
Abstract
Background:
The rate of glycemic control among diabetes patients in China is currently low. The current study aims at determining the effect of structured self-monitoring of blood glucose (SMBG) on blood glucose control as well as quality of life (QoL) in Chinese diabetes patients.
Methods:
In a 24-week, single-center, randomized, open-label, prospective trial, patients with glycated hemoglobin A1c (HbA1c) >8.0% were randomized to an intervention group for structured SMBG (n = 121) or a control group (n = 129). Patient data were analyzed separately according to treatment with or without insulin. At 0, 3rd, and 6th months, life satisfaction was assessed using the Chinese Normal Audit of Diabetes-Dependent Quality of Life (CN-ADDQoL) questionnaire.
Results:
The mean HbA1c decrease from baseline to the study end was significant for both groups with insulin treatment (intervention group: −1.79% ± 1.97%, P < 0.001; control group: −1.05% ± 1.87%, P < 0.001) or without insulin treatment (intervention group: −1.91% ± 1.90%, P < 0.001; control group: −1.35% ± 1.82%, P < 0.001). Moreover, the insulin-treated patients in the intervention group showed a significantly more robust HbA1c decrease than those in the control group (P = 0.007). Both therapeutic subgroups in the intervention group had a significantly higher frequency of SMBG than those in the control group (P < 0.001), but no strict deterioration of the QoL was detected. In addition, a significant HbA1c reduction after 6 months of SMBG was seen for both insulin-treated patients (P = 0.027) and noninsulin-treated patients (P = 0.006) younger than 66 years.
Conclusions:
Featured with no strict deterioration of QoL, structured SMBG was proven to be effective on the glycemic control in patients with insulin treatment, as well as in young and middle-aged patients without insulin treatment.
Introduction
I
Recently, the Chinese 3B study designed to assess the degree of control of blood glucose (BG), blood pressure, and blood lipids (3Bs) among patients with T2DM has revealed that only 47.7% of T2DM patients had reached the target glycemic level (glycated hemoglobin A1c [HbA1c] <7.0%), whereas this percentage was 41.1% in 2006. 3 This suggests that there are many diabetes patients with poor glycemic control in China, and new management strategies are necessary to improve their glycemic outcomes.
The clinical application guide of blood glucose monitoring in China (Edition 2011) recommends a test frequency of at least three paired tests every week in noninsulin-treated patients compared with a test frequency of three times per day in insulin-treated patients. 4 Paired glucose test is to encourage patients with diabetes to focus on “before and after” testing: before and after meals, before and after exercise, before and after sleeping, etc. This at least gives the person a sense of cause and effect and a pattern to the otherwise seemingly “random” affair of testing their blood throughout the day.
Although self-monitoring of blood glucose (SMBG) has been considered crucial for the long-term health of diabetes patients, patient adherence in China is poorer than that in the developed countries. Only 18.98% of the Chinese patients reportedly performed SMBG with the recommended frequency, whereas 81.02% of the patients did not. In addition, nearly 35.36% of the patients reported that they had never performed SMBG. In the insulin-treated subset, only 7.27% of the patients performed SMBG at least once a day, whereas 33.05% never did. 5 By contrast, the frequencies of SMBG among diabetes patients in the United States and United Kingdom are 19 and 17 tests per week, respectively. 6,7
A previous study of Chinese patients reported that a structured SMBG regimen increased SMBG frequency and improved HbA1c as well as quality of life (QoL) outcomes in insulin-treated T2DM patients. 8,9 This approach appears to facilitate a reduction in the HbA1c level and to increase the percentage of patients who reach the target HbA1c level within 6 months of intervention. Moreover, SMBG has been found to be effective as a tool in the self-management of glucose levels in patients with T1DM as well as those with T2DM receiving insulin therapy. 10
However, the benefits of SMBG in a noninsulin-treated patient with T2DM are mixed. In addition, there is little evidence regarding how SMBG affects the satisfaction, general wellbeing, or general health-related QoL in diabetes patients in China. It was thus hypothesized that a structured, paired SMBG regimen, supported by appropriate training in recording SMBG, would improve glycemic control and QoL among Chinese patients and encourage them to increase the daily frequency of SMBG measurements. The present single-center, prospective, randomized, controlled study was conducted in patients with poorly controlled diabetes in China, including both T1DM and T2DM treated with or without insulin, to evaluate the effect of paired BG measurements on the glycemic control and psychosocial and behavioral characteristics of diabetes patients in China.
Methods
Study population
Outpatients diagnosed with diabetes in the Shanghai Jiao Tong University Affiliated Sixth People's Hospital were enrolled in this study. To be eligible for inclusion, patients had to have been diagnosed with diabetes mellitus with HbA1c ≥8% measured within 1 month before enrollment. Patients should not have been performing SMBG on a regular (daily) basis within 3 months before enrollment, and be willing to perform daily SMBG during the follow-up period. The study was approved by the Ethics Committee of the Shanghai Jiao Tong University Affiliated Sixth People's Hospital. All participants provided written informed consent before enrollment. This study is registered with
Patients were not eligible for the study if they had any retinopathy that required photocoagulation or retinal surgery in the 6 months before enrollment or that might require photocoagulation or retinal surgery during the study. Patients were also excluded if they had any clinically significant condition that required hospitalization in the 2 months before enrollment or that might require hospitalization (e.g., elective surgery) during the study, or any clinically significant psychosis or cognitive impairment. Patients who were pregnant or contemplating pregnancy also were excluded.
Study procedures
After screening and a 3-month run-in phase, patients were randomized in a 1:1 ratio to either the intervention group (structured SMBG: perform one paired BG test compulsorily every day) or the control group (no-structured SMBG: perform routine BG tests as usual). The allocation sequence was generated by the institutional trial pharmacist and masked to the physicians (by the use of sealed envelopes) at the time of randomization (ensuring low risk of allocation bias). After randomization, the sequence was no longer masked for the study physicians (who also assessed outcomes and analyzed the data) or patients.
Demographic data and clinical characteristics at baseline, month 3, and month 6 were recorded for patients eligible and willing to participate in this trial. These characteristics included body mass index (BMI), HbA1c, fasting plasma glucose (FPG), 2-hour postprandial plasma glucose (2hPG) self-efficacy score, and QoL score.
Study parameters were evaluated using physician's records, laboratory results, and patient questionnaires. In the intervention group, patients were taught to use the BG meter and were asked to regularly perform one pair of BG measurements (two times before and after breakfast, lunch, or dinner) daily and to record the results in a log book. An educational program was delivered by the therapeutic group in the investigation center. The therapeutic group included a professional diabetes physician and a well-educated nurse. Both intervention and control groups are taught for the evaluation and management of their diabetes by the same course. In the control group, patients were not required to perform daily BG tests. Instead, they only needed to continue with their routine behaviors. The educational program also was delivered to these patients by the therapeutic group.
Both the intervention and control group underwent an initial teaching program for 30 min, during which patients were instructed on the types and use of antidiabetic drugs, setting of glycemic targets, and improvement of a healthy lifestyle. During the visits, there was a concomitant educational class during which the therapeutic group reviewed each patient's previous BG results and adjusted the patient's therapeutic regimen. The patient could then follow the adjusted prescription and perform further monitoring of BG.
The follow-up duration was 6 months for both groups. During the follow-up visits, patients in the intervention group used a meter to measure their BG. The physician assessed the correct use of the monitoring device and the accuracy of patient self-monitoring and provided an extra educational session to help the patient to manage his/her life pattern and BG monitoring. Meanwhile, the control group was not required to perform structured SMBG and received an educational program only for the self-management regimen. The patients in the control group received no instruction regarding their BG test frequency.
Patients in both groups returned for outpatient visits at the 3rd and 6th months for comprehensive blood and urine tests as well as completion of the QoL questionnaire. This study assessed the impact of recommending a structured SMBG regimen, supported by education and behavioral interventions, on treatment outcome.
To evaluate QoL, we used the Chinese Normal Audit of Diabetes-Dependent Quality of Life (CN-ADDQoL) instrument. 11 This instrument includes impact and importance scores. The impact score is determined by asking “If I did not have diabetes, my (life domain) would be”: with ratings of −3 to +1, whereas the importance score is determined by asking “My (life domain) is”: with ratings of 0 to +3. In addition, two overview items represent current QoL and QoL without diabetes, with ratings from −3 to +3 and −3 to +1, respectively. A higher score indicates that the issue is more impactful and important for life domain and that the current situation is poorer.
Four other questions were raised to examine patient-reported self-management of blood glucose: “Have you always followed your physician's prescription to test your BG?,” “Have you taken the medicine according to physician's prescription?,” “How often have you adjusted the insulin dosage based on paired BG test results?,” “How often do you test your BG every day?” The answers to the previous three questions were scored from +1 to +4, with a higher score indicating a poorer current situation. The result for the last question was calculated by the test frequency, with one pair of BG tests equaling two BG monitoring events.
Main outcomes
The primary endpoint was the change in HbA1c from baseline to the third and sixth months in both the intervention and control groups. Secondary endpoints included the change in QoL score from baseline and the change in daily testing frequency.
Statistical analysis
Patients were included in the analysis if they had completed the baseline protocol after assessment of exclusion criteria. Parametric tests were used because variables were found to follow a normal distribution. One-way analysis of variance was used to analyze the differences from baseline to the 3- and 6-month follow-ups in the same group. Independent Student's t-tests were used for comparison of characteristics and of differences in HbA1c and pre- and postprandial BG between groups in the baseline, 3-month, and 6-month visits. The generalized linear model was used to analyze the corelationship of timing, grouping, and therapeutic method with BG, QoL, and BG testing frequency. Data are reported as the mean ± standard deviation (SD) unless otherwise stated, and a P value of <0.05 indicated a significant difference. The Statistical Package for the Social Sciences for Windows, version 20.0 (2012), was used for data analysis.
We aimed to detect a difference of at least 0.5% in the change from baseline in HbA1c, assuming a SD of 1.5%, an α of 0.05, and a power of 90%. Based on a dropout rate of 20%, we calculated that a sample size of 205 patients was needed per arm for each patient segment.
We did an interim analysis when the 205th patient finished the final visit. The trial was terminated early due to a significant HbA1c efficacy outcome. At the time the trial ended, 250 patients had been recruited.
Results
Characteristics of patients included in the final analysis
Of the 250 patients enrolled and randomized in this study (Fig. 1), 121 were randomized to the intervention group and 129 were randomized to the control group. A total of 18 patients (10 from the intervention group and 8 from the control group) withdrew their consent, discontinued the study, or were withdrawn from the study. Among the enrolled population, the mean patient age was 58.67 ± 10.93 years, and 60.8% of patients were male and 39.2% were female. The demographic characteristics of the patients included in the final analysis are presented in Table 1.
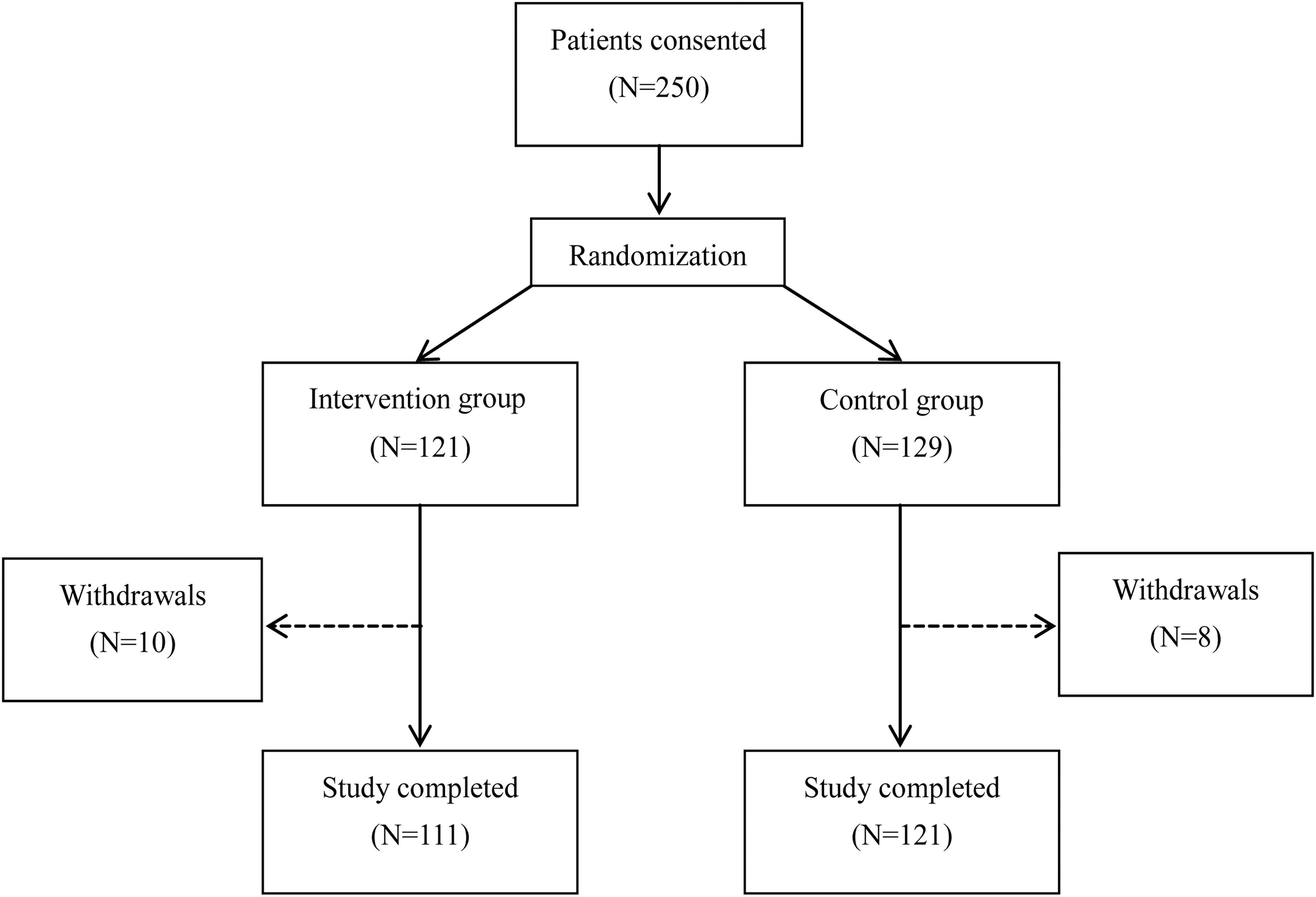
Study flow and patient grouping.
Data are expressed as mean ± SD, or n (%).
BMI, body mass index; DM, diabetes mellitus; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin A1c; 2hPG, 2-hour postprandial plasma glucose; SD, standard deviation.
Comparisons of glycemic control
No difference in HbA1c was observed between the intervention and control group at baseline. After 3 and 6 months of intervention, more significant reductions in HbA1c were observed in the intervention group compared with the control group (P = 0.003 and 0.001, respectively).
With further division of patients into insulin-treated and noninsulin-treated subgroups, the difference in HbA1c reduction between the intervention and control group was significant for insulin-treated patients, but not for noninsulin-treated patients (intragroup P < 0.05 in insulin-treated patients at months 6; intragroup P > 0.05 in noninsulin-treated patients at both months 3 and 6).
In further investigating the BG outcomes in noninsulin-treated patients, we found that the mean HbA1c level decreased from baseline to the end of month 3 (intervention group: −2.02% ± 1.91%, P < 0.001; control group: −1.43% ± 1.75%, P < 0.001) and month 6 (intervention group: −1.91% ± 1.90%, P < 0.001; control group: −1.35% ± 1.82%, P < 0.001). The mean HbA1c levels of patients in each group and at each visit are illustrated in Figure 2.

In intergroup comparisons, a significant difference only existed between the intervention group and the control group at the 6-month follow-up in the insulin-treated population (P = 0.035). A nonsignificant trend of HbA1c improvement was observed for noninsulin-treated patients in the intervention group, but not for those patients in the control group (P = 0.123).
Comparisons of the BG test rate
After 6 months of BG management, patients in the intervention group had an approximately once daily BG test rate, whereas those in the control group had a poorer BG test rate of less than once daily. Differences were observed between the two groups in terms of the changes in test rate after 3 and 6 months (P < 0.001). A time effect existed for both insulin-treated and noninsulin-treated patients in the intervention group and for insulin-treated patients in the control group.
Comparisons of impact scores for QoL events
The impact score for QoL events was poorer in the intervention group than in the control group at the 3-month follow-up (intervention group: −13.57 ± 7.68; control group: −11.25 ± 7.18, P = 0.016). However, the difference was not significant at the 6-month follow-up (intervention group: −15.42 ± 12.53; control group: −13.73 ± 13.51, P = 0.327). Moreover, the important score for the whole study period (the baseline, the 3-month follow-up, and the 6-month follow-up) showed no difference between the intervention and the control group (all P > 0.05).
When asked “In general, my present quality of life is”: patients in the intervention group showed better improvement after 6 months of BG management than those in the control group. Upon separation of patients according to treatment with or without insulin, both treatment strategies contributed to more significant improvement in the intervention group compared with the control group by the 6-month follow-up (P = 0.021 and P < 0.001, respectively). However, for the question “If I did not have diabetes, my quality of life would be”: there was no difference between the intervention and control groups independent of treatment with insulin.
Multiple factors influencing the reduction in HbA1c
There is no difference on insulin adjustment frequency at baseline when compared with that of the third-month follow-up and the sixth-month endpoint, both in intervention and control groups, and in insulin and noninsulin-treated patients. However, only the proportion of HbA1c <7% at the 3-month follow-up tended to be significantly different (8.7% vs. 22.8%, P = 0.025) between the intervention group and control group in patients treated with insulin. To identify the factors that influenced the reduction in HbA1c, we included age, BMI, physical activity statement, complications, and test frequency in the analysis. The results showed that age correlated negatively with the number of patients reaching the target HbA1c level (β = −0.006, P = 0.024); that is, as age increased, the likelihood of reaching the target HbA1c decreased.
Further analysis according to patient age
To further explore the role of age, we considered age as a segmented factor and found that patients younger than 66 years of age in the intervention group had a significantly greater reduction in HbA1c after 6 months of BG management compared with those of the same age in the control group independent of whether they were treated with insulin (P < 0.05, Fig. 3). Reductions in HbA1c differed significantly between the intervention group and the control group in patients older than 66 years of age with insulin treatment (P < 0.05, Fig. 3A). However, reductions in HbA1c did not differ significantly between the intervention group and the control group in patients older than 66 years without insulin treatment (P > 0.05, Fig. 3B). In addition, patients older than 66 years in the intervention group had a significant poorer QoL score compared with those of the same age in the control group (P = 0.017), whereas no difference in QoL score was found between the intervention group and the control group in patients younger than 66 years.

Discussion
Effects of structured SMBG on glycemic control
Recently, multiple clinical studies have focused on the effectiveness of SMBG in the management of diabetes mellitus in both T1DM and T2DM patients. 9,10,12 In the COMPASS study, a structured SMBG regimen supported by training in SMBG data interpretation and therapy changes based on SMBG data were found to contribute to an increased frequency of SMBG in insulin-treated, poorly controlled T2DM patients. 9 A meta-analysis showed that SMBG has confirmed antidiabetic efficacy in patients with T1DM and those with T2DM using insulin therapy, whereas, the overall effect of SMBG on glycemic control in patients with T2DM who are not treated with insulin is small. 10 In contrast, a Chinese meta-analysis came to a different conclusion that SMBG combined with diabetes management effectively improves glycemic control in noninsulin-treated T2DM patients. 12
In our study, education played an important role in the management of diabetes. Patients in both the intervention and control group received an extra 30 min of educational training during the recruitment and the follow-up visits, and the intervention group strictly complied with the physician's prescription of BG tests after the treatment, whereas the control group was only required to measure their BG levels as usual. After 6 months of monitoring, patients in both the intervention and control groups showed improvement in HbA1c. However, when categorized by treatment with or without insulin, the improvement in HbA1c was only significant in insulin-treated patients and not in noninsulin-treated patients.
The most probable reason for the lack of superiority to SMBG in noninsulin-treated patients is that although the frequency of SMBG increased in the intervention group, treatment adjustments were not made quickly by the patients themselves. Thus, a close “SMBG-report-manage-feedback” loop between patients and physicians was not formed. This means patients need to record their BG test results and related activities (SMBG) and then report them to their physicians (report) to support the prescription (management). Physicians could adjust treatment based on the BG results as well as suggest appropriate changes in lifestyle behaviors (feedback). Moreover, training for self-regulation of antidiabetic drugs plays an important role in glycemic control whether conducting SMBG or not.
As our study showed, both the intervention and control groups experienced a significant HbA1c reduction after 6 months. Consistent with previous studies, 13,14 our results also indicate that a structured SMBG regimen may have contributed to further improvement in glycemic control in patients with poorly controlled diabetes. Recently in China, limited by outpatient admission capability and patient flow, physicians seemingly always have insufficient time to provide effective patient education. To help Chinese patients better implement individual disease management strategies, the first step is to provide a better educational session.
The average frequency of SMBG in the intervention group, among those with and without insulin treatment, was once daily. Compared with the recommendations in guidelines, 4 this number of measurements is still not satisfactory. The frequency of BG measurement in the COMPASS study also was increased from once to twice daily, 8 and the change in HbA1c from baseline to the end of the COMPASS study was a decrease by 1.8% ± 1.9%. 9
In addition, the structured SMBG regimen consisted of SMBG and self-adjustment of insulin doses, which was supported by educational and behavioral interventions for glycemic control in the COMPASS study. Previous studies have provided evidence for the effectiveness of self-regulatory strategies in glycemic control. Our findings indicate that diabetes education by our healthcare providers would translate the monitoring results to the practical adjustment for treatment and thus an improvement in HbA1c level.
Effects of structured SMBG on QoL
Some studies have reported that in T2DM patients not receiving insulin treatment, structured SMBG was not associated with deterioration of QoL, 15 whereas others have showed that in insulin-treated T2DM outpatients, a structured SMBG program significantly improved QoL outcomes. 8 These results are strongly influenced by demographics and diabetes-related variables such as total glucose measurements, age, gender, duration of diabetes, and economic factors.
Until now, worldwide studies have not achieved consensus on a clear recommendation for SMBG in diabetes patients. 15,16 The COMPASS study only showed the influence of structured SMBG in insulin-treated patients, and there are no data for Chinese diabetes patients to support the benefit of SMBG for the QoL of noninsulin-treated diabetes patients.
In the present study, we observed that patients' QoL was impacted by SMBG statement in the short term, but after regular BG measurements for 6 months, the impact was diminished. Patients were educated when they visited the physician, but during their daily life at home, the diabetes self-management support (DSMS) may not have been followed strictly, and thus, diet, physical activity, and medicine titration likely were not adjusted in a timely manner. Thus, their response was no improvement of the statement in general life, but still improvement of the complicated QoL. Integrated BG management is far more effective than structured SMBG only. Although an educational course provides better HbA1c control, strict follow-up and feedback between patients and physicians are definitely necessary. Our findings should be considered when tailoring educational support for SMBG for these patients.
Subgroup analysis according to age
Early intensive therapy shows a long-term benefit according to the UKPDS (United Kingdom Prospective Diabetes Study). 17 Upon linear regression analysis in our study, age had a negative correlation with the number of patients reaching their target HbA1c level. Indeed, better BG outcomes were found in younger patients (<66 years). Given that age is an important factor for patient outcomes, we divided patients by age and found a significant improvement in QoL for patients younger than 66 years of age, but not in the older patients. Consistently, in a previous study, diabetes-specific locus of control improvement with SMBG measurement was associated with younger age. 15
However, there has been no strong evidence to support the relationship between age and QoL in elderly patients. This outcome indicates that it is necessary to initiate structured SMBG as early as possible. Otherwise, when using structured SMBG in elderly patients, a stricter integrated education and support system should be provided. The results were similar for glucose monitoring when we divided patients according to age younger than 66 years versus age older than 66 years. Patients in the younger group showed better HbA1c control after 6 months of intervention in the structured SMBG group. Moreover, independent of insulin treatment, there was no improvement in HbA1c control in the elderly group. The underlying benefits to glycemic control and QoL resulting from early initiated, structured SMBG are confirmed by these findings.
There are still some limitations in this trial. First, we did not collect the information about the patients' educational background, thus, being not able to adjust the impact of different educational levels in this trial. Second, in insulin-treated patients, we did not compare the insulin doses at baseline with those in the follow-up, which might not illustrate the efficacy of structured SMBG on insulin treatment clearly. Finally, why younger patients without insulin treatment could benefit from the structured SMBG could not be explained well by the evident theoretical basis. We need to further conduct another well-designed trial only focusing on patients without insulin treatment to support the results in this trial.
In conclusion, a structured SMBG regimen, combined with an educational course can benefit the patients on their glycemic control. Specifically, the benefit on the glycemic control is more evident with structured SMBG in patients with insulin treatment, as well as in young and middle-aged patients without insulin treatment. No strict deterioration of QoL is detected throughout the trial in the whole study population. Our findings indicate that in addition to the insulin-treated patients, young and middle-aged patients without insulin treatment should also be encouraged to devote more attention to the SMBG to reach the target of the glycemic control.
Footnotes
Acknowledgments
The authors are very grateful to all the staff for helping with the present study. They are grateful to all participants for their dedication in data collection and laboratory measurements. This work was funded by the Shanghai Municipal Education Commission–Gaofeng Clinical Medicine Grant Support (20161430), and the innovation foundation of translational medicine of the Shanghai Jiao Tong University School of Medicine, and Shanghai SJTUSM Biobank (15ZH4006).
Authors' Contributions
W.J. and J.Z. designed the study. F.G., Y.S., and Y.M. helped with the recruitment of the subjects. K.K., W.Z., F.L., and X.H. collected data. K.K. and W.Z. performed statistical analysis and wrote the article. J.Z., Y.B., and W.J. revised the article and contributed to discussion. K.K. and W.Z. had equal contribution to this article and were the guarantors.
Author Disclosure Statement
No competing financial interests exist.