
Abstract
Objective:
Officially licensed hybrid closed-loop systems are not currently available worldwide; therefore, open-source systems have become increasingly popular. Our aim was to assess the safety, feasibility, and efficacy of an open-source hybrid closed-loop system (AndroidAPS) versus SmartGuard® technology for day-and-night glucose control in children under extreme sports conditions.
Research Design and Methods:
Twenty-two children (16 girls, 6–15 years of age, median HbA1c 56 ± 9 mmol/mol) were enrolled in this pivotal winter sports camp study. The participants were divided into two groups using either the AndroidAPS or SmartGuard technology. Physical exertion was represented by all-day alpine skiing. The primary endpoints were mean glucose level, time below the threshold of 3.9 mmol/L, and time within the target range of 3.9 to 10 mmol/L.
Results:
The children using the AndroidAPS had significantly lower mean glycemia levels (7.2 ± 2.7 vs. 7.7 ± 2.8 mmol/L; 129.6 ± 49 vs. 138.6 ± 50 mg/dL, P < 0.042) than the children using the SmartGuard. The proportion of time below the target (median 5.0% ± 2.5% vs. 3.0% ± 2.3%, P = 0.6) and in the target zone (63% ± 9.5% vs. 63% ± 18%, P = 0.5) did not significantly differ. The AndroidAPS group experienced more frequent malfunctions of the cannula set (median 0.8 ± 0.4 vs. 0.2 ± 0.4, P = 0.02), which could have affected the results. No significant difference was found in the amount of carbohydrates consumed for the prevention and treatment of hypoglycemia [median 40 ± 23 vs. 25 ± 29 g/(patient ·3 days)]. No episodes of severe hypoglycemia or other serious adverse events were noted.
Conclusions:
This pilot study showed that the AndroidAPS system was a safe and feasible alternative to the SmartGuard Technology.
Introduction
C
Automatic functions, such as SmartGuard® Technology using Predictive Low-Glucose Management (PLGM), led to significant progress in T1D pump therapy. Several studies have demonstrated the effectiveness of PLGM in hypoglycemia prevention overnight, 3 during the day, 4 and even after prolonged periods of physical activity. 5 Moreover, PLGM technology was superior to sensor-augmented pump therapy alone, predominantly in hypoglycemia prevention in all studies. However, the reduction in hypoglycemia was accompanied by a modest increase in the mean morning glucose values and prolonged time in moderate hyperglycemia. 4 In addition, PLGM does not address the issue of everyday variability in insulin requirements, which remains an unmet need among patients with T1D.
Closed-loop delivery (artificial pancreas [AP]) differs from conventional pump therapy with threshold suspending technology by a control algorithm that automatically increases and decreases subcutaneous insulin delivery in response to real-time sensor-detected glucose levels. 6 Randomized trials investigating day-and-night closed loops under unsupervised free-living condition in children, adolescents, and adults have shown improved glycemic outcomes, reduced risk of nonsevere hypoglycemic events, and positive user experiences 6 –10 ; however, only one system (MiniMed 670G, Medtronic) is currently commercially available and is not accessible worldwide.
OpenAPS is an abbreviation for open-source AP System
In our study, we used the AndroidAPS app, which was created by Milos Kozak. This application was created based on the platform of the OpenAPS algorithm described above and belongs to the DIY AP systems, but the AndroidAPS app was adjusted for smartphones with the Android system. The pump is fully controlled by a smartphone with the AndroidAPS application, and the CGM and continuous subcutaneous insulin infusion data can be visualized on the smartphone.
The first OpenAPS pilot study was presented by Dana Lewis at ADA 2016 and included 18 patients who used OpenAPS for 16 months. 12 The use of the OpenAPS algorithm led to a significant improvement in HbA1c from 55 mmol/mol at baseline to 44 mmol/mol at the end of the study (7.2% to 6.2%). This improvement was accompanied by a prolonged time in the target range (4–8 mmol/L, 72–144 mg/dL) from 58% to 81%, and all patients reported significant improvement in theirs and their family members' quality of life.
The algorithm and its additional features have not received CE (Certification Europe) marking or FDA approval to date. However, because available products with hybrid closed-loop systems are lacking worldwide, the number of patients with T1D using these uncertified products is increasing, and physicians are increasingly confronted with T1D patients using this system. The community using OpenAPS includes patients with T1D and parents of children with T1D who are highly motivated to use modern technologies and promote T1D closed-loop treatments.
13
Therefore, experience-sharing and clinical studies are needed to increase clinicians' awareness of the advantages and limitations of this product. In fact, data regarding this system are limited in the literature.
14
Notably, the Juvenile Diabetes Research Foundation (JDRF) announced the New Initiative to Pave the Way for Open Protocol Automated Insulin Delivery Systems in 2017 (
The aims of our study were to examine and compare the mean glucose levels, time below the threshold of 3.9 mmol/L (70 mg/dL), time within the target range of 3.9 to 10 mmol/L (70 to 180 mg/dL), and time above 14 mmol/L (252 mg/dL) between a group using the AndroidAPS system and a group using the commercially available SmartGuard Technology system under extreme sports conditions during a winter ski camp.
Research Design and Methods
Patients
In total, 23 children were included in our pilot winter camp study. One subject was excluded from the study after losing the smart phone with the AndroidAPS app and Xbridge (data transmitter, see below) during the first day of skiing; thus, 22 children (16 girls, 6–15 years of age, median 12 ± 2.3) completed the study. For the detailed characteristics of the patients, see Table 1. The study inclusion criteria were a T1D duration of longer than 12 months, experience with an insulin pump, at least intermittent wearing of CGM for at least 12 months and the intention to be included in the study as expressed by the parents at the regular visits in the center for childhood diabetes.
Data are the mean (SD).
BMI, body mass index, CSII, continuous subcutaneous insulin infusion, IFCC, International Federation of Clinical Chemistry; DCCT, diabetes control and complications trial; PLGM, predictive low-glucose management; SD, standard deviation.
Because of very intensive sport activity during all camp none of the included patients had secondary diabetic complications, experienced severe hypoglycemia with consciousness impairment or suffered from hypoglycemia unawareness (determined by a Gold score >4 on the basis of the pre-study clinical records) during the previous year. All these exclusions were set from safety reasons.
All children were divided into the following two groups for three consecutive nights and days: the first group used the SmartGuard Technology system with PLGM (n = 12; MiniMed® 640G pump, Enlite™ Sensor), and the second group used the open-source hybrid closed-loop system AndroidAPS (Android Smartphone with AndroidAPS app, DANA Diabecare R pump, Dexcom G4™ Sensor, Xbridge, which transmits the data from the sensor to the Smartphone).
The division of the children into the groups was not random but was based on the type of pump currently used as follows: children using Medtronic pump MiniMed 640G continued to use this type of pump. They were experienced in using the PLGM. Children using other types of pumps (six children used Animas Vibe, two children Medtronic MiniMed Veo, and two children DANA Diabecare R) were included in the AndroidAPS group. Two children included in the AndroidAPS group had been using the AndroidAPS for 12 months before the study. This group was educated on how to work with AndroidAPS app.
One week before the study onset, all participants attended a run-in seminar, during which they were trained again on how to use the particular study pump and CGM device and calibrate the real-time CGM device according to the manufacturer's instructions. All technical procedures, including pump refill, priming tubes, or cannula insertions were under staff supervision.
The basal rates and settings of the bolus calculator were optimized for all children during regular outpatient control examinations 1 month before the study. All participants used the rapid-acting insulin analog Aspart (NovoRapid®, Novo Nordisk, Bagsvaerd, Denmark).
Physical activity was represented by whole-day downhill skiing (9 am to 4 pm) and evening entertainment activities (disco dance, 8 to 11 pm). The experience level in downhill skiing was very good in both groups (all children were intermediate or advanced skiers).
AndroidAPS hybrid closed-loop system
In our study, we used the AndroidAPS app, which was created by Milos Kozak (available at MilosKozak/AndroidAPSapp-pumpcontrol-wearcontrol-release_1.53.apk) and it was described above. All children used standardized version of the AndroidAPS oref0 and all had the same setting according to the study protocol. The target glycemia level and maximal change in the basal rates can be changed by the user (up to 300% of the original basal rate). In our study, the target glycemia level was set to 6.0 mmol/L (108 mg/dL) for all days, and the maximal increase in the basal rates was limited to 100% for safety reasons. All patients in this group uploaded AndroidAPS app and connected this application to their DANA R pump by themselves, but with help and supervision of the study team.
Setting of the SmartGuard technology
The PLGS was set to 3.2 mmol/L (58 mg/dL) during the nighttime and 3.4 mmol/L (61 mg/dL) during the daytime.
Throughout the camp, the subjects in both groups were monitored through CGM and by the study physicians 24 h per day. In addition, all data from Android app (as well as from other DIY AP systems) can be monitored in parallel by the web-based NightScout system, which is other open-source project by DIY technologies that enables real-time access to CGM data and its storage through personal websites (
The blood glucose levels were controlled in all participants using a personal glucometer every 3 h, and all cases of hypo- or hyperglycemia were reported on CGM. The glucometer data were used for control and calibration of CGM.
Hypoglycemia (real hypoglycemia defined as <3.9 mmol/L [70 mg/dL]; prevention of hypoglycemia <4.9 mmol/L [88 mg/dL]) was treated with dextrose only according to the hypoglycemia levels and glycemic trends assessed by CGM (see Supplementary Table S1; Supplementary Data available online at
Hyperglycemia (blood glycemia [BG] >14 mmol/L, 270 mg/dL) was immediately corrected with an extra bolus of insulin as calculated by a bolus calculator. All meals should have been disclosed by the participants to the study team. The participants were required by the study team to count carbohydrates and use a standard bolus calculator for premeal boluses according to usual practices in both groups. The basal rates and premeal and correction boluses were reduced during physical activity by 30% to 50% according to the age and total daily dose. The reduction was performed similarly across all 3 days in both groups. All data were uploaded through the CareLink® Professional system or NightScout and reviewed by the research team to verify that both systems were running appropriately. All glucose outcomes were computed based on the CGM records.
Statistical methods
The differences between the AndroidAPS and PLGM groups were analyzed using nonparametric tests (Kruskal–Wallis and ANOVA). The data of the mean glucose levels in the AndroidAPS and PLGM groups, including repeated measurements over three nights and days, were compared using a linear mixed-effects model. Sensor data were used for statistical analysis. P-values less than 0.05 were considered statistically significant. Analyses were conducted using the R statistical package, version 3.1.1.
Outcomes
The primary objective was to compare the mean BG levels, percentage of time in hypoglycemia (below 3.9 mmol/L, 70 mg/dL), and percentage of time in the target range (3.9 mmol/L to 10 mmol/L, 70 to 180 mg/dL) during all 3 days between the two groups.
The secondary objective was to describe the differences in the following markers of diabetes control between the groups: (1) percentage of time in normoglycemia (3.9 to 8 mmol/L, 70 to 140 mg/dL), (2) percentage of time in hyperglycemia (above 14 mmol/L, 252 mg/dL), (3) number of hypoglycemia events (defined as consecutive glycemia <3.9 mmol/L, 70 mg/dL, at least 20 min apart), (4) amount of dextrose (grams) used for hypoglycemic treatment in both groups, and (5) mean insulin dose per kg body weight/day. The outcomes were further divided by the following segments of the day: daytime (7 am to 10 pm) and overnight (10 pm to 7 am).
The study was approved by the Ethics Committees of the Motol University Hospital and Second Faculty of Medicine, and written informed consent was obtained from all parents of the participants before the study.
Results
Of the 22 children included in the study, 12 children were assigned to the PLGM group, and 10 children were assigned to the AndroidAPS group. The groups did not differ in age, anthropometric parameters, or duration of diabetes. All patients were well controlled, and their median HbA1c was 56.9 ± 11 mmol/mol International Federation of Clinical Chemistry (7.4% Diabetes Control and Complications Trial). At baseline, no significant differences were observed in the total daily insulin dose or basal-to-bolus ratios (Table 1).
Overall, the children using AndroidAPS had significantly lower mean BG levels than the children in the PLGM group (mean glycemia 7.2 ± 2.7 vs. 7.7 ± 2.8 mmol/L; 129.6 ± 49 vs. 138.6 ± 50 mg/dL, P < 0.042). The difference in the mean BG levels remained significant both during the day and night periods (daytime mean BG 7.3 ± 2.6 vs. 7.5 ± 2.7 mmol/L; 131.4 ± 47 vs. 135.6 ± 49 mg/dL, P < 0.001, nighttime mean BG in mmol/L 7.1 ± 2.7 vs. 8.0 ± 2.9; 127.8 ± 52 vs. 144 ± 52 mg/dL, P < 0.0001). The hour-by-hour analysis showed that the differences were particularly expressed between 6 and 10 pm (P < 0.001) and between 3 and 4 am (P = 0.02) (Fig. 1 for details).
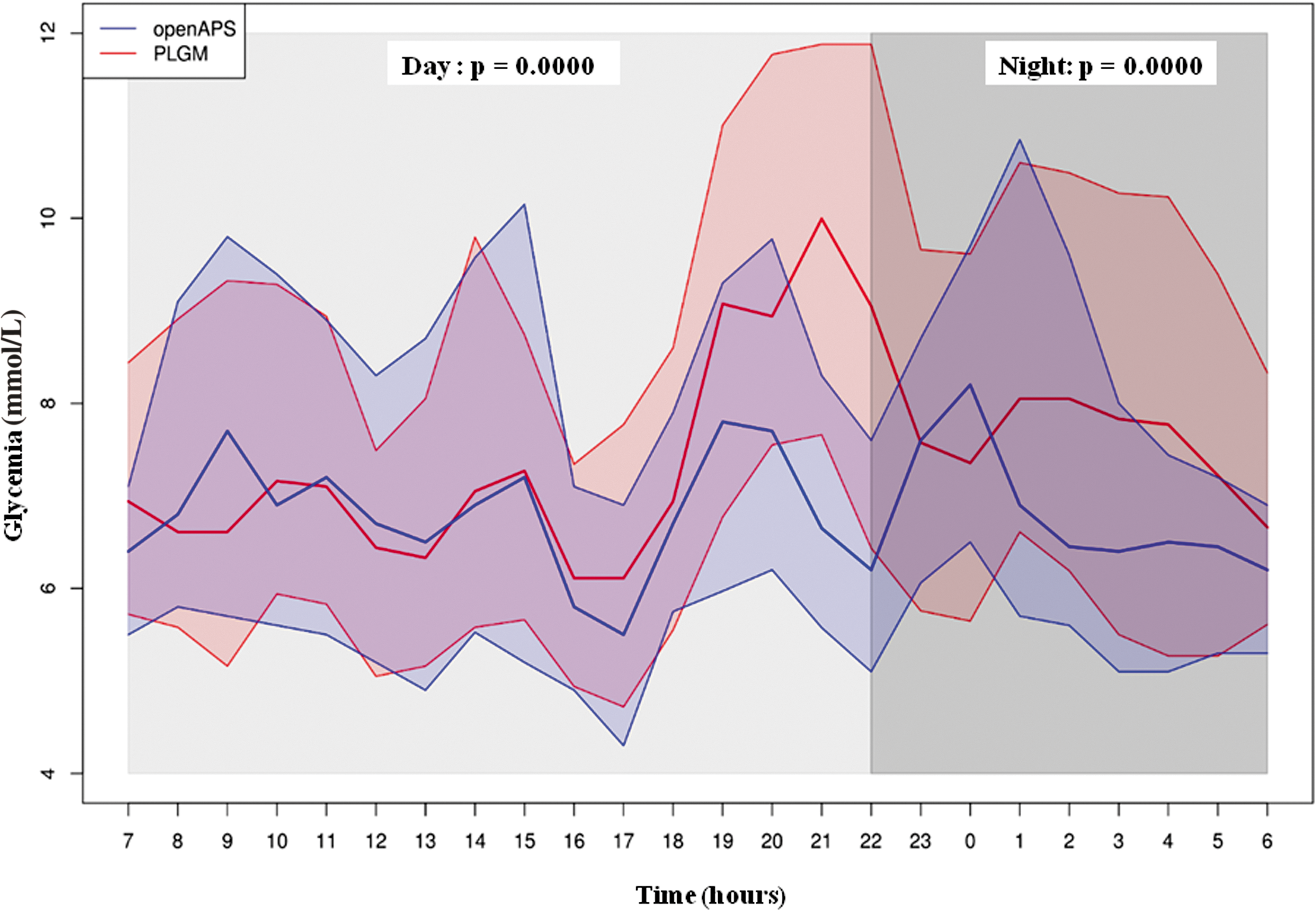
Sensor glucose profile (mmol/L) of all 3 days. The red line represents the PLGM group. The blue line represents the openAPS group. Data are the median (IQR). PLGM, predictive low-glucose management. (Color graphics available at
Despite the lower mean BG levels, the time spent in hypoglycemia (below 3.9 mmol/L; 70 mg/dL) was similar in both groups over the 3 days of monitoring (median 5.0% [IQR 2.0% to 6.2%] versus 3.0% [2.1 to 4.5], P = 0.6 in the AndroidAPS and PLGM groups, respectively). Similarly, the groups did not differ in the number of hypoglycemic events over all 3 days (median AndroidAPS 3.0 [1.8 to 5.1] versus PLGM 3.0 [1.2 to 4.1] episodes, P = 0.4), and the amount of dextrose used for the treatment and prevention of hypoglycemia per patient per day (median AndroidAPS 40.0 g [25.1 to 43.2] versus PLGM 25.3 [16.3 to 54.1], P = 0.6).
We did not observe any significant intergroup differences in the time in the target range (median AndroidAPS 82% [77 to 86] versus 82% [64 to 85], P = 0.3). The SD for BG as a surrogate of glycemic variability was slightly lower in the AndroidAPS group, but the difference was not statistically significant (median AndroidAPS 2.3 [2.1 to 2.8] vs. PLGM 2.6 [2.5 to 2.9], P = 0.09). Both groups exhibited a similar amount of time in the suspend mode during the study (PLGM group median 543 min [295 to 682], AndroidAPS group median 580 min [435 to 762], P = 0.50), and the frequency of activating the suspend mode was similar in both groups (median AndroidAPS 11.3 [9.5 to 15.0] vs. PLGM group median 12.1 [9.5 to 15.0]). The suspend mode was more frequently activated between 3 to 6 pm in the PLGM group (71% of patients, P < 0.01), whereas in the AndroidAPS group, the suspend mode was activated independently of the time of day.
The total daily insulin dose did not differ between the groups over the study period. In the AndroidAPS group, the algorithm reduced the basal dose by a median of 3.4 ± 2.0 U/24 h and increased the basal rate by a median of 2.7 ± 2.3 U/24 h. Cannula malfunction was reported significantly more in the AndroidAPS group (0.8 ± 0.4 vs. 0.2 ± 0.4 events/all 3 days, P = 0.02). No other adverse events were reported over the study period. For summary of results see Table 2.
Data are the mean (SD) or median (IQR).
Discussion
This study is the first to describe the safety, feasibility, and effectiveness of the AndroidAPS algorithm under real-life conditions. We observed that the AndroidAPS system was more effective in lowering the mean glycemia levels despite the similar time in hypoglycemia compared with the control PLGM group. Hypoglycemia prevention was effective even after prolonged and repeated physical activity, which is the main risk factor for hypoglycemic episodes. 16 –19
The time in the target range and the decreased time in hypo- and hyperglycemic episodes represent important parameters of T1D control in the CGM era. Most closed-loop studies have shown a decreased mean BG without an increase in the time in hypoglycemia, which is a difficult task using standard insulin delivery. Although the pilot design of our study does not allow us to generalize and make any strong conclusion, we consider it very encouraging that our results were comparable, and in some parameters (time in the target range) were even better than those published by other groups using the hybrid closed-loop technology even though our children were exposed to prolonged physical activity over the study period.
Over 3 days, in a randomized Summer Camp Crossover Trial designed for 5- to 9-year-old children, Favero compared the AP system with sensor augmented pump therapy (SAP). The AP system resulted in a significant reduction in the time in hypoglycemia (2% compared with 6.7% in the SAP group); however, a decreased time in target (56%) and increased mean glucose (9.4 mmol/L, 169 mg/dL) were observed. 20
The AP Ski Study by Breton tested the feasibility and effectiveness of hybrid closed-loop systems during physical activity in an outpatient setting similar to that in our study. This study was a randomized controlled 5-day trial involving 32 adolescents that compared a closed-loop system (the University of Virginia CLS system) to standard SAP. The participants in the closed-loop arm were in the target range 71% of the time and in normoglycemia 43% of the time. 21 This duration was shorter than that observed in our AndroidAPS group (82% in target and 63% in normoglycemia). We also observed significantly lower mean BG levels (7.2 vs. 8.7 mmol/L; 157 vs. 130 mg/dL). However, the closed-loop group in the Breton study had less time in hypoglycemia (1.8% vs. 5.0%). These differences might be attributable not only to the different efficacies of both closed-loop systems but also to the different settings of the target glycemia level in the algorithm. However, the settings were not mentioned in detail in the article by Breton. 21
A study by Sherr et al. focused on overnight BG control with or without a closed-loop system and with or without antecedent afternoon exercise. In that study, 12 children and young adults were included, and the closed-loop technology was clearly confirmed to be very efficient in the optimization of T1D after physical activity. The patients reached 90% of the time in the target range in the closed-loop arm and 60% of the time in the open-loop arm accompanied by decreased time in hypoglycemia (1.5% vs. 4%). 22 However, the study only focused on overnight BG control and was designed as an inpatient study.
A recent pivotal study using Medtronic 670G, which is the only commercially available hybrid closed-loop system, successfully confirmed its safety under in-home conditions. 23 The improvement in T1D control was only modest compared with that in the abovementioned studies, and the overall time in the target was 67.2% among the adolescents and 73.8% among the adults. The Medtronic HCL system is simple to navigate and use because both the carbohydrate/insulin ratio and the insulin sensitivity factor are algorithm derived. This feature is partially advantageous over the AndroidAPS, which requires a complete manual initial setting using a bolus calculator. In contrast, the ability to adjust the predetermined carbohydrate/insulin ratios for specific times of the day is limited by this feature and does not satisfactorily reflect individualized patient-derived needs.
In our study, we observed that the most significant differences in the BG levels between the AndroidAPS and PLGM groups occurred during the evenings (from 6 to 10 pm) and early in the morning (from 2 to 4 am) (Fig. 1). The tendency toward postprandial (postdinner) hyperglycemia in the PLGM group might be explained by the prolonged time in the suspend mode before dinner (6–6:30 pm). Alternatively, this phenomenon could be attributable to the inappropriately high reduction in the premeal bolus after physical activity; however, the reductions in the bolus and basal rates were similar in both groups.
The higher BG levels in the PLGM group in the early morning were caused by prolonged times in the suspend mode that were not corrected by the subsequent increase in insulin delivery. This issue, which is a main limitation of the current PLGM systems, was also observed in a randomized study conducted by Battelino et al. 4 comparing PLGM with SAP. Expectedly, the PLGM group exhibited significantly less time in hypoglycemia than the SAP group, but this positive trend was compensated for by longer time in the hyperglycemic range. Consistently, Biester et al. 24 showed that PLGM is very effective during the night; however, PLGM interfered with glycemia excursion after a meal during the day, which could be solved by rearranging the administered basal insulin in AndroidAPS. Nevertheless, both systems were similarly effective in hypoglycemia prevention during the daytime.
In our study, no participants experienced severe hypoglycemia or diabetic ketoacidosis during the study period. Notably, we recorded a high number of cannula dysfunctions due to bubbles in the AndroidAPS group. These events could have significantly influenced the results of the study, and we speculate that the results of the AndroidAPS group could have been even better without these episodes. A possible explanation could be the low level of practical experience with the DANA Diabecare R pump, which was new to most of our children and staff. Another explanation for the high frequency of cannula dysfunction might be the more vulnerable connection between the insulin reservoir and infusion set caused by physical activity.
The total time in the target glycemia range might have been influenced by an insufficient, that is, too conservative, correction by the increase in the basal rate (100%) in our study. Based on this experience, the setting of the maximal basal change to 300% in the AndroidAPS might be more effective, but further studies are needed to test the safety of this approach. The AndroidAPS app version, oref0, which we used in this study, has also some limitations. It requires an excellent setting of insulin sensitivity and insulin-to-carbohydrate ratio. The insulin sensitivity has to be readjusted several times during 1 day during increased physical activity in children, which could be challenging. The new version of AndroidAPS oref1 includes a so-called autosensitivity mode, which recalculates patient's insulin sensitivity throughout the day. This function could enable to reach better results.
There were several limitations to this study. First, the duration of the study was too short to make any strong conclusion about efficacy. Second, the number of patients included in the study was rather low, although the sample size was comparable to that in other closed-loop studies. The exclusion of patients with hypoglycemia unawareness or severe hypoglycemia in history can also bias the results. Next, as noted above, the insufficient previous experience of the children with the DANA Diabecare R pump might have contributed to more frequent cannula problems in the AndroidAPS group; finally, the tight supervision of both groups by the clinical staff during all 3 days might have influenced the results of our study compared with the real-life conditions.
In conclusion, this pilot study shows that the AndroidAPS, which is an open-source hybrid closed-loop system, is a feasible tool for the optimization of T1D management during and after prolonged physical activity in children with T1D. Future studies are needed to assess its long-term efficacy and test the optimal settings of the algorithm. Our study supports the idea that DIY technology might represent a promising, technically comparable alternative to the most advanced commercially available products. These systems will probably be used by an increasing number of patients worldwide in the future because of the limited availability and reimbursement of new high-tech products. Therefore, knowledge regarding the advantages and limitations of this technology is mandatory for diabetologists.
Footnotes
Acknowledgments
The authors would like to thank Milos Kozak, a creator of the AndroidAPS app, for the technical support during our winter camp. They would like to thank Aranka Medkova, David Medek, and Radka Kozakova for sharing their personal experiences of the AndroidAPS and DIY systems with the authors. This study was supported by the Ministry of Health, Czech Republic—Conceptual Development of Research Organization, Project # 00064203.
Author Contributions
L.P. designed and coordinated the study, and wrote the article; P.J., V.N., L.P., V.P., and J.S. supervised and controlled the patients at winter camp, and wrote the article; S.P. wrote the article; Z.S. supervised and wrote the article; and B.O. was the study coordinator.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.