
Abstract
Backgrounds:
This study aims to compare glycemic control of persons with type 1 diabetes using multiple daily injections (MDI) with insulin glargine versus insulin detemir or with continuous subcutaneous insulin infusion (CSII) in daily practice.
Subjects and Methods:
All adult individuals with type 1 diabetes (n = 1053) were identified from the electronic patient database in North Karelia, Finland. The persons' individual data for insulin treatment, diabetic ketoacidosis (DKA), and hemoglobin A1c (HbA1c) measurements during the year 2014 were obtained from medical records. Persons using long-acting insulin analogs or CSII were included in the analyses (n = 1004).
Results:
Altogether, 47.7% used glargine, 43.9% used detemir, and 8.4% used CSII. The mean HbA1c was lower in the CSII group (63 mmol/mol [7.9%]) compared with the glargine group (66 mmol/mol [8.2%]) or the detemir group (67 mmol/mol [8.3%]). The overall rate of DKA was 5.1% per year. The rate of DKA was higher in the detemir group compared with the glargine group (6.3% per year vs. 3.8% per year, respectively, P < 0.049). In logistic regression analyses, the higher rate of DKA with detemir use was explained by HbA1c.
Conclusions:
In daily practice, the glycemic control of type 1 diabetes patients with MDI was similar regardless of basal insulin, glargine, or detemir, whereas CSII allowed better glycemic control than MDI. The rate of DKA was higher with detemir than with glargine, but this is likely related to higher HbA1c rather than insulin regimen.
Introduction
T
Conventional basal insulin, neutral protamine Hagedorn (NPH) insulin, does not mimic basal insulin requirements optimally, because it has an inadequate duration of action, pronounced peaks a few hours after injection, and great intrapatient variability. 6 To overcome these limitations, new long-acting insulin analogs (glargine, detemir, and recently other regimens) have been developed. 7 In comparison with NPH insulin, long-acting analogs have a small lowering effect on HbA1c and reduce the risk of nocturnal and severe hypoglycemia. 7 Randomized clinical trials have established that there are no clinically relevant differences between glargine and detemir in terms of glycemic control or in the occurrence of overall hypoglycemia. 8,9 However, the risks of severe and nocturnal hypoglycemia may be lower with detemir. 8
The administration of insulin via continuous subcutaneous insulin infusion (CSII) mimics the body's physiologic release of insulin better than multiple daily injections (MDI) of insulin. In a recent meta-analysis of adults with type 1 diabetes, treatment by CSII with insulin analogs has been demonstrated to decrease HbA1c more than MDI. 10 The meta-analysis included studies using long- and rapid-acting insulin analogs or NPH and regular insulin in the MDI groups, because both regimens are used in current practice.
Comparisons of different insulin regimens and modalities for the treatment of people with type 1 diabetes have been performed in clinical trials and crossover studies. But the evidence is lacking as to whether one insulin treatment is superior to another in daily practice in population-based settings. This population-based study aims to compare glycemic control and the risk of diabetic ketoacidosis (DKA) in adults with type 1 diabetes using MDI with glargine versus detemir or CSII in daily practice.
Subjects and Methods
The region of North Karelia in eastern Finland consists of 13 municipalities. All of the local primary healthcare centers and central hospital have a common regional electronic patient database. The detailed descriptions of database and information regarding the diabetes diagnoses are reported in our previous study. 5
Subjects and data
From the patient database, all persons who had a type 1 diabetes mellitus diagnosis according to ICD-10 codes (E10.1–E10.9) were selected. Altogether, 1053 adults (≥20 years of age at the beginning of 2014) who were alive at the end of 2014 were identified. Altogether, 920 (87.5%) used long-acting insulin analogs, 84 (8.0%) used CSII, 45 (4.3%) used NPH insulin, and 2 (0.2%) did not use any long-acting insulin (due to the temporal remission of newly diagnosed diabetes). As the aim of the study was to compare modern insulin treatment modalities, we included 1004 subjects using long-acting insulin analogs or CSII.
During 2014, the following data were obtained from medical records: date of birth, gender, data for insulin regimens and other medications, HbA1c measurements, documented diabetes complications (ICD-10 codes E10.2–E10.9), hypertension (ICD-10 code I10), and hospitalizations due to DKA (ICD-10 code E10.1). The recurrent DKA admissions of the same person during the 12-month period are not included in the numbers. We included all the HbA1c measurements during the year 2014 and calculated the mean values of them for the analyses.
Biochemical methods
All HbA1c samples were analyzed in the same laboratory (Eastern Finland Laboratory) using the turbidimetric inhibition immunoanalysis method (TINIA), and values were standardized to International Federation of Clinical Chemistry (IFCC) units. The normal range was 20–42 mmol/mol (4.0%–6.0%), and the average coefficient of variation was 3%.
Statistical analyses
Statistical analyses were performed using the IBM SPSS statistics program (Statistical Package for the Social Sciences). The significance of differences was estimated with the chi-square test for frequencies and ANOVA of Student's t-test for mean values.
This research was approved by the Ethics Committee of the North Savo Hospital District (which includes the North Karelia Hospital District) on 13.11.2012.
Results
Out of 1004 participants included in the analysis, 479 (47.7%) used glargine, 441 (43.9%) used detemir, and 84 (8.4%) used CSII. Altogether, 1.1% used regular short-acting insulin, and 98.9% used short-acting insulin analogs.
Comparison of treatment groups
Table 1 demonstrates comparison of characteristics and glycemic control in the different treatment groups (glargine, detemir, and CSII). The CSII users were younger and 71.4% of them were women. The use of short-acting insulin analogs and other medications differed between groups. The detemir group had less complicated diabetes. The overall mean HbA1c during 2014 was 66 mmol/mol ±15 mmol/mol (8.2% ± 1.4%). The mean HbA1c was lower (P = 0.053) in the CSII group (63 mmol/mol ±11 mmol/mol [7.9% ± 1.0%]) compared with the glargine group (66 mmol/mol ±14 mmol/mol [8.2% ± 1.3%]) and the detemir group (67 mmol/mol ±16 mmol/mol [8.3% ± 1.5%]).
Comparison between glargine and CSII groups, Student's t-test, NS.
Comparison between detemir and CSII groups, Student's t-test, P = 0.023.
CSII, continuous subcutaneous insulin infusion; ASA, asetosalisylic acid; ACE, angiotensin converting enzyme; ATR, angiotensin receptor.
Figure 1 shows the mean HbA1c categories by treatment groups. Of all persons with type 1 diabetes mellitus, 16.9% reached an HbA1c level <53 mmol/mol (7.0%), and 23.6% had an HbA1c level >75 mmol/mol (9.0%). The CSII group had a high HbA1c (>75 mmol/mol [9.0%]) less frequently (12.0%) than the glargine group (23.7%, P = 0.035) or the detemir group (26.0%, P = 0.009).

HbA1c categories assessed using the mean of HbA1c measurements during 12 months by treatment groups. *Comparison between Glargine and CSII groups, χ 2-test, P = 0.035. **Comparison between Detemir and CSII groups, χ 2-test, P = 0.009. CSII, continuous subcutaneous insulin infusion.
Diabetic ketoacidosis
Altogether, 51 persons had one or more DKA events (18 in the glargine group, 28 in the detemir group, and 5 in the CSII group). The overall rate of DKA was 5.1% per year (53.4 per 1000 person-years). The rate of DKA was higher in the detemir group compared with the glargine group (6.3% per year vs. 3.8% per year, respectively, P < 0.049), but there was no difference compared with the CSII group (Fig. 2). Comparing MDI users with and without DKA, Table 2 shows that persons with DKA had a significantly higher HbA1c and used more detemir. The association of DKA with different long-acting insulins (detemir vs. glargine) and other factors were further analyzed by logistic regression analyses (Table 3). In logistic regression analyses, there was a trend showing that detemir increased the risk of DKA, but the association was not significant (OR 1.74, 95%CI: 0.95–3.19; P = 0.075). This association was explained by HbA1c, which was significantly associated with the risk of DKA (OR 1.41, 95% CI: 1.15–1.72, P = 0.001).
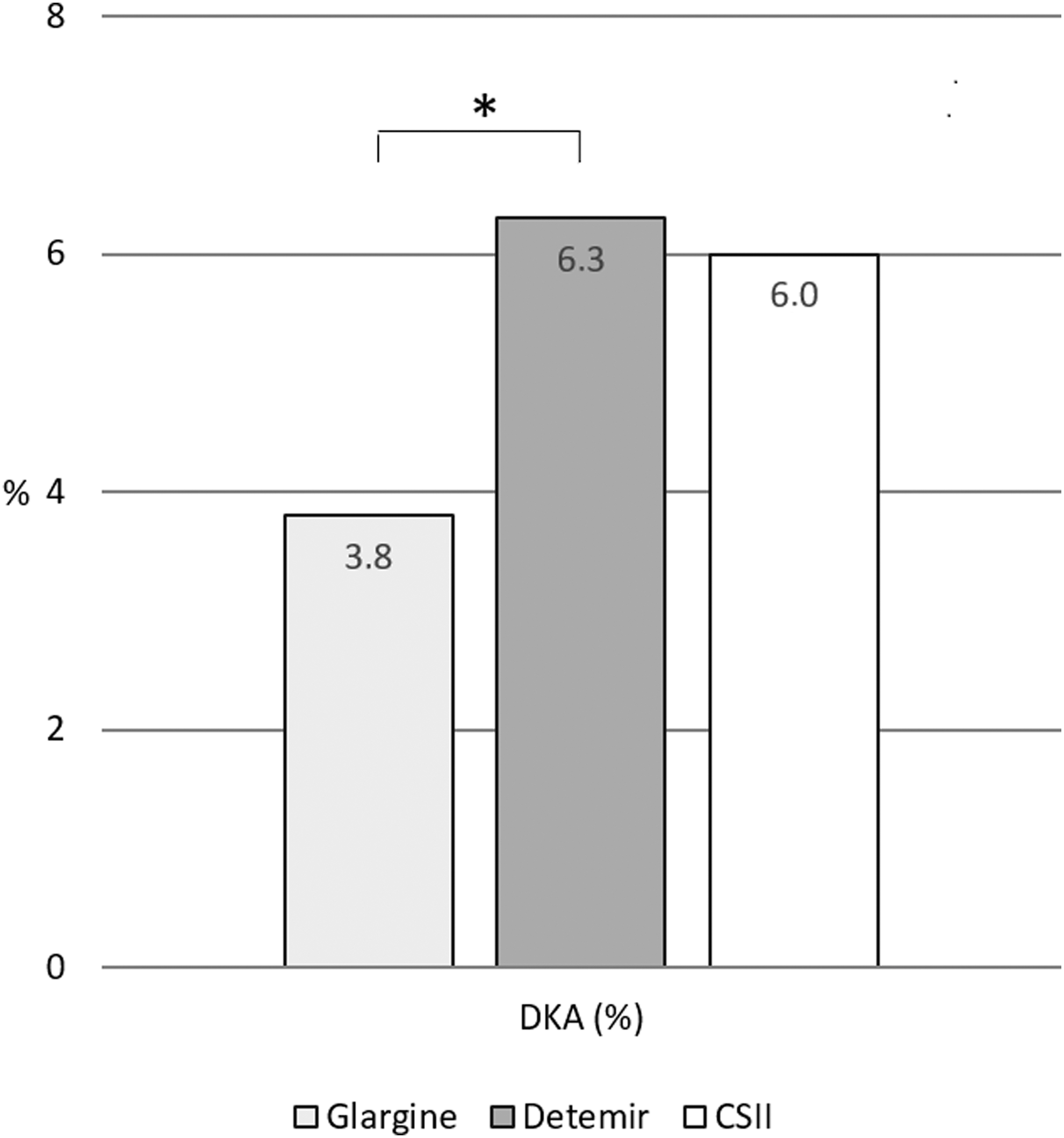
Rates of DKA during 12 months by treatment groups. *Comparison between Glargine and Detemir groups, χ 2-test, P = 0.049. DKA, diabetic ketoacidosis.
MDI, multiple daily injections; DKA, diabetic ketoacidosis.
Discussion
The present study is the first population-based study comparing different insulin treatment modalities of people with type 1 diabetes in a “real-world” setting utilizing local electronic patient records. The major finding of this study is that in the daily practice of adults with type 1 diabetes, glycemic control is similar with long-acting insulin analogs, glargine and detemir, whereas CSII treatment results in better glycemic control than did MDI treatment. Detemir seems to increase the risk of DKA compared with glargine, but higher HbA1c rather than insulin detemir itself likely explains this.
Strengths and limitations
The strength of the study is that we included all diagnosed adults with type 1 diabetes in our region. We managed to obtain accurate data on these persons. Our joint regional electronic patient database allowed us to collect data concerning diabetes medication, complications, and glycemic control covering all primary health centers and the secondary care hospital. Laboratory data were comparable and valid, because all HbA1c measurements were performed in the same laboratory, and HbA1c values were collected automatically from the electronic database.
We acknowledge the limitations of this study. The definition of type 1 diabetes is based on the diagnosis found in patient records. There might be some deficiency in the registering of the diagnoses in patient records, and the number of these dropouts remains unknown. However, this database should include, quite comprehensively, adults with type 1 diabetes who have visited a physician at their health center or the hospital since 2011. The diagnosis of DKA was based on the diagnosis documented during hospitalization due to it (ICD-10 code E10.1). Because moderate or severe DKA requires hospital admission, it is likely that most of the DKA cases are included in this study. The total number of persons diagnosed with DKA was small. Unfortunately, the numbers of persons with severe hypoglycemia (ICD-10 code E10.00) found in the database were not reliable.
Many of the hypoglycemic episodes were treated at home by emergency medical assistance from ambulance services; and, therefore, they were not always recorded in patient records. In addition, the exact diagnosis of diabetes complications was not available from 12.5% of persons, because only ICD-10 code E10 without a specifying decimal number was documented in their medical records. Because the data were obtained from an electronic database, some essential data (such as duration of diabetes and detailed information about insulin treatment) were not available.
Comparison of insulin glargine and detemir use
The use of glargine and detemir was equally common among people with type 1 diabetes. The national Finnish Current Care Guidelines do not suggest any preference between glargine and detemir for people with type 1 diabetes. 11 In Finland, the pricing of these two insulins is equal. In the recent large register study from Germany and Austria, the use of glargine (38.0%) was more common compared with detemir (19.9%) among people with type 1 diabetes. 12 In the DAFNE (Dose Adjustment for Normal Eating) study from the UK, 16.6%–17.8% of program participants used NPH insulin as basal insulin. At baseline, 31.6% used detemir and 48.0% used glargine; whereas, after 12 months follow-up, a portion of glargine users had switched to detemir making usage numbers more equal (detemir 40.2% and glargine 42.0%).
In the present study, type 1 diabetes adults using glargine or detemir differed from each other. The persons using glargine were older, had higher body mass indexes (BMIs), had slightly more diabetic complications, and used more of other medications. The majority of persons had insulin aspart as their short-acting insulin, but persons using glargine more often had insulin lispro as their short-acting insulin compared with those using detemir. We can only speculate the factors affecting the selection of certain insulins for individual persons. Selection is probably based on the practice of clinicians prescribing certain insulins and the characteristics of insulins (such as duration of action, predictability, and tolerability) to suit the needs of individual persons.
We found that glycemic control (HbA1c) was similar with the two insulin analogs. In daily clinical practice, the evidence regarding whether glargine or detemir has any advantage or disadvantage over each other is scarce. In the clinical trials, there has been no clinically relevant difference in glycemic control between glargine and detemir, 8,9,13 but data regarding safety and detailed glucose variability have yielded conflicting results. 8,9 Some data have indicated the superiority of glargine in terms of more stable glycemic control, 14,15 whereas another study demonstrated that detemir has a more predictable glucose lowering effect. 6 A Canadian study reported that the treatment of people with type 1 diabetes with glargine (instead of detemir) can generate long-term cost savings, which are mainly driven by the lower dose of insulin required for glargine compared with detemir. 16
Continuous subcutaneous insulin infusion
In the current study, 8.0% of all adults with type 1 diabetes used CSII in our region in Finland. Over two-thirds of CSII users were women, and they were on average younger and had more complicated diabetes than MDI users. In an Italian study of people attending diabetes centers, 15% of adults with type 1 diabetes were treated with CSII. The mean age of CSII treated persons was 40.3 years and 43% were men. 17 Higher rates of CSII use were reported in an annual report of the Swedish National Diabetes Register, in which the proportion of adults with type 1 diabetes treated by CSII was 22.7% (27.3% women and 19.0% men) in 2016. 18
The results of our study are in agreement with the previous findings that CSII treatment allows better glycemic control than MDI treatment, and it does not increase the rate of DKA. Importantly, we found that CSII resulted in better glycemic control, despite use in a population with more complicated diabetes. In our region, all people with CSII used short-acting insulin analogs. The meta-analysis of Yeh et al. indicated that adults with type 1 diabetes treated by CSII with insulin analogs had better glycemic control (witnessed by decreases in HbA1c) than those treated by MDI with insulin analogs, NPH, or regular insulin. 10 A recent review showed that CSII treatment of type 1 diabetes is cost-effective compared with MDI in people who have poor glycemic control and/or problematic hypoglycemia, with cost effectiveness being highly sensitive to the reduction in HbA1c and hypoglycemia frequency associated with CSII. 19
DKA over the past 12 months
In the present study, hospitalizations due to DKA (within a 12-month period) were documented in 5.1% of 1004 adults with type 1 diabetes. A similar frequency of DKA, 4.8% over the past 12 months, was reported in the T1D Exchange Clinic Registry study of 6796 adult participants in the United States. 20 Another study from the same registry found that the rate of DKA during 12 months was more common, up to 12%, in the fair to poor control group (HbA1c ≥ 60 mmol/mol [8.5%]) compared with 1% of the excellent control group (HbA1c < 48 mmol/mol [6.5%]). 21 In our study, the rate of DKA was not significantly different between CSII and MDI users; confirming previous findings. Meta-analyses have demonstrated that CSII does not increase the risk of DKA. 22
However, we found that the occurrence of DKA was slightly higher in the detemir users than in the glargine users (6.3% per year vs. 3.8% per year, respectively, P < 0.049). In logistic regression analyses, this difference disappeared when HbA1c (which was significantly associated with the risk of DKA) was taken into account. Therefore, the higher rate of DKA in detemir users seems to be related to their slightly higher HbA1c compared with glargine users rather than choice of insulin regimen. There is no previous report of detemir increasing the risk of DKA compared with glargine.
The mechanism by which detemir would predispose persons to DKA could not be established in our study. Theoretically, a possible explanation could be the duration of action or the number of daily insulin injections. Our data did not allow us to get information on the number of insulin injections. Controversy exists as to whether both analogs can be used for once-daily dosing. 23 It has been demonstrated that glargine has a longer duration of action (27 h) compared with detemir (23 h) under steady-state conditions. 23 Twice-daily dosing might decrease the adherence to treatment. A recent review found no systematic differences in HbA1c between once- and twice-daily basal insulin use of glargine or detemir. 24 On the contrary, there is evidence that detemir might have greater indirect effects on hepatic glucose metabolism than glargine. 25
Conclusions
In conclusion, this population-based study confirms that CSII allowed better glycemic control than MDI in daily practice of adults with type 1 diabetes. Two basal insulins, glargine and detemir, were similar in terms of glycemic control. The rate of DKA was higher with detemir than with glargine, but this is likely to be explained by higher HbA1c rather than insulin regimen. However, the possible unfavorable effect of detemir on the risk of DKA compared with glargine warrants further investigation.
Footnotes
Acknowledgments
The authors gratefully acknowledge Markku Savolahti from the North Karelia IT center for providing patient data from the electronic database.
The authors acknowledge the Research Committee of the Kuopio University Hospital Catchment Area for the State Research Funding (project QCARE, Joensuu, Finland) and the Finnish Foundation for Cardiovascular Research for financial support.
Author Disclosure Statement
The authors declare that they have no conflict of interest.