
Abstract
Background and Aims:
To evaluate the clinical accuracy of a flash glucose monitoring device FreeStyle Libre (FSL) among children with type 1 diabetes in real-world settings during a summer camp.
Materials and Methods:
During a summer camp, children with type 1 diabetes (n = 79, aged 8–18 years) were provided with FSLs for 12 days. On days 3, 7, and 11 of the study, they underwent supervised glucose testing at 8 timepoints. Glycemia was estimated by using FSL and measured with a personal glucometer within a period of 2 min. The glucose trend arrows were recorded.
Results:
The study was completed by 78 children (median: age 12.8 years, diabetes duration 5.8 years, HbA1c 58.5 mmol/mol). Mean absolute relative difference (MARD) between the FSL and the glucometer was 13.5% ± 12.9%. FSL was the most accurate in stable glycemic conditions: MARD 11.4% ± 10.4%, less accurate when glycemia was falling >2 mg/(dL·min) [0.111 mmol/(L·min)—MARD 22.6% ± 18.6%; P < 0.001 vs. stable conditions] and when the device could not determine the glucose trends (16.5% ± 16.3%, P = 0.01 vs. stable conditions). The FSL demonstrated lower accuracy during the day than the night [MARD 14.9% ± 14% vs. 11.2% ± 10.6%, P < 0.0001]. Out of 1655 data pairs of glucometer and FSL, using the Surveillance Error Grid methodology we determined that 80.36% of FSL readings were associated with no clinical risk, 18.73% with slight risk and only one high-risk measurement was detected.
Conclusion:
FSL is accurate in children, but its accuracy depends on the glucose trend. Results flagged by the rapid fall flag and “trend undetermined” should be verified by blood glucose measurements.
Introduction
T
Maintaining a high frequency of self-monitoring of blood glucose (SMBG) is the cornerstone for meeting HbA1c goals and preventing serious hypoglycemia. 4 An increased number of tests is also associated with significantly lower rates of diabetic ketoacidosis. 5 The guidelines of the American Diabetes Association have recently increased the recommended number of BG measurements, especially in patients with a short duration of diabetes or long life expectancy 6 who should perform SMBG tests 6 to 12 times daily. Such a number is, however, difficult to achieve, especially for children and young people, for whom the invasiveness of SMBG is a significant barrier for self-monitoring. 7
To improve this situation, other systems have been introduced to replace traditional capillary BG measurement. Continuous glucose monitoring (CGM) offers efficient glycemic control with a reduced need for manual tests and associated inconveniences. Recent studies have demonstrated that the use of CGM systems reduces glycemic variability and time spent in hypoglycemia of subjects with diabetes, and HbA1c, in well-controlled individuals and those using insulin pumps. 8 –12 A health-economic analysis by Roze et al. found that sensor-augmented pump therapy represents good value for money in terms of improving quality-adjusted life expectancy and delaying diabetes complications 13 ; however, the high cost of CGM still hinders its widespread use.
Recently, a new flash glucose monitoring (FGM) system (Abbott Diabetes Care, Alameda, CA) was introduced into the market along with a dedicated device: FreeStyle Libre (FSL). It offers a factory-calibrated sensor that can be worn for 14 days without manual calibration by using blood testing, a reader combined with a standard glucometer, and dedicated software. The user receives a current glucose measurement along with historic results from the preceding 8 h by scanning the sensor with the FreeStyle reader. Recordings are taken in 15-min intervals. The glucose trends are displayed as arrows on the reader along with alerts. As the device requires active scanning by the user, it does not report alerts in real time.
FSL was proposed as an alternative for those who cannot afford CGM, find CGM too complicated, or complain of alarm fatigue. Children and adolescents could clearly benefit from using the FGM system. 14 However, initial observations suggested that its users may forego SMBG measurements and rely solely on FGM. This raises the question—Is FGM accurate enough to replace standard glucometers, or should it be just a complementary addition to SMBG? So far, only one study tested the accuracy of FSL in a pediatric population, and the data obtained by FGM were hidden from participants. 14
This study examines the introduction of FSL to children with T1D in a real-world setting during a summer camp. During the study, the children could observe current glucose levels, trend arrows, and the 8-h glucose concentration history on a reader screen. The main aim of this study was to establish the accuracy of FSL FGM system in reference to the glucometer and pinpoint the factors that may affect said accuracy. The secondary objective was to assess the children's attitude toward the device and its possible association with measurement accuracy.
Materials and Methods
This was a prospective single-arm study conducted during an annual summer camp for children and adolescents with T1D. The study protocol was approved by the Ethical Committee of the Medical University of Lodz (No. RNN/223/16/KE) and registered in the German Clinical Trials Register (DRKS-ID: DRKS00011751). Informed written consent was obtained from parents, and so was informed assent from the children.
Children from 12 diabetes care centers from Poland took part in the camp, which took place in the period from July 24 to August 5, 2016. They were provided with full medical care and asked whether they would like to use FSL. Out of 80 approached children, 79 accepted the opportunity to participate in the study. One child did not complete the study. FSL readers and sensors were provided by Abbott Laboratories Poland LLC. On the second day of the camp, the children were introduced to the FGM system and the sensors were attached to the back of their upper arms, according to the manufacturer's instructions. In the case of the sensor dislodging or any technical issues, the sensors were replaced in each child up to two times.
The children had basic training in using FSL, limited to device handling and explanation of trends and alerts. On the seventh day, the authors collected feedback from children and created initial clinical guidelines for the interpretation of glucose trend arrows, which were subsequently taught to the children.
On the 3rd, 7th, and 11th days of FSL use, the children underwent supervised glucose testing at eight predefined time points each day: before and 2 h after breakfast, before and 2 h after their midday meal, before and 2 h after dinner, at midnight, and at 3 a.m. At each timepoint, glycemia was measured twice within 2 min: once in the interstitial fluid by scanning the FGM sensor, and again in the capillary blood by using a Contour Plus One glucometer (Ascensia Diabetes Care Poland, Warszawa, Poland), compliant with ISO 15197:2013 accuracy criteria. 15 The glucose trend arrows of the FGM were recorded. The sensors were removed on the 12th (last) day of the camp, and the skin was carefully examined by physicians. After sensor removal, data from the readers were downloaded and analyzed. Each reader was also reviewed manually.
Medical history was collected, and physical examination was performed by pediatricians. At the end of the camp, body height and weight were measured and capillary blood samples were taken for HbA1c assessment (D-10 Hemoglobin A1c Program [Bio-Rad Laboratories, Hercules, CA, Bio-Rad, Marnes-la-Coquette, France]). Body mass index (BMI) was recalculated into standard deviation Z-scores based on local BMI charts. 16
On the last day, a custom-designed questionnaire was administered to assess the degree of satisfaction with FGM use. The children rated their experience and satisfaction with FSL on a five-point scale from strongly agree to strongly disagree. The questionnaire included 13 closed questions regarding ease of using the device, pain when applying the sensor to the arm, the comfort of wearing the sensor, possible inconvenience, whether the sensor got in the way of daily activities, and the occurrence of pain or itching at the site of insertion.
The detailed questionnaire is included in the Supplementary Data (Supplementary Data are available online at
Statistical analysis
FSL readings were compared with glucometer readings as the reference method. FSL readings beyond the sensor value range (<40 mg/dL reported as LO (low) and >500 mg/dL reported as HI (high)) were included in the analysis as 40 and 500 mg/dL, respectively. These extreme readings, however, were excluded from the analysis of glycemia trends, as such recordings had no defined trend mark by default. The accuracy was assessed by calculating the mean absolute relative difference (MARD) for each patient by using the following equation: MARD = mean|[(glucometer−FreeStyle Libre)/glucometer) × 100%]|.
The Pearson's test was used to determine the correlation of the two methods, and the Bland–Altman regression was used to assess bias (mean difference was compared with 0 by using the t-test). The clinical accuracy of the readings was tested by constructing a Clarke Error Grid, a Consensus Error Grid, and a Surveillance Error Grid for paired FGM and glucometer measurements. 17 –19 To determine the impact of clinical variables, t-tests were used for two-group comparisons, one-way analysis of variance was used for multiple groups (with the post hoc Tukey's test performed for significant results), and the Spearman's rank correlation was used for continuous variables that were not distributed normally.
The questionnaire assessing satisfaction with FSL was assessed by contingency tables. The patients were divided into subgroups depending on the answers given in the questionnaire, and their FGM accuracies were compared between the groups by using the Kruskal–Wallis test.
Results
A total of 79 children agreed to use FSL for the duration of the summer camp; however, one girl returned home before study completion and was excluded from the analysis. The analyzed group, therefore, numbered 78 children (43% boys, 88.6% treated with CSII) with a median age of 12.8 years (interquartile range [IQR]: 11.6–14.7 years) and a median T1D duration of 5.8 years (IQR: 3.8–8.5 years). Their median HbA1c at inclusion was 7.5% (IQR: 7.0%–8.0%) or 58.5 mmol/mol (53–63.9 mmol/mol). The median standardized BMI in the group was 0.29 (IQR: −0.3 to 0.89), four children were overweight (BMI between 90th and 95th percentile standardized for gender and age), and two children were obese (>95th percentile).
During the summer camp, children wore the sensors for median time of 10.5 days (IQR 10 to complete 11 days) and 10 sensors were replaced in eight children due to detachment.
The analysis included 1655 paired sensor/glucometer readings (median 23 pairs/patient, IQR: 21–24). Due to the need for sensor replacement, it was not possible to collect all measurements scheduled for the 3rd, 7th, and 11th day of FGM. In total, 668 readings were collected from the first timepoint, 539 from the second, and 448 from the third. The glycemic variability in the participants over the camp duration is presented in Table 1.
FSL readings showed a strong positive correlation with glucose meter measurements (r = 0.95, P < 0.0001). However, the Bland–Altman regression (Fig. 1) showed that the mean difference (7.35 mg/dL, 0.4 mmol/L) was significantly different from the expected value of 0 (P < 0.0001), suggesting that FSL was biased toward an overestimation of glycemia. In line, raw differences related to glucometer reference measurements produced a mean relative difference of −4.42% with a high standard deviation (17.87%). The MARD between FSL and the glucometer was 13.5% ± 12.9%. The MARD for each patient ranged from 10.4% to 24.7%. The distribution of MARDs by individuals is presented in Figure 2. The accuracy of FGM did not differ between days of sensor use (P = 0.11) and was not associated with BMI Z-score (R = −0.11, P = 0.31) or HbA1c (R = 0.07, P = 0.55). However, a weak positive correlation was found between age and MARD (R = 0.25, P = 0.024), and the sensors worn by boys displayed a lower accuracy than those worn by girls—median MARD 14.8% (IQR: 12.4%–17.3%) versus 12% (9.9%–13.6%), P = 0.0001.
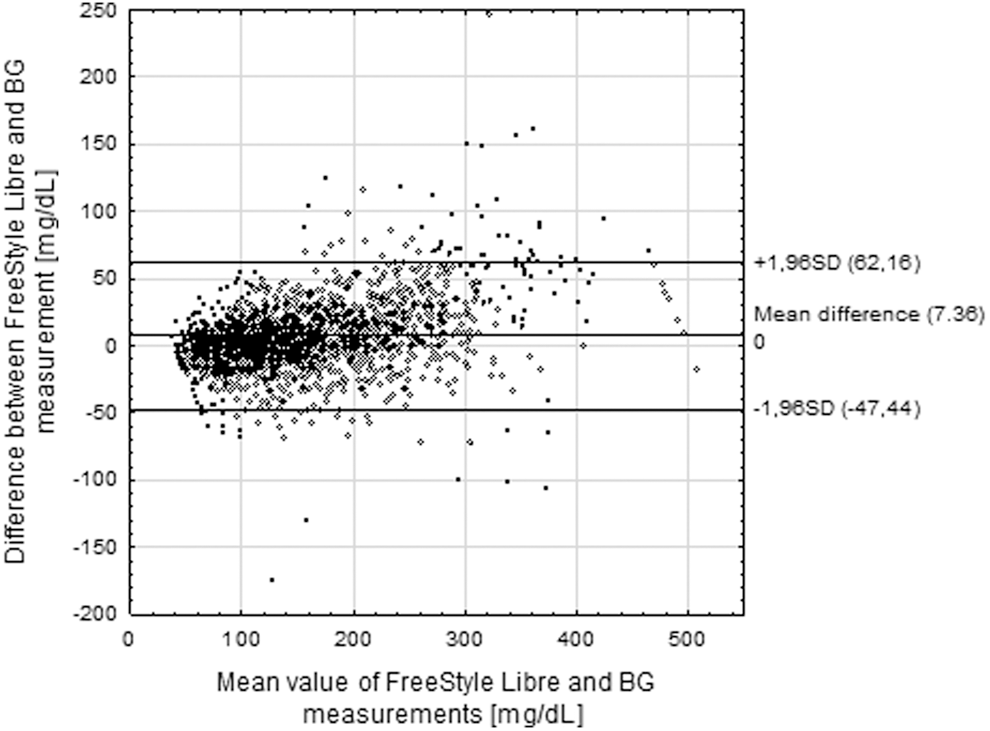
FreeStyle Libre measurements compared to BG with Bland–Altman regression plot. BG, blood glucose.
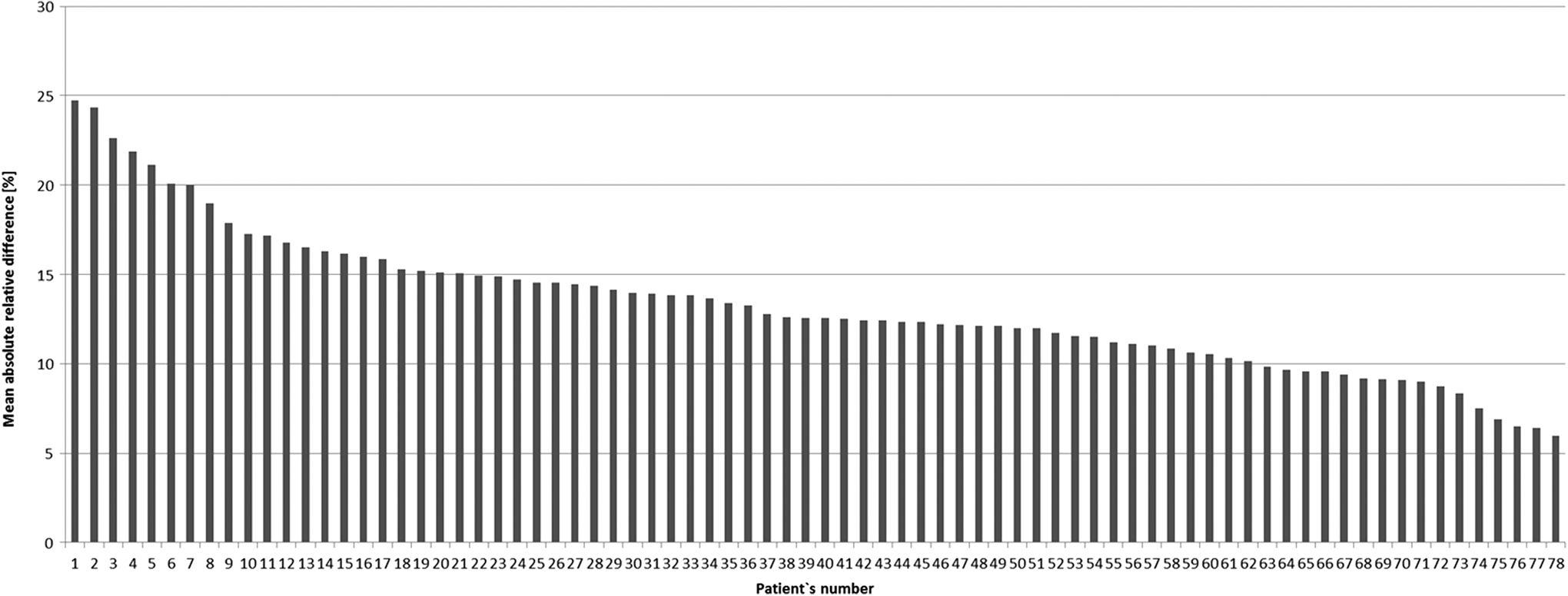
A bar graph of MARD values of individual patients. MARD, mean absolute relative difference.
In addition, the accuracy of FSL strongly depended on the current trend of glucose concentration (P < 0.0001) (Fig. 3). FSL measurements were the least accurate (MARD 22.6% ± 18.6%, mean relative difference −17.23% ± 23.73%) when glycemia was falling at a rate exceeding 2 mg/(dL·min) [0.111 mmol/(L·min)] compared with other trends (P < 0.0001). The greatest accuracy (MARD 11.4% ± 10.4%, mean relative difference −2.32% ± 15.3%) was achieved in stable conditions, when glycemia changes did not exceed 1 mg/(dL·min) [0.056 mmol/(L·min)] in either direction. Moreover, when the reading device could not determine the glucose trends and displayed no glucose trend arrow, the accuracy of FSL (MARD 16.5% ± 16.3%, mean relative difference −6.72% ± 22.28%) was significantly inferior to measurements performed in stable glycemic conditions (P = 0.001).
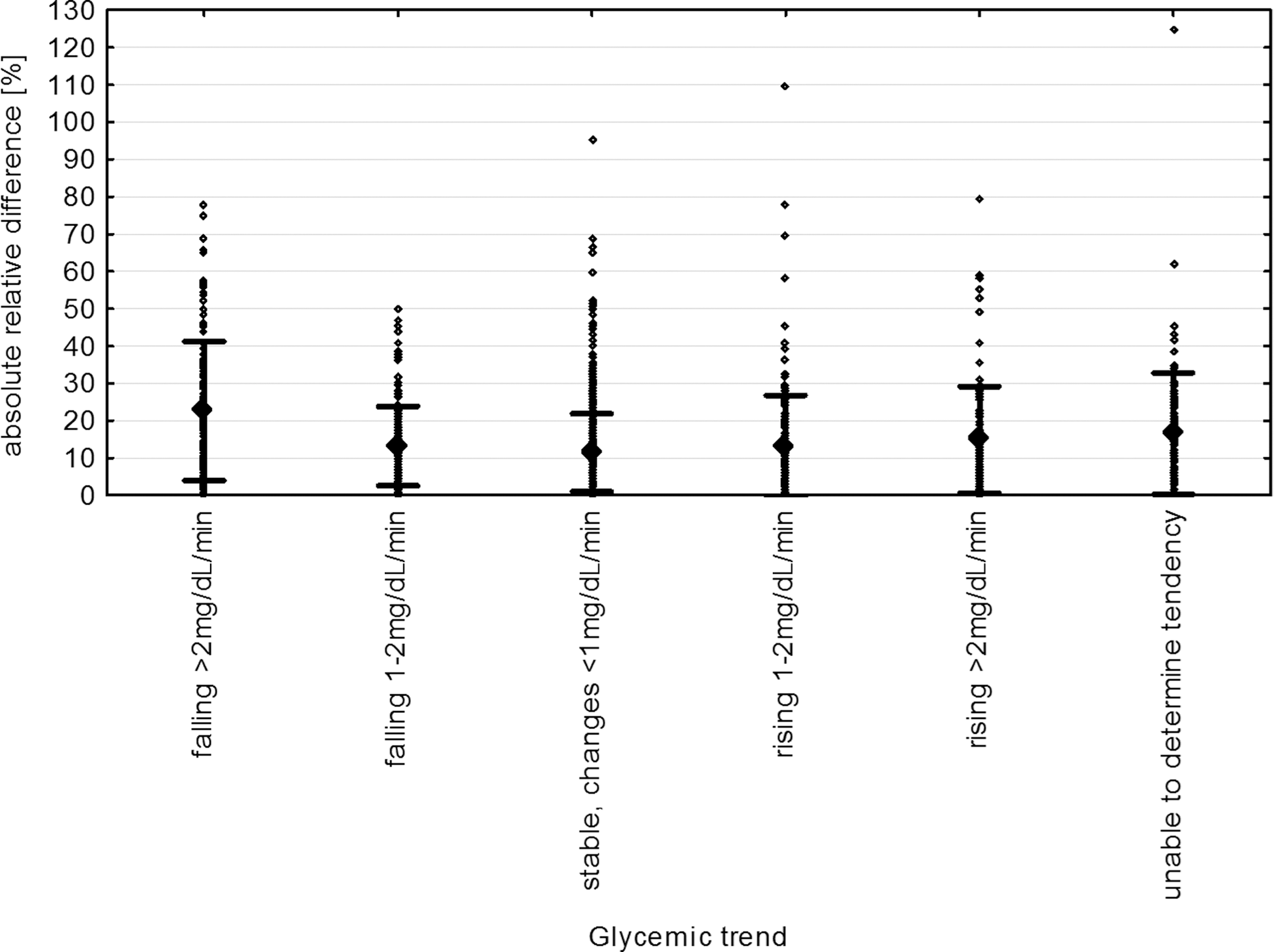
Accuracy of FreeStyle Libre in different glycemic conditions. The glycemic trends were determined by in-built software in the FreeStyle Libre reading device.
We detected a single extreme point in our data (absolute relative difference of 125%, no glucose trend arrow) that may have caused overestimation of the disparity between “unable to determine tendency” and “stable glycemic conditions.” Therefore, we removed this outlier and repeated the ANOVA analysis, which yielded significant results similar to the original ones (data not shown).
Further, daytime measurements taken by FSL were found to be less accurate than those taken at nighttime (i.e., midnight, 3 a.m. and after waking up) [MARD 14.9% ± 14% vs. 11.2% ± 10.6%, P < 0.0001].
Out of 1655 data pairs, 98.43% satisfied the clinical accuracy criteria (class A or B) of the Clarke Error Grid (Fig. 4a and Table 2) and 99.1% satisfied that of the Consensus Error Grid (Fig. 4b and Table 2). The Surveillance Error Grid (Fig. 4c and Table 3) labeled 1330 measurements (80.36%) as associated with no risk and 310 (18.73%) as associated with slight risk. The distribution of records in different classes of the Consensus Error Grid was similar among the patients (Supplementary Figure S1).
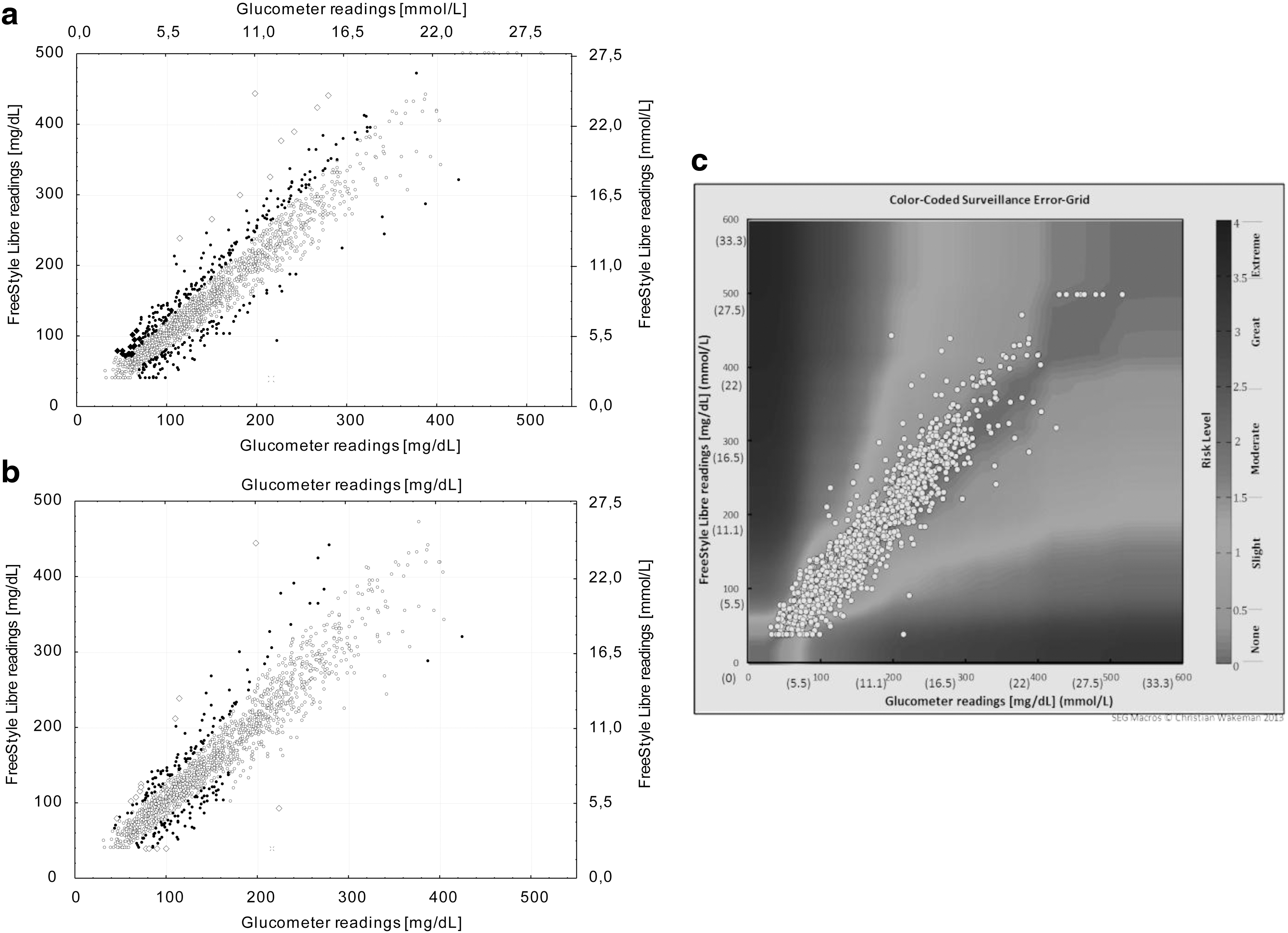
Error Grid Analysis of FreeStyle Libre results plotted against BG concentrations with:
No serious adverse effects were found to be associated with FSL sensor use during the study. In two boys, edema and rash were observed after sensor removal. During the camp, none of the children reported feeling pain or itching. However, in the retrospective questionnaire, 4 reported pain on sensor insertion, 13 reported itching, and 2 reported moderate pain during sensor use.
Sixty-eight (87.2%) children expressed a willingness to continue FGM use (see Supplementary Figure S2). In the open question regarding the advantages and disadvantages of the device, most of the participants regarded the discretion and painlessness of measurements as key advantages, and its inaccuracy, as perceived by the children, as a disadvantage.
Interestingly, sensor accuracy was not clearly associated with the accuracy of FSL, as perceived by children (P = 0.72), their trust in the sensor readings (P = 0.33), or their willingness to continue using FSL (P = 0.52).
Discussion
The study examines the utility of FSL in children and adolescents with T1D during a summer camp. FSL readings were found to correlate closely with BG measurements. So far, only three studies have analyzed the accuracy of FSL in real-life conditions. In adults, Bailey et al. observed MARDs as high as 12% in reference to a glucometer and 12.1% in reference to venous glycemia measured with YSI. 20 Similarly, Ji et al. reported MARDs of 10% in reference to BG measurements and of 10.7% in reference to venous measurements. 21 Edge et al. reported a slightly higher MARD in children (13.9%), which corresponds well with our findings. 14
We were also the first to evaluate FGM readings systematically with the Bland–Altman analysis, in which FSL demonstrated a fixed tendency to overestimate glucometer-measured glycemia. This bias was small (mean 7.35 mg/dL, 0.4 mmol/L) and negligible in most clinical situations, but on very rare occasions it may lead to the wrong clinical decisions. For this reason, all collected data pairs were assessed against published error grid scores 17,18 : the Clark, Consensus, and Surveillance Error grids. The most recently developed grid is the Surveillance Error Grid, which was developed in 2014. It was constructed by using feedback from medical professionals who represent a modern approach to diabetes care, based on DCCT study results and incorporation of technological advances such as insulin pumps into therapy.
Our study demonstrated that most FSL readings were localized in zone A or B of the error grids for more than 98% of cases, which means that they would not impact clinical decisions in a severe manner. Other studies have reported similar values regarding grid-assessed clinical accuracy for FGM versus glucometer in adult 20,21 and pediatric populations. 14 A single incidence of significant disparity was found between an FSL reading (<40 mg/dL, <2.2 mmol/L, reported as LO) and BG measurement (215 mg/dL, 11.9 mmol/L), which could be associated with potential clinically important consequences (class E by both Clark and Consensus Error Grid). This record was associated with sensor failure.
FGM accuracy did not correlate with the patients' BMI or HbA1c, which was in line with results reported by Bailey and by Edge. 20 However, in our study, MARD values were influenced by sex and age: The accuracy was a little worse in the boys. This may be associated with the higher physical activity demonstrated by the boys during the summer camp; however, as no objective measure of physical activity was included in our study group, this is impossible to confirm.
FSL accuracy was also found to be associated with the current glycemia trend: When glucose was falling rapidly, the FSL reading differed by up to 20% from BG measurements. This corresponds with results of Bonora et al., who report a significant increase in the MARD between FGM and CGM during hypoglycemic conditions. 22 Moreover, when glycemia was falling by more than 2 mg/(dL·min) [0.111 mmol/(L·min)], the mean difference reached −20 mg/dL (−1.1 mmol/L), which caused the FGM unit to overestimate the true current glycemia value. This discrepancy may have been caused by the lag time known to exist between glucose concentrations in the interstitial fluid reaching those in the blood. 20 This phenomenon was first described by Aussedat et al. 23 in rats and has become one of the focal points in theorycrafting of artificial pancreas. It complicates the interpretation of glucose concentrations measured in the interstitial fluid as the delay must be accounted for in closed-loop algorithms and by users of FGM and CGM devices who want to make therapeutic decisions.
Importantly, the lag is unfortunately no constant difference but its magnitude, direction, and dynamics may change, depending on glucose uptake, utilization, and elimination in peripheral tissues. 24 In humans, physiological lag between venous and interstitial glycemia was measured to be around 6 to 10 min in adults without 25 and with type 1 diabetes. 26 So far, no study has investigated the physiology of the glycemic lag in children. The tendency of FGM to overestimate falling glycemia fits well with the “push and pull” hypothesis formulated by Aussedat et al. 23 and their observation that during insulin-driven hypoglycemia the interstitial glucose concentrations fall slower than intravenous ones.
Moreover, FSL demonstrated significantly lower accuracy (compared with stable conditions), when the reading device could not determine the glycemic trend. This and the rapid decline scenario are, therefore, indicators for the patient to verify the result with capillary glucose measurement by using a glucometer. These results are in contrast to those reported by Edge et al., 14 who report a steady relative difference of 6%–7% between FSL readings and BG under extreme glucose trends (rapidly falling and rapidly rising) but negligible differences between the two methods (around 1%) for other trends. However, their study examined children using FSL in home-based conditions, whereas this study evaluates children during a summer camp: Increased physical activity, irregular eating patterns, and other factors may have contributed to the differences between the reported results and the ones shown in our study. These conditions might make both studies incomparable in this regard.
In the studies regarding CGM, the main barriers to continue using them were unrealistic expectations of users and lack of proper education. 27 In our study, the children were asked to assess the usefulness of FSL. In general, children graded the 2-week-long experience with FSL positively. Most of the children expressed willingness to continue using this device. It is possible that the good reception of FGM may result from its minimal invasiveness, when compared with standard BG measurements, and added value in the form of easily interpretable glucose trend arrows.
As noted in other studies, no serious adverse effects were observed while using FSL. 14,20 Skin allergic reactions were only found in fewer than 3% of patients.
The limitation of our study is its short (12 days) duration. Studies with longer observation times are needed to evaluate whether FSL could provide lasting improvement in glycemic outcomes. Moreover, our results are limited by the high rate of sensor removal. More effective means are needed to safely fix the sensor in place for studies in children.
A minor limitation was also comparing FSL readings only with glucometer measurements. However, use of the laboratory reference method during the camp would demand drawing venous blood in a nonsterile environment and would create logistic problems with storage and transport of samples. Similarly, using the Hemocue system for reference was not possible in this study for a few reasons. First, although the Hemocue microcuvettes can be stored in room temperature, the measurements were often taken in the outdoor conditions in temperatures exceeding 25°C; the microcuvettes are highly moisture sensitive and could be easily damaged. Further, the sampling size needed for Hemocue is around 4 μL of blood.
We used the glucometer that required a considerably smaller volume of only 0.6 μL to prevent children's pain and discomfort and to ensure good compliance. Finally, the number of participants in our study would demand many Hemocue analyzers to be used at once to carry out the testing.
Finally, the comparison of FGM with reference laboratory methods has been already done by the producer and other researchers 14,20,21 —the added value of our study is that it provides an opportunity to analyze the accuracy from a user's point of view. The reference-related error was minimized by using the Contour Plus One glucometer (Bayer HealthCare LLC, Diabetes Care, Whippany, NJ) as a comparator: It has high accuracy with an MARD of below 10% in comparison with reference methods. 15 On the other hand, such a protocol provided great insight into FGM accuracy from the users' perspective, as most clinical decisions are based on SMBG performed with a glucometer.
Conclusions
Results showed that the FSL FGM device offers good accuracy in comparison to capillary BG in children and adolescents with T1DM. However, the performance of FGM is strongly affected by the glycemia change trend at the time of measurement. Therapeutic decisions should not be solely based on measurements flagged by a rapid change flag on the FGM: Such measurements should first be verified by using a BG measurement.
Footnotes
Acknowledgments
The authors would like to thank Prof. Boris P. Kovatchev, Prof. Marc D. Breton, Dr. David C. Klonoff, and Mr. Christian Wakeman, who provided the tool for calculating the Surveillance Grid Score risks, and the medical staff for collecting data during the summer camp. The authors would also like to thank the organizers of the camp, charity foundation “Diabeciaki” for the opportunity to carry out the study and for providing FSL sensors for children.
Author Disclosure Statement
All authors took part in the study. None of the authors have any competing financial interests with the content of the study. The FSL sensors were provided by the producer to the camp organizers (charity foundation “Diabeciaki”), but Abbott Laboratories Poland had no involvement in the study design and course. A.S. reports being a speaker for Abbott Laboratories Poland and Bayer. A.G. reports being a speaker for Abbott Laboratories Poland and Bayer. A.M., D.Z.-Z., W.F., and W.M. report no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.