
Abstract
Background:
Continuous glucose monitoring (CGM) provides glucose trend information that can be used to guide treatment and motivate patients with diabetes. Currently, the evidence on effectiveness of CGM in patients with type 2 diabetes is debatable. We aim to provide a systematic review and meta-analysis to synthesize current evidence of effectiveness of CGM in adults with type 2 diabetes.
Materials and Methods:
Cochrane, Embase, PubMed, and Web of Science were searched to include all studies that reported effectiveness of CGM in terms of HbA1c in adults aged 18 and older, with type 2 diabetes, on any treatment for diabetes. Heterogeneity (I 2) was used to determine the variability between studies. All data were analyzed using Review Manager 5.3 software.
Results:
Seven randomized controlled trials and three cohort studies, involving 1384 patients for real-time CGM (RT-CGM) and professional CGM (P-CGM) and 4902 patients for flash glucose monitoring (FGM), were included. RT-CGM and P-CGM were associated with a modest but statistically significant reduction in HbA1c of 0.20% (95% confidence interval [CI] −0.31 to −0.09) compared with control. Patients who received FGM had a nonsignificant reduction of 0.02% (95% CI −0.07 to 0.04) compared with control. The meta-analysis indicated a low heterogeneity between studies.
Conclusion:
Our analysis of current evidence suggests that RT-CGM and P-CGM are effective in improving HbA1c in adults with type 2 diabetes. Due to insufficient evidence, it is premature to form conclusions on the effectiveness of FGM. Future multicenter trials accessing the effectiveness of CGM as well as safety and cost-effectiveness may be necessary.
Introduction
T
The CGM system has a body sensor that is inserted subcutaneously to measure glucose levels in the interstitial fluid of the patient. Depending on the device, the transmitter wirelessly sends glucose values to a receiver as often as every 5 min. The CGM data can be used to treat and prevent hypoglycemic and hyperglycemic episodes and encourage lifestyle modifications in patients. The American Diabetes Association currently recommends CGM in patients with hypoglycemia unawareness and/or frequent hypoglycemic episodes. 4
Professional CGM (P-CGM) and real-time CGM (RT-CGM) are available. RT-CGM provides real-time data with high and low glucose alerts to the patient. 5 In contrast, real-time data are masked to the patient using P-CGM and are retrospectively evaluated by the clinician. Both devices require fingerstick calibration by the patient at least twice a day. Education and training are required to integrate information into treatment decisions and to prevent adverse events.
Recently in 2017, another variety of CGM system, FreeStyle® Libre Flash (flash glucose monitoring [FGM]), was approved in the United States by the U.S. Food and Drug Administration (FDA) for adults older than 18. FGM is significantly different from other CGM because it provides glucose values for the previous 8-h period only on scanning, does not give glucose alerts, and is factory callibrated. 3,6 Since no fingerstick calibration is needed, FGM provides greater convenience to the patient and avoids errors related to the calibration. It is also lower in cost compared with other CGM.
Currently, the effectiveness of CGM in patients with type 2 diabetes on reduction of HbA1c level is not consistent. Meta-analysis studies have been conducted in the past, which reported a reduction in HbA1c in patients who received RT-CGM and P-CGM. 7,8 However, the results were based on older evidence from a few randomized controlled trials (RCTs). Since the time of publication, larger studies have been conducted using more advanced CGM technology, and not all studies reported significant improvement in glycemic control. Also, no previous meta-analysis studies have been conducted on effectiveness of FGM in improving HbA1c. Due to inconsistent results between studies and the recent approval of FGM, we performed a systematic review and meta-analysis to synthesize current evidence of effectiveness of the CGM systems in terms of improving HbA1c measures in adults with type 2 diabetes.
Materials and Methods
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement. 9 All included studies received informed consents and ethics approval from their respective institutions.
Search strategy and study selection
A comprehensive search for literature was conducted through databases, including Cochrane, Embase, PubMed, and Web of Science. The controlled vocabulary and keywords used in the search were diabetes mellitus, glycated hemoglobin A, CGM, FGM, blood glucose monitoring, and ambulatory glucose profile. The detailed search strategy is reported in Supplementary Table S1.
Identified articles were initially screened for relevance to research question by title and abstract. Full text was retrieved for relevant studies and reviewed further for exclusion criteria (Fig. 1).
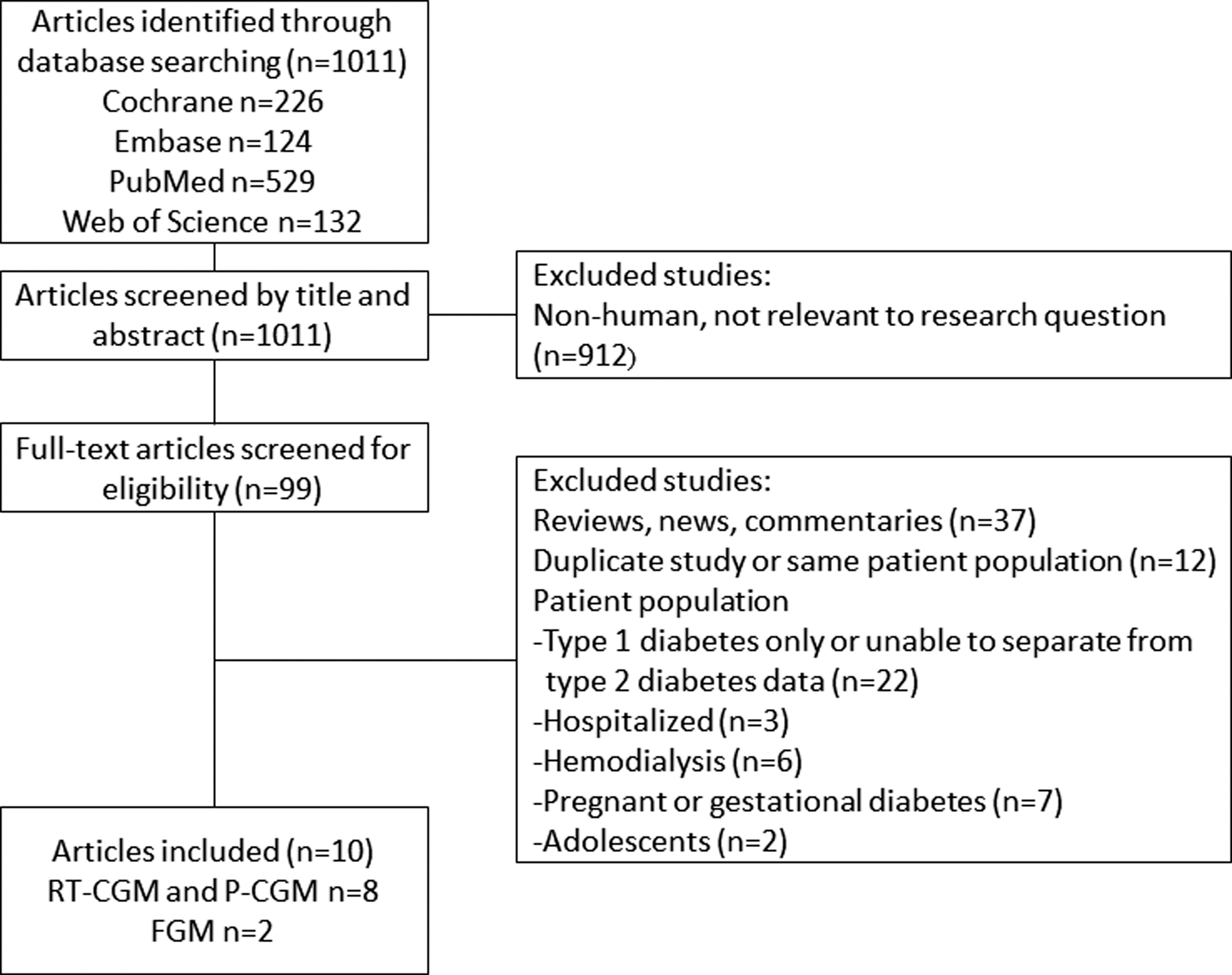
Study selection process.
Selection criteria
RCTs and observational studies that reported change in HbA1c in the CGM and control groups were considered for review and analysis. Included patient populations were adults aged 18 and older with type 2 diabetes on any treatment for diabetes such as lifestyle modifications, oral hypoglycemic agents, insulin therapy, and combination therapy. Exclusion criteria were duplicates, reviews, news, commentaries, and studies that included the following patient populations: type 1 diabetes or unable to separate from type 2 diabetes data, pregnant or gestational diabetes, neonatal and adolescents, hemodialysis, and hospitalized or critically ill (Fig. 1). No studies were excluded based on study size, publication year, and geographic location.
Data extraction
Data were collected from individual studies for sample size, study duration, country, device manufacturer, baseline patient characteristics (age, gender, and insulin use), inclusion and exclusion criteria, change in HbA1c from baseline, and other outcomes (adverse effects, blood pressure, body mass index [BMI], weight, exercise time, and changes in hypoglycemic agents).
Assessment of risk of bias
The Cochrane risk of bias tool was used to appraise the quality of research methods of RCTs based on random sequence generation, allocation concealment, blinding of participants, data collectors and outcome assessor, bias due to selective outcome reporting, percentage of total population who were lost to follow-up, intention-to-treat analysis, and source of study funding (Supplementary Table S2). 10 The Newcastle–Ottawa Scale was used to appraise the quality of research methods of observational studies. 11 There were a maximum of four stars that can be earned in the category of selection, two stars in comparability, and three stars in outcome (Supplementary Table S3).
Statistical analysis
The meta-analysis was conducted for RT-CGM and P-CGM studies and for FGM studies. The outcome was change in HbA1c from baseline in treatment and control groups. Heterogeneity (I 2) was used to determine the variability between studies. I 2 values of 25%, 50%, and 75% were assigned low, moderate, and high heterogeneity, respectively. 12 Potential publication bias was evaluated by funnel plot. All data were analyzed using Review Manager 5.3 software. 13
Results
Search results
The initial search from databases identified 1011 potentially relevant studies. Of these, 912 articles were removed for being irrelevant to research question. Further excluded articles were reviews, news, and commentaries (37), duplicates (12), and studies that included the following patient populations: type 1 diabetes or unable to separate from type 2 diabetes data (22), pregnant or gestational diabetes (7), adolescents (2), hemodialysis (6), or hospitalized (3). Six RCTs and two cohort studies that used P-CGM and RT-CGM were included for review and analysis (Fig. 1). For the analysis of FGM, one RCT and one observational study were included.
Study and patient characteristics
The details of the included studies are provided in Table 1. Studies were published between 2008 and 2017 in North America (3), Europe (2), and Asia (5). Study duration ranged from 8 to 32 weeks. Devices used were Dexcom™ SEVEN®, Dexcom™ G4 Platinum, iPro®2, Medtronic™ MiniMed, GlucoDay®, Guardian® RT, and FreeStyle® Libre. All trials reported change in HbA1c as a primary outcome.
AGP, ambulatory glucose profile; BG, blood glucose; BMI, body mass index; BP, blood pressure; CGM, continuous glucose monitoring; CI, confidence interval; DQOL, Diabetes Quality-of-Life Questionnaire; DTSQ, Diabetes Treatment Satisfaction Questionnaire; FBG, fasting blood glucose; FGM, flash glucose monitoring; PBG, postprandial blood glucose; P-CGM, professional CGM; RT-CGM, real-time CGM; SD, standard deviation; SMBG, self-monitoring blood glucose.
The pooled sample size of all included studies that used RT-CGM and P-CGM was 1384, of which 574 patients received the intervention and 810 patients were in the control. The mean age was 56.8 years, and 65.2% of subjects were males. Patients on insulin therapy with or without other hypoglycemic agents were 65.5%. The pooled sample size of RCTs only was 426 patients with 213 patients who received CGM and 213 patients for the control. The mean age was 58.5 years, and 49.4% of subjects were males. Patients on insulin therapy with or without other hypoglycemic agents were 62.0%.
For FGM, the pooled sample size of all included studies was 4902, of which 2488 patients received the intervention and 2414 patients were in the control. The mean age was 57.3 years, and 61.4% of subjects were males. Patients on insulin therapy with or without other hypoglycemic agents were 69.1%.
Glycemic control
Patients who received RT-CGM and P-CGM had a significantly greater reduction in HbA1c compared with the control group in all studies and in RCTs only. The standardized mean difference (95% confidence interval [CI]) was −0.20 (−0.31 to −0.09) in all studies and −0.33 (−0.52 to −0.13) in RCTs (Figs. 2 and 3). There was a low heterogeneity between studies as measured by I 2. The I 2 value for all studies was 8% and for RCTs was 3%. The funnel plot did not show asymmetry (Fig. 4).
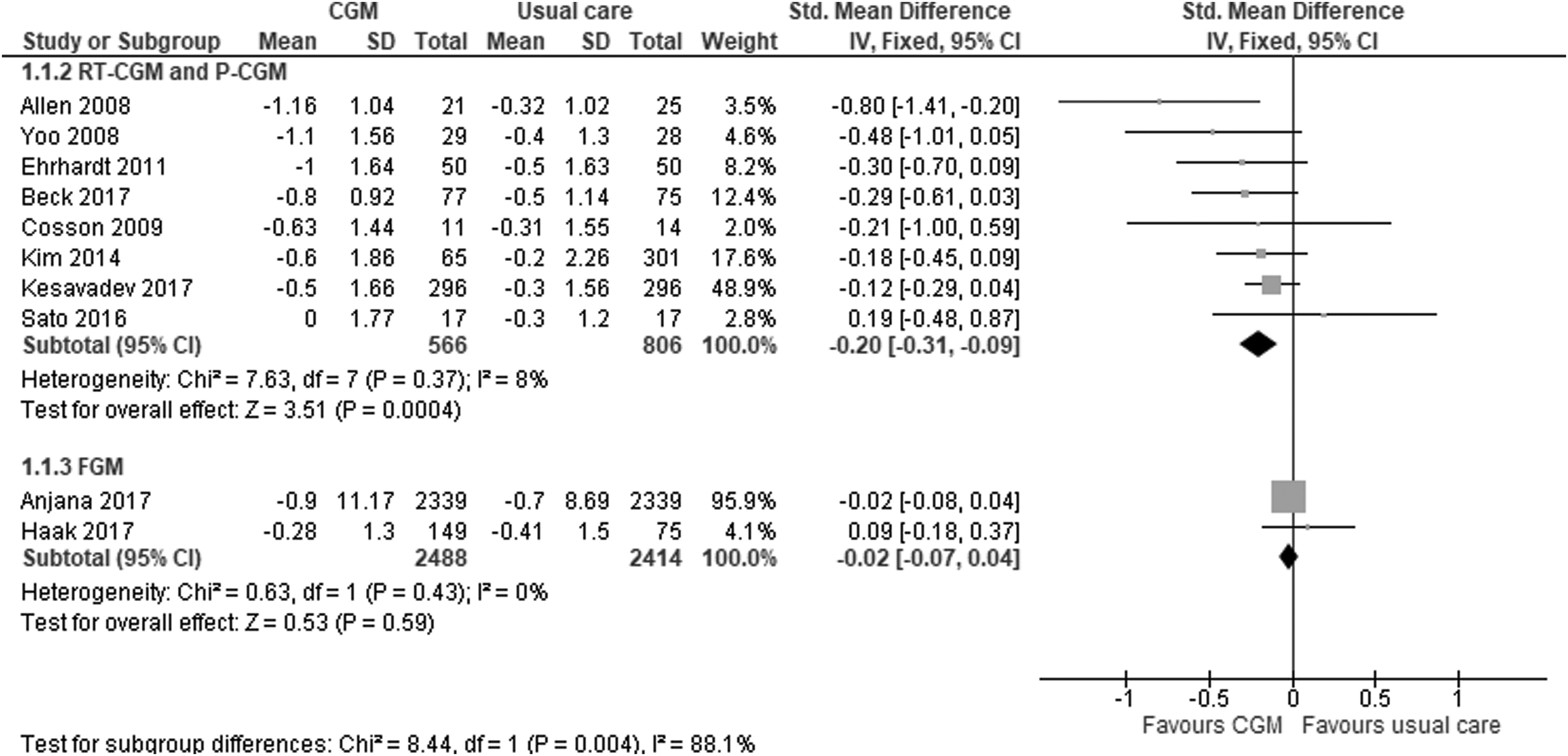
Analysis of all studies. The forest plot demonstrating a significantly increased reduction in HbA1c from baseline associated with the RT-CGM and P-CGM use and a nonsignificant reduction for FGM. CGM, continuous glucose monitoring; FGM, flash glucose monitoring; P-CGM, professional CGM; RT-CGM, real-time CGM.

Analysis of randomized controlled trials only. The forest plot demonstrating increased reduction in HbA1c from baseline associated with the RT-CGM and P-CGM use and a nonsignificant reduction for FGM.
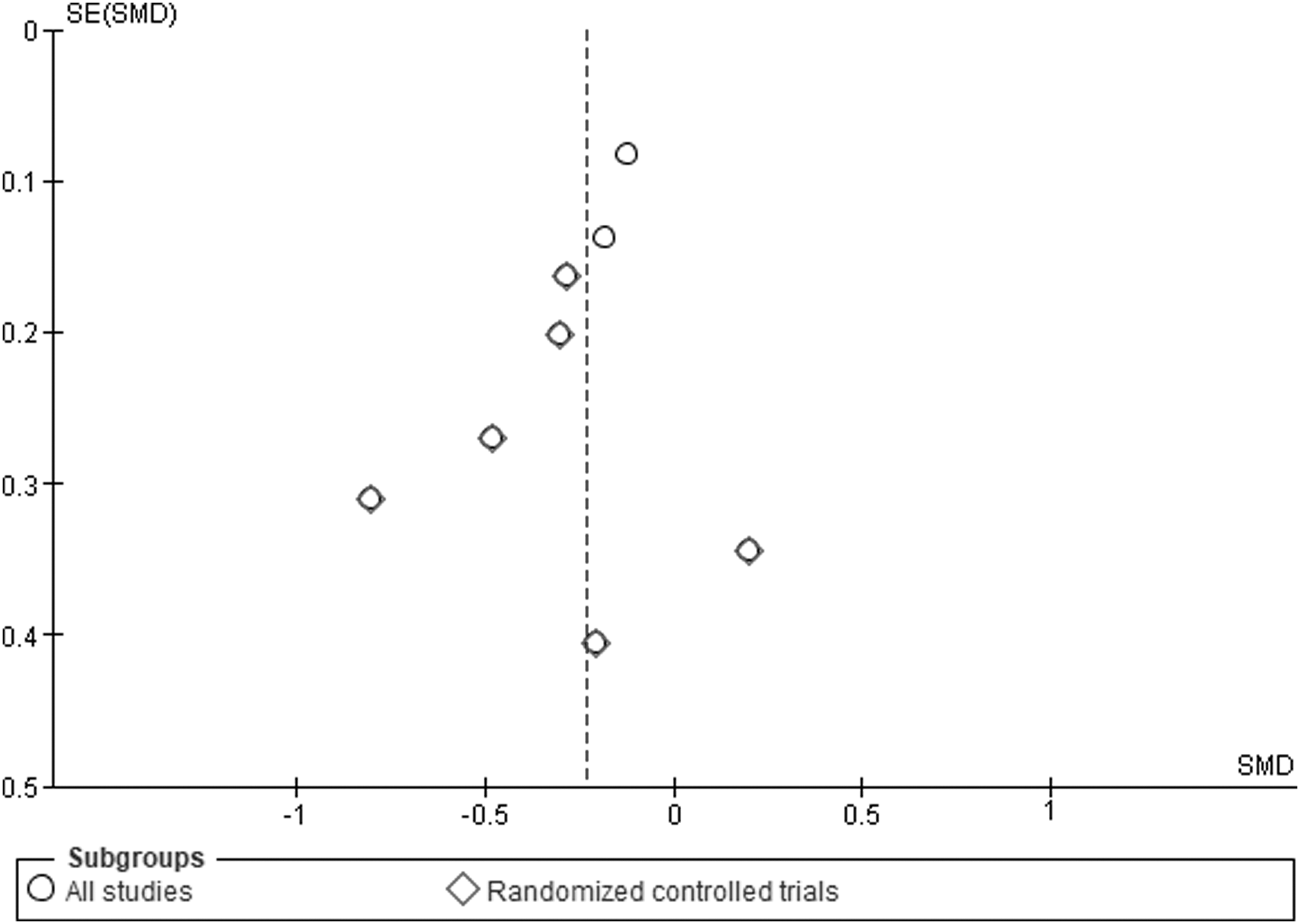
The funnel plot of RT-CGM and P-CGM studies demonstrating no evidence of publication bias.
Patients who received FGM had a nonsignificant reduction in HbA1c compared with the control group. The standardized mean difference (95% CI) was −0.02% (95% CI −0.07 to 0.04) in all studies (Fig. 2). There was no statistical evidence for difference between studies as measured by I 2 (0%).
Due to insufficient data and heterogeneity of outcome assessment and reporting, the meta-analysis of other criteria for assessing the quality of glycemic control was not conducted. Therefore, these outcomes, including time in range, time in hypoglycemia, time in hyperglycemia, and glycemic variability, are provided in Supplementary Table S4.
Adverse effects
No severe hypoglycemic episodes were observed in patients who received any type of CGM device. 14 –17 Patients who experienced implantation site skin reactions using RT-CGM were 0% and 5.8% in the study by Yoo et al. and Cosson et al., respectively. 15,16 Reported skin reactions required no specific treatment and resolved without complications. Four percent of patients who received FGM reported sensor-adhesive reactions that were treated with topical medications. 17
Other outcomes
The meta-analysis of the secondary outcomes was not conducted due to heterogeneity of outcome assessment and reporting.
Two observational studies reported significantly more changes in the treatment modality in the P-CGM group compared with control. 18,19 The authors suggested that the CGM data allowed clinicians to make more changes in the patient's therapy, which resulted in better glycemic control. However, three studies, including one that used FGM, did not show significant changes in hypoglycemic agents in the intervention group compared with usual care. 20 –22
In two RCTs, clinicians used the CGM data to counsel patients on the benefits of physical activity in glycemic control. A significant increase in the physical activity time was observed in the intervention group compared with the control. 16,22 Yoo et al. reported a significant increase in exercise time from 188.2 to 346.6 min/week in the intervention group (p < 0.01) and a nonsignificant change in the control. 16 Allen et al. reported an increase of 5.48 min/day in the intervention group (p < 0.05) and a nonsignificant change in the control. 22
Studies reported inconsistent results in the reduction of blood pressure, BMI, and weight associated with the CGM use. 16,21,22
Discussion
Summary of results
The effectiveness of the CGM system was evaluated by 10 studies, of which seven were RCTs. Each study reported a reduction in HbA1c from baseline as a primary outcome. The meta-analysis of all participants showed a modest but statistically significant reduction in HbA1c in the CGM group compared with the control group. However, the patients who received FGM did not have a statically significant reduction in HbA1c. Majority of the participants who received CGM experienced no severe hypoglycemic events and minor skin reactions related to the device.
Strengths and limitations
The current meta-analysis has important strengths, including high consistency between studies as measured by I 2 and an analysis of all relevant RCTs, which provide the highest level of evidence. Multiple databases were searched to identify all studies relevant to research question. Three of the included studies were observational. However, the overall analysis of all studies reported similar results. According to Shrier et al., including observational studies in addition to RCTs in a meta-analysis can increase precision. 23
Some of the limitations were that included RCTs had small sample size and a short-term follow-up. Different CGM devices were used in the studies, but the subjects were instructed to calibrate using a fingerstick to prevent inaccurate readings. Also, the patients and clinicians were not blinded. However, this was necessary to assess the effect of disclosing CGM data to guide treatment and motivate patients. Not all studies reported tolerability and adverse effects of CGM to assess its safety.
In our analysis, we combined RT-CGM and P-CGM data. Although they are different types of CGM, RT-CGM was used for a limited period ranging from 48 h to 14 days per cycle in all studies except Beck et al. 14 After intervention, the CGM data generated by P-CGM were used by clinicians to adjust therapy and motivate patients throughout the study duration of 8 to 32 weeks. When used for a short period of time, the differences between RT-CGM and P-CGM would not be likely significant. In addition, separating P-CGM from RT-CGM data in all studies did not significantly change the results in our analysis. The standardized mean difference (95% CI) was −0.39 (−0.65 to −0.12) in RT-CGM studies and −0.29 (−0.5 to −0.08) in P-CGM studies (Supplementary Figs. S1 and S2).
There are other criteria for assessing the quality of glycemic control, including time in range, time in hypoglycemia, time in hyperglycemia, and glycemic variability. 24 Due to insufficient data and heterogeneity of outcome assessment and reporting, our analysis was limited to the reduction in HbA1c.
Comparison with other studies
The results of this meta-analysis, which supports the use of RT-CGM and P-CGM, were consistent with previous studies that were published in the past. 7,8,25 In 2011, Gandhi et al. included only three studies and reported a significant reduction in HbA1c of 0.70% in adults with type 2 diabetes using CGM compared with SMBG. 8 Another meta-analysis of four studies reported 0.31% reduction in HbA1c in adults with type 2 diabetes who received CGM. 7 Both of these studies did not include FGM. More recently in 2017, Taylor et al. published a systematic review of nine RCTs and three observational studies that assessed for HbA1c reduction as well as lifestyle and behavioral changes with CGM. 25 The study supported the use of CGM to promote glycemic and weight control and lifestyle modifications in adults with type 2 diabetes. However, they did not perform a meta-analysis due to high heterogeneity of interventions and outcomes of the included studies. With the inclusion of recent studies on RT-CGM and P-CGM that assessed glycemic control, our analysis showed a significant reduction in HbA1c of 0.20% in all studies and 0.33% in RCTs only.
No previous meta-analysis studies have been conducted on effectiveness of FGM in improving HbA1c. Our analysis of two studies showed a nonsignificant reduction in HbA1c of 0.02%. In the past, trials have shown that FGM is effective in improving short-term glycemic measures. 17,26 Bolinder et al. 26 conducted an RCT in 239 adults with well-controlled type 1 diabetes in Europe. Compared with control, the intervention group that used FGM daily had a significant reduction in hypoglycemia, which was defined as glucose levels below 70 mg/dL. At 6 months, the difference in adjusted means was −1.24 h/day, which was 38% reduction in the intervention group (p < 0.0001). This result was consistent in another study that included patients with type 2 diabetes. 17 According to our analysis, however, the long-term impact on HbA1c was not improved with FGM use. This may be due to lack of real-time data and alerts in FGM or due to the reduction in hypoglycemia that can affect HbA1c levels.
Clinical implications and future studies
Our analysis of current evidence suggests that RT-CGM and P-CGM are effective in improving HbA1c in adults with type 2 diabetes. Due to insufficient evidence, it is premature to form conclusions on the effectiveness of FGM in lowering HbA1c. CGM data provide glucose trend information as well as high and low values that can be used to guide treatment and motivate patients. The findings of this systematic review and meta-analysis can be used to assist clinicians in optimizing therapy for patients with type 2 diabetes.
Currently, not many high-quality studies reporting the effectiveness of CGM in reducing HbA1c are available. Also, the data on safety and cost-effectiveness of CGM are limited. Therefore, future multicenter trials accessing these outcomes may be necessary.
Footnotes
Acknowledgment
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.