
Abstract
Background:
Subcutaneous insulin infusion (CSII) therapy is a challenge for both patients and healthcare providers. The long-term CSII use is scarce. The aim of this study is to describe the impact of CSII therapy for 10 years of use at our center.
Methods:
This single-center retrospective study includes 162 type 1 diabetes patients using CSII for >3 years during October 2004 until October 2014. Data were collected through the electronic medical record system, cross-sectional analysis (telephone, e-mail, or social media), and CSII reports generated by Carelink Therapy Management Software (Medtronic, Northridge, CA).
Results:
Patients were analyzed in three age groups: 12–18, 19–24, and >25 years. All patients were treated with CSII for >3 years. Total daily dose of insulin was >0.9 U/(kg·day) in age group 12–18 years old, which was significantly higher than other two age groups (P < 0.05). Basal ratio was lower in younger age (<40%) and showed trend of increasing with age and longer diabetes duration (up to 44%). Younger patients used bolus wizard on regular basis (>75%), which was significantly higher than other age groups (P < 0.05). More than 50% of patients achieved glycated hemoglobin (HbA1c) <7.0% and >70% of patients achieved HbA1c <7.5%. HbA1c level significantly changed from baseline in all groups (P < 0.05).
Conclusion:
Our study shows improved glucose control in long-term CSII users. A reduction of HbA1c levels by −1.1% was maintained during the study period.
Introduction
T
Continuous subcutaneous insulin infusion (CSII) is an established model for mimicking physiological insulin, which can assist in achieving and maintaining these goals. Multiple daily injection (MDI) barriers such as dose adjustments by unit, less flexibility, and insulin stacking can be minimized using CSII. Multiple trials have shown that CSII therapy can improve diabetes management in T1D patients by improving glucose control and better quality of life with less hypoglycemic events. 6 –8 It can decrease glycemic variability, dawn phenomenon, and improve glycemic control. 7,9,10 Several retrospective studies have shown the long-term benefit of improvement in hemoglobin A1c (HbA1c), 11,12 wherein this therapy appears to be safe and effective in T1D regardless of age. 13
The use of CSII in Macedonia as out-of-pocket policy began in 2002. The first 1-year experience 14 showed improved glucose control among uncontrolled T1D patients, decreasing HbA1c to 7.4%. Our experience and several publications in CSII, continuous glucose monitoring (CGM), and sensor-augmented pump (SAP) 15,16 was used to influence on the Health Care Authorities to start a program for reimbursement of CSII and disposals. Our center treated >97% of T1D patients on CSII (October 2014), which can be a representative model for Macedonia.
The objective of this retrospective and cross-sectional study of cohort of patients with T1D treated by CSII is to describe insulin pump characteristics and long-term effects on glucose control in real-life conditions.
Methods
This single-center retrospective and cross-sectional study was conducted by the Center for Insulin Pump and Sensor at University Clinic of Endocrinology in Skopje. The study enrolled patients with T1D using CSII for >3 years during October 2004 until October 2014. Our Center uses Medtronic Minimed insulin pumps (Medtronic 722 and 754; Medtronic, Northridge, CA), where previous models (Medtronic 508 and 711) were upgraded accordingly (pump malfunction, no pump disposals available, or upgrade after 5 years of use).
Patients were excluded from the study if CSII use was transitory or for <3 years and diagnosis of T1D was not firmly established. According to our standards of care, CSII treatment was initiated during a 5-day out-patient group education program (2–3 patients) with previous carbohydrate-counting sessions.
CSII therapy was usually started with 10%–20% reduction in total daily dose (TDD) of MDI, basal/bolus distribution 40/60, four to five basal rates, and insulin-to-carbohydrate ratio (ICHR) formula of 300–450/TDD and insulin sensitivity factor (ISF) formula of 90–110/TDD (mmol/L). We set glucose target range from 5.0 to 7.2 mmol/L, with two ISFs (nighttime is usually 10%–20% higher than the daytime).
Baseline data at CSII initiation were collected through the electronic medical record system used at our center: sex, age, weight, diabetes duration, and initial and current HbA1c levels.
The cross-sectional analysis was conducted from January 2016 to December 2016 by telephone, e-mail, or social media (Facebook and Viber) to collect actual data, including the recent HbA1c level, weight, insulin daily dose, basal ratio, and bolus wizard use. Collected data were analyzed together with CSII reports generated by Carelink Therapy Management Software (Medtronic).
Statistical analysis was performed with SAS version 12.5 for Windows (SAS Institute, Cary, NC). Quantitative variables are expressed as the mean ± standard deviation. Number of basal rates, ICHR, and ISF are expressed as the median (interquartile range). The HbA1c variation from baseline was analyzed using the paired Student's t-test. Comparisons between HbA1c levels according to CSII duration and between age groups (12–18, 19–24, and >25 years) were performed using a Student's t-test. A P value <0.05 was considered to denote significance.
Results
Among 189 CSII-treated patients during the 10-year period, 162 patients met criteria for analysis (as shown in Figure 1). Patients were distributed according to age (12–18, 19–24, and >25 years) to meet different habits, lifestyle, and real conditions. Demographic characteristics of this population are described in Table 1. Indication for CSII was high HbA1c (58%), dawn phenomenon (21%), glucose excursions (12%), hypoglycemia (5%), and patient preference (4%). Diabetes duration was longer in adults than in adolescents.
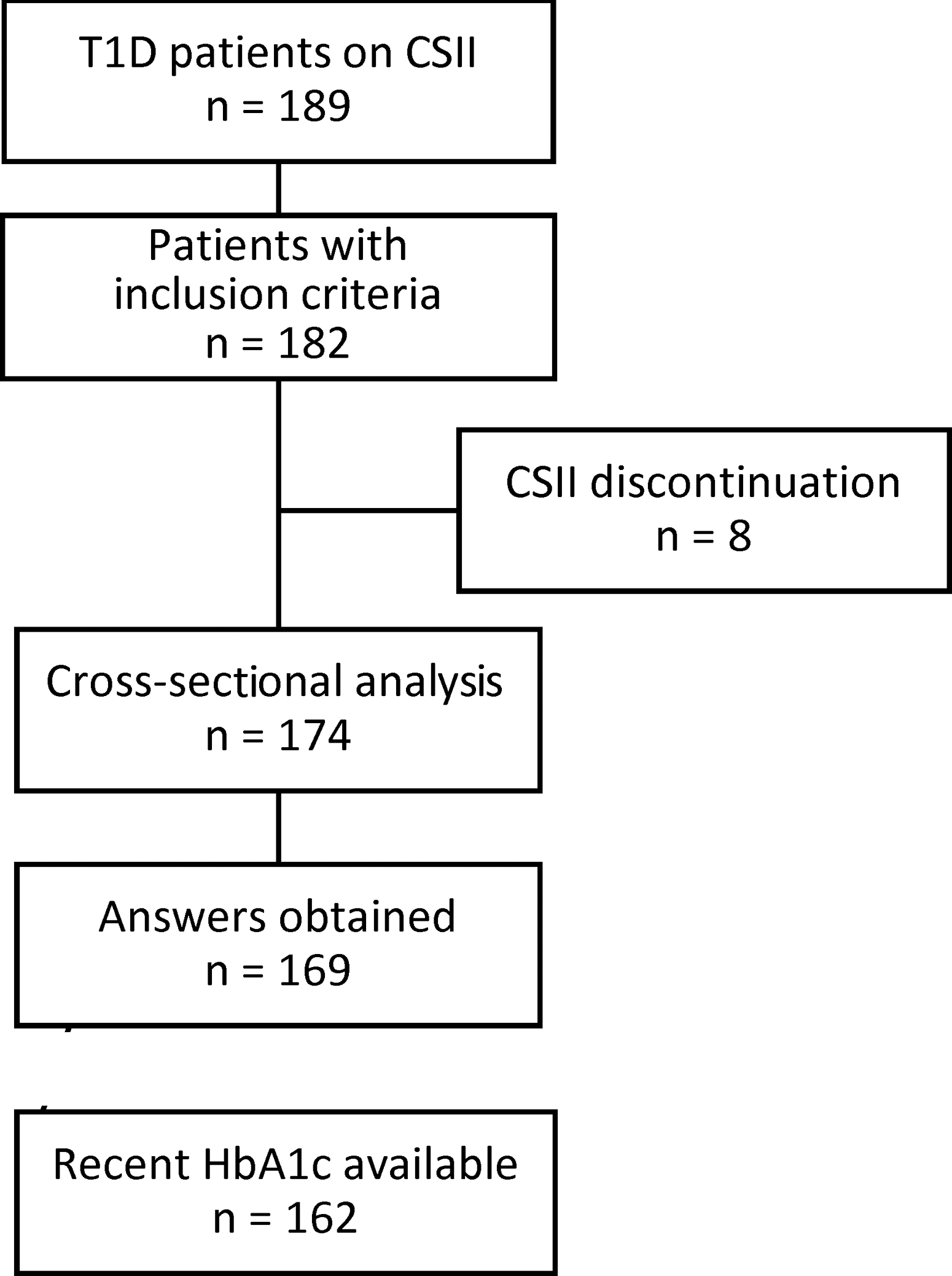
Flowchart. CSII, subcutaneous insulin infusion; T1D, type 1 diabetes.
CSII, subcutaneous insulin infusion; HbA1c, hemoglobin A1c.
All patients were treated with CSII for >3 years. TDD was >0.85 U/(kg·day) in age group 12–18 years (Table 2), which was significantly higher than that in the other two age groups (P < 0.05). Basal ratio was lower in younger age (<40%) and showed a trend of increasing with age and longer diabetes duration (44%). No significant difference was found in number of basal rates in all groups. Younger patients used bolus wizard on a regular basis (>75%), which was significantly higher than other age groups (P < 0.05). There was no significant difference in ICHR, ISF, and active insulin between groups. More than 50% of patients achieved HbA1c <7.0% and >70% of patients achieved HbA1c <7.5%.
Values are expressed as mean ± standard deviation unless otherwise indicated.
ICHR, insulin-to-carbohydrate ratio; IQR, interquartile range; ISF, insulin sensitivity factor; N.S., not significant; TDD, total daily dose.
HbA1c level significantly changed from baseline in all groups (P < 0.05). No significant difference between groups was found. Highest reduction of HbA1c levels by −1.3% was found in patients with CSII duration from 3 to 6 years (Fig. 2).
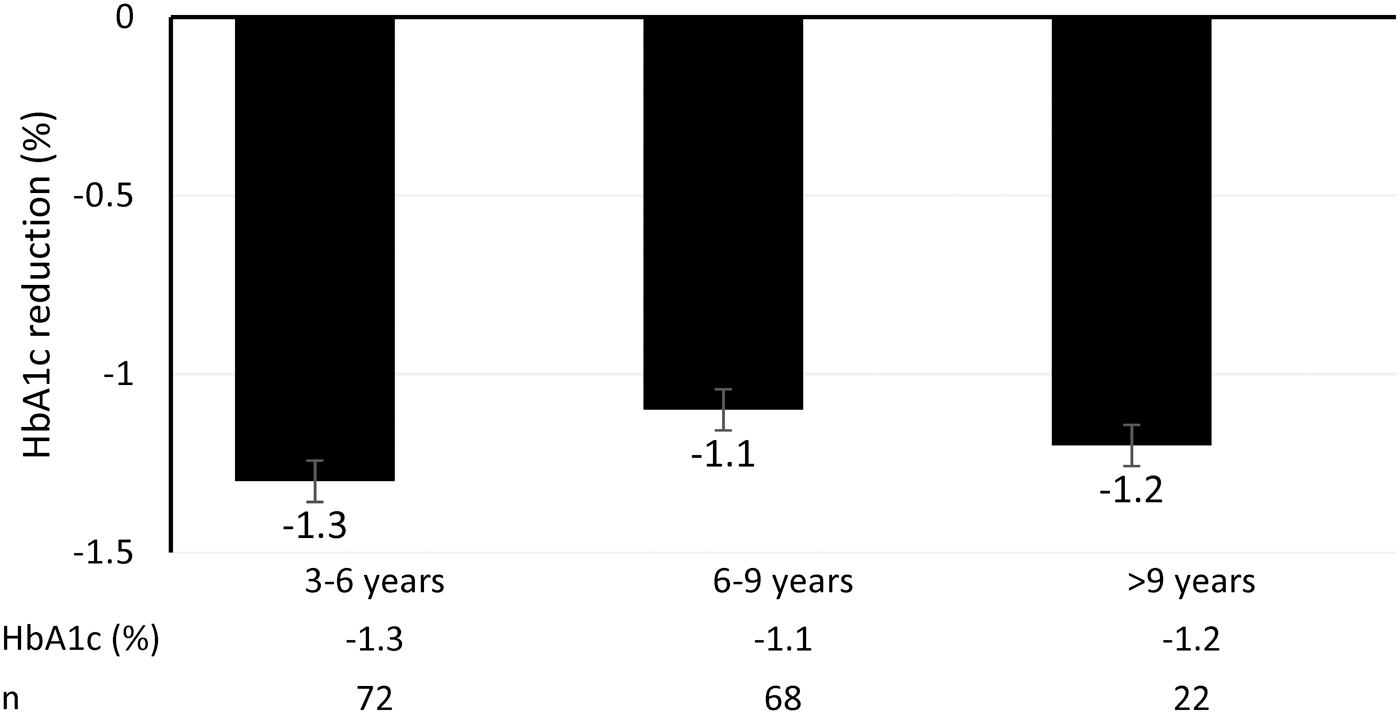
HbA1c variation from baseline to recent value (during analysis) according to CSII treatment duration (mean ± standard deviation). HbA1c, hemoglobin A1c.
Weight was significantly increased in patients with CSII duration >3 years (<3 years, 59.4 ± 10.2 kg; 3–6 years, 64.6 ± 9.2 kg; >6 years, 63.7 ± 8.7 kg)
Discussion
In this study, we described insulin pump characteristics and long-term effects on glucose control of a cohort of patients with T1D treated with CSII for several years. The design of our study included data collection on CSII utilization and reports obtained by CSII downloads. The CSII duration in our study is >4 years in all age groups, which can be a representative model for long-term analysis.
In this study, CSII efficacy and safety could not be analyzed due to retrospective design, lack of a control group, and missing data. Previous meta-analyses of prospective studies reported reduction in HbA1c levels of −0.2% to −0.7% 17,18 and retrospective studies showed decreased HbA1c levels by −0.5% to −1.3%, 13,19,20 both with CSII in comparison with MDI. In contrast, our finding shows sustained reduction of HbA1c levels by −1.1% with CSII utilization after 6 years. In our study, >70% of patients achieved and maintained HbA1c <7.5%. Possible explanation of improved glucose control is high degree of educational support for Flexible Insulin Therapy (FIT) at the moment of CSII initiation, re-education sessions on a yearly basis, and social media use between patients and healthcare providers. Around 74% of our CSII patients use social media to gain diabetes knowledge and information and interact in their daily insulin adjustments. 21,22
We did not find significant difference in basal ratio (38%–45%) and number of basal rates (4–5), which are comparable with other studies. 23,24 The average of four basal rates in adults can be explained with our standards of care of CSII initiation at the age of adolescent in this group.
Several authors found an improvement in glucose control when using the bolus wizard function, 25 –27 where the use of this feature is from 50% to 100%. Another study reports that 60% of all patients are using advanced functions continuously. 28 Our results support this finding, where 78% of adolescents and >50% of adults use the bolus wizard feature. More focus should be made during education session in adults to stress the importance of this feature. ICHR and ISF in all age groups are calculated and used by a well-established calculation formula. 29
Concerning safety issues, we found an incidence of 0.01 events per patient/year for severe hypoglycemia, which is particularly low. Low rate of hypoglycemia was also reported by other authors, 30 where CSII therapy achieves and maintains its efficacy mainly in terms of reducing severe hypoglycemia. 31 We also found a very low rate of hospitalization for diabetic ketoacidosis (DKA), which can be explained by improved glucose control, frequent visit, motivation, and education in patients. The incidence of DKA with CSII utilization is controversial, with an increase in studies performed before 1995 and conflicting results in subsequent studies. 19,32 DKA can be reduced and avoided with proper education to functional insulin therapy and good diabetes care. 33
Our study presents several limitations including the lack of a comparative group of MDI, existence of missing data, and single-center study for possible missed data for self-reported severe hypoglycemia. However, the strengths of our study are its large sample population, its long length of follow-up, and its real-life conditions.
Conclusion
In this study, we showed improved glucose control in long-term CSII users, where safety and efficacy were maintained for several years of pump utilization. A reduction of HbA1c levels by −1.1% was maintained during the study period.
Footnotes
Acknowledgments
G.P. performed the study concept and design, data acquisition, statistical analysis and interpretation of data, drafting the article, and clinical revision of the article. M.Z. performed data acquisition, statistical analysis and interpretation of data, and clinical revision of the article. S.S.S. performed statistical analysis and interpretation of data. B.J.T. performed data acquisition.
Author Disclosure Statement
No competing financial interests exist.