
Abstract
Background:
To improve insulin pump therapy results, a special test for patients was devised. The model successfully used to achieve a license to operate different machines was followed.
Methods:
The test (a practice and a full run, with a time limit) contained 42 questions, each with four optional choices, and could be answered online. Patients could familiarize themselves with the whole question pool first. Patients could repeat a full run attempt if they failed and were offered focused remedial education. The study group composed of adults, 46 females, and 54 males, all treated for type 1 diabetes, 38/100 newly introduced to insulin pump therapy.
Results:
Eighty-five of 100 patients successfully completed their first full run attempt (80% or higher correct answers) and 3 of 100 on their second full run attempt; 12 of 100 patients were not able to succeed. The median of the test score was 2 mistakes (range 0–17 mistakes). The most problematic topics were diet and insulin regimens and their application. The crucial factor influencing the test score was the willingness to try practice run(s). Those who practiced had a significantly higher total test score with better results in 5 of 8 tested knowledge domains. Age and diabetes existing >15 years had an impact on the result, too. Both patients' and caregivers' opinions on the test were predominantly positive (or neutral).
Conclusions:
The type of test introduced is a good tool for checking a patient's theoretical knowledge and indirectly revealing a patient's level of motivation.
Introduction
O
When we are looking at a large type 1 diabetes mellitus (T1DM) registry of data (e.g., the T1D Exchange Clinical Registry examining the overall state of metabolic control and current use of advanced diabetes technologies in the United States), it is clear that considerable room remains for improving outcomes of treatment of T1DM across all age groups and all treatment modalities. 3
Of the Czech Republic's 10 million citizens, almost 1 million persons are treated for diabetes, mostly type 2 diabetes mellitus. Fifty-six thousand patients are reported to have T1DM; several thousands of them are treated by CSII. Our Diabetology Centre (DC), which is a part of the Department of Internal Medicine at the University Hospital Motol, is one of the largest diabetology centers for adults in the Czech Republic. Improvement in glycated hemoglobin (HbA1c) is observed after introducing CSII, but despite extensive education, most patients do not reach the recommended HbA1c and/or other target values. Similar data are reported from other centers. 4 Together, the national data (nationwide as well as local) are consistent with the experience indicated from other countries.
The basic premise for this study is that the CSII therapy has underused potential, and its main task is to determine how therapeutic strategy could be improved.
For this reason, a special test for insulin pump users was prepared, which is described in detail in the Methods section. The test is based on one of the books recommended for ongoing self-study of the patient at home. 5 From the test results, the patient's education was personalized by offering extra educational session(s), focusing on the problems a patient encountered during a training phase (attempts at sitting a practice run, described below). The test can be completed on a printed version or accessed on a web page and can be repeated. In our strategy, we followed a model that has been successfully used for many years to achieve a license to operate different machines such as a car or even an aircraft.
Each patient receiving a new insulin pump from our DC is strongly encouraged to complete the test successfully. CSII therapy in the Czech Republic is free of charge for patients fulfilling the defined indication criteria. (Details are mentioned in the Discussion section.) Therefore, improving the outcomes from this therapy is desirable from an individual (higher QOL) as well as a collective point of view (improving patients' health translates into lower usage of healthcare services due to the reduction of diabetes complications).
The article studies this method, with a special focus on revealing the factors that influence the test's results. A related and important question is whether educational outcomes vary between different patient subgroups.
Methods
The testing tool is based on Moodle (Modular Object-Oriented Dynamic Learning Environment), an interactive platform used mainly for teaching and testing students at many universities. 6 Two frameworks were prepared, one for a practice run and one for a full run. The difference between a full run and a practice run lies in the test duration and the shortest possible time interval between each trial. The time limit given for completing a full run is 60 min, whereas a practice run has no time limit. If a full run is failed, another attempt can be made after 1 week, but the time interval between practice runs is not limited.
The test (a practice run and a full run) contains 42 questions with four answer options. The test covers eight domains, specified in Table 1. Each domain has its own question pool comprising 10–32 questions. The algorithm creates a test by randomly picking five questions from each of the eight question pools (except for domain 5 diet, which is covered by seven questions). The answer options are always given in a random order. A patient can study all the questions before attempting the test, even during the practice run test; a full question set is available online or as a hard copy. The patient is also provided with all the possible answers to each question (this includes marking the correct one). Passing the full run successfully (minimum is 80% correct answers) lets patients print a certificate confirming that they are sufficiently prepared to use an insulin pump. The test and the set of all questions are available on the Diabetes Association of the Czech Republic website, at
CGM, continuous glucose monitoring.
Study group
The study group included 46 females and 54 males, all treated for T1DM. Their basic characteristics are summarized in Table 2.
BMI, body mass index; CSII, continuous subcutaneous insulin infusion; DCCT, Diabetes Control and Complications Trial; MDII, multiple daily insulin injections.
Thirty-eight patients were newly introduced to CSII therapy. These patients underwent at least one structured education session (for beginners) led by a diabetologist from our DC plus repeated training sessions with a representative of the company whose device the patient selected (focused on handling the pump). In 62 of 100 cases, the test was administered to patients receiving a new device after 4 years. These patients underwent a structured education session as well (modified for experienced insulin pump users) and a practical training with a company representative was provided only if a new type of the pump was prescribed. Note that patients approved for CSII therapy each receives new device every 4 years in the Czech Republic, when the indication for CSII is re-evaluated. In 36% of cases, patients were treated outside our DC and were referred only to start or restart and supervise CSII treatment.
During each visit, patient's glucometer and insulin pump are downloaded. Mean glucose and glycemia variability (calculated as standard deviation—SD) were obtained from the newest glycemia or continuous glucose monitoring (CGM) profiles. Additional patient information is summarized in Table 3.
DM, diabetes mellitus.
Statistical analyses
Data were analyzed by SPSS software, v.24. Testing for data normality has shown that data cannot be considered normally distributed. Due to this fact, the comparison of two groups was realized by using Mann–Whitney U test and correlation analysis was done by using Spearman's correlation test. Selecting concrete thresholds for creating different groups for group comparisons is described below. The significance threshold was set to 0.05.
Results
Test results: overall result evaluation
Of 100 patients, 85 were successful (80% and more correct answers) on their first full run attempt. The median of the test score was 2 mistakes per 42 questions (range 0–17 mistakes). Twenty-one patients achieved a score of 100% on their first attempt. Three patients succeeded on their second attempt, 10 patients finished the full run test but failed (their test score was below 80%) and were not able to pass a full run successfully (despite remedial education). Two patients did not finish their full run attempt. Patients who succeeded completed their full run test in the range of 15–58 min (median of the attempt duration was 35 min). The median of the attempt duration for those who did not reach the threshold was 40 min (range 20–60 min).
The most difficult topics were domains 2 (insulin regimens and their application) and 5 (diet). Conversely, questions about basal dose adjustment (domain 7) posed minimal problems.
Influence of diabetes-related characteristics
Patients were split into two groups, using an A1c threshold of 70 mmol/mol (8.6% according to the Diabetes Control and Complications Trial (DCCT)). This threshold was selected because if patients wished to continue with CSII therapy, one of the criteria they had to fulfill was to achieve HbA1c below that threshold. Surprisingly, patients with a higher HbA1c scored better in domain 2 (insulin regimens and their application; P = 0.007), which may indicate their higher level of motivation and greater efforts at studying this topic.
Patients having higher glucose variability (glycemia SD >3.5 mmol/L resp. 63 mg/dL) made significantly more mistakes in topics diet P = 0.02 and bolus doses P = 0.049. These patients had higher mean glucose as well, but this difference was not significant.
No significant differences were observed when patients receiving the insulin pump for the first time were compared with experienced insulin pump users as well as when different reasons for starting/continuing CSII therapy were analyzed.
We did not observe the influence of hypoglycemia(s) but this reason for starting/ongoing CSII therapy was present only in six patients. During the follow-up phase, two cases of severe hypoglycemia were reported.
Patients who had suffered diabetes for a shorter period scored better. The difference was mainly prominent when the threshold was set to 15 years of diabetes duration. Patients who had been treated for diabetes for more than 15 years had a worse overall test score (P = 0.014) and found questions in domains 2 (insulin application and insulin regimens) and 3 (introduction to insulin pump therapy) significantly more challenging (P = 0.028 and P = 0.008, respectively).
Patients already suffering from chronic microvascular complications had a better overall score (P = 0.008), but the converse was evident, specifically in domain 8 (CGM and handling special situations), where all patients with no microvascular complications had 0 mistakes (P = 0.002).
The influence of the presence of comorbidities (hypertension, dyslipidemia, etc.) was not observed.
When patients were split according to total insulin dose per kilogram (within the recommended values and above, respectively), patients with an appropriate insulin dose scored better in domain 3 (introduction to insulin pump therapy; P = 0.012) and, unsurprisingly, had a lower body mass index (BMI) (P = 0.044) compared with patients with a higher insulin dose. All patients who scored 100% had an appropriate total insulin dose per kilogram (e.g., ≤0.5 IU/kg).
Forty-five patients selected a pump capable of CGM signal receiving, 17/45 of these patients use CGM frequently (>21 days per month), others occasionally, mostly prior control visits in the hospital. The reasons for low frequency of CGM use include mainly financial reasons, alarm fatigue, and sensor inaccuracy. On the contrary, of 55 patients who selected a pump incapable of CGM signal receiving over this fact, 7 patients use CGM frequently (2 of them continuously) with a smart phone as a receiver. One frequent CGM user succeeded until his second attempt. Other frequent CGM users scored well but they had significantly better results only in the domain no. 5 (diet; P = 0.01). They did not differ in age or education, but within frequent CGM users men prevailed (20 males and 4 females).
Results were not significantly different when patients treated in our DC were compared with patients who were sent to the hospital from a private diabetologist only for insulin pump indication evaluation, (remedial) education, and therapy supervision.
Influence of personal characteristics
Patients were split into three groups according their age (<30 years and ≥30 years but <50 years and ≥50 years), and results (aggregated as well as in single domains) were compared within these groups. Younger patients scored higher, which was mainly prominent in domains 5 (diet; P = 0.032) and 7 (basal doses; P = 0.008).
The test results were not influenced by a patient's sex or BMI. Surprisingly, the effect of a patient's level of education was also negligible, and no influence from living arrangements was observed. The patient's general health and related behavior expressed as experience with addictive substances (cigarettes, alcohol, cannabis, etc.) were also of interest.
The crucial factor influencing the test score was the willingness to attempt practice run(s). Exactly 50% of patients (n = 50) tried the practice run at least once. The median of the number of practice run sessions was 1, the mean was 4 (3.96 exactly). One patient finished 28 training sessions (maximum), but this case was, of course, an outlier excluded from the statistical analysis. Those who practiced by themselves had a significantly higher total test score (P = 0.014; Fig. 1A) with better results, prominently in domains 4, 5, 6, 7, and 8 (insulin pump operation P = 0.049, diet P = 0.004, bolus doses P = 0.008, basal doses P = 0.034, and CGM and handling special situations P = 0.016, respectively). Patients who practiced were unsurprisingly able to finish the full run in a shorter time (P = 0.049; Fig. 1B). These cooperative patients did not have any specific characteristics (generally or related to diabetes).
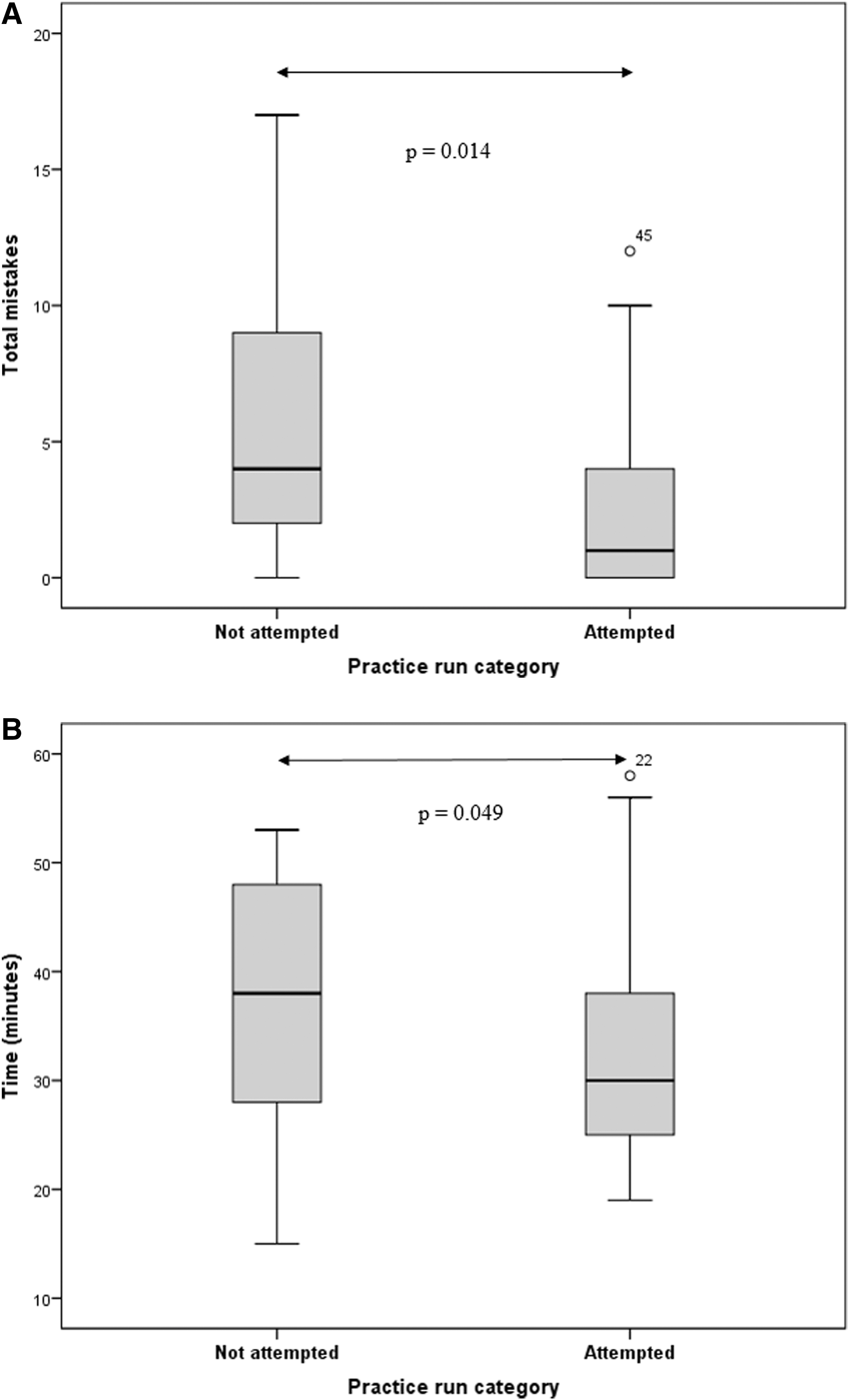
The positive effect of self-training (attempting practice run tests).
Patient's and caregiver's opinions of the test
Patients were willing to cooperate, and we did not encounter problems with test administration. In an anonymous opinion survey, patients expressed positive or neutral attitudes about the test. The survey was completed by 63 patients who mainly appreciated that the test could be repeated and that there was no maximum limit for attempting full runs. The reaction of caregivers (other doctors, nurses, relatives) was also positive with one exception only.
Discussion
In different countries, the ratio of patients treated with CSII and the magnitude of financial self-participation in this therapy is not the same.
Health insurance in the Czech Republic covers 100% of CSII costs (with the exception of glucose sensors), and access to insurance is provided to all Czech citizens under the Constitution. CSII prescription is restricted to diabetology centers that cooperate with local private diabetologists. Defined indication criteria for CSII therapy must be fulfilled and approval from the insurance company medical specialist for this therapy is required.
According to the national register established at the initiative of the Czech Diabetology Society (CDS), 4383 patients (87.9% with T1DM) are treated with CSII. 4 Data from this register show improvement of HbA1c after introducing insulin pump therapy, but still only a small number of patients achieve the therapeutic goals (e.g., an HbA1c below 53 mmol/mol, 7% according to DCCT, with low glycemia variability and no severe hypoglycemia) despite a standardized education (specified in CDS treatment standard for insulin pump therapy). 4,7 This observation is consistent with data reported from other countries, with the conclusion that barriers to more effective use of current treatments need to be addressed. 3
To improve the therapeutic outcomes of our patients, a test was devised to help stimulate patients to learn and reveal their knowledge deficiencies.
As the test is universal (not made for a specific pump type), the practical skills of patients were checked (handling an insulin pump) during the routine educational process. As mentioned in the Introduction, a model was followed that has been successfully used for many years to achieve a license to operate different machines such as a car or even an aircraft. To receive a driver's (pilot's) license after theoretical and practical training, everyone must take a knowledge-based test and prove practical skills with machine handling. The pool of questions is known in advance so all possible questions can be studied before taking the test. In our test, the complete set of questions is also given to patients in advance. 8
Patients agreed to the implementation of this strategy of insulin pump training, and nobody found the approach to be restrictive or unfair. On the contrary, not everyone completed the anonymous opinion survey. For healthcare professionals, the explanation of the system to patients is not very time-consuming (written instructions for patients are available) and they were satisfied with it. Moreover, some time may be saved when education process is focused according to patient's needs.
The median of time of full run attempts indicates that the time limit was set appropriately, and patients were not under duress for time when taking the full run.
We were not surprised that one of the most problematic topics was diet. Questions related to diet were accompanied by meal photography (when suitable to the question's context). We focused on carbohydrate counting and the estimation of a meal's effect on glycemia (glycemic index). Accuracy of carbohydrate counting is a big challenge in diabetes education. Quite recently, a study was published reporting 59% accuracy in carbohydrate counting in a group of adult patients, 9 which corroborates our experience. A more surprising fact was that questions about insulin regimens and application were also problematic. This topic and diet are considered fundamental, and patients are instructed in these from the beginning. These results indicate that in remedial education, basic knowledge must be repeated. Conversely, both patients newly introduced to CSII and experienced patients were well prepared regarding knowledge associated with insulin pump handling and basal dose adjustment.
Surprisingly, test results were not influenced by an individual's characteristics, as we expected. We observed a negative impact due to older age. Unfortunately, as we grow older, many aspects of our cognitive functioning show age-related declines. 10 The effect of other characteristics on an individual's results was negligible. A big survey of university students searching for predictors of successful outcomes suggests that our primary assumption was wrong (except for age). In that study, a student's success was not significantly connected to an individual's characteristics (gender or social origin) and the best predictor for the probability of graduating, and the final grade obtained at university was the final high school grade. 11
Regarding diabetes-related factors, patients with a worse HbA1c scored better in one of the two most problematic domains (insulin application and insulin regimens). It is known that persons with higher HbA1c before beginning CSII show greater HbA1c improvement. 1 This observation may demonstrate a greater effort to improve in patients with worse results. Also, it may be speculated that greater efforts to study due to an already poor experience with diabetes may explain better the overall test score in patients suffering from microvascular complications.
We did not observe the effect of the experience with severe hypoglycemia but it may be due to the fact that severe hypoglycemia(s) was not a frequent cause to start/continue insulin pump therapy. Surprisingly, this is an agreement with data from the national register of patients treated with an insulin pump where this indication is not among the three most common ones. 4
In the Czech Republic, patients can select from different types of insulin pumps, only tubeless devices are not available yet. They can select even a pump capable of CGM signal receiving if they wish and fulfill indication criteria. According to our internal survey, patients use CGM more and more but still not enough for different reasons. In our study, patients who use CGM frequently (>21 days per month) were mostly younger men who have irregular daily activities and who travel a lot (businessmen, etc.). They were unsurprisingly able to better handle questions regarding diet but they were not superior in other topics. With exceptions, they did not practice and they were very confident about their knowledge.
Diabetes duration was analyzed in relation to the test results, and a threshold after which patients began to score worse was sought. This was determined as 15 years of diabetes duration. It may be consistent with the aforementioned influences due to age, but it may also indicate the time horizon after which patients are at higher risk of developing burnout syndrome and they are not so open to new treatment options and cooperation. Not only caregivers (professionals or family members) are at risk of developing burnout. Patients suffering chronic diseases can also develop burnout syndrome, and these patients cannot be expected to improve therapeutically without first resolving psychological problems. 12,13 In absolute agreement with this statement is the observation that a clear predictor of test success was the willingness to try practice run(s) and discuss problematic areas with doctor(s) or nurse(s). The willingness to cooperate was linked to patients' current life situation and also to their personality type. Patients who practiced did not differ in HbA1c or other values, which may indicate that they are cooperative but their previous education was not for some reason sufficient enough (meaning education at the time of diagnosis, etc.).
It was demonstrated how a patient's personality type influenced compliance with using a medical device. This compliance was, of course, directly connected to therapeutic success or failure. 14 Fortunately, there are techniques for working with persons having different personality types. 15
Now we are trying to overcome some limitations and improve our testing schema. We are expanding the pool of questions and we are preparing a standardized practical part of the examination. The tubeless insulin pumps will be available in the Czech Republic soon, so we plan to add questions related to this topic as well. It would be useful to prepare different language versions (at least English one, for foreign patients living in our country) and in co-operation with pediatric diabetologist to adapt the system for children and their parents. If professionals from other countries will be interested in our idea, it is possible to start work on an international version of the system reflecting national differences. We would like to implement a gamification strategy into the practice run as well.
We conclude that this type of test is a good tool (which can be of course improved further) to check a patient's theoretical knowledge and indirectly, but efficiently, reveal a patient's level of motivation. We consider it to be the final component of a very intensive process of introduction of people to use of CSII (or change of a pump model).
Footnotes
Acknowledgment
Supported by the Czech Ministry of Health Project No.15-25710A (P08 panel).
Author Disclosure Statement
The authors declare that there is no conflict of interest.