
Abstract
Background:
The purpose of this study was to compare the efficacy and safety of intensive insulin therapy (premixed insulin lispro vs. insulin glargine) in patients with type 2 diabetes mellitus (T2DM).
Methods:
MEDLINE, EMBASE, the Cochrane Library, and
Results:
A total of 13 RCTs and 5401 patients were included in this study. In parallel trials and crossover trials, premixed insulin lispro was found to be superior to insulin glargine at reducing glycosylated hemoglobin (HbA1c) (parallel trials: weighted mean difference [WMD] −0.18%; 95% confidence interval [CI] −0.31 to −0.06; P = 0.004; crossover trials: WMD 0.37%; 95% CI −0.51 to −0.23; P < 0.00001). Premixed insulin lispro resulted in more weight gain than insulin glargine (parallel trials: WMD +0.64 kg; 95% CI +0.14 to +1.15; P = 0.01; crossover trials: WMD +0.74 kg; 95% CI +0.19 to +1.29; P = 0.009), and premixed insulin lispro was associated with a higher risk of hypoglycemia than insulin glargine (parallel trials: odds ratio [OR] 1.20; 95% CI 1.06–1.36; P = 0.005; crossover trials: OR 2.24; 95% CI 1.45–3.46; P = 0.0003).
Conclusions:
Premixed insulin lispro provides a larger reduction in HbA1c and is associated with a significantly higher risk of hypoglycemia and greater weight gain in patients with T2DM. These findings may be helpful in selecting therapy for individual subjects.
Introduction
D
For patients with T2DM, basal insulin (e.g., insulin glargine U-100, detemir, isophane, degludec, glargine U-300) and premixed insulins (usually protamine combined with a rapid-acting insulin analog) are two of the major forms of therapy. If glycemic control is not reached, a gradually increasing mealtime insulin dose is added. 5 Premixed insulin is a combination of short-acting or fast-acting insulin and intermediate-acting insulin, for example, insulin lispro mix (LM)75/25, 75% insulin lispro protamine suspension with 25% insulin lispro injection or LM50/50, 50% insulin lispro protamine suspension with 50% insulin lispro injection. Most clinicians consider basal bolus insulin therapy with four injections per day to be a gold standard for reaching the goal of glycemic control. 6 Other clinicians prefer to use a premixed insulin as the initial form of insulin therapy due to its relative ease of use, requiring fewer injections and less frequent use of glucose monitoring.
Our aim was to determine whether there is a benefit of using insulin glargine compared with LM50/50 or LM75/25 in terms of HbA1c control, weight gain, and hypoglycemia in patients with T2DM who were either insulin naive or had intensified insulin therapy for a better glycemic control. We conducted a meta-analysis of all randomized clinical trials (RCTs) that met the predefined admission criteria.
Methods
Data sources and searches
A search for “insulin glargine,” “glargine, insulin,” “insulin lispro,” “premixed insulin lispro,” “diabetes mellitus, type 2,” “diabetes mellitus, noninsulin-dependent,” and “randomized controlled trial” was performed in MEDLINE (PubMed), EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL) to identify RCTs published through December 1, 2017. In addition, completed but still unpublished trials were identified through a search of the
Study selection
Two reviewers (D.S. and X.Z.) independently reviewed the documents retrieved from the databases according to the inclusion criteria. Any discrepancy was resolved by the two reviewers through discussion.
Data extraction and quality evaluation
A meta-analysis was performed including all trials with a duration of 24 weeks that enrolled patients with T2DM and compared premixed insulin lispro with insulin glargine. This duration was chosen based on the fact that the therapeutic effect of HbA1c may require several weeks to occur. The baseline characteristics of the studies included in the present meta-analysis were extracted, including the publication data (title, first author, year), study design, baseline characteristics of the participants of the studies (sample size, drop out, age, HbA1c level, body mass index [BMI]), intervention, treatment duration, and primary outcome measures (change from baseline to study endpoint for HbA1c, body weight, and incidence of hypoglycemia). The risk of bias tool of the Cochrane Library was used to assess the quality of the literature.
Statistical analyses
The weighted mean difference (WMD) with the 95% confidence interval (CI) for continuous variables and the odds ratio (OR) with the 95% CI for dichotomous outcomes were calculated. P < 0.05 represented a statistically significant difference. Heterogeneity was assessed using I 2 statistics. Heterogeneity was considered to be I 2 > 50%. The size of heterogeneity determined whether a fixed- or random-effects model was used for the analysis. All statistical analyses were performed with the Review Manager statistical software package (version 5.3).
Results
Study characteristics and methodological quality
We identified 13 eligible studies (Supplementary Fig. S1; Supplementary Data are available online at
Glycosylated hemoglobin control
Analysis of the data from the studies that compared the efficacy of premixed groups with glargine groups in parallel trials (random-effects model) showed that treatment with premixed groups led to a significantly greater change in HbA1c levels from baseline (WMD −0.18%; 95% CI −0.31 to −0.06; P = 0.004), and the difference was statistically significant (Fig. 1). In crossover trials (fixed-effects model), HbA1c levels were significantly reduced in premixed groups compared with glargine groups (WMD −0.37%; 95% CI −0.51 to −0.23; P < 0.00001). The differences were also statistically significant (Fig. 1).
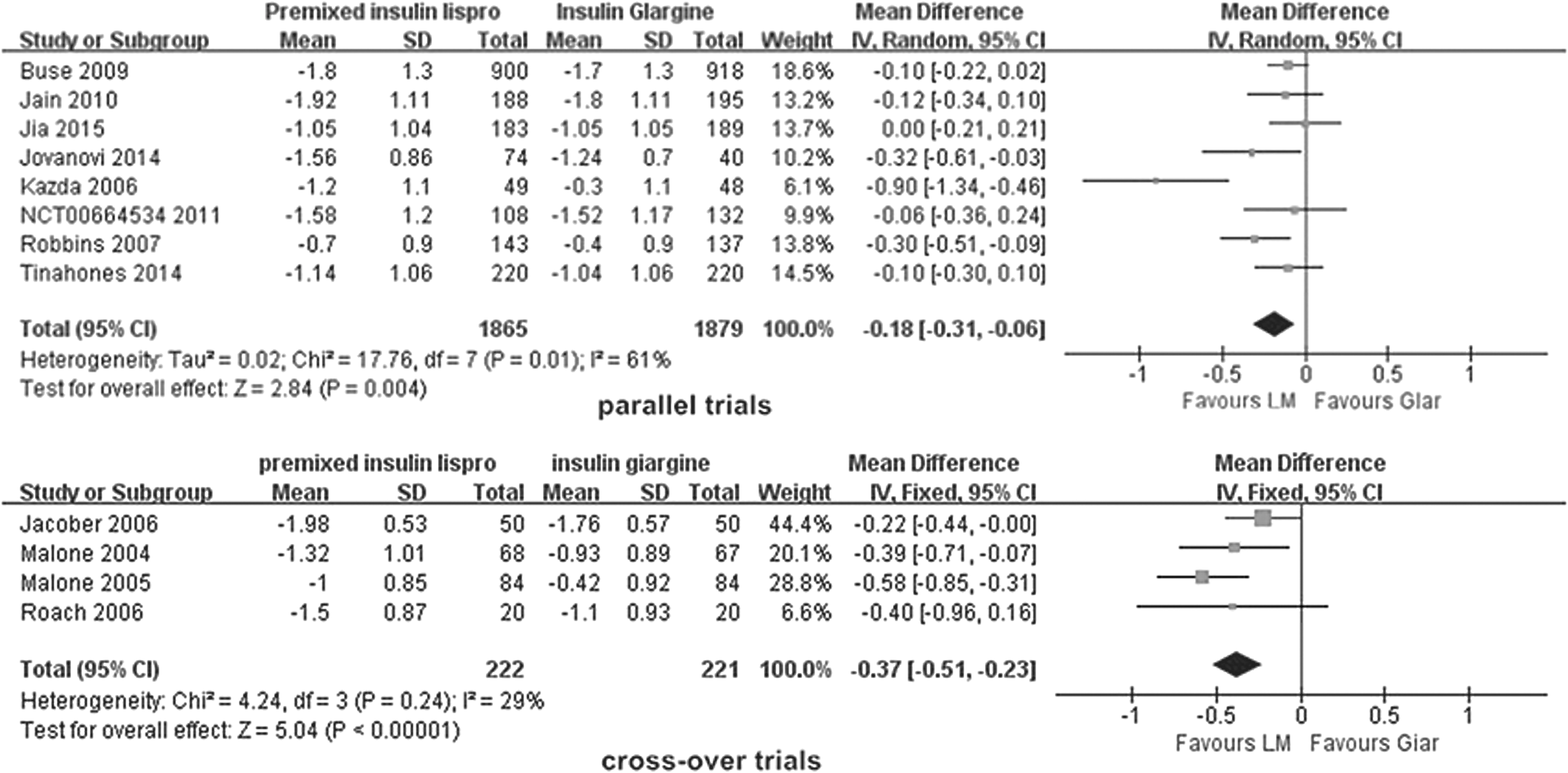
WMD in change in HbA1c for premixed insulin lispro versus insulin glargine. Glar, insulin glargine; HbA1c, glycosylated hemoglobin; LM, premixed insulin lispro; 95% CI, 95% confidence interval; SD, standard deviation; WMD, weighted mean difference.
Weight gain
Both the premixed and glargine groups showed an increase in body weight. However, the premixed groups had greater weight gain than the glargine groups in parallel trials (WMD 0.64 kg; 95% CI 0.14–1.15; P = 0.01) (Fig. 2). Similarly, the premixed groups showed greater weight gain than the control group in crossover trials (WMD 0.74 kg; 95% CI 0.19–1.29; P = 0.009) (Fig. 2).
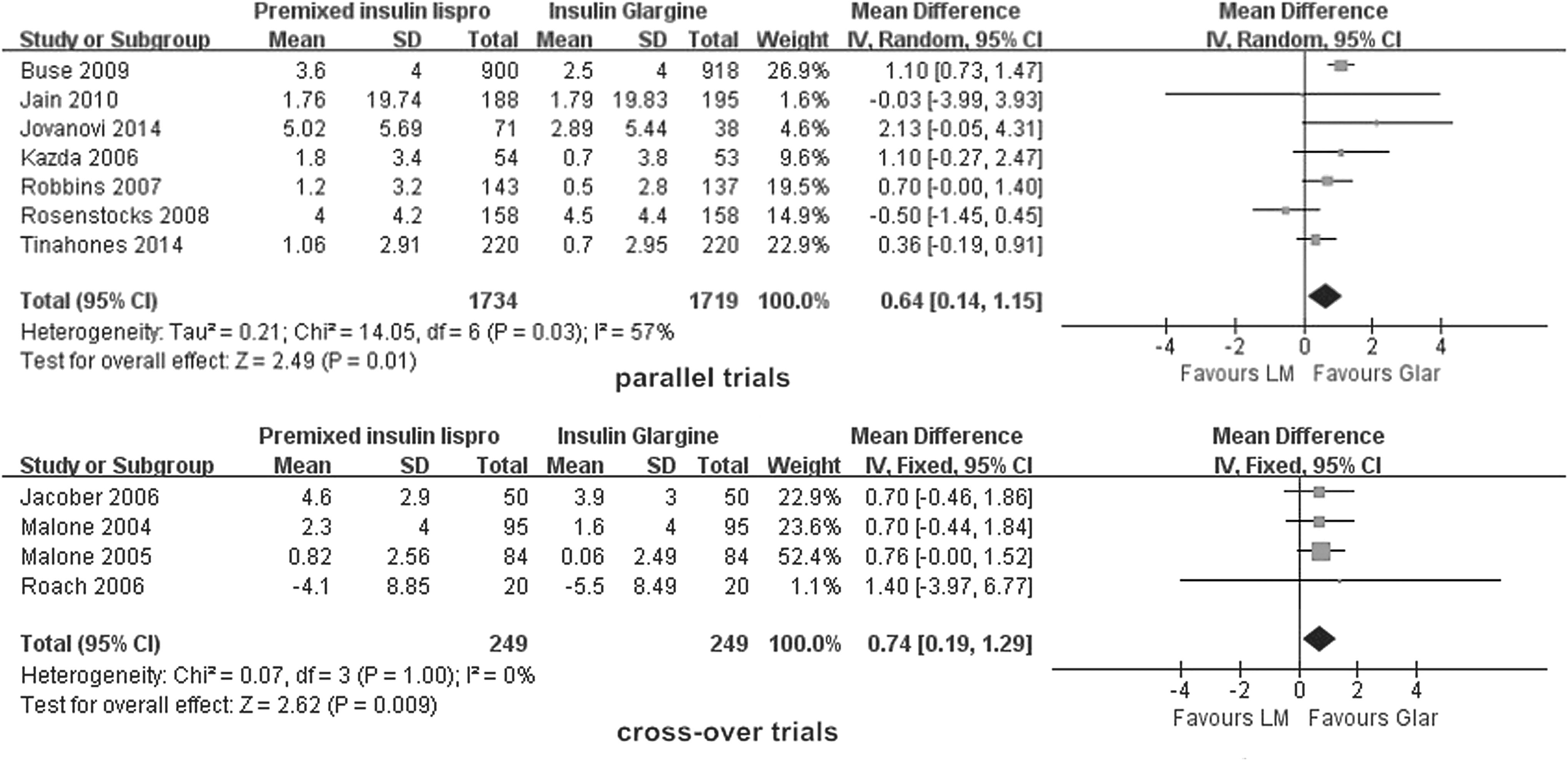
WMD in weight gain for premixed insulin lispro versus insulin glargine.
Hypoglycemia
The total number of hypoglycemia cases was 2667 (1392 and 1275 in the premixed groups and glargine groups, respectively) for a total of 4931 patients (2451 and 2462 in the premixed and glargine groups, respectively). The collected Mantel-Haenszel odds ratio (MH-OR) for parallel trials was 1.20 (95% CI 1.06–1.36; P = 0.005). The incidence of hypoglycemia in the premixed group was higher than that of the glargine group, and the difference was statistically significant (Fig. 3). Crossover trials showed a significantly greater increase in the incidence of hypoglycemia in the premixed group compared with the glargine group (Fig. 3). The collected MH-OR for crossover trials was 2.24 (95% CI 1.45–3.46; P = 0.0003).
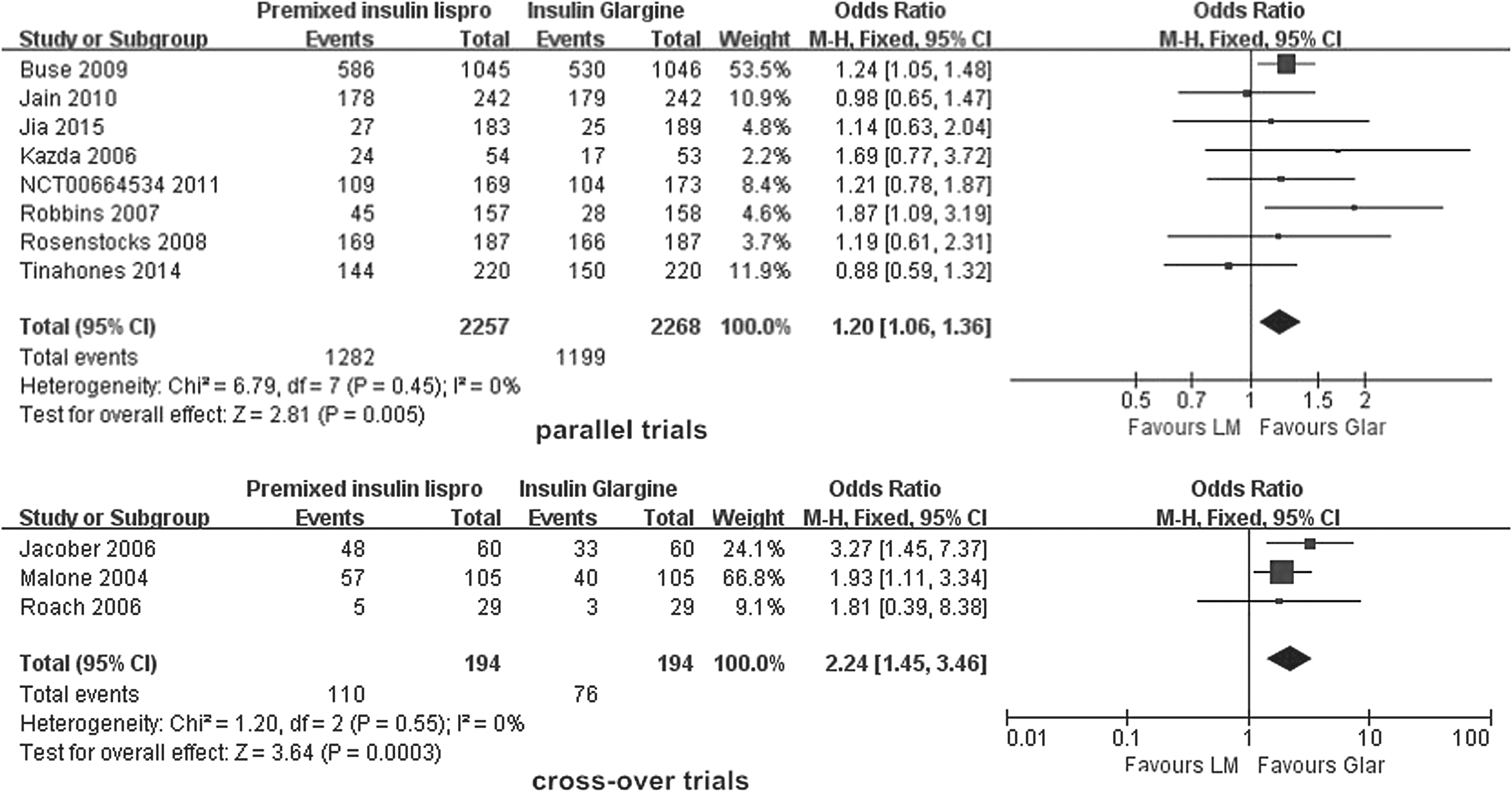
OR in hypoglycemia incidence for premixed insulin lispro versus insulin glargine. OR, odds ratio.
Discussion
This meta-analysis incorporates research trials designed for multicenter studies. Patients' ethnicities included Asians, Latinos, and Afro-descendants, making the results of the meta-analysis universal for all of the above ethnic groups. This meta-analysis contained a total of 13 RCTs comparing the effects of insulin glargine and premixed insulin lispro on HbA1c, body weight, and hypoglycemia in T2DM (Supplementary Table S2).
The meta-analysis included in the study design was divided into crossover trials and parallel trials. Each subject in the crossover trial was self-controlled, eliminating variability among subjects and facilitating the screening of the best interventions. 20 The main problem with the crossover trial was the inability to handle the carryover effect, which is described as the long-lasting effects of the intervention given over a period of time that will persist into the next stage and may affect the efficacy of follow-up interventions. 21 The Cochrane Handbook clearly states that, in principle, crossover trials can be combined with parallel trials in the same meta-analysis. However, it is important to consider that there may be differences in other important characteristics of different types of tests. It is suggested that meta-analyses of parallel and crossover trials be carried out separately.
This study performed a combined analysis assuming that the treatment effects of LM50/50 and LM75/25 belonged to the same premixed insulin lispro, but the short-acting insulin and intermediate-acting insulin had a different proportion of ingredients. To compare the two effects, we referred to Zafar et al. 22 A total of 146 patients were enrolled in this study. Group A received LM50/50, and group B received LM75/25. The results showed that LM50/50 better reduced HbA1c levels and FPG levels. However, there was no significant difference between the two groups with regard to weight change or the incidence of hypoglycemia. Farcasiu et al.'s 23 study noted that there was no difference between the two groups with regard to the reduction in HbA1c levels and the incidence of hypoglycemia, although the LM75/25 induced better effects on weight change and reducing FPG levels. Few studies have compared the efficacy of LM50/50 and LM75/25, and therefore, large-sample, multicenter clinical trials are needed to confirm the difference in efficacy between the two treatments.
Overall, eight pooled studies 11 –13,15 –19 showed that the premixed group was superior to the glargine group at reducing HbA1c levels in parallel trials (P = 0.004). However, there was a large amount of heterogeneity among the eight parallel trials (P = 0.01; I 2 = 61%), and sensitivity analysis revealed that the heterogeneity mainly came from Kazda et al.'s 12 study. The reason for the heterogeneity in Kazda et al.'s study may be because there was no combination of OADs in the two groups, while the other studies included a combination of OADs, which may have affected the treatment's efficacy in the two groups to a certain extent. After removing study heterogeneity, the difference was still statistically significant (WMD −0.13%; 95% CI −0.20 to −0.05; P = 0.0009; I 2 = 2%). In the crossover trial, four pooled studies 7 –10 showed less heterogeneity (I 2 = 29%), and the premixed group was superior to the glargine group in reducing HbA1c levels. There was no heterogeneity in hypoglycemia for the crossover and parallel trials (I 2 = 0%), and premixed groups were associated with a higher risk of hypoglycemia than insulin glargine groups (parallel trials: P = 0.005; crossover trials: P = 0.0003). These results were consistent with most available systematic reviews 24,25 comparing basal insulin and premixed insulin, which have shown that compared with basal insulin, premixed insulin is associated with better glycemic control but also a higher risk of hypoglycemia.
In terms of body weight, the results of seven studies 12,13 –18 in parallel trials showed that there was a statistically significant difference between the two groups (P = 0.01). The premixed groups experienced greater weight gain than the glargine groups, and the results were heterogeneous (P = 0.03; I 2 = 57%). Sensitivity analysis revealed that the heterogeneity mainly came from Rosenstock et al.'s 14 study, possibly because the baseline weight of the patients in that study was significantly greater than that in other studies. The results of the meta-analysis remained unchanged after the sensitivity analysis was performed to exclude the sources of heterogeneity, indicating that the analysis results were very robust (WMD 0.83 kg; 95% CI 0.46–1.20; P < 0.0001; I 2 = 25%). This result was also confirmed in Rys's study, 26 which analyzed 2639 patients in three articles. The results showed a lower mean body weight gain in patients who received glargine+OAD than in patients who received premixed insulin+OAD.
However, the available systematic reviews 6,27 showed that HbA1c levels, hypoglycemia, and weight gain were not significantly different between basal bolus and premixed insulin regimens. This result may be because the two articles included several types of basal insulin (insulin glargine and insulin detemir) and premixed insulin (Humulin 70/30, Novo Mix 30, Aspart30, and so on). These studies did not consider the complexity of insulin therapy, and the treatment effect of different insulins on the disease was not the same, which significantly limited the accuracy of the conclusions.
It is worth noting that although our study found statistically significant differences between the premixed group and the glargine group with regard to HbA1c and body weight, the differences were small. Small changes in HbA1c and body weight are not important in diabetes treatment. More attention should be paid to the occurrence of hypoglycemia. Hypoglycemia can increase the risk of death from cardiovascular disease by four times in T2DM patients, and severe hypoglycemia can increase the risk of Alzheimer's disease in older T2DM patients. 28 The results of this study show that premixed insulin lispro is associated with a significantly higher risk of hypoglycemia; therefore, users of premixed insulin should pay close attention to the occurrence of hypoglycemia.
Conclusions
In summary, for T2DM, premixed insulin lispro is better at reducing HbA1c levels, with a higher risk of hypoglycemia and a higher extent of weight gain. Both premixed insulin lispro and insulin glargine have advantages regarding clinical efficacy and safety in patients with T2DM. These findings may be helpful in adapting treatment to individual patient needs.
Footnotes
Acknowledgments
The authors are thankful for the help of the doctors and nurses at the Nursing Teaching and Research Department of the First Affiliated Hospital of Liaoning University of Traditional Chinese Medicine.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.