
Abstract
Dear Editor:
Hypoglycemia remains an unresolved complication of insulin therapy. Continuous glucose monitoring and artificial pancreas systems have mitigated, but not eliminated, the risk of hypoglycemia for people with type 1 diabetes. 1,2 The risk of hypoglycemia is particularly pronounced during and after exercise and in individuals with hypoglycemia unawareness. 3 Several groups are developing fully integrated dual-hormone artificial pancreas systems, which deliver insulin or glucagon in response to changes in glucose as an additional approach to maintain euglycemia. Dual-hormone systems have been shown to improve time in range and hypoglycemia as compared with usual care 4 –6 and also to improve time in hypoglycemia as compared with an insulin-only artificial pancreas system. 7 The dose of glucagon required per day is variable depending on factors such as a person's physical activity and the glucagon dosing algorithm, but typically ranges from 0.033 to 0.82 mg/day. 8 Dual-hormone systems hold the potential to reduce hypoglycemia, but there are potential risks with the chronic administration of glucagon, and to be realized, these systems require a stable-in-solution glucagon analogue suitable for chronic use. 9
Dasiglucagon is a novel glucagon analogue stable in an aqueous formulation. In a randomized double-blind trial in patients with type 1 diabetes comparing pharmokinectic and pharmacodynamic characteristics, dasiglucagon was well tolerated and had characteristics similar to GlucaGen. 10 The principal effect of glucagon is to increase circulating glucose through increased hepatic glycogenolysis and to a lesser degree gluconeogenesis. Glucagon also has other known physiological effects including decreasing gut motility and increasing satiety, glomerular filtration, water reabsorption, cardiac output, and heart rate. 11 What we describe here is a toxicity study with dasiglucagon to determine whether the results of chronic administration of dasiglucagon are consistent with exaggerated pharmacological effects of glucagon and to support the chronic use of dasiglucagon, including within a dual-hormone artificial pancreas system.
Rats and dogs were dosed subcutaneously daily for 26 and 39 weeks, respectively, in 4 groups of 20 rats with 0 (vehicle), 0.5, 2, or 8 mg/(kg·day); 4 groups of 4 beagle dogs with 0, 0.02, 0.1, or 0.3 mg/(kg·day). Delayed toxicity and recovery for any findings noted within the treatment period was evaluated after a 4-week treatment-free period in both studies. Assessment of toxicity was based on clinical observations, food consumption, body weight measurements, ophthalmic observations, ECG measurements (dogs only), hematology, clinical chemistry, urinalysis, macroscopic pathology, and histopathology. Blood samples were collected for exposure evaluations on week 1 and week 26/week 39 (rats/dogs), respectively, of the dosing phase and for antidrug antibody evaluations on week 1 and week 26/week 39 of the dosing phase and week 4 of the recovery phase. Samples for analysis of plasma glucose and insulin concentrations were taken post-dose at week 26/week 39 (rats/dogs), respectively.
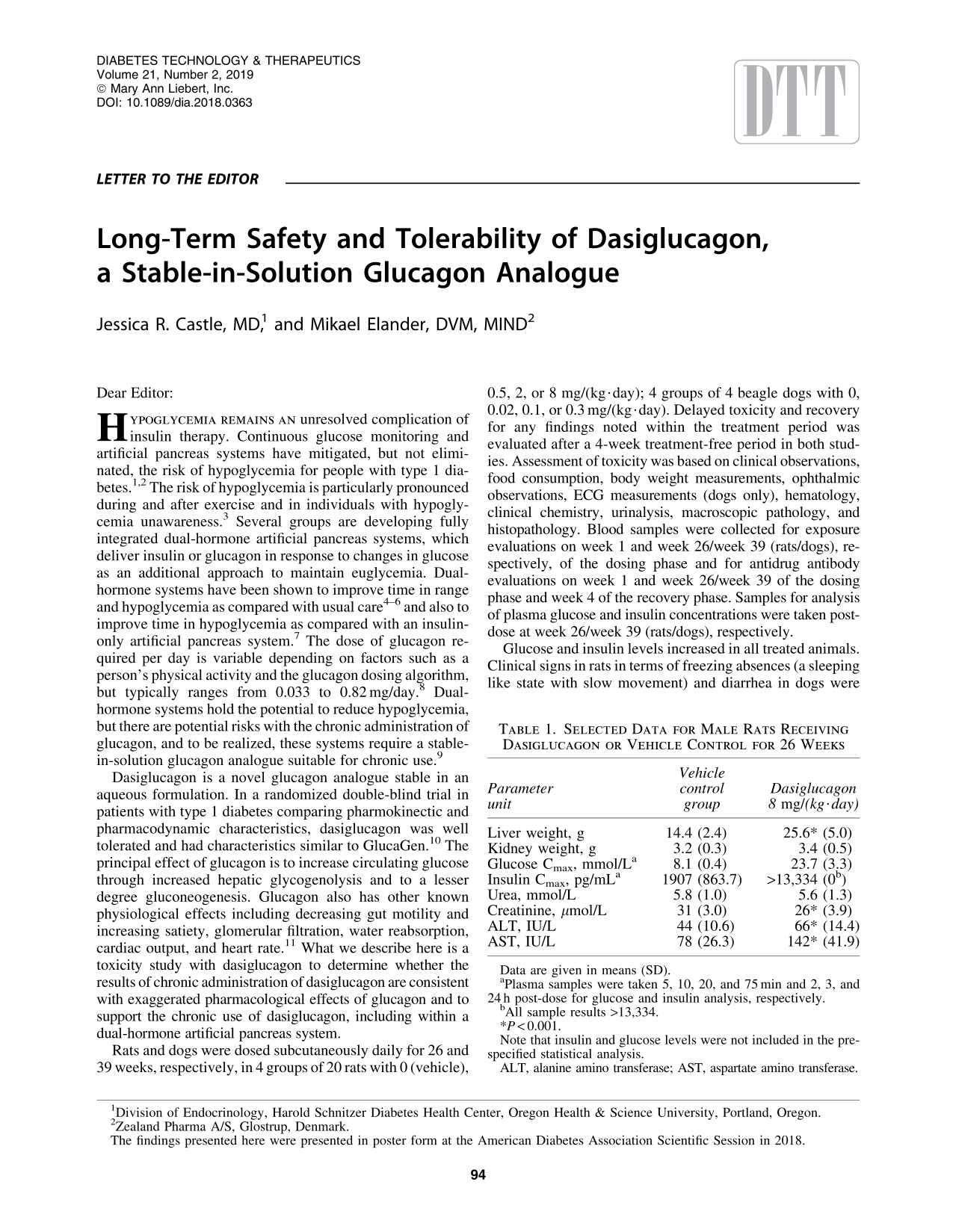
Glucose and insulin levels increased in all treated animals. Clinical signs in rats in terms of freezing absences (a sleeping like state with slow movement) and diarrhea in dogs were noted. Heart rate increased in dogs at the 0.1 and 0.3 mg/(kg·day) dose level, which correlated with increased heart weights noted in both rats and dogs. Liver and kidney weights increased at all dose levels in both species, and microscopic pathology demonstrated increase in hepatocyte glycogen vacuolation and increased incidence of chronic progressive nephropathy in rats and hyaline/granular casts in the kidneys in dogs. The hepatocyte glycogen vacuolation was associated with increases in alanine amino transferase and aspartate amino transferase. The markers of kidney function, creatinine and urea, were not increased despite the histopathological changes. See Table 1 for a detailed summary of the findings. All findings showed full/partial recovery after 4-week treatment-free periods. A dose-dependent increase in antidrug antibodies was noted. The no observed adverse effect level dose of 2 mg/(kg·day) in rats and 0.1 mg/(kg·day) in dogs represents exposure multiples (area under the curve) of 22 and 2 compared with anticipated human doses of up to 1 mg/day.
Selected Data for Male Rats Receiving Dasiglucagon or Vehicle Control for 26 Weeks
Data are given in means (SD).
Plasma samples were taken 5, 10, 20, and 75 min and 2, 3, and 24 h post-dose for glucose and insulin analysis, respectively.
All sample results >13,334.
P < 0.001.
Note that insulin and glucose levels were not included in the pre-specified statistical analysis.
ALT, alanine amino transferase; AST, aspartate amino transferase.
The change in behavior in rats described as freezing absences has not previously been reported for glucagon, but a comparative study (Table 2) showed that this behavioral change is noted after administration of both dasiglucagon and glucagon. These clinical signs were not seen in other species used for toxicity testing of dasiglucagon (mice, rabbits, or dogs). In a study wherein glucagon was administered in a dual-hormone artificial pancreas for up to 11 days to patients with type 1 diabetes, 4 there were no comparable effects to the freezing absences in rats, supporting that this behavioral change is specific to rats administered a glucagon receptor agonist.
Clinical Signs in Male Rats Receiving Dasiglucagon or Glucagon
Incidence reflects number of animals with at least one observation of freezing absences throughout the 4-week treatment period.
Glucagon dose selected to give comparable pharmacodynamic response as dasiglucagon at 2 mg/(kg·day).
The diarrhea noted in dogs is related to the known effects on gastrointestinal motility for glucagon. Hepatocyte glycogen accumulation likely occurred in these animals as they were not diabetic and they were not on insulin therapy. In this setting, dasiglucagon administration led to hyperglycemia that stimulated insulin release, to a maximal insulin concentration of more than sevenfold in the rats treated with 8 mg/(kg·day), which, in turn, stimulated glycogen storage (Table 1). The risk of glycogen accumulation is not considered relevant for humans treated with dasiglucagon to maintain euglycemia as excessive glycogenesis is induced by a combination of hyperglycemia and hyperinsulinemia. 12
The histopathological changes noted in the kidneys of both rats and dogs are normal background findings in these species that may have been exacerbated by the increase in glomerular filtration rate. As these histopathological changes are species specific and are not considered relevant for humans, the increase in glomerular filtration rate is and may impose an increased workload on the kidneys. The development of antidrug antibodies was not associated with changes in pharmacodynamic properties, indicating that these were not neutralizing. There were no occurrences of vasculitis or other secondary findings relating to the antidrug antibodies. In addition, there were no skin findings, including no evidence of local toxicity at the injection sites.
In summary, the chronic administration of dasiglucagon in animals multiple times above relevant human doses was well tolerated. All findings were consistent with the known pharmacological effects of glucagon, with the exception of the freezing absences in rats, which is specific only to rats and occurs with both glucagon and dasiglucagon, and the accumulation of hepatic glycogen, which occurred in the setting of marked hyperglycemia and hyperinsulinemia in nondiabetic animals. Limitations of this study include that the insulin levels in the group receiving the highest dose of dasiglucagon were above the upper limit of the assay and, therefore, the degree of hyperinsulinemia in this group is unknown. In addition, the standard toxicology testing described here was done in animals without diabetes, which do not mimic the physiology of type 1 diabetes. The hypothesis that hepatic glycogen accumulation would not occur in insulin-deficient animals with diabetes was not tested and further studies are needed to test this hypothesis. Also, toxicity testing in animals is necessary before testing in humans but testing in animals without diabetes does not replace testing in people with type 1 diabetes. These findings support long-term human testing of dasiglucagon in dual-hormonal artificial pancreas systems.
Footnotes
Author Disclosure Statement
J.R.C. has received honorarium from Zealand Pharma (advisory boards), Novo Nordisk (advisory boards), and Dexcom Inc (consulting), and she has received research funding from Xeris Pharmaceuticals. M.E. is an employee of Zealand Pharma.