
Abstract
Background:
Lipohypertrophy (LH) at insulin injection sites is a common but preventable complication in type 1 diabetes mellitus (T1DM). We evaluated the prevalence, contributing risk factors, and consequences of LH, specifically the glycemic variability (GV) among T1DM patients.
Methods:
This is a cross-sectional study conducted at a tertiary care center in India, wherein 139 subjects with T1DM were randomly selected and evaluated for the presence of LH through visual and palpation examinations. Demography, anthropometry, and injecting practices were evaluated using a validated questionnaire and their effect on LH was determined. Subsequently, the effect of LH on GV and unexplained hypoglycemia (UH) was studied. Mean glucose, mean amplitude of glycemic excursions (MAGEs), and continuous overlapping net glycemic action (CONGA) were assessed in a subset of patients who injected insulin alternately in LH and non-LH sites.
Results:
The overall prevalence of LH was 69.8%, and was significantly higher in adults than in children (P = 0.038). Improper rotation of sites (P < 0.0001) and insulin syringe reusage for more than five times (P = 0.009) significantly increase the risk of LH. The presence of LH has a significant effect on GV and UH with adjusted odds ratios of 17.65 (P < 0.0001) and 28.02 (P < 0.0001), respectively. Ambulatory glucose monitoring on a subset of patients confirmed that the mean glucose, MAGE, and CONGA were higher when subjects injected insulin at LH sites than at non-LH sites.
Conclusions:
Improper rotation of sites and reuse of needles are the leading causes of LH in Indian T1DM patients, which, in turn, significantly increases the risk of GV and UH.
Introduction
L
The primary aim of this study was to evaluate the prevalence of LH and to determine the contributing risk factors to LH in Indian T1DM patients. Our secondary objective was to determine the clinical consequences of LH with emphasis on GV and UH in these patients.
Research Design and Methods
This was a prospective observational study that followed the International Guidelines on Good Clinical Practices and was approved by the institutional ethics committee. Subjects with T1DM were recruited randomly from outpatients attending a tertiary care center at Nagpur, India, during the period November, 2015 to March, 2017. They represented a population from central and southern India. Furthermore, patients attending residential education camps for T1DM, organized by Non-Government Organizations, were included in the study. Details of the study and its objectives were explained to each patient before obtaining their informed consent. The inclusion criteria required subjects to be taking insulin for >1 year (either self-administered or injected by a caregiver) through either an insulin pen or syringes. Children below the age of 5 years were excluded. A total of 145 subjects with T1DM gave consent to participate. Six of these were found to be using insulin pumps and were excluded. Thus the data on 139 subjects were available for downstream analysis. A validated questionnaire was used to capture patients' response on injecting practices. 7 –9
A trained team of resident doctors, diabetes educators, nurses, and dieticians was involved in the study. Observation and palpation techniques were used in assessing LH rather than only visual examination. To feel subtle skin thickening, a gel lubricant was used and the hand was stroked firmly over the injection sites with sweeping and undulating movements. LH was graded as grade 0, no changes (normal fat texture); grade 1, visible hypertrophy of fat tissue but palpably normal texture; grade 2, massive thickening of fat tissue with firm texture compatible with palpable LH; and grade 3, lipoatrophy. 3 Patients' age, height, weight, body mass index (BMI), duration of diabetes, HbA1c, type of insulin use, insulin regimen, needle length, use of syringes or pens, number of daily injections, needle reuse, rotation of site, insulin regimen, and skin fold technique were collected. Subjects or their parents were asked about the site rotation practices and it was ascertained for the correct rotation technique. A history of injecting insulin into any LH site was elicited.
The evaluation of GV and UH was based on the analysis of patients' self-monitored BG recordings, which were required at least twice a day at different time points. Hypoglycemia was defined as the occurrence of more than one symptom of low sugar (palpitations, tiredness, sweating, strong hunger, dizziness, tremor, etc.) and a confirmed BG meter reading of <70 mg/dL (3.9 mmol/L). 10 Frequent UH was defined as hypoglycemia occurring one or more times a week in the absence of definable precipitating event such as change in medication, diet, or activity. 11 GV was diagnosed in the presence of BG oscillations from <70 mg/dL (3.9 mmol/L) to >250 mg/dL (13.8 mmol/L), at least three times a week in an unpredictable and unexplained manner with such a pattern present for at least the previous 6 months. 12,13
Ambulatory glucose profile (AGP) monitoring was performed on 10 subjects (∼10%) with LH and age >18 years, after obtaining their consent. Freestyle Libre Pro™ flash glucose monitoring system (Abbott Diabetes Care, Mumbai, India) was used to construct the profile. The Libre Pro technology uses an electrochemical sensor that measures interstitial glucose every 15 min for 14 days with a range of 40–500 mg%. The sensor was implanted in the left arm using aseptic techniques. Subjects were asked to inject their regular insulin doses into LH for the first 7 days and then into normal tissue sites (without LH) for the next 7 days.
GV was studied by calculating the mean glucose, mean amplitude of glycemic excursions (MAGEs), and continuous overlapping net glycemic action (CONGA). MAGE is the arithmetic mean of differences between consecutive peaks and nadirs of glucose readings, which was manually calculated by taking 24-h glucose values from the 2nd day compared with 24-h glucose readings from the 14th day. First and 15th days were not considered, as they often have incomplete readings. 14 Similarly, the CONGA metric calculates a difference between the current BG level and readings obtained n hours (days) earlier and then calculates the standard deviation of the differences. 15,16 The estimates were obtained for selected patients on the 2nd day when insulin was injected at LH sites and on the 14th day when injected at non-LH sites.
Figure 1 shows the order of analyses. At level I, demographic, anthropometric parameters, total daily doses (TDDs) of insulin, and injection techniques were evaluated and their association with LH was determined. At level II, the effect of LH on GV and UH in the presence of the demographic parameters was evaluated. GV was further ascertained by calculating mean BG, MAGE, and CONGA using AGP. Both level I and II analyses were performed separately.
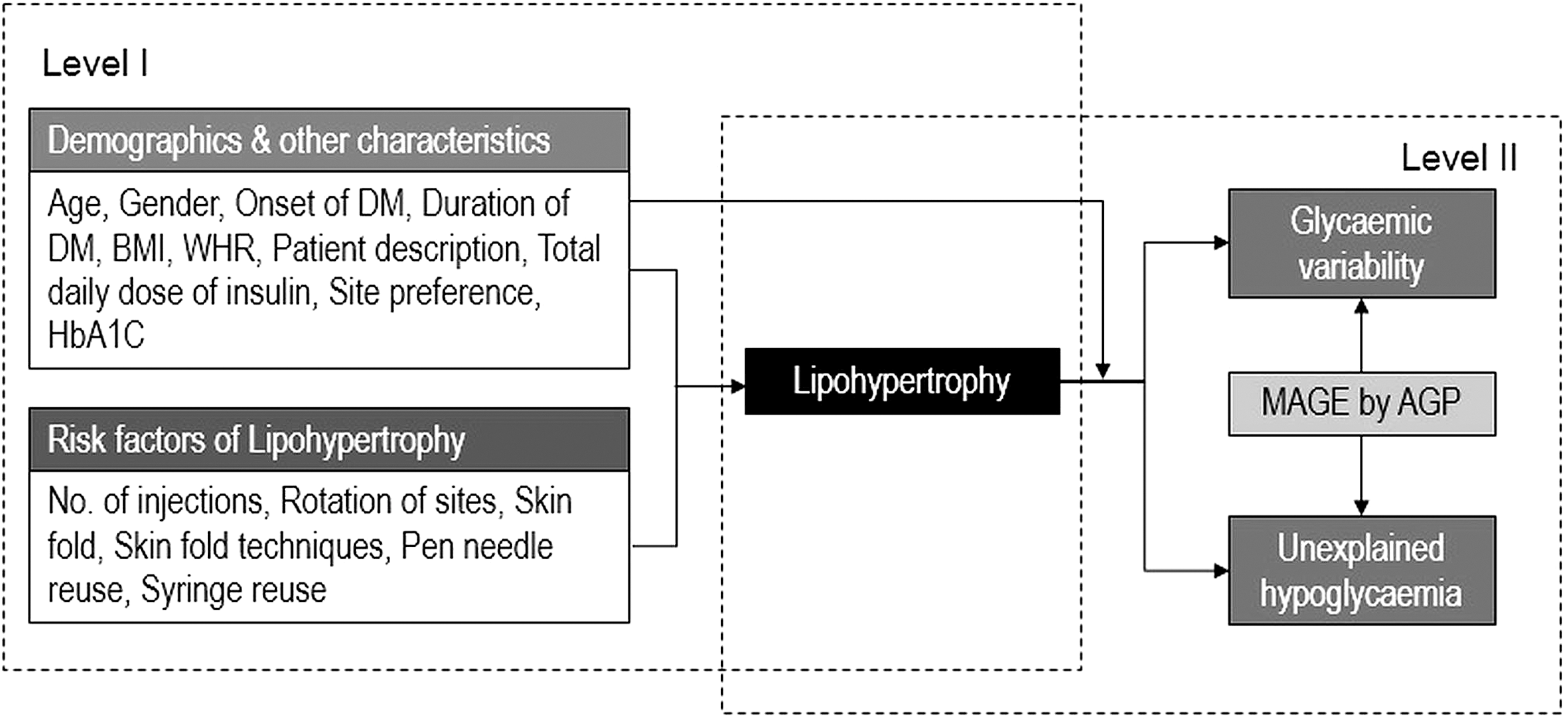
Conceptual flow of analysis.
Statistical Methods
Descriptive statistics including mean and standard deviation were obtained for all continuous variables, whereas frequencies and percentages were obtained for categorical variables. The significance of association of various categorical variables with LH condition was determined using the Pearson chi-square test. At level I, univariate analysis was performed to estimate the odds associated with different risk factors of LH. Multivariate logistic regression was performed to obtain the adjusted odds associated with these risk factors. Goodness of fit was assessed by the Hosmer–Lemeshow test. At level II, the effect of LH on GV and UH was evaluated independently and in presence of covariates. The mean difference of BG, MAGE, and CONGA, between LH and non-LH sites, was tested using a paired t-test. All the analyses were performed using SPSS ver. 20.0 (IBM Corp, Armonk, NY) and the statistical significance threshold was set at 5%.
Results
Prevalence of LH
The overall prevalence of LH in T1DM patients was 69.8% (97/139). Among children (<18 years), it was 60.6% (37/61), whereas in adults (>18 years), it was 76.9% (60/78). The difference between these two values was statistically significant (P = 0.038). Furthermore, in males, the prevalence was 66.7% (50/75), whereas in females it was 73.4% (47/64). The descriptive statistics for various characteristics of T1DM with and without LH are shown in Table 1. The overall age of patients was 21.71 ± 11.78 years with a mean duration of diabetes of 8.70 ± 7.52 years. The mean age of children in the LH group (11.61 ± 3.72 years) and the non-LH group (11.91 ± 4.38 years) differed insignificantly, and the same held for adults. Other characteristics such as gender, age of onset of diabetes, duration of diabetes, HbA1c, BMI, and waist-to-hip ratio (WHR) showed statistically insignificant differences between LH and non-LH groups. Among those with LH, 74 (76.3%) had grade I, 23 (23.7%) had grade II, whereas there was no case of grade III (lipoatrophy). The mean size of LH in the abdomen was 2.42 ± 0.97 cm, that in the thigh was 2.53 ± 1.13 cm, and that in the arm was 1.6 ± 0.55 cm. The difference in the mean sizes across sites was statistically insignificant (P = 0.306) per one-way ANOVA.
Using t-test for independent samples.
using Pearson's chi-square test.
BMI, body mass index; DM, diabetes mellitus; NS, not significant; S, significant; WHR, waist-to-hip ratio.
Impact of insulin-injecting practices on LH
The prevalence of LH in self-injecting adults was significantly higher than in self-injecting children (P = 0.005). Lack of correct rotation of sites was significantly associated with LH (P < 0.0001). The frequency of LH in patients who used a single needle >5 times was significantly higher than in those using it ≤5 times (P = 0.009). The overall mean TDD was 42.16 ± 17.41 IU. In the LH group, it was 42.87 ± 18.57 IU, whereas in the non-LH group it was 40.37 ± 14.11 IU (P = 0.401). Thus though numerically higher, the difference of means was statistically insignificant. Other injecting practices also showed insignificant difference between the two groups (Table 1).
Associated risk factors of LH
The association of various risk factors with LH was determined by calculating the odds ratio (OR) (Table 2). Univariate analysis (unadjusted OR) revealed that adults had a significantly increased risk of LH than children with an OR 2.16 (95% CI: 1.04–4.51; P = 0.038). Other factors such as gender (female), duration of diabetes >10 years, BMI ≥23 kg/m2, abnormal WHR, and number of injections per day showed marginally increased OR of LH than their respective references, but did not achieve statistical significance. Correct rotation of sites was associated with significantly reduced prevalence of LH (OR: 0.002; 95% CI: 0.0003–0.01; P < 0.0001). Insulin needle usage of >5 times significantly increased the likelihood of LH compared with usage ≤5 times (OR: 3.41; 95% CI: 1.42–8.58; P = 0.009). The effect of significant risk factors on LH was further studied through multivariate logistic regression analysis (adjusted OR). This revealed that all predictors had a statistically insignificant effect on LH, except for rotation of sites. Correct site rotation continued to show significantly reduced risk of LH with an adjusted OR of 0.001 (95% CI: 0.0–0.009; P < 0.0001).
LH, lipohypertrophy; OR, odds ratio.
Clinical implications of lipohypertrophy
The effect of LH, independently and in the presence of demographic and anthropometric parameters, was studied for two outcome variables, GV and UH. Of 139 patients, 115 (82.7%) had GV (Table 3). The adjusted OR in adults was 0.25 (95% CI: 0.07–0.94; P = 0.04), suggesting that children were at higher risk of GV than adults. Furthermore, the adjusted OR for females was 4.23 (95% CI: 1.27–14.09; P = 0.019), indicating a significant increase in the risk of GV for them as compared with males. Subjects with >10 years duration of diabetes were at higher risk (OR: 4.34; 95% CI: 0.95–19.83; P = 0.058) of GV than those with ≤10 years duration. The adjusted OR of GV in LH was 17.65 (95% CI: 5.11–61.03; P < 0.0001), showing significantly increased GV with LH. The adjusted OR linking GV to LH was >10%, indicating substantial influence of covariates in the model.
We performed a similar analysis using UH as an outcome variable (Table 4). Of 139 subjects, 116 (83.4%) had UH. Females showed an increased risk of UH with an adjusted OR of 3.99 (95% CI: 1.15–13.87; P = 0.029). The adjusted OR of UH associated with LH was 28.02 (95% CI: 7.28–107.8; P < 0.0001), showing that LH has a very significant effect on UH. The same influence of covariates in the model applies here as well.
Ambulatory glucose monitoring
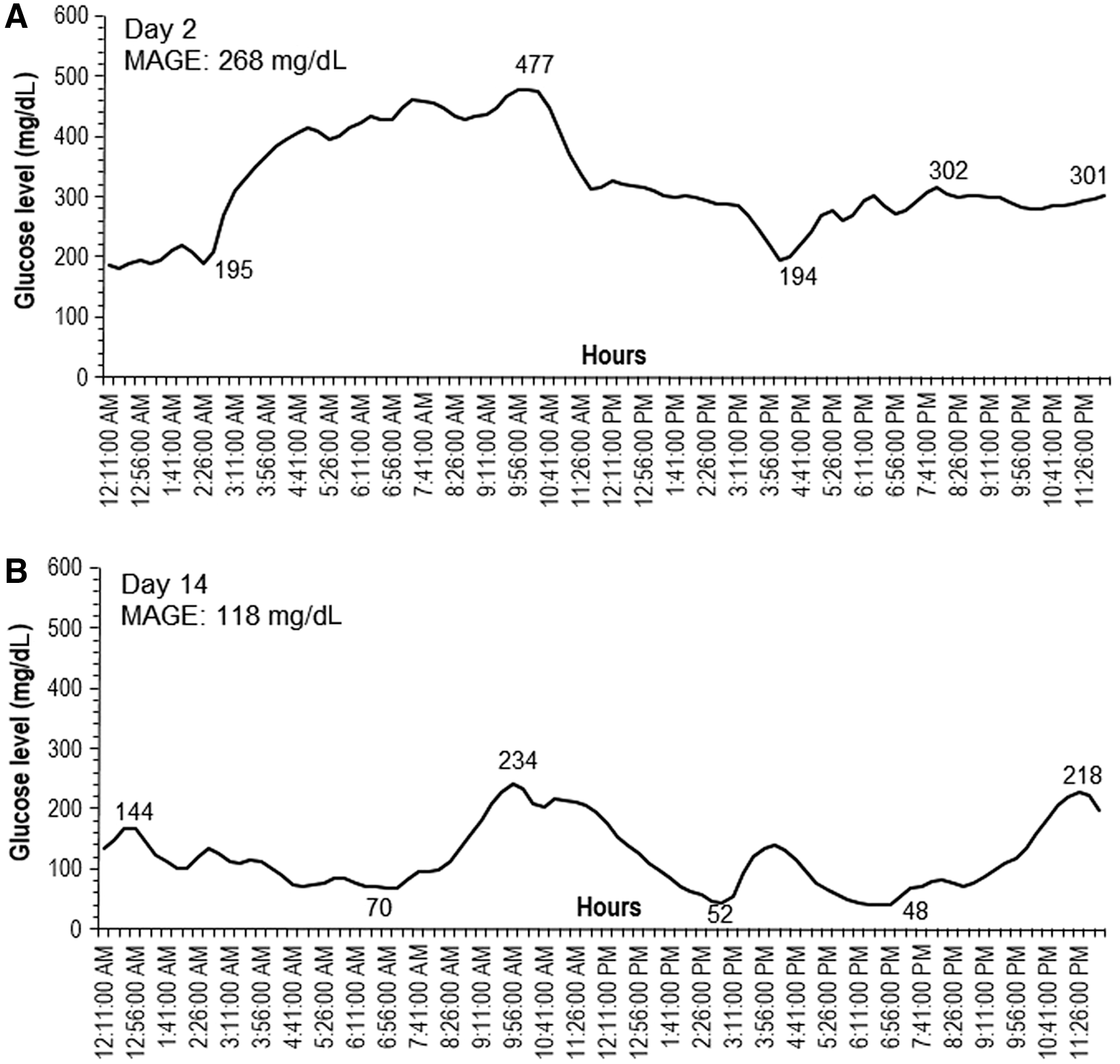
AGP was obtained for 10 (∼10%) subjects having LH to ascertain the GV in such patients. The mean size of LH among these participants was 5.11 ± 3.51 cm. The mean glucose measured by AGP when subjects were injecting insulin into LH sites (first 7 days) was 224.8 ± 76.19 mg/dL, with a median of 214 mg/dL, interquartile range of 102.25 mg/dL, coefficient of variation (CV) of 33.9%, and 10th and 90th percentiles as 134.5 mg/dL and 379.7 mg/dL, respectively. The mean glucose level at normal (non-LH) sites (next 7 days) was 165.40 ± 49.56 mg/dL with a median of 169.5 mg/dL, interquartile range of 80.0 mg/dL, CV of 29.96%, and 10th and 90th percentiles as 82.8 mg/dL and 236.9 mg/dL, respectively. The mean difference between the two sites was 59.4 ± 69.06 mg/dL, which was significantly >0 (P = 0.027). The MAGE data on mean excursions for both the sites were also obtained for each of these 10 patients. The mean MAGE at the LH sites was 216.3 ± 62.97 mg/dL, whereas at normal sites it was 173.7 ± 63.52 mg/dL, a difference that is highly statistically significant (P < 0.0001) (also see tracings in Fig. 2A, B). Moreover, the GV was further studied using CONGA. The estimates were obtained on the 2nd day (injection at LH site) and on the 14th day (injection at non-LH site). The mean on the 2nd day was 196.78 ± 67.6, whereas on the 14th day, it was 98.44 ± 35.58, again a highly statistically significant difference (P = 0.002). Thus, mean glucose, MAGE, and CONGA all supported the OR estimate of GV due to LH.
Discussion
This is the first large hospital-based study on Indian T1DM patients that determined the prevalence of LH and assessed its relevance to GV and UH. The overall prevalence of LH among our subjects was 69.8%, which is close to 76.3% reported by Blanco et al. 9 Cunningham and McKenna 17 in their study on 55 insulin-treated people (41 T1DM and14 T2DM) reported that 51% had LH. de Villiers 18 in his single-center study on 23 T1DM observed LH in 52%. Kordonouri et al. 3 found the LH prevalence to be 47.8% in young T1DM children treated with modern insulin regimens and devices. They also observed a 62% prevalence of grade 1 LH, and 38% of grade 2 LH (using identical definitions as we did), whereas none had lipoatrophy. Similarly, Omar et al. 19 studied 119 T1DM children and identified LH in 54.9%. LH was more common in males (62.7%) than in females (48.4%).
In our study, the prevalence of LH was higher in females than in males (73.4% vs. 66.7%) and adults showed a greater prevalence than children (76.9% vs. 60.6%). As with Kordonouri et al. 3 and Omar et al., 19 our study also found that among subjects with LH, 76.3% had grade I, whereas 23.7% had grade II LH; there was no case of grade III (lipoatrophy). Sawatkar et al. 20 have shown the prevalence of LH to be 41% in their observational study of various cutaneous manifestations among South Asian T1DM subjects. Deng et al., 2 in their systemic review and meta-analysis of 26 studies with a total of 12,493 participants, showed that the pooled prevalence of LH in T1DM was 49%. Frid et al. 21 in a questionnaire-based survey performed in 2014–2015 on 13,289 insulin-injecting patients (with T1DM, T2DM, and pregnancy diabetes) from 423 centers in 42 countries found a self-reported LH prevalence of 29.0%, and 30.8% through physical examination by healthcare professionals. That survey found that LH was seen almost twice as frequently in patients with T1DM as in those with T2DM.
Our study did not find any statistically significant influence of gender, age of onset, duration of diabetes, BMI, WHR, HbA1c, mean number of injections per day, use of human versus insulin analogue, or basal bolus regimen versus premixed insulin use on LH. Other observational studies have reported significant increases in TDD of insulin when injecting into LH sites. 9,19,22 Our data have shown a numerically increased TDD among those injecting insulin into LH sites but this did not achieve statistical significance. That finding could be explained by the overall poor glycemic control in both the groups; HbA1c was nearly 10% in both LH and non-LH groups (Table 1). Cunningham and McKenna 17 also did not observe any statistically significant difference in TDD between LH and non-LH groups.
Although the prevalence of LH was higher in our subjects using the arm, this was statistically insignificant compared with other sites. Omar et al., 19 however, found LH more frequently in the arms than in the thigh or abdomen. That study also showed that the type of insulin, number of injections per day, frequency of changing the needle, and delivery of insulin through injections were not significantly associated with LH. Similarly, Blanco et al. 9 observed that the LH prevalence did not differ significantly by gender, use of pens versus syringes, needle length, frequency of injections, and insulin analogue use. Cunningham and McKenna 17 also did not find significant differences in the prevalence of LH as regards to TDD and the length of the needle. Other studies have found that patients with LH had significantly higher HbA1c values, more daily insulin injections, and longer diabetes duration. 3,9,17 In one study, LH was also found to be higher among females and people with higher BMI. 23
Vardar and Kizilci 1 observed that the length of time insulin had been used, the frequency of changing injection sites, and the frequency of changing needles had a statistically significant influence on the development of LH. In our study, correct rotation of sites is shown to significantly reduce the risk of LH. Syringe needle usage of >5 times significantly increased the risk of LH as compared with usage ≤5 times, although the observation was different for pens. This might be due to fewer number of pen users (n = −47) versus syringe users (n = 92) (Table 1). Blanco et al. 9 found that LH was more prevalent among those who reused needles (P < 0.05), especially when the needle was used more than five times. Saez-de Ibarra and Gallego 24 and Chowdhury and Escudier 6 have also reported the lack of correct rotation of injection sites as an independent risk factor for LH.
Cunningham and McKenna 17 showed the association of lack of rotation of injection sites, high number of injections per day, and longer duration of insulin use with LH. Strauss et al. 8 observed that incorrect rotation of injection sites, use of smaller injection zones, longer duration of insulin use, and the reuse of pen needles were associated with LH. Our data did not show any significant relationship between LH and the duration of diabetes or the number of injection per day. Importantly, multivariable modeling of our data unmasked a negative relationship between injection frequency and the presence of LH, highlighting even more the importance of site rotation.
Ours is one of the few studies to show a statistically significant association of LH with GV and UH. These observations could be due to defective absorption and changes in pharmacodynamics of insulin at LH sites. Females showed a significantly increased risk of GV and UH. Blanco et al. 9 found that the rates of frequent UH and GV were more than six to seven times higher in patients with LH (39% vs. 6%) than in those without LH (P < 0.01). Of those with LH, 39.1% had UH and 49.1% had GV compared with only 5.9% and 6.5%, respectively, in those without LH (P < 0.01). They further found that 92% of these patients with UH and 93% of those with GV had LH.
Our data have also observed that 95.9% of subjects with UH and 93.8% with GV had LH. Strollo et al. 22 have also shown a higher risk of UH and GV among T1DM patients with LH. Another study showed an increased risk of GV and UH in LH, with the absorption of insulin aspartin LH having a 25% lower Cmax. The study's authors speculated that this might be due to local degradation of insulin in the LH tissue. 25 Famulla et al. 5 conducted a crossover trial on 13 patients with T1DM. Subjects were given subcutaneous abdominal injections of insulin lispro into LH and normal adipose tissue (NAT). They also performed euglycemic clamp study with two injections each into LH and NAT, and on another day, one injection per region was given before a standardized mixed meal (75 g carbohydrates), all in randomized order. They demonstrated reduced insulin absorption and blunted action with injection at LH site, leading to profound deterioration in postprandial glucose control.
Earlier studies have also shown that the absorption of Neutral Protamine Hagedorn (isophane) insulin, as determined by plasma-free insulin, was significantly lower in LH. 26 Similarly, the absorption of regular insulin in LH was found to be delayed, as determined by the clearance of 125I-insulin. 27 From these studies it was concluded that the differences were of sufficient magnitude to be of clinical importance. 26,27 Barola et al. 28 published a case report on insulin-mediated LH, an uncommon cause of diabetic ketoacidosis, which is due to poor absorption of insulin at LH sites.
Our subgroup study quantitatively assessed GV through significant changes in mean BG, MAGE, and CONGA using AGP for 2 weeks, with subjects injecting insulin into LH sites for the first 7 days and thereafter into non-LH sites for the next 7 days. The data has shown a significant decrease in mean glucose values after injecting insulin into non-LH sites as compared to the values after injecting insulin into LH sites. Notably, a study using continuous glucose monitoring system to monitor fluctuations of BG documented a significant correlation between the mean of daily differences of glucose and the severity of LH at injection sites. 29
Strength and limitations of the study
There is scanty data available on LH in T1DM from Southeast Asia. The strength of our study is that it is the first in India with significant number of T1DM participants, which has shown GV and UH as two important clinical consequences of LH. Moreover, by using AGP it has addressed the improvement in GV after proper rotation of injection sites; however, we recruited only 10% of the subjects in this exercise, a limitation of the study. This was due to limited resources, budget constraints, poverty, poor health awareness, and lack of insurance support in developing countries like India, which makes providing healthcare challenging. Second, the study was carried out in a single tertiary care center, although one with a good patient representation from central and southern regions of India. From an analytic perspective, multiple testing comparisons were not performed across various parameters, another limitation of the study.
Conclusion
There is a high prevalence of LH among people with T1DM in India. Improper rotation of sites and reuse of insulin syringes are the leading causes of LH, which, in turn, significantly increases the risk of GV and UH, both of which can be of serious clinical concern. The increase in mean glucose, MAGE, and CONGA when injecting insulin into LH sites, as documented by AGP, shows that we should focus our messages on this inadequately addressed medical disorder. It is important not only to diagnose LH but also to give patients simple and practical advice on how to detect and/or prevent it.
The authorities in developing South Asian countries need to focus on this message and design strong programs on injection technique awareness. They should use the various guidelines such as those published by the Forum for Injection Technique, Indian Recommendations. 30 The clinical benefits of detection and intervention in LH would include lowering of its prevalence and better control over GV and UH. These together may help to reduce the risk of associated morbidity and mortality rates. Economically, it might reduce the risk of hospitalization and the overall direct and indirect costs of the treatment and may improve the quality of life. In short, emphasizing continuous education on injection technique guidelines is one of the more pressing needs of the hour.
Footnotes
Acknowledgments
The authors thank Dr. Dhananjay Raje for statistical analysis support; Juvenile Diabetes Parent's Organization of India (JDPAI) for organizing type 1 diabetes camp; Sunil's Diabetes Care n' Research Centre Pvt. Ltd. for subject recruitment; and Dr. Kenneth Strauss for reviewing the article.
Authors' Contributions
Dr. Sunil Gupta wrote the article and Mrs. Kavita Gupta, Dr. Sachin Gathe, Mr. Shlok Gupta, and Mrs. Parvinder Bamrah were involved in screening support and data entry.
Author Disclosure Statement
No competing financial interests exist.