current study utilized insulin pumps and many also utilized CGM. However, CGM use in the context of sensor-augmented pump therapy during the UC period was not predictive of improvements in psychosocial outcomes during either the UC or BP periods, and controlling for CGM use during the UC period did not alter the findings. Further studies with larger and more diverse samples will be needed to see how these and other factors affect the psychosocial outcomes with the BP system. Finally, the BP used in this study was an engineering prototype. The next generation will be fully integrated into a single device, which should be easier to use. Therefore, some of the concerns expressed by the current participants may be less of an issue for the newer versions of the BP.
New technologies in healthcare promise to improve clinical outcomes, but more information is needed about how such technologies affect patient quality of life, management burden, worries, and concerns. Even the most sophisticated technologies are of limited clinical value if patients will not use them or find them excessively burdensome. The results of this study demonstrate the complexities of introducing a major new technology to a clinical sample. Other evaluative studies of the BP show improved glycemic control, increased time in target range, and reduced risk of hypoglycemia. 12 –16 These results suggest that BP may provide significant improvements in the personal experience of managing diabetes, along with better clinical outcomes.
Footnotes
Acknowledgments
The authors gratefully acknowledge the participation and dedication of the families who participated in the study. They also thank the study coordinators and staff at each of the four clinical sites for their important contributions. In particular, they thank Courtney Balliro, BS, RN, CDE, Mallory Hilliard, BS, RN, Mary Larkin, RN, MS, CDE, and Debbie Mondesir, BS for entering and organizing the data from all of the clinical sites.
Authors' Contributions
J.W.B. helped design the study, completed the literature review and wrote, reviewed, and edited the article. D.H. analyzed the data, wrote the ![]() section, reviewed the article and provided crucial edits of the article. L.F. helped design the study, reviewed the article, and provided crucial edits of the article. S.R. oversaw data collection for this part of the multisite study as well as the larger study, and reviewed and edited the article. W.H.P. helped design the study, reviewed the article, and provided crucial edits of the article.
section, reviewed the article and provided crucial edits of the article. L.F. helped design the study, reviewed the article, and provided crucial edits of the article. S.R. oversaw data collection for this part of the multisite study as well as the larger study, and reviewed and edited the article. W.H.P. helped design the study, reviewed the article, and provided crucial edits of the article.
Guarantor Statement
J.W.-B. is the guarantor of this work, and as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
No competing financial interests exist.