
Abstract
Background:
Type 1 diabetic patients have high instability of daily glucose levels. The aim of this study was to evaluate the long-term effects of continuous subcutaneous insulin infusion (CSII) therapy, compared with multiple daily injections of insulin (MDI), on glucose variability, in young type 1 diabetic patients transitioned to the adult diabetes care.
Methods:
Patients aged 18–30 years and considered eligible for insulin pump therapy were included in the study. Ninety-eight patients who started CSII therapy and 125 who remained in MDI completed a 2-year follow-up. Glucose variability was assessed with continuous glucose monitoring using blood glucose standard deviation (BGSD), mean amplitude of glycemic excursion (MAGE), continuous overall net glycemic action (CONGA-2 h), low blood glucose index, high blood glucose index, and average daily risk range.
Results:
MAGE and BGSD decreased in both groups, with adjusted differences at 2 years of −0.74 mM (95% confidence interval [CI] −1.22 to −0.26, P = 0.003) and −0.3 (CI −0.52 to −0.1, P = 0.005) favoring the pump-therapy group. No significant differences between groups in the other variability indexes were observed. HbA1c decreased in both groups without significant difference (0.05%, −0.26, 0.35, P = 0.77); fasting glucose, insulin dose, and overall hypoglycemia (daily, nocturnal, and severe) decreased more in patients with CSII, compared with those with MDI.
Conclusions:
Among young adults with type 1 diabetes transitioning from the pediatric care, the use of CSII is associated with lower glucose variability, fasting glycemia, and overall hypoglycemic events than MDI during a 2-year period of follow-up.
Introduction
E
Intensive insulin therapy, including multiple daily injections of insulin (MDI, up to four or more injections per day) or continuous subcutaneous insulin infusion (CSII or insulin pump), is the recommended treatment regimen to lower HbA1c levels and prevent microvascular complications in type 1 diabetes. 10,11 There is some evidence from short-term randomized trials (RCTs) 12 –14 and case–control 15,16 or observational 17 studies that CSII therapy is associated with reduced glucose variability in type 1 diabetes, although other studies 18,19 did not find any effect. However, no prospective study specifically investigated the long-term effect of intensive glucose control (IGC) on glucose variability in young type 1 diabetic patients transitioning from the pediatric clinic to the adult healthcare.
The aim of the present study was to evaluate the long-term effects of CSII, compared with MDI, on glucose variability, assessed with continuous glucose monitoring (CGM), in a population of young adults with type 1 diabetes with suboptimal glycemic control. To this purpose, we used data of the Management and Technology for Transition (METRO) study, a longitudinal observational study of type 1 diabetic patients in transition from the pediatric clinic to the adult diabetes care center. In accordance with the ADA recommendations for transition from pediatric to adult diabetes care systems, 20 we focused on the age range of 18–30 years.
Subjects and Methods
Study design and participants
The METRO study is a single-center, observational prospective study designed to evaluate the effects of CSII versus MDI on glycemic and metabolic outcomes in young adults with type 1 diabetes in transition from the Pediatric Clinic to the Diabetes Unit at the Teaching Hospital of University of Campania “Luigi Vanvitelli” (Naples, Italy). The study was approved by the local ethics committee, and all participants signed an informed consent before enrollment. The protocol of the study has been described elsewhere. 21,22 Briefly, patients aged 18–30 years, with type 1 diabetes for at least 12 months and previously treated with MDI, were recruited from March 2012 to March 2015 and followed over time. Participants were excluded if they were pregnant or planning to become pregnant in the next 2 years, were not able to use the study devices, used therapeutic CGM or needed retrospective CGM outside the planned study visits, had history of severe chronic diseases, or drug or alcohol abuse. Patients were considered eligible for CSII if they showed persistent HbA1c levels ≥7.5% (58 mmol/mol) despite optimized education therapy, recurrent severe hypoglycemic episodes or high glucose variability, and the willingness to wear the insulin pump. Patients eligible for CSII therapy who preferred to remain on MDI therapy were selected as control group.
All participants in the study used blood glucose meters and test strips and were asked to perform self-monitored plasma glucose measurements four times daily (bedtime and pre-prandial). Moreover, they were instructed to the correct use of the insulin devices (insulin pump or prefilled pen) and trained to carbohydrate counting, insulin dose adjustment, and management of hyper- and hypoglycemic episodes. All patients starting CSII therapy received a rapid acting insulin analog (lispro, aspart, or glulisine) through a multiprogrammable insulin infusion pump, whereas patients of MDI group were treated with three injections of a rapid acting insulin analog at meals and one injection of insulin glargine or degludec, usually at bedtime.
Participants of both groups (CSII and MDI) had regular follow-up visits at the Diabetes Center, each 2 weeks for the first month and each 12–16 weeks for the following period. All participants in the study were followed for 2 years; data on fasting glucose, HbA1c, insulin dose, weight, and mean amplitude of glycemic excursion (MAGE) were collected at 6, 12, and 24 months, and the other outcome measures at baseline and after 2 years.
Assessment of glucose variability
Participants of both groups underwent blinded CGM for 14 days at basal evaluation, and before the study visits at 6, 12, and 24 months. Patients used the Dexcom G4 CGM system (Dexcom, Inc., San Diego, CA) composed of a 7-day transcutaneous sensor, a transmitter, and a receiver. The sensor was implanted in the anterior abdominal wall. All patients were instructed to change the sensor every 7 days; moreover they were asked to perform the required sensor calibration procedure according to the manufacturer's instruction within 2 h from placing the sensor and then each 12 h. Glucose data have been downloaded with Dexcom STUDIO. Glycemic readings from CGM were entered in the EasyGV© software (
Study measurement
A complete medical history, including smoking status and concomitant pathologies, was obtained by patients' interview or clinical chart review. Hypoglycemia was defined as symptoms or signs associated with hypoglycemia experienced by the patient and self-treated, or the glucose level reduction below 70 mg/dL (3.9 mM), whereas severe hypoglycemic episodes referred to an episode requiring assistance of another person for its resolution. 24 Daily and nocturnal hypoglycemia were defined as hypoglycemic events occurring between 7.01–23.00 and 23.01–7.00, respectively. Both daily and nocturnal hypoglycemic events were extracted from the glucose readings collected with CGM. Severe hypoglycemic episodes were collected from participants if reported at study visits. Height and weight were recorded with participants wearing lightweight clothing and no shoes using a Seca 200 scale (Seca, Hamburg, Germany) with attached stadiometer. Body mass index (BMI) was calculated as weight in kg divided by the square of height in meters (kg/m2). Total insulin dose was recorded at each study visit and expressed as units per kilograms of body weight. Arterial blood pressure was measured thrice, at the end of the physical examination with the subjects in sitting position, after a 15 min rest. Patients whose average blood pressure levels were greater or equal to 140/90 mmHg or who were under medication were classified as hypertensive. Eye complications were defined as the presence of any grade of diabetic retinopathy or maculopathy on dilated eye examination. Renal complications included micro- or macroalbuminuria. Diabetic neuropathy was assessed according to the recent American Diabetes Association guidelines for somatic and autonomic neuropathy. 25
Fasting plasma glucose, total and high density lipoprotein cholesterol, triglycerides, and HbA1c were measured at the hospital's chemistry laboratory.
Diabetes treatment satisfaction
The validated Italian version of the Diabetes Treatment Satisfaction Questionnaire (DTSQ) was administered at the beginning of the study and at the end of the 2-year follow-up. 26 This instrument evaluates changes in patients' satisfaction related to therapy modifications, but is also useful for comparing levels of satisfaction in subjects using different treatment strategies. The questionnaire consisted of eight questions: six questions were grouped in a total score addressing general satisfaction with a score from 0 to 6 for each question (0 = worst); one concerned the perception of hyperglycemia and another the perception of hypoglycemia, both with a score from 0 (none of the time) to 6 (most of the time).
Statistical analysis
The primary end point was blood glucose variability, measured as change in MAGE. Secondary end points were changes in HbA1c levels, fasting glucose concentrations, number and severity of hypoglycemia, total insulin dose, body weight, lipid profile, blood pressure, and diabetes treatment satisfaction. Continuous variables were reported as mean and standard deviation (SD) or median and interquartile range (IQR) according to distribution and compared with unpaired Student's t-test or Wilcoxon rank-sum test as appropriate. Categorical variables were reported as absolute number and percentages and compared with chi-square test or Fisher exact test when appropriate. Difference between the two treatment regimens (MDI vs. CSII) was estimated using propensity scores to adjust for the bias inherent to the different characteristics of patients. The propensity scores were estimated by fitting a logistic regression model with intensive insulin regimen (CSII or MDI) as dependent variable. The covariates included in the propensity score models were age, sex, diabetes duration, BMI, fasting glucose, glycated hemoglobin, insulin units, MAGE, total cholesterol, and systolic blood pressure at basal level. Repeated measure ANOVA analyses were performed for each variable, including as covariates propensity score as continuous variable, type of treatment regimen, the time points of observations (Time: 0, 6, 12, and 24 months), and their interaction. Adjusted differences (and 95% confidence interval) between the two treatment regimens at 2 years were estimated from these analyses. The same model was used for the other measures of variability. A sensitivity analysis was performed, including quintile categories of propensity score as covariates, instead of the linear term. A two-tailed P-value <0.05 was considered significant. Data were analyzed using STATA software version 14.0.
Results
Four hundred and fifty-two type 1 diabetic patients transitioning from the pediatric clinic to our Diabetes Unit were initially examined for eligibility for CSII therapy. Among the 252 eligible patients, 123 started CSII therapy, and the remaining 164 chose to continue MDI. A total of 223 patients completed the 2-year follow-up (125 patients in the MDI group and 98 patients in the CSII group) (Fig. 1). Mean age was 24.8 years, and mean diabetes duration was 13.9 years. Mean baseline HbA1c level was 8.5% (69 mmol/mol). Table 1 shows the baseline demographics and characteristics of the study population according to the treatment regimen. The two groups were well matched for demographic and clinical characteristics. A similar percentage of patients in both groups had microvascular complications or concomitant autoimmune diseases. The frequency of the overall hypoglycemic events (daily, nocturnal, and severe) was also similar in both groups.
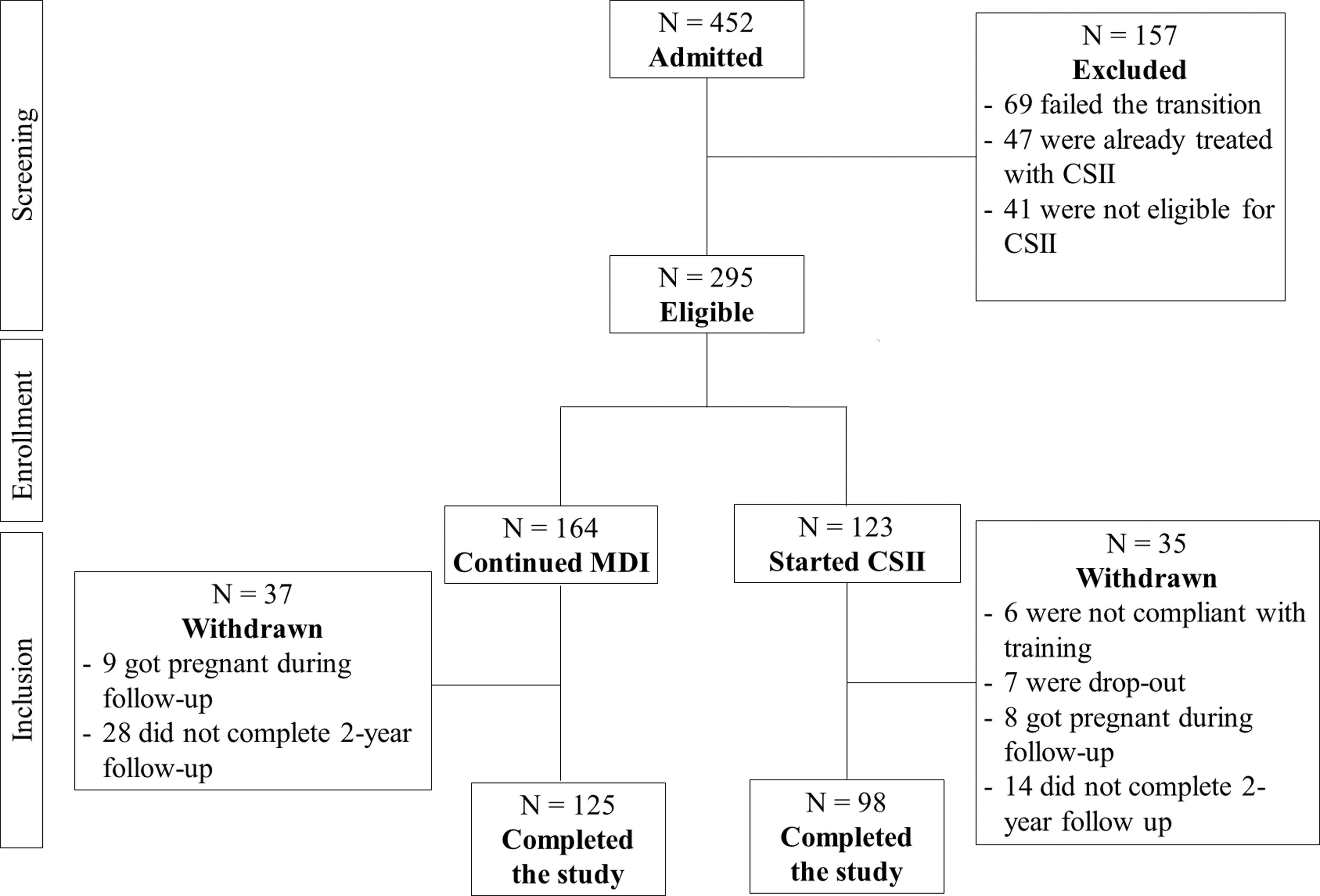
Process of patients selection. CSII, continuous subcutaneous insulin infusion; MDI, multiple daily injections of insulin.
Values are expressed as mean ± standard deviation (SD) or median (interquartile range).
MDI, multiple daily injections of insulin; CSII, continuous subcutaneous insulin infusion; BMI, body mass index; MAGE, mean amplitude of glycemic excursion; CONGA-2 h, continuous overall net glycemic action; BGSD, blood glucose standard deviation; HBGI, high blood glucose index; LBGI, low blood glucose index; ADRR, average daily risk range; SBP, systolic blood pressure; DBP, diastolic blood pressure; DTSQ, diabetes treatment satisfaction questionnaire.
Primary end point
Among patients treated with CSII, MAGE fell from baseline to 6 months and remained steady for the remainder of the study with significant differences compared with patients on MDI (Fig. 2). This change was significant between the two groups even after adjustment with the propensity score for the interaction treatment/time (Table 2). Table 3 summarizes the results at the end of the follow-up. After 2 years, both MAGE and BGSD decreased to 5.7 and 3.2 mM, respectively, in the CSII group, compared with 6.3 and 3.5 mM in the MDI group; the between-group adjusted differences favored the pump-therapy group by −0.74 mM (95% CI, −1.22 to −0.26, P < 0.01) and −0.3 (−0.52 to −0.1, P < 0.01), respectively. CONGA, HBGI, LBGI, and ADRR decreased in both CSII and MDI groups, without any significant difference between them.
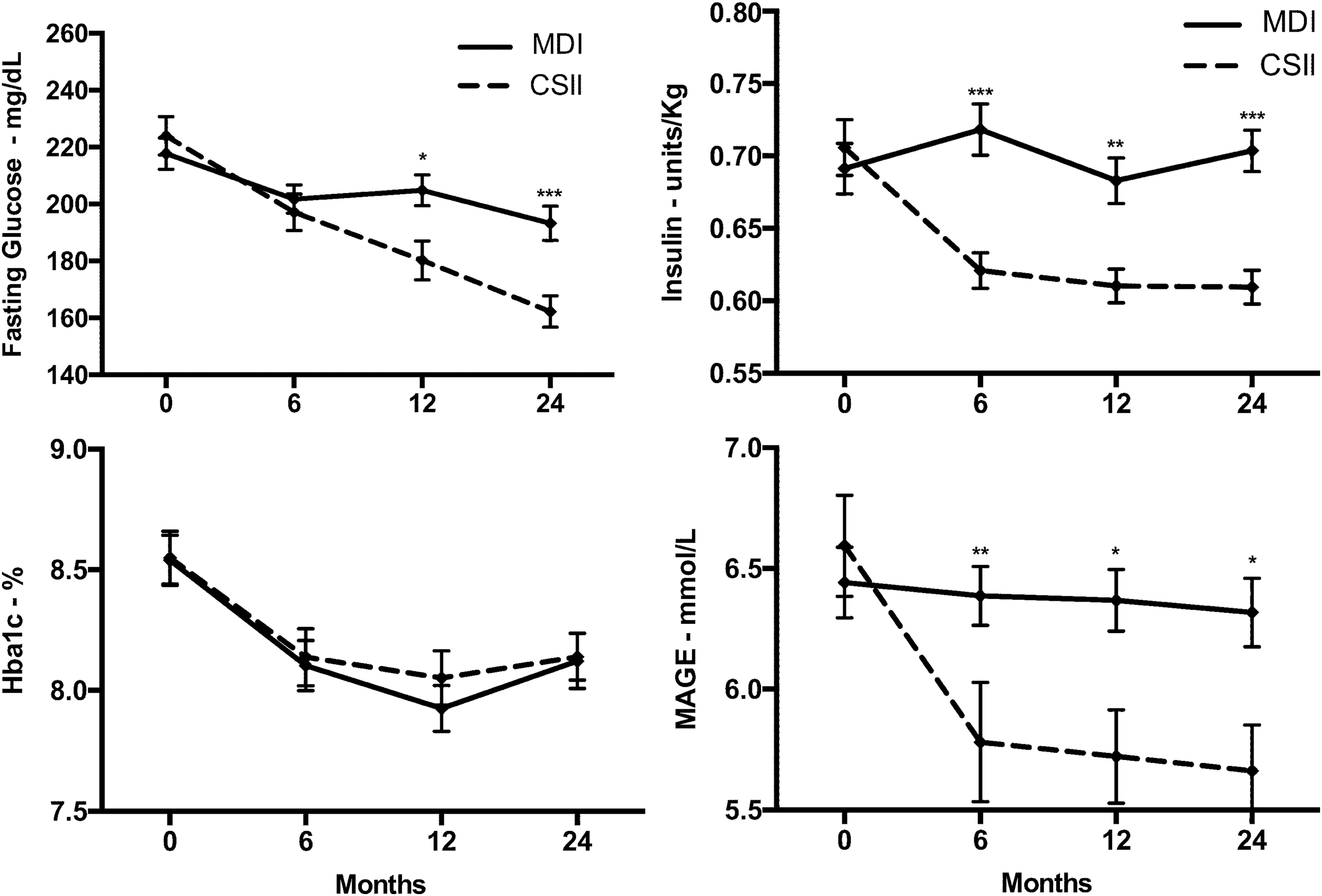
HbA1c levels, MAGE, fasting glucose, and insulin dose at 6, 12, and 24 months in all the study patients according to insulin regimen. Values are mean ± SE. Asterisks denote significant differences for all comparisons between pump therapy and injection therapy at each time point. * P < 0.05; **P < 0.01; ***P < 0.001. MAGE, mean amplitude of glycemic excursion.
Difference between groups adjusted with the propensity score.
For definition of abbreviations, refer to Table 1 footnotes.
Secondary end points
HbA1c decreased by
Table 4 describes the frequency of hypoglycemic events in the two groups at baseline and after 2 years. The proportion of patients with one or more daily hypoglycemic events decreased more in the CSII group and remained unchanged in the MDI group (P < 0.01). Moreover, the percentage of patients with one or more episode of nocturnal hypoglycemia decreased in the CSII group and increased in the MDI group (P < 0.01). Similar results were obtained when comparing the proportion of patients with one up to six nocturnal hypoglycemic episodes between groups (Table 5). The proportion of patients experiencing one or more episodes of severe hypoglycemia decreased in both groups; in both cases the difference at 2 years favored patients in the CSII group (P < 0.05).
In the first column, 0–5 (at baseline) and 0–6 (at 2 years) indicate the number of nocturnal hypoglycemic events. The number and the percentage of patients in both MDI and CSII group experiencing a certain number of nocturnal hypoglycemia are reported in the second and in the third column, respectively.
Discussion
Among young adults with type 1 diabetes with suboptimal glycemic control in transition from the pediatric clinic, the use of insulin pump, compared with multiple insulin injections, resulted in a greater decrease in glucose variability, fasting glucose, and insulin dose, but in similar reduction of HbA1c levels, during a 2-year follow-up period; moreover, CSII was better in decreasing overall hypoglycemia (daily, nocturnal and severe) and improving the rate of perceived hypoglycemia. Although previous studies have demonstrated benefits of insulin pump therapy on glucose variability in patients with type 1 diabetes, 12 –17 no study evaluated young adults over a long follow-up period using CGM to determine glucose variability indexes. CGM may be considered the best instrument for the evaluation of glycemic fluctuation in diabetes, given the very high number of determinations necessary to evaluate the parameters such as BGSD, MAGE, and CONGA. A sustained reduction in MAGE and BGSD over the other indexes of glucose variability occurred in patients treated with CSII but not in those with MDI and translated in less glucose fluctuations and more homogeneous glycemic levels. Interestingly, compared with patients on MDI, patients in the CSII group showed a greater decrease in fasting glucose and overall hypoglycemia, which could have contributed to the reduction of glycemic fluctuations.
The role of glucose variability in the development of diabetes complications is still debated. A positive association between glucose variability and diabetes-related complications has been reported in type 2 diabetes, although this evidence mostly comes from retrospective studies. 27 In contrast, there is still a contradictory evidence about the role of glucose variability in vascular complications of type 1 diabetes. Data from the Diabetes Control and Complication Trial failed to demonstrate a role of the glycemic variability in the development of diabetic microvascular complications in the long term. 28,29 The use of the 7-point glucose profile to determine the measures of glucose variability remains the main limitation of these studies, as it fails to capture the full degree of glycemic fluctuations as the CGM can capture. Despite this, in vitro studies 30,31 showed a more detrimental effect of glucose fluctuations than persistent hyperglycemia on endothelial function, mainly due to the generation of oxidative stress, which has been suggested as the key link between hyperglycemia and diabetic complications.
We found a similar reduction in HbA1c levels in both CSII and MDI groups. Our findings are novel, given the lack of long-term studies comparing the effects of insulin pump or multiple injections on glycemic outcomes in transition-age youth with type 1 diabetes. A 2-year RCT of 267 adults with type 1 diabetes (mean age 41.5 years) assigned to CSII or MDI therapy reported a not significant mean difference of −0.24% (−0.53 to 0.05) in HbA1c levels favoring participants with insulin pump. 32 In contrast, two recent meta-analyses of RCTs concluded that use of insulin pump is more effective than MDI at decreasing HbA1c in adults with type 1 diabetes. 33,34 Moreover, previous long-term (up to 5 years) observational studies of both children 35 and adults 36,37 with type 1 diabetes showed that CSII therapy, compared with MDI, may produce a significant decrease in HbA1c levels which declines over time. Obtaining a good level of glycemic control for the transition-age patients is difficult, as this represents a particularly vulnerable population of patients, subjected to the influence of the “metabolic memory”. 11 According to the American T1D Exchange registry, only the 14% of young adults aged 18–25 are currently achieving the ADA recommended target of HbA1c. 38
The prevention of severe hypoglycemia remains a challenge in the management of type 1 diabetic patients. The DCCT/EDIC study 39 showed that, after about 30-year follow-up, the rate of severe hypoglycemia was similar in both the intensive and conventional treatment groups, in association with advancing duration of diabetes and similar HbA1c levels. In our study, severe hypoglycemia decreased with both intensive insulin regimens, although the number of patients with more than one episode of hypoglycemia was smaller in the CSII group. Compared with patients of the DCCT/EDIC cohort, our population of young type 1 diabetic patients may reflect an earlier diabetes stage which can primarily take advantage of insulin pump to reduce the risk of severe hypoglycemia. A longer follow-up could clarify whether the rate of severe hypoglycemia will equilibrate over time.
In a shorter follow-up (3 months), young type 1 diabetic patients treated with CSII had a higher degree of satisfaction for treatment, compared with those treated with MDI. 22 With the longer follow-up (2 years), the overall DTSQ score was similar between patients treated with both IGC regimens, suggesting that the initial advantage obtained with CSII is lost over time. The situation may be different in adults with type 1 diabetes, as the largest case–control, cross-sectional study of 1341 adults with type 1 diabetes treatment with CSII was associated with a markedly higher DTSQ score compared with MDI. 40
Compared with young patients with MDI, those with CSII showed lower levels of fasting glycemia, associated with a significant reduction of insulin dose. This may have occurred because patients using MDI have less flexibility in adjusting their insulin basal delivery than pump users, who can modify the basal insulin rate in the different times of the day and night according to increasing or decreasing glucose concentrations or planned activities, including physical exercise. 41 Moreover, the higher rate of nocturnal hypoglycemic events occurring in patients with MDI, compared with those treated with CSII, may have contributed to increasing fasting glucose levels of patients using insulin injections, as a result of both a counter-regulatory response and corrections made by patients themselves.
Strengths of this study are the narrow age range of type 1 diabetic patients investigated (18–30 years), the largest sample so far investigated in this age range, the long-term follow-up, the contemporary evaluation of many indexes of glucose variability, and the use of a valid tool (CGM) to measure glucose fluctuations. This study also has limitations. First, the lack of randomization due to its observational nature may have introduced a selection bias. However, this study represents a real life experience, reflecting the indication by ADA and EASD Diabetes Technology Working group to an appropriate selection of candidates for pump therapy, which must have poor glycemic control and be willing and able to use the device. 42 Moreover, the use of the propensity score allowed to eliminate, at least in part, the allocation bias. The single-center nature of the study may be seen as another limitation due to the lack of generalizability of our findings. In contrast, homogeneity is much higher in single-center studies, compared with multicenter studies, as indicated by the lack of any differences in clinical and metabolic characteristics between the two groups at baseline.
In conclusion, in young adults with type 1 diabetes transitioning from the pediatric care, the use of CSII is associated with lower glucose variability, fasting glycemia, and overall hypoglycemic events than MDI during a 2-year period of follow-up. Our data support the use of CSII therapy as an appropriate treatment regimen to improve glycemic control in transition-age adults with type 1 diabetes, with the advantage of less glucose variability and hypoglycemia.
Footnotes
Acknowledgments
The authors thank all the members of the METRO study group, and specifically Dr. Filomena Castaldo, Dr. Maria Rosaria Improta, and Dr. Annalisa Sarnataro for the medical expertise; Dr. Mariangela Caputo for the dietetic educational support; and Sig. Concetta Verazzo for nursing assistance.
Author Disclosure Statement
No competing financial interests exist.