
Abstract
Background:
Young adults with type 1 diabetes (T1D) experience poor glycemic control, disengagement in care, and are often lost to the medical system well into their adult years. Diabetes providers need a new approach to working with the population. The goal of this study was to determine whether an innovative shared telemedicine appointment care model (CoYoT1 Clinic [pronounced as “coyote”; Colorado Young Adults with T1D]) for young adults with T1D improves care engagement, satisfaction, and adherence to American Diabetes Association (ADA) guidelines regarding appointment frequency.
Subjects and Methods:
CoYoT1 Clinic was designed to meet the diabetes care needs of young adults (18–25 years of age) with T1D through home telemedicine. Visits occurred every 3 months over the 1-year study (three times by home telemedicine and one time in-person). Outcomes were compared to patients receiving treatment as usual (control).
Results:
Compared with controls, CoYoT1 patients attended significantly more clinic visits (P < 0.0001) and increased their number of clinic visits from the year before the intervention. Seventy-four percent of CoYoT1 patients were seen four times over the 12-month study period, meeting ADA guidelines, but none in the control group met the ADA recommendation. CoYoT1 patients used diabetes technologies more frequently and reported greater satisfaction with care compared with controls.
Conclusions:
Delivering diabetes care by home telemedicine increases young adults' adherence to ADA guidelines and usage of diabetes technologies, and improves retention in care when compared to controls. Home telemedicine may keep young adults engaged in their diabetes care during this challenging transition period.
Introduction
I
Poor glycemic control in young adults may be exacerbated by psychosocial changes that occur during the transition from adolescence to adulthood. Academic pursuits, work commitments, social priorities, lack of adherence to strict routines, and reduction of diabetes-specific support pose serious threats to transitioning young adults' diabetes management. Young adults with diabetes struggle to address many self-care behaviors, including satisfying the ADA recommendation of completing ≥4 clinic visits annually and performing routine HbA1c tests. 6,7 In addition, as young adults, feelings of “invincibility” and fewer immediately life-threatening medical comorbidities often contribute to lower adherence to medication regimens, which may lead to higher risk of diabetic ketoacidosis, poor mental health, or multiple physiological complications in later adulthood (e.g., neuropathy, kidney disease, cardiovascular diseases, and eye disease). 8 –11
Existing T1D interventions do not address young adults with diabetes adequately, as they are often focused on the care needs of either pediatric or adult patients, or do not provide developmentally appropriate peer support or other means of engagement for young adults. 12 To improve health outcomes for young adult patients with T1D, interventions must focus on improving patient–provider communication and addressing young adult developmental needs. 13
Recent advances in health technologies have allowed care providers to address communication issues by using telemedicine to engage patients; replacing routine, in-person medical appointments with online video conferencing. Patients in telemedicine studies often report improved satisfaction with care and demonstrate better medical outcomes. 12,14 –19 In studies focused on T1D patients, those who utilized telemedicine maintained glycemic control more successfully and followed-up with care providers more efficiently than with routine in-person visits. 12,15,16,19
Telemedicine has been used successfully with pediatric and adolescent patients with T1D, but often in conjunction with another intervention addressing the psychosocial needs of this age group. 1,20 For example, Telehealth Behavioral Therapy (TBT) for T1D patients ages 9–17 years addresses how parental discord may influence adherence to diabetes regimens. 18 Similarly, Behavioral Family Systems Therapy for Diabetes (BFST-D) has been delivered using videoconferencing and was equally effective in providing diabetes team contact, peer support, and disease management as the in-person intervention. 14,17
In our previous work, we designed and evaluated a shared medical appointment (SMA) model called “Team Clinic,” which addresses the developmental and psychosocial needs of adolescent patients with T1D. 21 Team Clinic not only allowed providers to deliver care more efficiently and effectively but also increased patient satisfaction, comfort, and willingness to engage with care providers when compared to routine appointments. Pilot data from the Middle School Team Clinic cohort found high satisfaction in patients, families, and providers and a trend toward increased visit frequency and improved glycemic control when comparing patients in Team Clinic to controls (in press). Data from the High School Team Clinic pilot found increased satisfaction for patients, families, and staff while also meeting ADA recommendations for routine visits with all members of the diabetes team. 22 The Team Clinic model was also applied to young adults with diabetes. Although satisfaction and qualitative feedback was positive, regular attendance for in-person Team Clinic was poor in the young adult population (unpublished data).
Based on lessons learned from Team Clinic and the desire to find a way to connect with young adults, we developed an innovative care model called “CoYoT1 Clinic” (pronounced as “coyote”; Colorado Young Adults with T1D), that delivers supportive SMA care using telemedicine. 23,24 In the current study, we evaluated the feasibility and acceptability of CoYoT1 Clinic, examining rates of care retention and follow-up, patient satisfaction, and adherence to ADA guidelines regarding appointment frequency, compared to patients in usual care.
Methods
CoYoT1 Clinic
The CoYoT1 Clinic structure, a virtual adaptation of the Team Clinic model, consisted of individual appointments with a diabetes-focused pediatric endocrinologist or nurse practitioner, and group appointments with a certified diabetes educator or peer leader. 23,24 Participants completed these telemedicine appointments from any location of their choosing, using any Internet-connected device equipped with a camera and speakers (e.g., tablets, smartphones, personal computers) and Vidyo™ web-conferencing software (Vidyo, Inc., Hackensack, NJ), a HIPAA-compliant encrypted platform provided by Children's Hospital Colorado and the Barbara Davis Center for Diabetes (BDC), which allowed healthcare professionals to discuss private health information with patients securely. Before appointments, patients uploaded data from diabetes management devices (e.g., insulin pump, blood glucose monitors, continuous glucose monitors [CGM]) to a secure website, and completed laboratory studies (including HbA1c) at any convenient local care provider or laboratory (e.g., student health clinic, general physician's office, free-standing laboratory) who sent laboratory results to our office. Visits were scheduled every 3 months in compliance with ADA recommendations for patients with T1D.
Group sessions, routinely consisting of four patients each, focused on topics relevant to young adults with T1D, including stress management, building social support, developing self-advocacy and efficacy in diabetes and symptom management, and using diabetes technology to improve quality of life. Group sessions were completed with Visits 1, 2, and 4. A certified diabetes educator led Visits 1 and 2, and a peer leader working in our diabetes center, who was trained by the study team, led Visit 4. No group session was conducted during the in-person appointment (Visit 3).
Visit 1 included an orientation to the clinic process, participants shared their diabetes story, and patients reviewed self-advocacy and self-efficacy at work, school, and other social scenarios. Visit 2 focused on diabetes stress and burnout, including barriers to care and potential methods to address barriers. Visit 4 focused on diabetes technology and research, including patients reviewing what had worked or not worked for them. In each group, patients were encouraged to ask questions of one another versus the facilitator driving discussion. The goal was for patient-driven, topic-focused discussion to meet their needs while also setting sufficient structure for topic review.
During the individual appointment within the telehealth visit, care providers reviewed laboratory results, discussed blood sugars and insulin doses, considered barriers to an individual's diabetes management, addressed the young adult's questions and concerns, and worked with the patient to develop a care plan. Diabetes team members were also available by phone or email before and after scheduled appointments to answer additional questions. Further details and description of the CoYoT1 Clinic can be found in our previously published work. 23,24
Study participants and design
Patients with T1D at BDC between ages of 18 and 25 years were invited to participate in CoYoT1 Clinic. Patients were excluded from the study if they did not attend any clinics during the year before enrollment; if they did not have access to an Internet-connected device; if they were newly diagnosed patients, who had not yet completed the required diabetes education program; if they did not speak English; if they were not able to be within the State of Colorado at the time of their online appointments; or if they were diagnosed with severe behavioral or psychological disorders that would preclude effective group participation.
In this prospective cohort pilot study, patients self-selected into either the CoYoT1 Clinic arm, where patients could complete three telemedicine visits and one in-person appointment with their diabetes care provider; or to the control arm, where participants could continue routine in-person visits at BDC as per clinic standard. Details about study visits are shown in Figure 1. Recruitment occurred over ∼4 months, with lack of interest in the study and inability to be within the State of Colorado for appointments being cited as the main reasons for not participating. Patients in both groups received small monetary incentives for completion of questionnaires at baseline and study completion, but they did not receive compensation for visit completion.

Study visits for CoYoT1 and control patients. CoYoT1, Colorado Young Adults with T1D.
Patients in both CoYoT1 Clinic and standard care received appointment reminder phone calls before their appointments. Both groups received reminders 1 week before the appointment, but patients in CoYoT1 received additional reminders (1 week and 3 days before their appointment) to complete laboratory testing and diabetes device downloads in preparation for online clinic appointments. Diabetes device downloads include glucometers, insulin pumps, and CGM downloads. For patients in CoYoT1, device downloads were done at home and sent to the clinic electronically. For control patients in standard care, device downloads were either completed at clinic (requiring patients to take the device to an appointment) or were completed during another medical appointment around the scheduled date of clinic visits.
Patients in CoYoT1 were compared with control patients at 3-month intervals (at baseline, 3, 6, and 9 months). This appointment attendance schedule is consistent with the ADA's recommendation for young adults with T1D to be seen quarterly. 7 Adherence to ADA guidelines for visit frequency was established as quarterly appointments (≥4 visits over the 12-month time period). Similarly, adequate HbA1c monitoring was defined as completion of tests on a quarterly basis (≥4 values over the 12-month time period), and adequate blood glucose monitoring was defined as checking blood glucose levels by finger stick ≥4 times per day.
To increase opportunity for participation in the control arm, patients receiving routine care were given an extended time window (∼15 months) to increase visit completion during the study period. These patients were also allowed to submit device data outside of their scheduled clinic visits. All procedures were reviewed and approved by the Institutional Review Board of the University of Colorado Denver. Before participation in the study, all patients provided informed consent.
Patient satisfaction
Patient satisfaction with the group and individual appointments (online or in-person) was assessed using a brief online survey, which asked patients to rate how much they agreed or disagreed with statements about the appointments on a 5-point Likert scale (1 = Strongly Disagree to 5 = Strongly Agree). Five statements asked participants about how well the appointments worked for their schedules, as well as feeling supported and comfortable asking the doctor questions (e.g., “I was able to speak freely and express myself”). Some item wording varied between groups because of differences in appointment structure (e.g., “[Online appointments are] easier than normal …” vs. “[In-person appointments are] easy for me …”). After one reverse-scored item was recoded (“Appointments … take a lot of time …”), all scores ranged from 1 to 5, where higher scores indicated greater satisfaction.
An average appointment satisfaction score was computed by summing the items and dividing by five, resulting in one score on the same scale as the original questions. Appointment satisfaction questions were completed by control participants once, ∼6 months after their baseline study appointments; CoYoT1 Clinic participants completed these questions every 3 months throughout the study. As the survey was administered to control participants only once and follow-up with these patients was poor, control participant appointment satisfaction data were compared to CoYoT1 participant data collected ∼6 months after study entry.
An additional five statements asked CoYoT1 Clinic participants about using online technology to receive care (e.g., “I felt comfortable using technology for my online visit,” “I would recommend this technology to others”). CoYoT1 participants completed these questions every 3 months following their baseline study appointment, until the end of the study period. Average technology satisfaction scores were computed at each time point using the same procedure used for appointment items, and used to assess satisfaction with technology use among CoYoT1 participants over the course of the study.
Statistical analyses
Patient demographic and clinic attendance data in the year before study enrollment were obtained from the electronic health record. Age, T1D duration, appointment satisfaction, average number of appointments attended before and during the study period, and numbers of HbA1c and blood glucose checks completed were compared between groups using Student's t tests. Overall changes in HbA1c, as well as changes in the number of HbA1c and blood glucose checks over time, were compared using repeated measures analysis of variance (RMANOVA). Attendance and adherence to T1D care at each clinic session were compared between groups using chi-squared or Fisher's exact tests, wherever appropriate. Overall changes in attendance and care adherence percentages over time within each group were compared using Cochran's Q test, a nonparametric equivalent of RMANOVA for dichotomous outcomes. All analyses were conducted using Stata 14.2 (StataCorp, LLC, College Station, TX).
Results
Patient characteristics
Forty-two patients who enrolled in the CoYoT1 Clinic were compared to 39 patients who enrolled in the control arm and received treatment as usual. The mean age of CoYoT1 patients was 19.8 years, compared to 20.5 years in controls (P = 0.10).
Patients in the control group reported longer T1D duration on average (mean = 11.7, standard deviation [SD] = 5.5) compared with patients in CoYoT1 [mean = 8.2, SD = 4.7; t(79) = 3.08, P = 0.003], but there were no other significant differences at baseline. Both groups were distributed similarly in terms of sex (females: 55% CoYoT1, 51% controls), and most patients were white and non-Hispanic (79% CoYoT1, 74% controls). Additional demographic and clinical characteristics of 81 study participants are shown in Table 1.
Duration of T1D was significantly shorter in the CoYoT1 Group compared with the Control Group, P = 0.003. No other comparisons were significant.
CoYoT1, Colorado Young Adults with T1D; HbA1c, hemoglobin A1c; SD, standard deviation; T1D, type 1 diabetes.
Notably, the 11 patients who enrolled in the study, but attended no clinic sessions during the study period were all in the control group and were significantly older (mean = 21.4, SD = 1.4) than those patients who participated in at least one session [n = 70, mean = 20.0, SD = 1.8; t(79) = 2.41, P = 0.02]. These 11 patients also reported longer T1D duration than those who attended at least one appointment [mean = 13.6 vs. 9.3 years, SD = 5.2; t(79) = 2.56, P = 0.01] and exhibited marginally higher HbA1c levels at baseline [mean = 9.5 vs. 8.6, SD = 1.7; t(75) = 1.70, P = 0.09]. These patients were included in all comparisons of clinic attendance and care adherence.
Clinic attendance
In the year before the study, patients in the CoYoT1 group attended 2.6 clinic visits on average, compared to 2.3 clinic visits for patients in the control group (P = 0.28). During the study period, patients in CoYoT1 completed 3.5 visits on average compared with 1.1 visits on average for the control group, t(79) = 10.77, P < 0.0001. While CoYoT1 patients increased visit adherence by, on average, nearly one visit compared to the previous year, control patients were seen for at least one visit fewer compared to the previous year. Furthermore, 74% of CoYoT1 patients were seen four times over 12 months, meeting ADA guidelines, but no patients in the control group met the ADA recommendation (Table 2). During the year preceding the study, only 21% of patients who participated in CoYoT1 were seen at least four times during the year, compared to 8% of control patients (P = 0.51), which resulted in 50% of CoYoT1 patients moving into compliance with ADA visit frequency recommendations during the intervention.
Patients in the control condition were offered a fifth clinic at the end of the study year, attended by 19 patients (44%). This fifth clinic is included in the mean value and number of clinics attended percentage, reported above.
Care adherence
In addition to attending more clinics, patients in the CoYoT1 group demonstrated greater care adherence throughout the study period compared with patients in the control group (Fig. 2). Patients in CoYoT1 had significantly fewer completed HbA1c tests at baseline compared with controls (90% vs. 100%), less frequent insulin pump usage (45% vs. 51%), and nearly equal rates of downloading diabetes device data (82% vs. 79%). However, over the course of the study period, patients in CoYoT1 continued to adhere to care recommendations at approximately twice the rate of patients in the control group (Fig. 2).
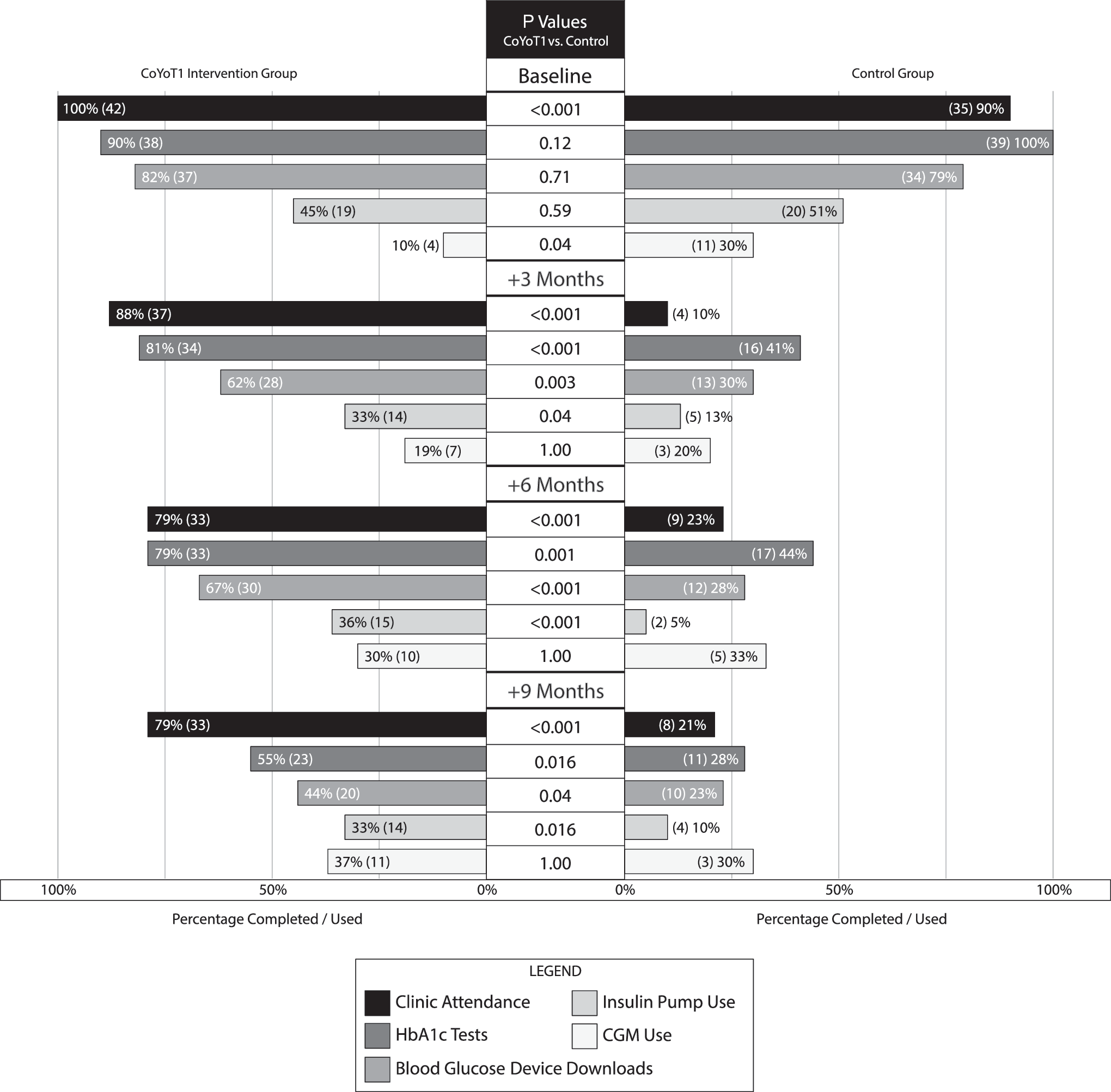
T1D care adherence and technology use by study group. P values reported above compare the relative frequencies of diabetes care adherence and technology usage between the CoYoT1 Intervention and Control groups. Numbers at the end of each bar are the compared percentages, with raw n values for each group in parentheses representing the number of people who provided data about their care adherence or attended clinic at each study time point. Percentage scaling is noted on the horizontal axes. T1D, type 1 diabetes.
At the end of the study year, 21 patients in CoYoT1 (50%) met the goal of 4 or more HbA1c measures over the year, compared with 7 control patients who met the goal (18%, P = 0.002). Also, 44% of CoYoT1 patients provided blood glucose data at the last Clinic (compared to 23% of control patients, P = 0.04), although few patients in either group consistently tested blood glucose more than four times per day by the end of the study year (nine in CoYoT1, three in standard care). Furthermore, 33% of CoYoT1 patients still used insulin pumps at the end of the study year (compared to 10% of control patients, P = 0.02).
When considering changes in individual patient adherence over time, completion of HbA1c tests significantly decreased over the study year in both groups, but more drastically in the control group [Control Group Cochran's Q χ2 (3) = 43.91, P < 0.0001; CoYoT1 Group Cochran's Q χ2 (3) = 25.24, P < 0.0001]. Similarly, diabetes device downloads significantly decreased in both study groups, but the decrease in adherence in the control group was larger [Control Group Cochran's Q χ2 (3) = 35.30, P < 0.0001; CoYoT1 Group Cochran's Q χ2 (3) = 17.43, P = 0.0006]. On the contrary, insulin pump usage was nearly constant in the CoYoT1 group over the study year [Cochran's Q χ2 (3) = 2.83, P = 0.42], but decreased significantly in the control group following the baseline assessment [Cochran's Q χ2 (3) = 37.8, P < 0.0001].
Use of CGM was different at baseline, but this difference did not persist at the end of the study period. While 30% of participants in the control group and only 10% of those in CoYoT1 reported using CGM at baseline (P = 0.04), this significant difference was not present at any assessment conducted after baseline due to an increase in CGM use in patients in CoYoT1 Clinic (30% of control and 37% of CoYoT1 patients used CGM at the end of the study, P = 1.00). While CGM usage was nearly constant in the control group [Cochran's Q χ2 (3) = 3.00, P = 0.39], it increased significantly in CoYoT1 patients [Cochran's Q χ2 (3) = 8.68, P = 0.03].
Patient satisfaction
Compared with patients in the control group (mean = 3.85, SD = 0.70), patients in the CoYoT1 group (mean = 4.18, SD = 0.49) reported higher appointment satisfaction after ∼6 months of participation in the study, t(58) = 2.17, P = 0.03. Although patients in both groups felt equally supported, comfortable, and able to speak freely during appointments, patients who participated in standard clinical care reported some difficulty with fitting appointments into their schedules.
Within the CoYoT1 Clinic group, satisfaction with the online technology used to conduct appointments stayed high over the course of the study year, starting at 4.44 (SD = 0.49) after 4 months of participation, and increasing slightly to 4.61 (SD = 0.55) after 12 months of participation, t(63) = 1.33, P = 0.19. Overall, patients in CoYoT1 would recommend the technology to others, felt they received the care they needed, and thought the format allowed them to express concerns comfortably and privately.
HbA1c and blood glucose checks
Although a separate visit to a commercial laboratory was required to obtain an HbA1c value before the CoYoT1 telehealth visit, participants in the CoYoT1 group completed slightly more HbA1c tests on average over the course of the study year than patients in the control group (CoYoT1 = 3.0, control = 2.6; Table 3). However, this difference was not statistically significant. Furthermore, HbA1c values did not significantly change over the course of the study year in either group (RMANOVA group × time interaction P = 0.92). Patients in the control group exhibited a 0.04 decrease in HbA1c (SD = 0.96) from baseline, while patients in CoYoT1 Clinic experienced a 0.14 decrease (SD = 1.18; P = 0.76).
We used Student's t-test for pairwise comparisons, and RMANOVA for examination of overall group × time interactions. All P-values reported above are from these tests.
RMANOVA, repeated measures analysis of variance.
Participants also did not significantly differ in terms of the number of blood glucose checks performed per day over the course of the study year (RMANOVA group × time interaction P = 0.86). Although participants in CoYoT1 checked blood glucose more frequently after 1 year (mean = 5.1, SD = 6.9) compared with patients in the control group (mean = 3.4, SD = 1.8), this comparison did not reach statistical significance (P = 0.44).
Subanalysis of clinic attendees
The poorer attendance of control participants (including 11 who attended no clinics) likely altered outcomes attributable to this group as a whole. To address this issue, the subset of patients who attended at least one session during the study (CoYoT1 or control) was examined in a separate subanalysis. The notable changes between the subanalysis results and the complete study results are in completion of Blood Glucose downloads and HbA1c tests, where the relative percentages of adherence in control patients who attended at least one clinic during the study year are greater relative to the adherence of the whole control group, shown in Figure 2. In all cases, highly significant differences remain significant, and marginal effects (e.g., reports of Insulin Pump use in Clinic 2; Blood Glucose test adherence reported at Clinic 4) emerge where differences between CoYoT1 and all control patients were less extreme.
Discussion
Young adults with T1D are routinely disengaged from their care and lost from the medical system until they are well into their adult years. 7,10,12,25 “Meeting them where they are” through telemedicine may present a useful means for maintaining engagement in young adult patients as they transition to adulthood by improving healthcare access and potentially reducing healthcare cost. The CoYoT1 Clinic model applied home telemedicine to routine young adult T1D care and retained nearly 80% of patients, who participated in diabetes care activities, including diabetes medical visits and HbA1c testing, more frequently than their peers in routine care. Thus, telemedicine may be a vital key to improving care access and engagement for young adults with diabetes. Of note, decreasing barriers to clinic attendance with telemedicine likely had a significant impact on the frequency of visits in CoYoT1 patients. Patients completed visits on campus between classes, from their break rooms at work, from the campus library, in their cars (not while driving) between various daily activities, from their dorm rooms or apartments, and from their family's home over breaks from school.
Although CoYoT1 patients and those in routine young adult T1D care attended clinic at nearly equal rates in the year before the intervention, patients in CoYoT1 attended clinic between 4 and 10 × more frequently during the study year. Furthermore, 74% of CoYoT1 patients saw their diabetes provider at least four times during the study year, adhering to the care recommendations outlined by the ADA. Of note, recent data have shown that increased visit frequency may be the one modifiable factor associated with decreased emergency department visits in young adults with T1D. 26 The increased engagement and visit frequency seen in CoYoT1 Clinic may result in healthcare cost-savings in addition to preventing the loss to follow-up routinely seen in young adults with T1D.
It is important to comment on the 11 patients who initially enrolled in the study, but completed no study visits. It is hypothesized that these patients transferred to other providers, moved out of the area, and/or became disengaged in their diabetes care. Unfortunately, the study team was unable to connect with these patients, so the actual reasons for lack of participation are unknown. The baseline differences between the patients who did not participate following enrollment and those who did were older age and longer T1D duration in those patients who attended no study visits. This could have resulted in the patients moving to a provider outside of the BDC. However, BDC has neither age nor insurance requirements for transfer of care, and adult providers are available in the diabetes center, which makes the need to transfer care less likely.
Following an initial clinic visit at study enrollment, when participation in care activities was nearly equal, patients seen in CoYoT1 Clinics completed HbA1c and diabetes device downloads for medical review at almost twice the rate of patients in routine care. CoYoT1 patients also reported insulin pump use at three to six times the rate reported by control patients over the course of the study year. CoYoT1 patients used CGM less frequently than patients in usual care at the beginning of the study, but patients in both groups reported equal usage in subsequent clinic visits. Thus, telemedicine may promote patient usage of diabetes care technologies, and greater adherence to care recommendations overall. Group discussions in CoYoT1 could have also impacted patients' frequency of CGM use, as patients frequently related their experiences with CGM use during these sessions. Patients not using CGM before the intervention may have been impacted by their peers' positive reports during the group discussions, resulting in increased interest in adding the technology for their own diabetes management.
Telemedicine may even encourage patient engagement across all forms of care. Seventy-nine percent of CoYoT1 patients attended their single in-person appointment (Clinic Visit 3), compared with 23% of control patients who attended their third clinic visit, or 46% of control patients who completed their final annual assessment appointment (Clinic Visit 5). This two- to fourfold increase in their in-person clinic attendance in the CoYoT1 group may be attributable to the limited in-person requirement (i.e., patients are more likely to attend a single in-person visit if offset with online visits) or the overall higher level of engagement with their own diabetes care management, which is impressive.
Patients in the CoYoT1 group were more satisfied with their care experiences during the study year compared with control patients. In addition, they were highly satisfied with the technology throughout the intervention, indicating that telemedicine-enabled visits are not generally viewed as burdensome, despite some patient reports of technical issues. The main issue encountered with technology was the impact of Internet firewalls at work establishments, but patients were able to address this barrier by using different connections or leaving work for their appointment (e.g., using public wireless vs. their work wireless Internet connection). However, only a few CoYoT1 patients reported this issue. The chief complaint among the patients in routine care was the difficulty in fitting appointments into their schedules.
The flexibility of the CoYoT1 telemedicine model is a likely reason for increased attendance and patient adherence in that group, even with limited in-person requirements. As mentioned previously, patients only needed an Internet connection, microphone, and camera to allow for participation, which resulted in appointments being conducted at home, work, school, and multiple other locations without significantly impacting their daily schedule compared to the additional time required for travel to and from a physical appointment.
Despite greater adherence, attendance, and satisfaction, patients in the CoYoT1 group did not experience significant improvements in HbA1c levels over the course of the study year compared with control patients. This result is consistent with other studies examining the use of telemedicine for diabetes care management, 27 and is not unexpected during this feasibility pilot study. Potential reasons for this may be (1) the duration of follow-up was too short, (2) lack of randomization, and/or (3) high attrition rates in the control group despite providing extended time to complete their final visit and data collection process. In addition, we did not provide an extensive, focused curriculum on behavioral change in the young adults. Although the group component did include these topics, the purpose of this study was not to test a formal curriculum, but to examine the feasibility and acceptability of the CoYoT1 Clinic model. Further work is underway to design a robust curriculum with continued emphasis on interventions for behavior change and improved diabetes outcomes in the young adult population with diabetes.
Limitations
Our study has multiple accompanying limitations. First, the study was not a randomized controlled trial, which may limit its generalizability to more technology savvy young adults. CoYoT1 participants self-selected into the intervention, and may have been more motivated to change their care behaviors or attend medical care sessions generally. Second, patients participating in CoYoT1 were not billed for appointments, which could have biased their initial involvement in the study while also influencing their continued follow-up. Third, patients participating in CoYoT1 had more direct contact for scheduling appointments with personalized reminders versus the automated reminder systems used in the diabetes center for regular appointments. This could have impacted patient engagement and follow-up. Also of note, CoYoT1 participants had shorter duration of disease, which may explain some differences in care behavior (i.e., longer disease duration may be associated with more hopelessness about care and reduced participation).
Nevertheless, care behaviors in the year preceding the study were similar in both patient groups, suggesting that the CoYoT1 telemedicine model is useful for changing patient behavior positively—an important first step in patients regaining glycemic control. Finally, patients in CoYoT1 experienced both group visits and home telemedicine, which could have impacted their outcomes. Future studies need to delineate the impact of each of these interventions on patient outcomes.
Future directions
eHealth-based interventions have the potential to support the monitoring of physical and psychosocial well-being, facilitating peer contact and support, interaction between members of the healthcare team, and exchange of data between patients and healthcare professionals. 28 Successful implementation of web-based interventions is often complicated by factors such as the level of information technology availability, technical support, and the ease of use. 29 Despite these previously reported findings, we did not encounter similar barriers in CoYoT1 Clinic, and technology satisfaction and use were high among our participants. Attrition is also a commonly noted problem associated with eHealth interventions; 27,30,31 however, the retention rate in the CoYoT1 patients was quite high and those who participated attended medical visits with significantly greater frequency than their peers in the control group. Experts have recommended user-centered approaches (e.g., user-centered design and individualization within programs); increased emphasis on engagement (e.g., gamification or telepresence); improved collaboration in development, testing, and data sharing; and timely implementation of interventions as keys to improving outcomes in eHealth interventions. 32 These recommendations are being reviewed for future adaptations of CoYoT1 Clinic.
Future studies of the CoYoT1 Clinic model will examine psychosocial outcomes of patients participating with the goal of identifying potential targets for more structured intervention and curriculum, designing a randomized controlled trial of the revised CoYoT1 Clinic model, evaluation of cost effectiveness of the intervention, and eventual expansion to other systems and healthcare models.
Conclusion
In this pilot study, we found high engagement, retention, and satisfaction in young adult patients with T1D participating in CoYoT1 Clinic. The study met our goal of designing a feasible and acceptable care model for young adults with T1D—a historically challenging population. Keeping young adult patients engaged in their care while they transition to adulthood may produce several benefits, including decreased healthcare costs, improved quality of life, and better psychosocial and mental health outcomes. These patients may see decreased healthcare costs through avoidance of more expensive healthcare services (e.g., emergency department visits or hospital admissions), early detection of serious complications (due to completion of regular screenings), and identification of care barriers than can be addressed by the diabetes team. The improved peer support, positive relationships with their healthcare team, and true patient-centered care may directly impact their behavioral and mental health outcomes beyond improving the engagement in care.
Footnotes
Acknowledgments
The authors thank Jackie Shea, Kylie Benson, and Kaitie Ketchum who participated in study recruitment and implementation. The authors are also deeply grateful to the patients who participated in this research. We are inspired and motivated by your journey with diabetes. Funding source: The Leona M. and Harry B. Helmsley Charitable Trust.
Author Disclosure Statement
The authors report no competing financial interests exist.