
Abstract
Aims:
The aim was to evaluate the effectiveness of sensor-augmented pump therapy with predictive low-glucose suspend function (SAP-PLGS) in real-world use in children and adults with type 1 diabetes (T1D).
Methods:
Patients with T1D treated with the MiniMed 640G® pump with PLGS function at three referral hospitals were retrospectively evaluated. HbA1c at baseline and at 6, 12, 18, and 24 months was analyzed. Two weeks of data from pumps, sensors, and/or glucose meters were downloaded. Patients completed satisfaction questionnaires at the last follow-up visit.
Results:
A total of 162 patients were included. Mean age was 32 ± 17 years, 28% were (n = 46) children, and 29% (n = 47) were with a history of severe hypoglycemia. Median follow-up was 12 months (6–18). HbA1c was reduced from 55 ± 9 to 54 ± 8 mmol/mol (7.2% ± 0.8% to 7.1% ± 0.7%) at 12 months (P < 0.03, n = 100). In patients with suboptimal control, there was a reduction in HbA1c from 66% ± 7% to 61 ± 10 mmol/mol (8.2% ± 0.6% to 7.7% ± 0.9%) at the end of follow-up (n = 26, P < 0.01). Three percent (n = 5) of the patients experienced severe hypoglycemia during follow-up. A reduction in the percentage of self-monitoring of blood glucose values <70 mg/dL was achieved (10% ± 7% to 6% ± 5%, P = 0.001, n = 144). Time in range 70–180 mg/dL was 67% ± 13% at the end of follow-up and predictors of a higher time in range were identified. The use of sensors was high (86%) and 73% of the patients showed high satisfaction. In patients using sensors at baseline (n = 54), the time spent at <54 and <70 mg/dL was reduced.
Conclusion:
SAP-PLGS reduces hypoglycemia frequency while maintaining glycemic control in adults and children under real-life conditions.
Introduction
M
The use of continuous glucose monitoring (CGM) associated with insulin pump therapy (sensor-augmented pump therapy, SAP) has been an important milestone in T1D management during recent years. This therapy allows patients to adjust their insulin treatment more frequently and precisely and has been demonstrated to improve HbA1c, in both clinical trials and real-life studies, without increasing hypoglycemia and even reducing it. 5 –8
In recent years, the incorporation of control algorithms into SAP systems has allowed for automated suspension of basal insulin delivery in response to detected or predicted low-glucose level (low-glucose suspend [LGS] and predicted LGS [PLGS], respectively). The use of LGS has been associated with a reduction in hypoglycemia in randomized clinical trials when patients at high risk of hypoglycemia are included, 9 and the analysis of the real-world use of this feature confirms these data. 10 Similarly, the evaluation of PLGS function in randomized clinical trials has shown a reduction in hypoglycemia in in-clinic conditions 11,12 as well as in short-term observational studies. 13 –15
Despite the proven benefits of this technology, the use of these systems in some countries is scarce. There are a number of reasons for this, but one significant reason is that CGM devices are not reimbursed. Data that demonstrate the benefits of this therapy in real-world use are needed to convince both authorities and health professionals that the investment of time and resources required to implement this therapy is worthwhile.
For these reasons, our objective has been to evaluate both the effectiveness and the acceptance of the SAP with PLGS therapy in real-world use in children and adults with T1D during medium-/long-term follow-ups.
Material and Methods
All the patients with T1D treated with the MiniMed 640G® pump with PLGS function at three referral hospitals in Spain were retrospectively evaluated. All the patients who started using the system between May 2015, when it became available in Europe, and May 2017 were included in the study. Demographic characteristics and indication for SAP-PLGS, as identified by the clinician, were recorded. Baseline HbA1c, using the average of the last two values, and HbA1c at 6, 12, 18, and 24 months were registered. Two weeks of pump, CGM, and/or glucose meters downloads at baseline and 2 weeks SAP-PLGS downloads at last follow-up visits were analyzed using the CareLink Pro® software. In those downloads, the number of self-monitoring of blood glucose (SMBG) readings per day and the percentage of SMBG values <54, <70, >180, and >250 mg/dL, the frequency of sensor use, and the time spent in different ranges of sensor values were evaluated. Severe hypoglycemia episodes, recalled by the patients, at any time in the past at baseline and during the use of the system at the end of follow-up were registered. Satisfaction questionnaires were sent by e-mail or post to adults, children, and children's parents at the last follow-up visit. Ten questions regarding general satisfaction with the therapy had to be answered in a 1–5 Likert scale by adult patients and by children's parents. Children up to 10 years of age were asked to complete a six-item questionnaire, with picture options (“happy” or “sad” faces). The questionnaires were designed ad hoc for the study (see Supplementary Data at
Data analysis was conducted using SPSS statistics software v22. Results are presented as mean ± SD values or median (interquartile range [IQR]). A paired Student's t-test or a Wilcoxon signed-rank test was used for the analysis of differences. For nonpaired samples, the independent samples t-test was used. Comparisons between proportions were analyzed by a chi-squared test. A P value <0.05 was considered statistically significant.
The study was approved by the local research ethics committee.
Results
A total of 162 patients were included in the analysis with a minimum follow-up of 3 months using the MiniMed 640G pump with PLGS function. The age (mean ± SD) was 32 ± 17 years, with a range between 2 and 72 years old; 28% (n = 46) of the patients were younger than 18 years and 62% (n = 100) were women. The diabetes duration was 19 ± 13 years and 47 patients (29%) had a history of severe hypoglycemia in the past. Owing to different regional policies, 67% (n = 109) of the patients were reimbursed for the cost of CGM.
Median (IQR) follow-up was 12 months [6–18] in the whole group and 18 months [6–18] in children. Maximum follow-up was 24 months in seven patients.
The main indication for SAP-PLGS was frequent hypoglycemia (57%, n = 92), followed by poor glycemic control (17%, n = 28), high glycemic variability (14%, n = 22), a need to improve quality of life (8%, n = 13, 10 of them children), and pregnancy planning (4%, n = 6). Frequent hypoglycemia, as the main indication defined by the healthcare professional, could refer to severe hypoglycemia or frequent mild to moderate hypoglycemia.
Before starting to use the system, most patients (81%, n = 131) were already on a pump, without CGM or with different CGM devices, but not implemented with the PLGS function. Thirty-one out of 162 patients (19%) were on multiple daily insulin (MDI) injections therapy, with or without CGM-associated treatment. Regarding glucose monitoring, 59% (n = 96) of the patients used SMBG, whereas the rest used CGM or flash glucose monitoring. One patient had started using SAP-PLGS at diabetes onset, at the age of 2 years. Only nine patients (5.5%), six children and three adults, stopped using the system during follow-up due to lack of benefit or poor compliance.
Baseline HbA1c dropped from 55 ± 9 to 54 ± 7 mmol/mol (7.2% ± 0.8% to 7.1% ± 0.7%) at 12 months (P < 0.03, n = 100), with no significant differences at 6 or 18 months (P = 0.242, n = 134; P = 0.162, n = 55, respectively).
Specifically regarding those patients in whom SAP-PLGS was started because of poor glycemic control, HbA1c dropped from 66 ± 7 to 61 ± 10 mmol/mol (8.2% ± 0.6% to 7.7% ± 0.9%) at the end of follow-up (n = 26, P < 0.01), without an increase in the percentage of SMBG readings <70 mg/dL (5.9% ± 4.1% vs. 3.5% ± 3.6%, P: N.S.).
The greatest benefit in terms of HbA1c was found in the group of patients treated with MDI + SMBG before SAP-PLGS, in which HbA1c dropped from 58 ± 7 to 51 ± 7 mmol/mol (7.5% ± 0.6% to 6.8% ± 0.6%), (n = 20, P < 0.001).
In children, baseline HbA1c and HbA1c at the end of follow-up were not significantly different (53 ± 7 mmol/mol vs. 52 ± 7 mmol/mol (7.0% ± 0.6% vs. 6.9% ± 0.6%), P = 0.550), whereas a significant decrease was found in the adult group (56 ± 10 mmol/mol vs. 54 ± 9 mmol/mol [7.3% ± 0.9% vs. 7.1% ± 0.8%], P < 0.01) (Table 1).
Bold indicates p values significant difference.
Data are expressed as mean ± standard deviation.
SMBG, self-monitoring of blood glucose.
Twenty-nine percent (n = 47) of the patients had a history of severe hypoglycemia at some point before the study. However, only 3% (n = 5) of patients experienced severe hypoglycemia during the use of SAP-PLGS. These five patients included four adults and a 3-year-old girl. Three of the patients had experienced severe hypoglycemia before the start of the system. All of them had been using the system for at least 12 months.
The number of SMBG readings per day and the percentage of SMBG values <54, <70, >180, and >250 mg/dL were compared in baseline pumps, sensors, and/or meters with end of follow-up SAP-PLGS downloads (Table 1).
Sensor use was 6.0 ± 0.8 days/week (86% of the time) by the final follow-up visit. Sensor use was not significantly different in adults compared with children (5.4 ± 0.4 days/week in adults vs. 6.0 ± 0.4 days/week in children, n = 159, P: N.S.). Sensor use was also similar in patients who were reimbursed for CGM compared with patients who were not (P = 0.094).
Regarding the use of insulin pump therapy, bolus insulin increased from 52% ± 14% to 54% ± 13% (P < 0.01) at the end of follow-up, whereas the number of boluses per day and the number of boluses using bolus advisor per day did not show any significant differences. The total daily insulin dose per body weight slightly increased from 0.61 ± 0.22 U/kg at baseline to 0.64 ± 0.22 U/kg at the end of follow-up (P = 0.007).
Regarding PLGS use, the suspend “before low” threshold was set between 60 and 70 mg/dL in 76% (n = 123) of the patients. At the last follow-up, the mean time that the pump was stopped due to hypoglycemia prediction was 162 ± 96 min/day, with an average of 2.7 ± 1.3 events per day. Nineteen percent of hypoglycemia events <70 mg/dL happened at nighttime and 81% of them at daytime. PLGS was effective in avoiding hypoglycemia <70 mg/dL in 83% of the times it was activated, both at nighttime and daytime. Nevertheless, PLGS was followed by hyperglycemia slightly more frequently during the day, 10% of the times, than during the night, 7% of the times it was activated.
The time spent in different ranges of sensor values at the last follow-up visit was analyzed (Fig. 1). No differences in the percentage of time in the range 70–180 mg/dL were found between men and women or between patients with or without reimbursement for CGM.
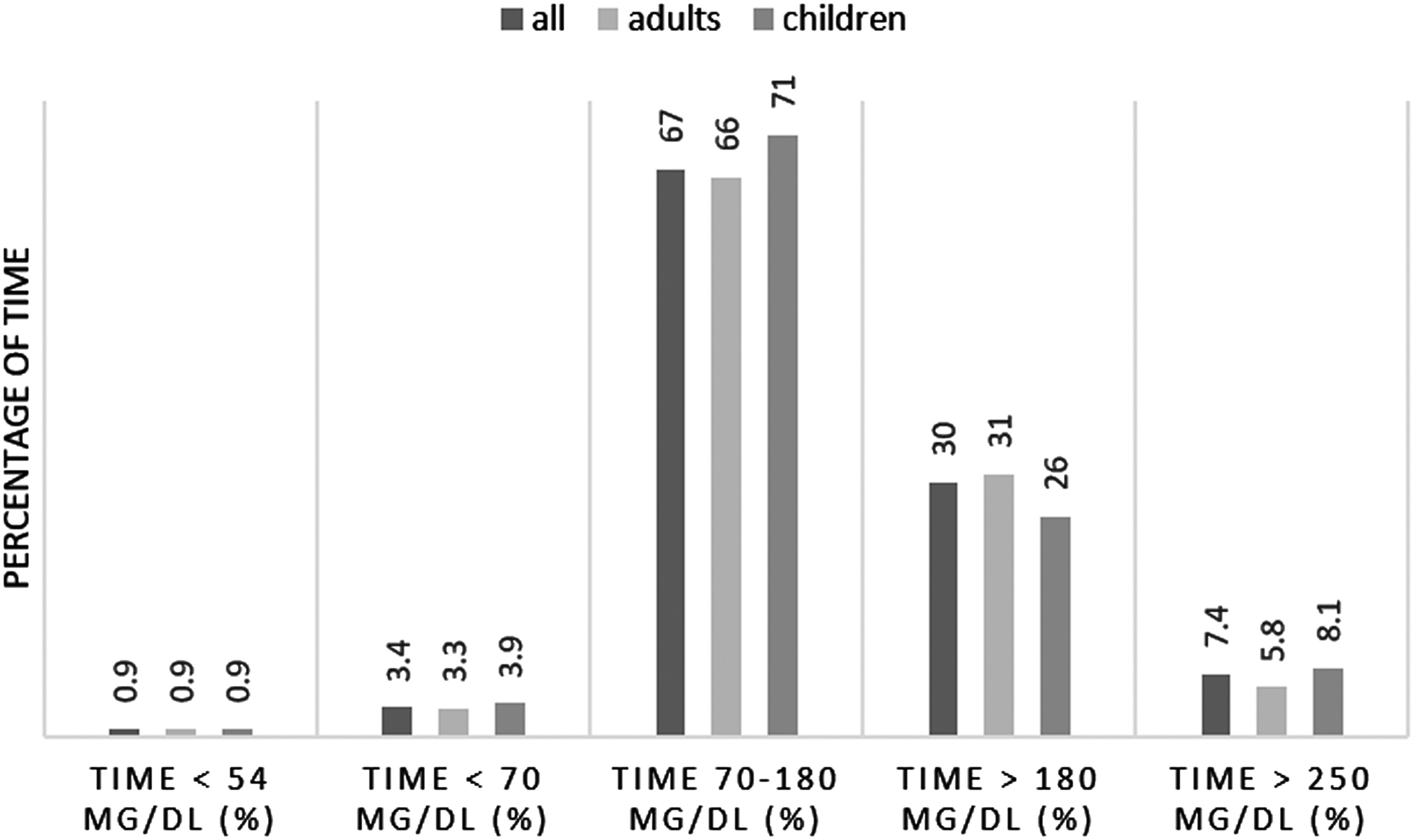
Time in different ranges in sensor values at the last follow-up visit. P = 0.013 adults versus children time 70–180 mg/dL, P = 0.011 adults versus children time >180 (independent samples t-test).
In a univariate analysis, some differences in the baseline patient characteristics and the pump use at baseline and during follow-up were seen among the patients with the lowest and the highest time in ranges at the end of follow-up (Table 2). In a multivariate logistic regression analysis, the predictors of a higher time in range 70–180 mg/dL at the end of the follow-up were a lower baseline HbA1c (β = −8.5, 95% confidence interval: −10.750 to −6.250; P = 0.001), a higher percentage of bolus insulin at baseline (β = 0.185, 95% confidence interval: 0.065 to 0.305; P = 0.003), and a higher time in suspension “before low” at the last follow-up visit (β = 0.001, 95% confidence interval: 0.000–0.001; P = 0.001).
Data are expressed as mean ± standard deviation.
CSII, continuous subcutaneous insulin infusion; SAP-PLGS, sensor-augmented pump with predictive low-glucose suspend function.
The sensor values were compared from baseline to the end of follow-up in the group of patients using CGM before SAP-PLGS (Table 3), showing an improvement in the time spent in hypoglycemia with a slight increase in mean sensor glucose. In these groups, we found that 25% (n = 14) of the patients reduced both their HbA1c and the time they spent in hypoglycemia <70 mg/dL, 41% (n = 22) reduced the time in hypoglycemia range but not their HbA1c levels, and 17% (n = 9) only reduced their HbA1c but not their time in hypoglycemia; finally 17% (n = 9) of the patients did not improve either of them.
Bold indicates p values significant difference.
n = 54. Data are expressed as mean ± standard deviation. Median follow-up: 12 months, 15% (n = 8) children. Previous treatment: n = 45 SAP with low-glucose suspend function, n = 3 SAP without low-glucose suspend function, n = 6 MDI + CGM, 72% hypoglycemia as indication for SAP-PLGS.
CV, coefficient of variation; MDI, multiple daily insulin.
Patient satisfaction was high in 73% of patients (n = 80); this figure was similar in children's parents, children, and adults.
Discussion
This study analyzes the use of sensor-augmented insulin pump with predictive low-glucose suspension in real-world conditions, showing a reduction in the percentage of time in hypoglycemia without deterioration in HbA1c in T1D patients.
Some randomized clinical trials have been published analyzing SAP with PLGS system both in and out of hospital. 12,16 –18 Despite differences in the design and in the characteristics of the patients included in the studies, all of them have shown a reduction in hypoglycemia when using the system. In the same line, our study has shown a decrease in both the percentage of SBMG values <70 mg/dL and the percentage of time in CGM <70 and <54 mg/dL. Moreover, these results have been achieved in both adults and the pediatric population. In the out-of-hospital randomized clinical trials published, some increase in time in hyperglycemia has been shown: in Battelino et al's 2 weeks study, 6 only time >140 mg/dL was increased, without differences in time >180 mg/dL, but in Abraham et al's 6 months study, 18 both time between 180 and 270 mg/dL and time >270 mg/dL were increased, with an increase in HbA1c, in the group using PLGS at 6 months (58 ± 9 mmol/mol to 62 ± 9 mmol/mol; 7.5% ± 0.8% to 7.8% ± 0.8%). However, in our study, the improvement in hypoglycemia has been achieved without HbA1c deterioration, even with a statistically but not clinically significant improvement of HbA1c at 12 months (−1 mmol/mol [0.1%]) and without an increase in time >180 and 250 mg/dL.
Most of the patients included in our study (57%) had hypoglycemia as the main indication for starting SAP with PLGS system, so in this group a reduction in hypoglycemia frequency is the main outcome to achieve. However, in the subgroup of patients in which the start of SAP with PLGS system was because of suboptimal glucose control (n = 26, 16%), the use of the system resulted in a decrease in HbA1c by 5 mmol/mol (0.5%) without an increase in hypoglycemia frequency, demonstrating that in a real-world setting, this system can improve results in both hypoglycemic patients and patients with suboptimal metabolic control.
Several studies using SAP, with and without automatisms, have shown that the efficacy of these systems is strictly related to the frequency of sensor use. 6,19,20 Sensor use in our study was very high (86% of the time in the total cohort) and no differences in the frequency of use were seen between adult and the pediatric population, nor between those who had reimbursement for CGM and those who did not. This suggests that the frequency of the sensor use is not related to age or financial factors. However, the appropriate selection of the patients and the provision of an educational program at the start of the sensor use, to minimize technical problems and maximize the benefits of the therapy, are key factors in achieving a high frequency of use of the sensor. The satisfaction questionnaires had been sent to the patients by e-mail or post at the end of follow-up and we had a 50% rate of response, which could limit the interpretation of the results. Nevertheless, we believe that the high sensor usage and the low discontinuation rate reinforce this point as they reflect a high patient satisfaction.
We have analyzed factors associated with higher time in range 70–180 mg/dL at the end of the follow-up. We observed, in a multivariate analysis, that the higher the time in suspension “before low,” the higher the time in range achieved. In our study, the mean time that pumps were stopped due to hypoglycemia prediction was 162 ± 96 min/day, which is greater than values published in other studies: 118 min/day in Ref. 13 Moreover, other changes in the pump use have been shown. The insulin administered as bolus was higher with the use of PLGS, with differences neither in the number of boluses nor in the bolus wizard use, suggesting that PLGS patients and/or their healthcare professionals might be more confident and program the bolus wizard settings more aggressively. Also, a higher percentage of bolus insulin at baseline and during SAP-PLGS predicted a higher time in range, reflecting that patients needing a lower basal rate could benefit more, or suffer from less hyperglycemia after predictive low-glucose suspensions, than patients needing more basal insulin. To our knowledge, no other studies have previously evaluated these aspects of the use of pump therapy during SAP-PLGS therapy.
In our data, 19% of the hypoglycemia events happened at nighttime. This result agrees with other data in the literature that show 20% of nocturnal hypoglycemia in patients with T1D in a prospective analysis. 21 PLGS was effective in avoiding hypoglycemia 83% of the times it was activated, similar to the data shown in the Medtronic 640G user evaluation. 13 This effectiveness was similar at nighttime and daytime. However, PLGS was followed by hyperglycemia slightly more frequently during the day, 10% of the times, than during the night, 7% of the times, probably due to more interference by the patients.
We are aware that our study has many limitations. First, it is a retrospective study performed in real-life conditions, so we do not have a control group to compare outcomes, and patients at baseline were treated with different treatment modalities. However, we believe that this kind of study complements the information provided by randomized clinical trials and adds information about the effectiveness of the therapy in a real-world setting. Moreover, sensor glucose information at baseline is only available for a third of the patients, those who used CGM therapy before the start of SAP with PLGS, so we could not compare time in different ranges between baseline and the end of the study in the total cohort, although the percentage of SMBG lectures was used for this comparison at baseline. We were not able to separate the PLGS events that were terminated manually or automatically or to evaluate the specific effect of the predictive low-glucose suspend function during exercise.
In conclusion, SAP-PLGS suspension reduces time in hypoglycemia and maintains glycemic control in children and adults with T1D in a real-world clinical setting, with good patient acceptance and satisfaction.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.