
Abstract
Aims:
The aim was to investigate the prevalence of diabetic sensorimotor polyneuropathy (DSPN) and cardiovascular autonomic neuropathy (CAN) in a Danish population of young adults with type 1 diabetes (T1D) using both established and novel measuring modalities. Furthermore, to investigate the association between continuous subcutaneous insulin infusion (CSII) treatment and these complications.
Materials and Methods:
CAN was assessed by cardiovascular autonomic reflex tests. DSPN was assessed not only by perception of light touch and pain, vibration perception threshold (VPT), Brief Pain Inventory (BPI), and Michigan Neuropathy Screening Instrument questionnaires but also by novel modalities: electrochemical skin conductance (ESC), sural nerve conduction velocity (SNCV), and sural nerve amplitude potential (SNAP).
Results:
The study comprised 156 young adults with a mean age of 22 years (standard deviation 1.6). The prevalence of CAN and early CAN was 9% and 28.1%, respectively. Subclinical DSPN was 55.1% and confirmed DSPN was 2.6%. Prevalence of abnormal SNAP was 23.8%, SNCV was 37.1%, ESC on the hands and feet was 4% and 8%, respectively, VPT was 1.3%, and BPI questionnaire was 1.9%. No association was found between CSII treatment and the measures of DSPN and CAN.
Conclusion:
DSPN and CAN are prevalent in young adults with T1D with no association found with CSII treatment. The use of novel measuring modalities identified a higher number of subjects with DSPN compared with established measures. Screening for diabetic neuropathy in young adults may be beneficial to detect and prevent nerve damages at early stages.
Background
D
Prevalence of diabetic neuropathy in adults with type 1 diabetes varies considerably for both DSPN (10%–41%) 7,8 and CAN (5%–35%). 1,7,9 –12 Previous studies have shown that diabetic neuropathy is prevalent in children and young adults with type 1 diabetes. Recently, a prevalence of DSPN of 7% was found in youth with type 1 diabetes. 13 However, as for adults varying prevalences have been reported for children and young adults with type 1 diabetes, where the prevalence varies between 7%–62.5% for DSPN 13 –20 and 3%–75% for CAN. 14,16,17,20 –23 This variation in prevalence may be due to marked differences in the studied populations and a lack of consensus on the applied measuring methods and diagnostic criteria for DSPN and CAN.
Several studies have demonstrated that the pathological mechanisms leading to damages of the nerve tissue begin early in the course of diabetes in both type 1 14 –17,21,22,24 and type 2 diabetes. 15,25,26 Diabetic neuropathy is often a rare problem during childhood but may be present in young adults with longer diabetes duration. 14 In addition, it has been demonstrated that puberty might be a risk factor for developing diabetic neuropathy. 27,28 Thus, it is plausible that the prevalence of diabetic neuropathy increases substantially when patients mature to young adults. Detecting diabetic neuropathy at an early stage may have an impact on the subsequent development. Improved glycemic control in patients with type 1 diabetes has been shown to prevent and revert early stages of DSPN and CAN and also slow the progression toward definite CAN. 2,7,29 –31 Meta-analyses have demonstrated that treatment with continuous subcutaneous insulin infusion (CSII) leads to a slightly larger reduction in HbA1c compared with multiple dose injections (MDI). 32,33 Yet, only few studies have assessed the potential benefits of CSII compared with MDI by insulin pen on the development of complications such as diabetic neuropathy. 34,35
Thus, there is a need to examine the prevalence of early and definite stages of diabetic neuropathy in early diabetes and to examine possible differences between CSII and MDI therapy in association with diabetic neuropathy.
The aim of this cross-sectional study was to investigate the prevalence of DSPN and CAN in a Danish population of young adults with type 1 diabetes using both established and novel measuring modalities and to determine the association between CSII treatment and DSPN and CAN.
Materials and Methods
Subjects
Patients were eligible for enrollment if they were aged between 18 and 24 years and were diagnosed with type 1 diabetes. All young adults were recruited from the outpatient clinic at Steno Diabetes Center Copenhagen, Gentofte, Denmark. Three hundred forty patients received a written invitation and later if no response they received more detailed information about the study by phone and were invited again to participate. The patients were comprehensively contacted to give most patients the opportunity to participate and avoid selection bias. Ethical approval of the study was obtained from the Danish Research Ethics Committee and written informed consent was obtained from all patients. All measurements were performed between 1 pm and 5:30 pm.
Patients restrained from vigorous exercise 24 h before examination and consumption of caffeine on the day of examination. No restrictions on use of medicine were applied. Patients treated with beta-blockers did not perform CAN measures.
Measures of DSPN
DSPN was assessed and categorized according to recommendations made by the Toronto Diabetic Neuropathy Expert Group 5 and included measures of symptoms, signs, and objective measuring methods.
To assess symptoms of DSPN, patients were asked to fill in questionnaires. See the Questionnaires on Peripheral Neuropathy and Exposures section for further details.
Signs of DSPN were assessed by established measures: Light touch perception was assessed by applying a 10 g monofilament (Neuropen®; Owen Mumford Ltd, Oxford, United Kingdom) to three points at the distal bilateral foot pads; just proximal to the great, third, and fifth toe. Pain sensation assessment was performed using a 40 g pinprick device (Neuropen; Owen Mumford Ltd) applied at the dorsal side of the toes just proximal to the nail on the great, third, and fifth toe. Vibration perception threshold (VPT) was determined using a biothesiometer (Bio-Medical Instruments, OH) at the distal end of the great toe on both sides. Age-stratified perception thresholds were used to assess if VPT tests were abnormal. 16 Bilateral abnormal results were defined as pathological tests.
Newer and non-established measuring modalities were applied to objectively assess DSPN.
Small autonomic fiber function was assessed using the noninvasive device Sudoscan™ (Impeto Medical, Paris, France), which performed an electrochemical skin conductance (ESC) test on the hands and feet. Sudoscan has previously been validated as a reliable, objective, and quantitative device when screening for diabetic peripheral neuropathy. 36 Age- and gender-stratified ESC thresholds for hands and feet were used. 37 Sural nerve conduction velocity (SNCV) and sural nerve amplitude potential (SNAP) were measured with the use of the handheld NC-stat® DPNCheck™ (NeuroMetrix, Inc., Waltham), recently demonstrated to have high reliability and acceptable accuracy compared with gold standard methods for the sural nerve. 38 Age- and height-stratified threshold limits for SNAP and SNCV were applied to identify abnormal results. 39 Patients were examined for bilateral abnormalities in SNAP and SNCV, but a composite measure, “sural nerve conduction” (SNC), was used if the patients had abnormalities in SNAP, SNCV, or both bilaterally.
DSPN was defined according to four categories. The label “possible DSPN” was given if the patient had symptoms of peripheral neuropathy assessed by questionnaires, or signs assessed by VPT and light touch and pain perception. If presence of symptoms and signs, the label “probable DSPN” was added. “Confirmed DSPN” was given if either the test for SNC or ESC was abnormal and if the patients had symptoms or signs. “Subclinical DSPN” was defined as the presence of abnormal SNC or ESC without symptoms or signs.
Measures of CAN
Three standard cardiovascular autonomic reflex tests (CARTs) and measures of 5-min resting heart rate variability (HRV) were used to evaluate CAN. All four tests were performed in a quiet examination room in the afternoon.
HRV measures were obtained after 5 min of supine rest. HRV indices were analyzed in time domain and frequency domain. Time-domain analyses included the root mean square of the sum of the squares of differences between consecutive R–R intervals (RMSSD) and standard deviation of normal-to-normal intervals (SDNN). Frequency-domain analyses included low-frequency power band (LF) (0.04–0.15 Hz), high-frequency power band (HF) (0.15–0.4 Hz), total frequency power (Total), and the ratio of low-frequency power/high-frequency power (LH/HF-ratio). 40
Following the 5-min resting HRV, the three CARTs recommended for diagnosing CAN were performed. The CARTs include the lying-to-standing test (30:15), the deep breathing test (E:I), and Valsalva maneuver. If one of the three CARTs was abnormal, the diagnosis “early CAN” was given. “Definite CAN” was diagnosed if two or three of three tests were abnormal. 9 Age-stratified thresholds of CARTs were used to identify abnormal results. 41
Resting HRV indices and CARTs were registered by using the device Vagus™ (Medicus Engineering, Aarhus, Denmark).
Questionnaires on peripheral neuropathy and exposures
All patients were asked to fill in the questionnaires Brief Pain Inventory (BPI) and Michigan Neuropathy Screening Instrument (MNSI) to assess the presence of symptoms of DSPN. Patients were considered having painful diabetic neuropathy if they, in the BPI questionnaire, answered having pain in both legs and/or both arms peripherally. 42 An MNSI score of ≥7 was interpreted as presence of neuropathy. 43
A questionnaire considering lifestyle factors such as smoking status (current, former, or never) and weekly amount of exercise was also filled in by each patient.
Blood pressure and anthropometric measures
Blood pressure and heart rate (HR) were measured after 10 min of rest and calculated as the mean of three consecutive measures performed with intervals of 1 min. Automated oscillometric blood pressure recorders were used (AND UA-787plus; A&D Medical, CA).
Height and weight were measured with clothes on but without shoes using a fixed rigid stadiometer (Seca, Chino) and an electronic scale (Mettler Toledo, Glostrup, Denmark), respectively.
Biochemical measures
All biochemical measures were analyzed from venous blood samples except for urine albumin and creatinine. Blood samples were drawn on the same day as the examination. The participants were nonfasting.
HbA1c was analyzed by high-performance liquid chromatography on a Tosoh G7 (Tosoh Corporation, Japan). C-peptide was measured using a Cobas e411 (Roche Diagnostics, Mannheim, Germany). Triglycerides, high-density lipoproteins, and total cholesterol were analyzed by standard enzymatic colorimetry techniques on a Vitros 5600 (Ortho Clinical Diagnostics, France). Serum low-density lipoprotein (LDL) cholesterol was calculated using the Friedewald equation. Plasma creatinine was analyzed by a two-point rate enzymatic technique. The Chronic Kidney Disease Epidemiology equation was used to estimate the glomerular filtration rate. 44 Urinary albumin-to-creatinine ratio was analyzed by quantitative immunological turbidimetry.
Medication
Data on medication and use of MDI and CSII were extracted from hospital electronic records and validated by the patient on examination day.
Statistical analysis
Patient characteristics are presented as means with standard deviation (SD) or in case of skewed distributions as medians with interquartile range [IQR].
Prevalence of the outcome measures of DSPN and CAN is presented in n and %.
All characteristics and prevalences were determined for the whole study population which was additionally stratified into subgroups according to CSII or MDI treatment.
Patients were excluded from a specific test if the values were missing.
The associations between the use of CSII as a determinant and measures of DSPN and CAN were analyzed by logistic regression for categorical outcomes. The results are presented as odds ratios with 95% confidence interval. The association between the duration of CSII treatment and neuropathy was analyzed in the subgroup of patients on CSII treatment. To avoid small-sample bias, determinants of DSPN and CAN were not included in the analyses if the number of affected patients was less than five.
Linear regression analyses were used for continuous outcomes. To meet model assumptions, outcomes were log-transformed before analysis and subsequently back-transformed to original scale, where appropriate.
Three models of adjustments were applied: model 1: age and gender; model 2: model 1+HbA1c and diabetes duration; model 3: model 2+systolic blood pressure, LDL cholesterol, triglycerides, current smoking, body mass index (BMI), and exercise. HR was included in the models when outcome was HRV measures.
The same method was applied to investigate the association between diabetes duration and measures of neuropathy. The abovementioned models of adjustments were used excluding diabetes duration as a confounder.
Adjusting for multiple testing was performed by the Benjamini–Hochberg procedure. 45
All analyses were performed in SAS 9.4 (SAS Institute, Cary, NC).
Results
Population characteristics
The 156 patients consisted of 65 males (41.7%) and 91 females (58.3%). Mean age of the study population was 22 years (SD 1.6) (range 18–24 years) and mean diabetes duration was 11.3 years (SD 5.1). Seventy-five patients (48.1%) were treated with CSII and the rest of the study cohort was treated with MDI. In the group treated with CSII, the median duration of CSII treatment was 85 months [IQR 36;113]. Mean BMI was 24.7 (SD 3.8), 35 patients (22.6%) were smokers, and 143 (92.3%) exercised regularly (pooled light and moderate/vigorous exercise) for 9 h weekly. HbA1c was 8.3% (IQR 7.4;9.2) (66.5 mmol/mol [IQR 58;77]), cholesterol 4.5 mmol/L (SD 1.1), and LDL 2.6 mmol/L (SD 0.9). All patients were on insulin. About 4% were in antihypertensive treatment and about 4% used psychotropics (selective serotonin reuptake inhibitor [SSRI], serotonin–norepinephrine reuptake inhibitors [SNRI], second-generation antipsychotics, and noradrenergic and specific serotonergic antidepressants [NaSSA]). A greater proportion of males were treated with MDI compared with CSII (n = 25 vs. n = 40). HbA1c in the groups of MDI and CSII were similar. Participant characteristics are presented in Table 1.
Characteristics of the Study Population
Data are given in means (SD), medians [IQR], or proportions %.
BMI, body mass index; CSII, continuous subcutaneous insulin infusion; eGFR, estimated glomerular filtration rate; HDL, high-density lipoproteins; IQR, interquartile range; LDL, low-density lipoproteins; MDI, multiple dose injections; NA, not applicable; SD, standard deviation.
Prevalence of neuropathy
Subclinical DSPN was diagnosed in 55.1% (n = 86). Prevalence of confirmed and possible DSPN was 2.6% (n = 4) and 3.2% (n = 5), respectively. None was detected with probable DSPN. Prevalence estimates of symmetric abnormal SNAP and SNCV were 23.8% (n = 36) and 37.1% (n = 56), respectively. The prevalence of pooled SNAP/SNCV (SNC) was 53.0% (n = 80). A total of 5.2% (n = 8) had abnormal ESC results on feet and 3.2% (n = 5) on hands. A total of 1.3% (n = 2) was detected with symmetrically abnormal VPT, 1.9% (n = 3) with BPI questionnaire, and none detected with abnormal results when testing light touch and pain perception nor with MNSI questionnaire.
Definite CAN was diagnosed in 9.0% (n = 14), and 28.1% (n = 43) had early CAN.
Only one patient was treated with beta-blockers and was excluded from the CAN measures. Six patients were excluded from the SNAP and SNCV measures because of incorrect use of the equipment (n = 4) and discomfort during the test (n = 2).
Distribution and prevalence estimates of the outcomes are presented in Figure 1 and Table 2.
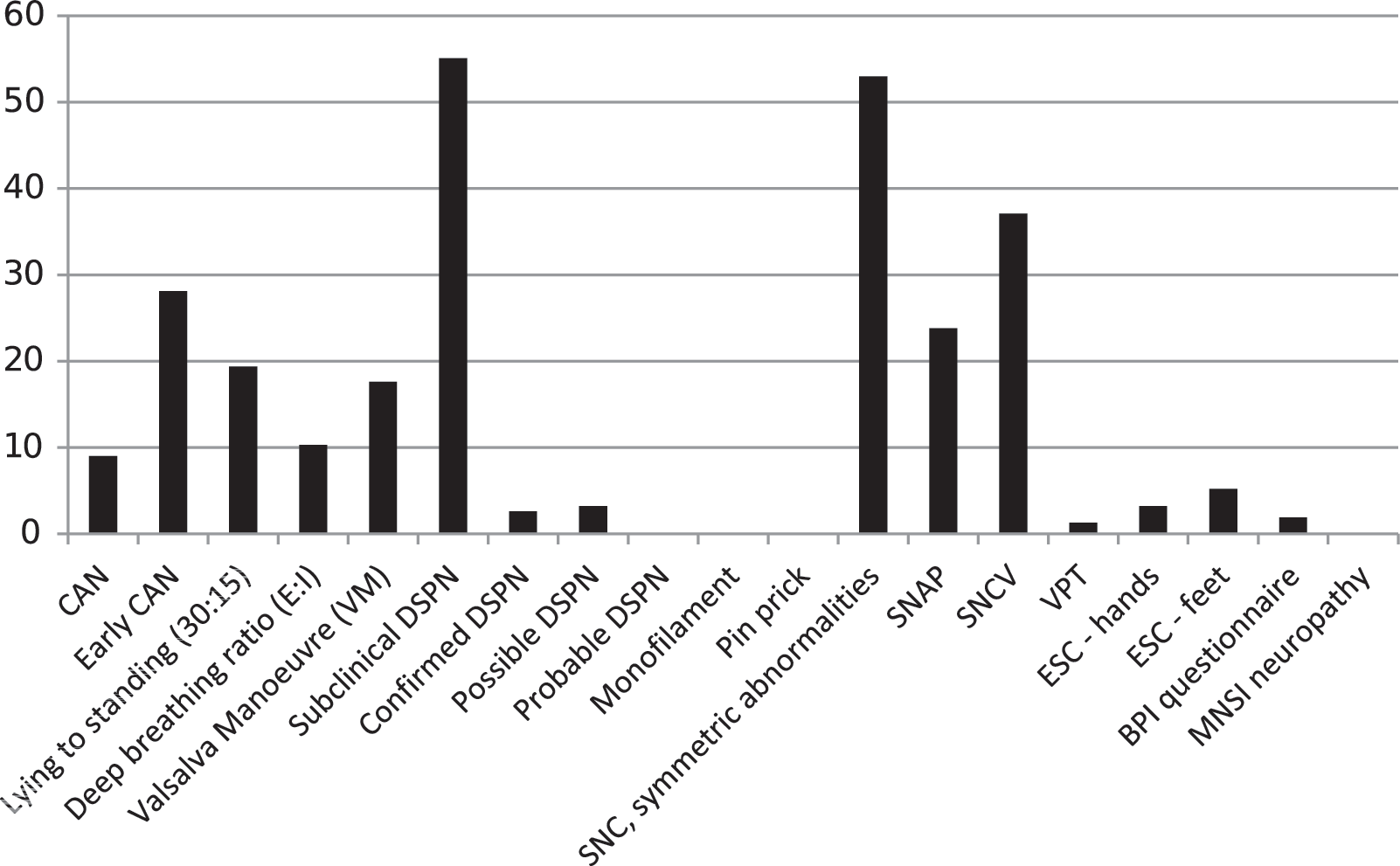
Prevalences of abnormal results of DSPN and CAN in a population of young adults with type 1 diabetes. Prevalences of neuropathy as composite endpoints and pathological tests as %. BPI, Brief Pain Inventory; CAN, cardiovascular autonomic neuropathy; DSPN, diabetic sensorimotor polyneuropathy; ESC, electrochemical skin conductance; MNSI, Michigan Neuropathy Screening Instrument questionnaire; SNAP, sural nerve amplitude potential; SNC, sural nerve conduction; SNCV, sural nerve conduction velocity; VPT, vibration perception threshold.
Distribution of Outcome Measures and Prevalences of Abnormal Results in a Population of Young Adults (18–24 Years) with Type 1 Diabetes
Data are given in means (SD), medians [IQR], or proportions.
BPI, Brief Pain Inventory; CAN, cardiovascular autonomic neuropathy; DSPN, diabetic sensorimotor polyneuropathy; ESC, electrochemical skin conductance; LF/HF ratio, low-frequency power/high-frequency power ratio; MNSI, Michigan Neuropathy Screening Instrument questionnaire; NA, not applicable; RMSSD, root mean square of the sum of the squares of differences between consecutive R–R intervals; SDNN, standard deviation of normal-to-normal intervals; SNAP, sural nerve amplitude potential; SNC, sural nerve conduction; SNCV, sural nerve conduction velocity; VPT, vibration perception threshold.
Association between diabetic neuropathy and CSII
There were no significant associations between the use of CSII and any of the measures of DSPN or CAN in models 1, 2, or 3. Estimates are presented in Table 3.
The Association Between Measures of Diabetic Neuropathy and Treatment with Insulin Pump
Model 1: adjusted for gender and age. Model 2: adjusted for age, gender, HbA1c, and diabetes duration. Model 3: adjusted for age, gender, HbA1c, diabetes duration, systolic blood pressure, LDL cholesterol, triglycerides, current smoking, BMI, and exercise. SDNN, RMSSD, LF, HF, LF/HF ratio, and Total are adjusted for HR in every model. Results are presented as OR for binary outcomes and estimates for continuous outcomes. Outcomes of DSPN are defined as presence of symmetric abnormal results. Binary outcomes were only included in the analyses if presence of 5 or more abnormal events.
No p-value was below 0.05.
CI, confidence interval; HR, heart rate; OR, odds ratios.
Also, no association was found between duration of CSII treatment and neuropathy outcomes. The estimates are shown in Table 4.
The Association Between Measures of Diabetic Neuropathy and Duration of Treatment with Insulin Pump in the Subgroup of Patients Treated with Insulin Pump
Model 1: adjusted for gender and age. Model 2: adjusted for age, gender, HbA1c, and diabetes duration. Model 3: adjusted for age, gender, HbA1c, diabetes duration, systolic blood pressure, LDL cholesterol, triglycerides, current smoking, BMI, and exercise. SDNN, RMSSD, LF, HF, LF/HF ratio, and Total are adjusted for HR in every model. Results are presented as OR based on logistic regression analyses for binary outcomes and estimates based on linear regression analyses for continuous outcomes. Outcomes of DSPN are defined as presence of symmetric abnormal results. Binary outcomes were only included in the analyses if presence of 5 or more abnormal events.
P < 0.05.
Association between diabetic neuropathy and diabetes duration
A significant association was found between type 1 diabetes duration and presence of subclinical DSPN (P = 0.009). However, the association was no longer significant when applying the Benjamini–Hochberg procedure. No other significant associations were found. Estimates are presented in Table 5.
The Association Between Measures of Diabetic Neuropathy and Duration of Diabetes
Model 1: adjusted for gender and age. Model 2: adjusted for age, gender, and HbA1c. Model 3: adjusted for age, gender, HbA1c, systolic blood pressure, LDL cholesterol, triglycerides, current smoking, BMI, exercise, and use of CSII. SDNN, RMSSD, LF, HF, LF/HF ratio, and Total are adjusted for HR in every model. Results are presented as OR based on logistic regression analyses for binary outcomes and estimates based on linear regression analyses for continuous outcomes. Outcomes of DSPN are defined as presence of symmetric abnormal results. Binary outcomes were only included in the analyses if presence of 5 or more abnormal events.
P < 0.05.
Discussion
This cross-sectional study, including 156 young adults with type 1 diabetes, shows that the prevalence of CAN was 9%, early CAN 28.1%, and subclinical DSPN 55.1%. Furthermore, no statistically significant associations between treatment with CSII and the measures of DSPN and CAN were found.
Cardiovascular autonomic neuropathy
The prevalence of CAN has previously been reported to vary between 3% and 75%. 14 –17,20 –22 With respect to younger patients, Tang et al. 21 have demonstrated a prevalence of CAN of 28% in a pooled cohort of 3943 children and young adults with type 1 diabetes, which is considerably higher than the prevalence of definite CAN in the present cohort study. The varying prevalence may be partially due to the applied diagnostic criteria used. According to the guidelines of the Toronto Consensus Panel on Diabetic Neuropathy, CAN should be assessed by applying the three CARTs used in the present study. 9 However, these diagnostic criteria have not been applied in any of the aforementioned studies in which a heterogenic array of methods such as HRV, pupil size determination, postural systolic blood pressure response, hand grip test, and baroreflex sensitivity have been used to diagnose CAN. 10,11,15 –17,20,27,28,46 In addition, CAN was diagnosed when only one abnormal CART was present, which may have resulted in a high CAN prevalence. 17,22
Diabetic sensorimotor polyneuropathy
As for CAN, the prevalence of DSPN varies in the literature (7%–62.5%) 14 –20 and has been assessed by different modalities such as nerve conduction, VPT, and cold/heat perception. 15 –17,19,28,46 For several studies, it is unclear if the reported abnormal results are symmetric or asymmetric. In addition, there is an inconstant use of age-, gender-, and height-stratified normal value thresholds. This makes comparisons between the present study and previous studies difficult. The Toronto Diabetic Neuropathy Expert Group 5 decided in 2009 on guidelines to assess DSPN, which take both symptoms, signs, and objective measures into account. However, the recommendations have not consequently been followed in subsequent studies.
An earlier study by Donaghue et al. 16 investigated diabetic neuropathy in 181 children and adolescents with type 1 diabetes with a lower average age compared with the average age in our study cohort (15 years vs. 22 years). Seven percent were detected with abnormal VPT. Age-stratified perception thresholds, similar to the applied threshold in the present study, were used. It is unclear if pathological VPT was assessed as bilateral deficits, if not, this may explain the difference in prevalence of abnormal VPT in the present study versus a study by Donaghue et al. (1.3% vs. 7%). Donaghue found a composite prevalence of DSPN (including VPT and thermal detection) of 24%, which is lower compared with the present study. Comparability is, however, compromised as the participants in the referred study were younger and measuring modalities differed.
A relatively high prevalence of subclinical DSPN (55.1%) was found in the present study. Majority of DSPN cases were identified by using novel, validated, and objective measures; ESC, SNAP, and SNCV. None of the patients was identified with monofilament, pinprick, or the MNSI questionnaire and very few had symmetric abnormal results of VPT (n = 2) and the BPI questionnaire (n = 3). Many established methods of assessing peripheral neuropathy such as monofilament, pinprick, thermal threshold perception, and VPT are biased by subjectivity; objective measures may therefore be more valid—especially in adolescents and young adults who may not have significant symptoms or sign yet. The high prevalence of subclinical DSPN identified in the study may indicate that these novel objective measures should be applied to detect DSPN in an early stage in young adults with type 1 diabetes before clinical manifestation.
CSII versus MDI
We found no association between CSII treatment or treatment duration and the measures of DSPN and CAN. These findings are not in line with previous studies. A study of 989 adolescents with type 1 diabetes aged between 12 and 20 years demonstrated that CSII treatment was associated with lower rates of peripheral neuropathy assessed by thermal threshold testing but not CAN assessed by HRV. 34 Kwai et al. demonstrated in a study, consisting of 41 patients with type 1 diabetes and a mean age of 28 years, that patients treated with MDI had abnormalities of nerve excitability assessed by an axonal ion channel function test compared with patients treated with CSII. 35 Reverse causation due to the cross-sectional design may bias our results if, for example, patients with large glucose fluctuations due to autonomic neuropathy are more likely to receive CSII treatment. Furthermore, when dividing the participants into CSII and MDI, the number of subjects with abnormal results of DSPN and CAN is relatively small, possibly causing a type II error when examining the association with CSII.
HbA1c levels in patients treated with CSII and MDI were fairly similar (8.3% [67 mmol/mol] versus 8.2% [66 mmol/mol], respectively), indicating that CSII- and MDI-treated patients had similar glucose control. These findings have been demonstrated previously. 34
Strengths and limitations
Recommended, novel, and established methods of detecting DSPN and CAN were used, which is a considerable strength in our study and may give a more detailed description of the nerve function.
It may be possible that more resourceful young adults chose to participate in the study after receiving the written invitation, which could have caused selection bias. We tried to avoid this bias by additionally inviting the young adults orally and by providing detailed information about the study.
Having a healthy control group was not in the scheme of the study but would have enabled a comparison with age- and gender-matched nondiabetic young adults.
It is recommended that patients avoid test confounders such as smoking, use of several drugs, and meals, before testing for CAN. 9 These recommendations were not met and may have affected CAN measures.
Generalizability
Steno Diabetes Center Copenhagen is specialized in treating diabetes, and young adults with type 1 diabetes regularly visit the Steno Diabetes Center Copenhagen to evaluate and optimize their treatment. In general, young adults with type 1 diabetes are offered to regularly visit a diabetes outpatient clinic and should therefore be able to receive similar management, making the study generalizable. However, in some cases, different settings such as long distance between home and the clinic or fewer follow-ups may result in impaired treatment.
Conclusion
This study has demonstrated that DSPN and CAN are prevalent in young adults with type 1 diabetes when using novel measuring modalities. Furthermore, the prevalence is similar in patients treated with CSII and MDI.
The prevalence of CAN is relatively low compared with other studies conversely. Prevalence of subclinical DSPN is relatively high compared with existing literature. The lack of consensus on diagnosing diabetic neuropathy and the use of heterogeneous measuring modalities may explain differences in prevalence rates. The relatively high prevalence of subclinical DSPN found in this study may be due to the novel and possibly more sensitive methods applied. Moreover, in our study, included patients were significantly older than in most of the reported studies. 15,17,21,22,24,34 The development of diabetic neuropathy may be more prevalent in young adults compared with children 14 and affected by puberty, 27,28 also explaining the higher identified prevalence of DSPN.
Type of insulin therapy was not associated with measures of DSPN and CAN in contrast with other studies. However, more studies with larger study populations compared with the present study are needed to prevent possible type II errors. No significant difference was seen between HbA1c levels in patients treated with CSII and MDI, which may indicate that metabolic control in the two groups was fairly similar. Diabetes duration was not associated with measures of neuropathy.
Taken together, diabetic neuropathy is prevalent in young adults with type 1 diabetes and as it has been suggested that diabetic neuropathy in early stages is reversible, adolescence may be an optimal time to screen for neuropathic defects. By applying novel perhaps more sensitive measuring methods, it may be possible to detect neuropathy at early stages.
However, interventional studies demonstrating an effect of intensified treatment are needed before implementing screening for early signs of neuropathy, as this may cause undue concern.
Footnotes
Acknowledgments
The Augustinus Foundation, 15–2274. The Toyota Foundation, BG 8687. The foundations had no involvement in the conducted research or preparation of the article.
Authors' Contributions
M.M.B.C. has contributed to the design of the study, acquired, analyzed and interpreted data, drafted the article, and approved the final version to be published. E.E.H., M.E.J., B.J.v.S., and J.F. have contributed to the design of the study, analyzed and interpreted data, revised the article critically, and approved the final version to be published. C.S.H. has contributed to the design of the study and acquisition, analysis and interpretation of data. He has revised the article critically and approved the final version to be published.
Author Disclosure Statement
J.F. holds stocks in Medicus Engineering. No other potential conflicts of interest relevant to this article were reported.