
Abstract
We sought to determine the real-life experiences of individuals traveling long distance (across five or more time-zones) with type 1 diabetes (T1D). Five hundred three members of the T1D Exchange online community (
Introduction
F
At present there is a paucity of research on the impact of long-distance travel and type 1 diabetes (T1D), with a number of online resources suggesting that potential travelers “discuss” this with their diabetes specialist teams. The aim of this study therefore was to capture the real life experiences of adults traveling long-distance with T1D, and to determine how overall self-management for travel may be impacted by use of different diabetes-related technologies for glucose monitoring and insulin delivery.
Methods
Survey description
We conducted a 45-question online survey assessing travel experiences for people living with T1D (Supplementary Data; Supplementary Data are available online at
Study procedure
Participants were recruited from the T1D Exchange's online patient community, Glu (
Statistical analysis
The cohort was stratified by duration of T1D [0–5 years, 6–10 years and >10 years] and whether or not participants used continuous subcutaneous insulin infusion (CSII) therapy and/or a continuous glucose monitor (CGM): CSII and CGM together, CSII only, CGM only, or neither CGM nor CSII. Data were analyzed using SPSS 23 (IBM, Chicago, IL). No transformations of the data were required. Frequency tables and cross-tabulations of categorical variables were created and evaluated using the Chi-squared statistic. For significance testing, the alpha was set at 0.05.
Results
Subject characteristics
Five hundred three individuals completed the survey and were included in the analysis, although not all questions were answered by each individual. Of this sample, 71% were women and the mean age was 44 ± 15 years (range 18–83 years). Eighty-five percent of participants had an HbA1c between 6.0% and 7.9%. The cohort reported duration of T1D 0–5 years (n = 78), 6–10 years (n = 48), >10 years (n = 368). Participants reported using diabetes management technologies (CSII therapy and/or a CGM) as follows: CSII and CGM (n = 307), CSII only (n = 102), CGM only (n = 23), or neither (n = 64).
Passport, destination, travel purpose
Eighty-one percent of participants reported having a current passport. Seventy-one percent had traveled internationally in the past 5 years. Participants mainly traveled long distance for vacation (84%), business/study (38%), and visiting family/friends (33%). The three most popular international destinations were Italy (25%), France (25%), and Canada (21%).
Travel challenges, fears, and frustrations
Nine percent of participants reported problems with their diabetes management causing them to avoid international travel altogether and half of these respondents reported experiencing diabetes-related problems causing them to consider alternative destinations in the future. A small proportion (4%) reported needing to seek medical attention for T1D-related problems while overseas during the past 5 years. Overall 74% reported more hypoglycemia and/or hyperglycemia while traveling abroad.
Participants noted the most challenging part of long-distance travel was trip preparation (30%) and navigating airport security (26%). Common practical difficulties included taking enough supplies (51%) and crossing time zones (47%). Their greatest fears regarding travel were losing supplies (30%), potential problems with airport staff/security (26%), and a perceived risk of unstable blood glucose levels (20%).
The most common resources used to find information on managing T1D during travel were the internet (55%) and a healthcare provider/diabetes educator (25%). However, participants also reported frustrations with the existing sources of information such as not taking into account the unpredictability of self-management needs (37%), there not being enough information (29%), and information not available in a single location (27%) (Fig. 1). Two-thirds reported that they would be open to using a flight calculator that generated suggested insulin dosage adjustments when crossing time zones, while almost a quarter already regularly use a smartphone for mobile diabetes care.
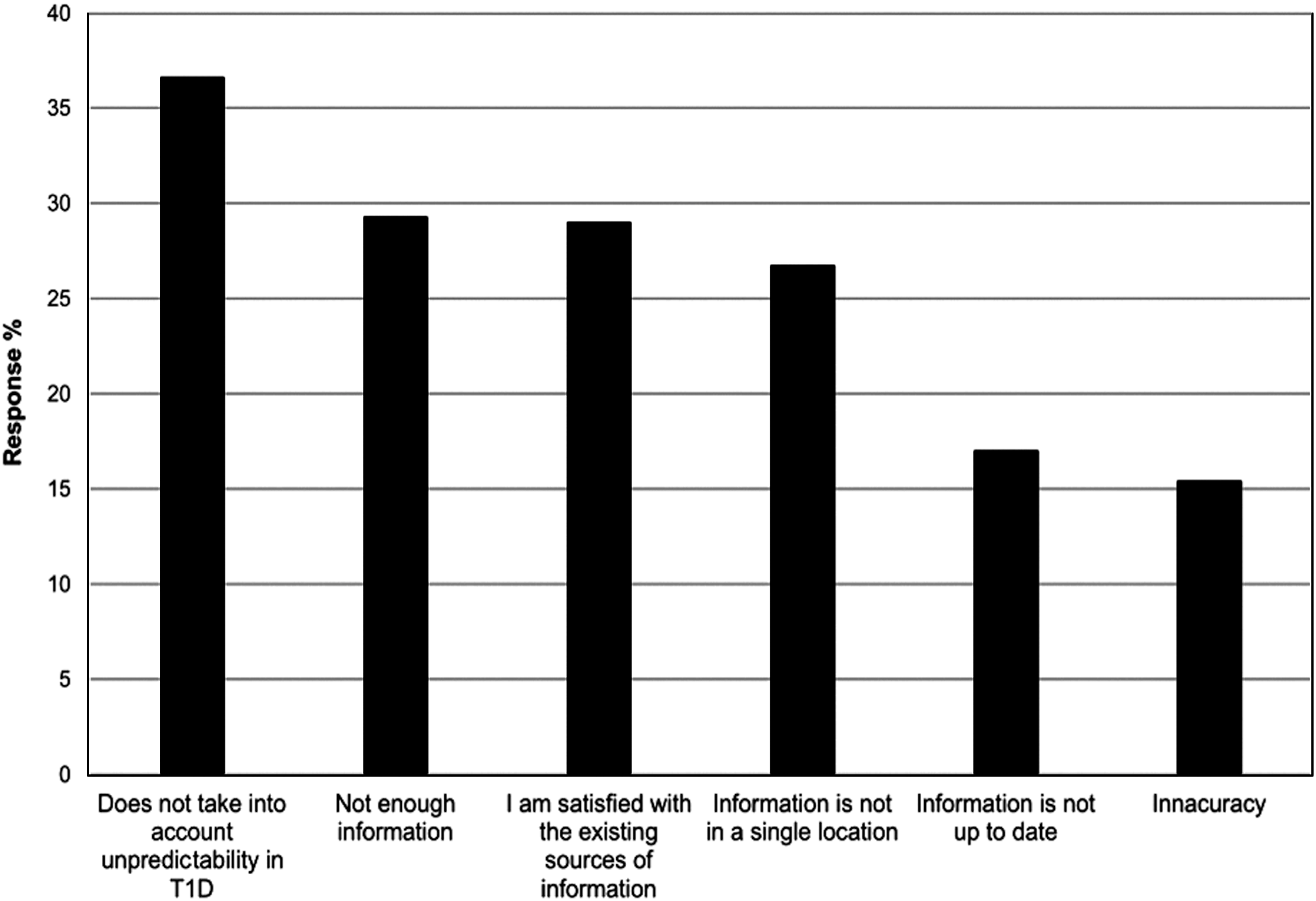
Percent of survey participants who agreed when asked “What is your biggest frustration with current sources of information for the management of T1D while traveling (choose all that apply)?” T1D, type 1 diabetes.
Airport security
Ninety-one percent of respondents did not notify the airline that they were planning to fly with a diagnosis of T1D. However, 72% of CSII and 43% of CGM users reported notifying airport security of their device. Furthermore, 42% of CSII users wore their device while going through body scanners and/or metal detectors, while 12% report disconnecting their device and sending through the X-ray scanner. Forty-four percent of participants noted having at least one negative issue with the airport security process in the past due to their T1D.
Insulin and device use while traveling
One-third of participants felt that their insulin did not “work the same” during an actual flight. For CSII users, 10% reported difficulties with their device during a flight. At a practical level, the majority (69%) always wore or carried medical identification highlighting their T1D and almost all followed manufacturer's instructions to store insulin in carry-on luggage (94%) rather than in the aircraft hold. However, 51% never carried emergency glucagon while traveling. Furthermore, 22% of participants had run out of insulin at some point during at least one trip in the last 5 years.
Device use and travel experiences
When asked, “Do you experience more episodes of hypoglycemia and/or hyperglycemia when traveling compared to when you are not traveling?” there were no differences between the device groups (Table 1). For CSII users their primary anxiety was “losing supplies,” while non-CSII users described concerns over “unstable blood glucose (highs and lows)” (P < 0.05). In addition, CSII users were also more likely to have difficulty with airport security than non-CSII users (P < 0.001). There were no differences between device use groups in the following categories: difficulty with crossing time zones, difficulty with insulin storage, taking enough supplies, or interacting with other travelers (Table 1).
CGM, continuous glucose monitor; CSII, continuous subcutaneous insulin infusion; T1D, type 1 diabetes.
Discussion
People living with T1D face unique challenges while traveling. Although only 2% of in-flight medical emergencies requiring support from a healthcare provider are due to diabetes, 3 we found that flying can be challenging and for some this can lead to complete avoidance of long-distance travel. The impact of long-distance travel can also result in negative practical and psychological experiences at all stages: from planning, dealing with airport security, during the flight, at the destination or during the return journey.
In this study, almost three quarters of participants with T1D and with experience flying long distance over the past 5 years reported more hypoglycemia and/or hyperglycemia while traveling overseas and 9% had subsequently avoided international travel altogether because of problems related to their diabetes management. In terms of planning long-distance travel and T1D, the respondents raised specific concerns about potential inadequacies of current sources of information available to them on this topic and also to the unpredictability of self-management needs while traveling. Overall respondents reported there are a lack of resources adequately addressing how to deal with emergencies while abroad, how to more easily navigate airport security, and managing insulin when crossing time zones. This is reflected in difficulties reported with even basic preparation, where 22% of participants had reported running out of insulin at some point during an overseas trip.
Although only 2% had insulin lost or stolen while traveling internationally, the potential for this was a cause of anxiety for a majority of CSII users, while non-CSII users were more concerned about “unstable blood glucose (highs and lows).” In addition, one in five participants reported they would attempt to make contact with their U.S. physician as their first response to an adverse event abroad such as losing their insulin, which could be difficult from abroad. One potential solution to provide immediate access to reliable information could be the incorporation of evidence-based smart phone apps in diabetes management.
Prior surveys show more than half of travelers with diabetes reported difficulties in glucose management during their journey compared to the month before leaving. 4 Around 10% of insulin-treated travelers experienced problems, most commonly hypoglycemia, during the journey or in the first 24 h after arriving at their destination. 5 For long-distance travel in particular, there is evidence that most physicians, including diabetes specialists, are uncertain about how to adjust insulin doses for patients who travel across several time zones with some of the information provided described as “potentially harmful.” 6 In addition, recent testimony from online bloggers and patient forums continues to highlight specific problems related to diabetes and travel. 7
Currently, few resources offer practical and easy to understand travel guidance to individuals with T1D and other insulin users. Available sources of information have been around for many years, and include publications targeting physicians and scientific researchers, online articles providing generalized tips (transportation and storage of supplies, suggested immunizations, diet regimens) and free electronic dosage calculators for modifying insulin doses across time zones. 8 –15 While for the most part these articles are well written and offer sound counsel, some guidelines are overly complicated with medical jargon and complex tables describing insulin dosing adjustments, posing a problem for both patients and providers looking for simple advice. 16,17 Furthermore, a prior travel study in the United Kingdom reported that most patients with diabetes still faced difficulties maintaining glycemic control even when clinic staff provided advice, and that there was great variation in the advice offered. 6
A limitation of this study is the potentially biased sample population. Eighty-one percent of participants reported having a current passport or other travel document allowing them to fly internationally, suggesting they may have given consideration to these issues before. It is also noteworthy that the average HbA1c for this population was lower than that reported from national registries for T1D. 18
Ultimately, while experiences of participants differed across travel patterns, the commonalities of lacking emergency abroad protocols, encountering security issues, and struggling to maintain regulated basal insulin rates across new time zones presented serious concerns. Thus, a better understanding of the fears, difficulties, and needs of patients traveling with T1D will allow for the development of individualized and practical resources.
Footnotes
Acknowledgments
We would like to acknowledge T1D Exchange, a program of Unitio, Inc., for supporting this study and we thank the Glu community for their participation. In addition, we would like to acknowledge Jenny Martinez, Project Coordinator, William Sansum Diabetes Center, for assistance in developing the survey and Dr. Danielle Gianferante for her assistance with statistical analysis. This article was funded in part by a grant from the Mosher Foundation to the William Sansum Diabetes Center.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.