
Abstract
Background:
This two-center pilot study combined for the first time an intra-arterial glucose sensor with a decision support system for insulin dosing (SGCplus system) in critically ill patients with hyperglycemia.
Methods:
Twenty-two patients who were equipped with an arterial line and required iv insulin therapy were managed by the SGCplus system during their medical treatment at the intensive care unit.
Results:
Time to target was 111 ± 195 min (80–150 mg/dL) and 135 ± 267 min (100–160 mg/dL) in the lower and higher glucose target group. Mean blood glucose (BG) was 142 ± 32 mg/dL with seven BG values <70 mg/dL. Mean daily insulin dose was 62 ± 38 U and mean daily carbohydrate intake 148 ± 50 g/day (enteral nutrition) and 102 ± 58 g/day (parenteral nutrition). Acceptance of SGCplus suggestions was high (93%).
Conclusions:
The SGCplus system can be safely applied in critically ill patients with hyperglycemia and enables good glycemic control.
Background
Both hyper- and hypoglycemia are associated with increased mortality in critically ill patients. 1 Discussions on safe target ranges are still ongoing. Current international guidelines recommend moderate glycemic control (110–180 mg/dL) without hypoglycemia. 2 To achieve this goal, frequent blood glucose (BG) measurements and according titration of insulin infusion rates are required which lead to increased workload for nursing staff.
Automated insulin titration algorithms incorporated into perfusor pump systems have shown to enable good glycemic control without increased hypoglycemia rates. In these studies, glucose values were measured using blood gas analyzers or point of care devices available in critical care units and were manually entered into the algorithm. 3 –5
In the present study, we combined for the first time the novel intra-arterial glucose sensor with the SGC system (a decision support system for insulin dosing in critically ill patients) in intensive care unit (ICU) patients with hyperglycemia. This combination, the SGCplus system, allows direct communication between glucose sensor, perfusor pumps, and the decision support system and shall facilitate glycemic management in critically ill patients.
Materials and Methods
This prospective, single-arm, two-center pilot study evaluated the feasibility of using the SGCplus system in critically ill patients with hyperglycemia requiring intravenous insulin infusion. Patients were hospitalized for any cause at either a medical or neurosurgical ICU.
The primary objective of this study was to investigate the functionality of the SGCplus system for glycemic control in critically ill patients for the whole length of continuous intravenous insulin treatment at the ICU with a maximum duration of 12 days.
Secondary objectives included accuracy of the SGCplus sensor, as well as safety and usability of the SGCplus system in the ICU setting. Secondary variables were as follows: SGCplus accuracy, percentage of time within predefined BG target, time to target, blood sampling frequency, insulin dose, enteral/parenteral nutrition, and adherence to SGC advice.
Main inclusion criteria were as follows: age ≥18 years, requirement for both arterial catheter and intravenous insulin therapy as judged by the treating physician. Exclusion criteria included pregnancy or breastfeeding and known insulin allergy.
The study was approved by the respective local Ethics Committees, Austrian health authority, and registered at the German Clinical Trials Register (
Study procedures
Patients who were equipped with an arterial line due to their underlying clinical condition (e.g., for hemodynamic monitoring or blood gas analyses) and required intravenous insulin to control their BG were enrolled into SGCplus treatment. The intervention phase started with initiation of SGCplus therapy and ended when SGCplus therapy was no longer required or the arterial access was lost without clinical indication of reinsertion.
SGCplus (three perfusor pumps with a user interface [Space Control] and a hardware module connected to Space Control; Fig. 1) is a decision support system for insulin dosing in critically ill patients. The system automatically derives information from infusion pumps administering parenteral and enteral nutrition and, under consideration of this information, suggests adaptions to the insulin dose once these nutrition rates are changed. The SGCplus systems requests glucose measurements in intervals between 30 min and 4 h, depending on glycemic stability of the patient, as defined by the model predictive control algorithm, integrated in the system. Based on the glucose levels and parenteral and enteral nutrition rates, the algorithm calculates an adjustment to the insulin infusion, which is directly transmitted to the insulin pump, connected with the system.
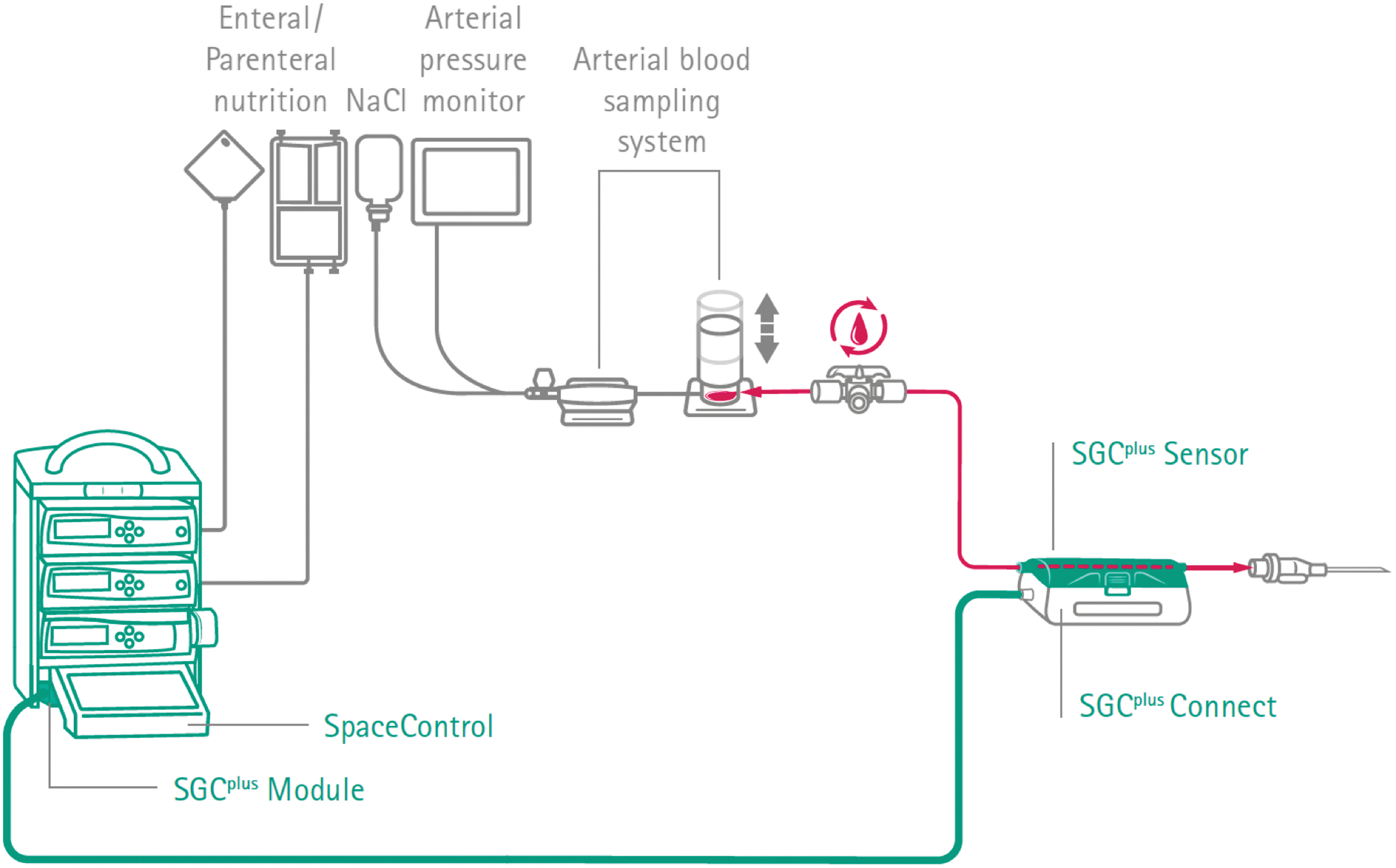
SGCplus system. Color images are available online.
The SGCplus system also provides an in vivo semiautomated arterial glucose measurement feature. The disposable optical glucose sensor with a lifetime of 4 days is located extracorporeally directly in the arterial access line of the patient, adjacent to the arterial catheter. The sensor does not interfere with arterial blood pressure monitoring or arterial blood sampling as required for other laboratory purposes.
Glucose measurement using SGCplus is activated via manual aspiration of arterial blood using the standard in-line arterial blood sampling system. As soon as the arterial blood reaches the disposable sensor, glucose measurement is activated and the signal is transmitted and displayed at the central user interface of the SPACE infusion system. The aspirated arterial blood sample is reinfused into the patients' artery. The measured glucose value is transferred to the insulin dosing algorithm embedded in SGCplus, which then provides a suggestion for the new insulin rate and the next BG sampling interval. The glucose sensor is based on optical fluorescence measurement using the enzyme glucose oxidase.
Within the study, the SGCplus system was operated by the nurse in charge. Both measured glucose level and insulin rate had to be confirmed by the nurse for a plausibility check. For study purpose, each BG sample was also measured using standard blood gas analyzer (Radiometer (ABL 90 FLEX (Medical University of Graz) and ABL 800 (Karl Landsteiner University St. Pölten), both Drott Medizintechnik GmbH, Wiener Neudorf, Austria)) to determine system accuracy. Whenever required by SGCplus, calibration was performed using BG data from standard blood gas analyzer.
Medical care for the underlying condition(s) was provided by the physician in charge. Amount and route of nutrition administration were at the discretion of the physician in charge. Arterial lines were otherwise treated as under routine conditions and flushed after use with saline solution. Heparin was administered for the treatment if required by the underlying condition or withheld in case of bleeding or thrombocytopenia; heparin was not used to flush the arterial line.
Two BG target ranges could be used within the study and were selected according to the treating physician's discretion: 80–150 or 100–160 mg/dL. The number of requested calibrations during the whole treatment time was collected excluding the initial calibrations of a new sensor and the daily recalibrations.
Statistical analyses
It was aimed to include 20–25 patients in this pilot study. Based on previous studies, it was expected to obtain 1000 measurements with this number of patients which is a representative sample size. 3 –5 Data are presented as mean ± standard deviation or median (IQR) if not otherwise specified. Categorical variable summaries included the frequency and percentage of patients who were in a specific category. Statistical analysis was performed using the statistical analysis software SAS®.
Results
Twenty-two critically ill patients (15 neurosurgical and seven medical) were enrolled. A historical control group of 22 medical intensive care patients requiring intravenous insulin infusion to control glycemia was used to compare efficacy of SGCplus to control glycemia. Clinical characteristics of both groups are indicated in Table 1.
Clinical Characteristics of the Investigated Study Population
CHO, carbohydrates; SAPS, Simplified Acute Physiology Score; TISS-28, Therapeutic Intervention Scoring System-28.
SGCplus performance
One thousand eight hundred forty-five SGCplus-based BG determinations were performed during 131 study days. The success rate of SGCplus-based BG determinations was 75%. Everyday 15.9 ± 5.3 SGCplus-based BG measurements were performed. Time to proposed next BG determination was 111 ± 72 min. A total of 0.8 ± 0.8 calibrations per day were required. A total of 68 sensors were used during the study. Mean number of sensor changes was 2.8 ± 1.7. 31 early sensor changes due to early sensor failure or loss of arterial line were required.
Sensor accuracy
Median absolute relative difference (MARD) was 5.1 (interquartile range 2.3; 8.4)% median. Sensor performance was worst in hypoglycemia and best in eu- and hyperglycemia. Data on MARD per glycemic range as well as separately indicated for patients with and without diabetes are reported in Table 2. Sensor agreement with reference glucose within 15 mg/dL (<100 mg/dL) or 15% (≥100 mg/dL) of reference glucose values according to ISO 15197:2013 was 89.3% (1236 out of 1384).
Parameters of Glycemic Control and Sensor Performance for the Overall Population and Separated for Patients With and Without Diabetes
BG, blood glucose; CV, coefficient of variation; MARD, mean absolute relative difference.
Data on system accuracy were assessed by Clarke Error Grid (Fig. 2). Clarke Error Grid analysis showed 99.8% of paired values in clinically acceptable error zones A and B. One value was located in zone C (0.07%) and two values in zone D (0.14%). The Bland–Altman analysis (Fig. 3) showed a tendency of SGCplus sensor to underestimate glucose −4.1 mg/dL (95% CI: −35.4 to 27.2) compared to reference.

Clarke error grid for SGCplus BG sensor versus reference over the course of treatment. 99.8% of values were located in the clinically benign zones A and B. One value was located in zone B and two values in zone D. BG, blood glucose.
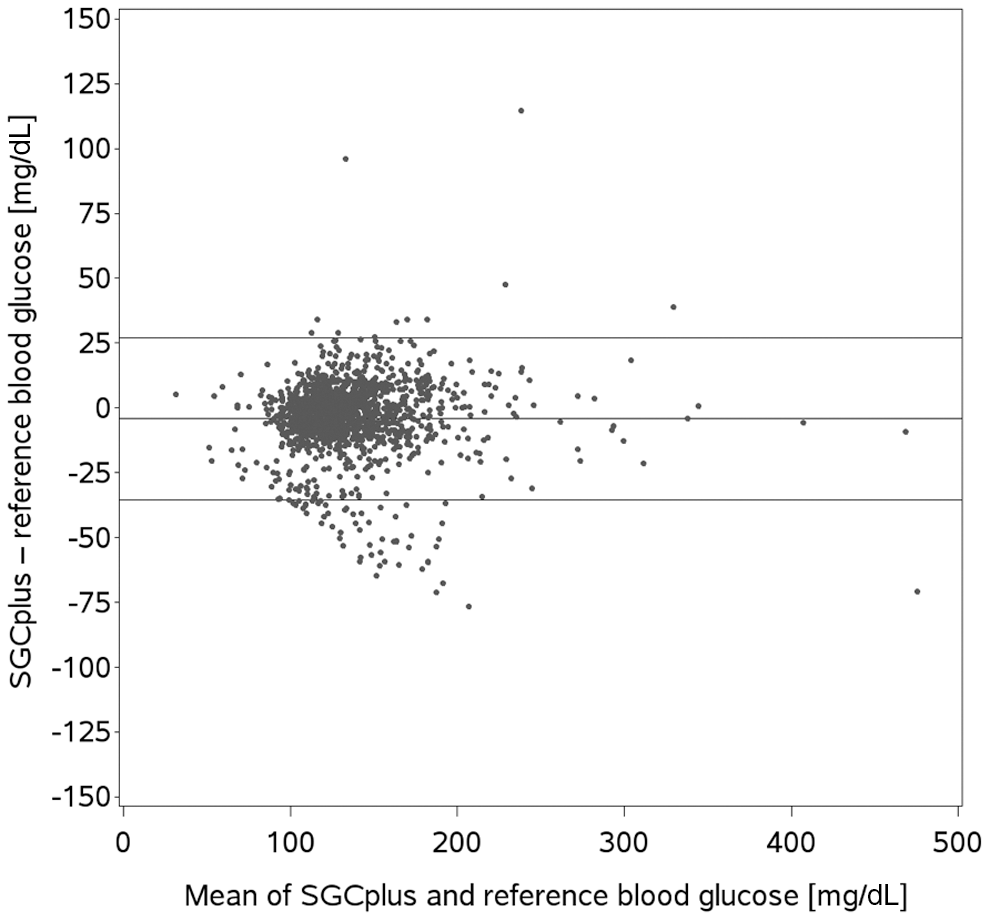
Bland–Altman plot for SGCplus BG—reference over the course of treatment (mean: −4.1 mg/dL [95% CI: −35.4 to 27.2]).
Diabetes management
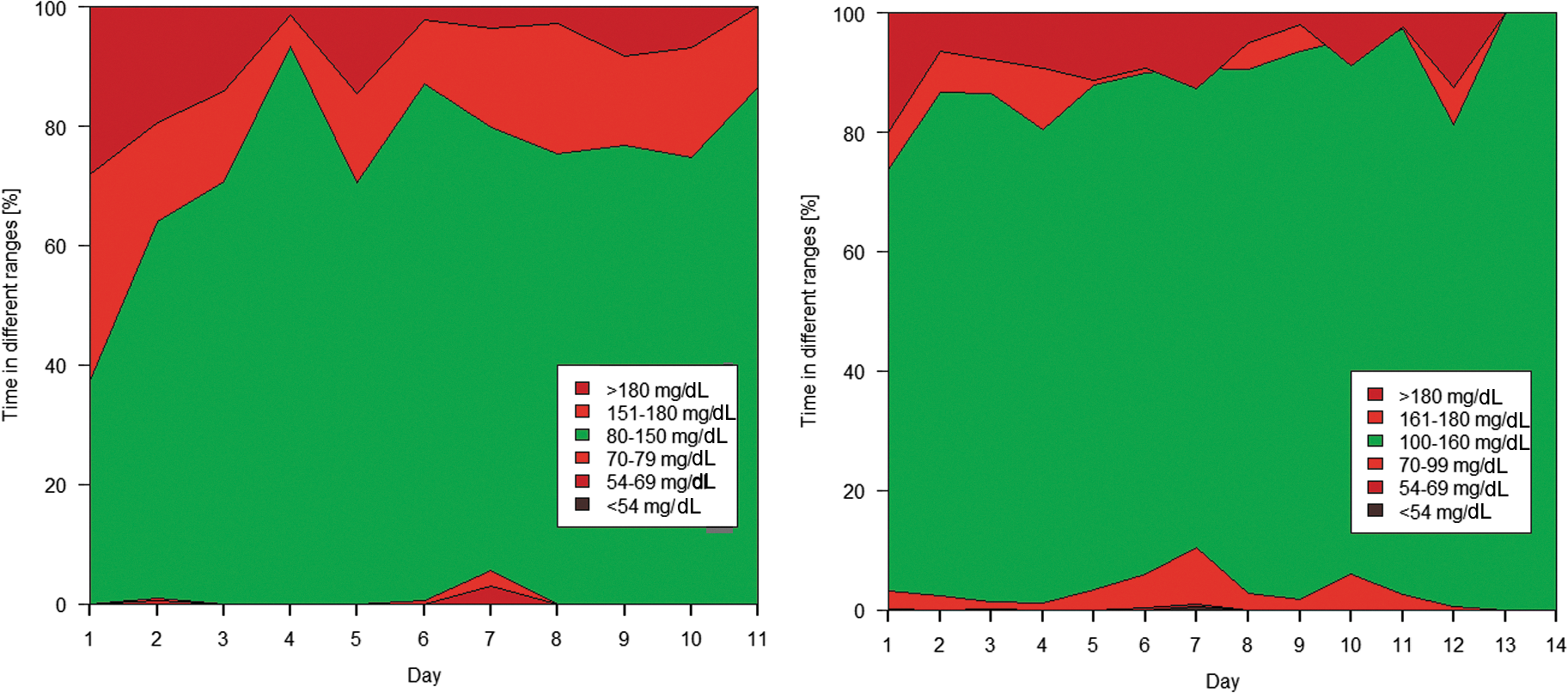
Mean treatment duration was 6.0 ± 3.8 days. SGCplus suggestions were accepted in 93%. Six patients were assigned to the lower and 10 to the higher target range; 6 patients were allocated initially to the lower and subsequently to the higher target range. Time to target was 111 ± 195 and 135 ± 267 min; BG measurements were 72% and 84% of the time within the allocated target ranges (80–150 and 100–160 mg/dL, respectively). Distribution of times in prespecified target ranges over the course of treatment is shown in Figure 4 (Fig. 4A, more stringent; Fig. 4B less stringent).
Mean BG across all subjects was 137 ± 45 mg/dL for the lower and 134 ± 27 mg/dL for the higher target range. Evolvement of mean BG over the course of treatment is depicted in Figure 5. The degrees of fluctuation in BG values per subject and treatment day are detailed in the Supplementary Tables S1, S2, S3, S4. A total of seven events <70 mg/dL occurred. Mean daily insulin dose was 62 ± 38 IU. Mean daily carbohydrate intake was as follows: 148 ± 50 g/day (enteral) and 114 ± 50 g/day (parenteral nutrition). There was a tendency for higher BG and higher insulin requirements in patients with preexisting diabetes when compared with those without (Table 2). No differences in hypoglycemia were observed.
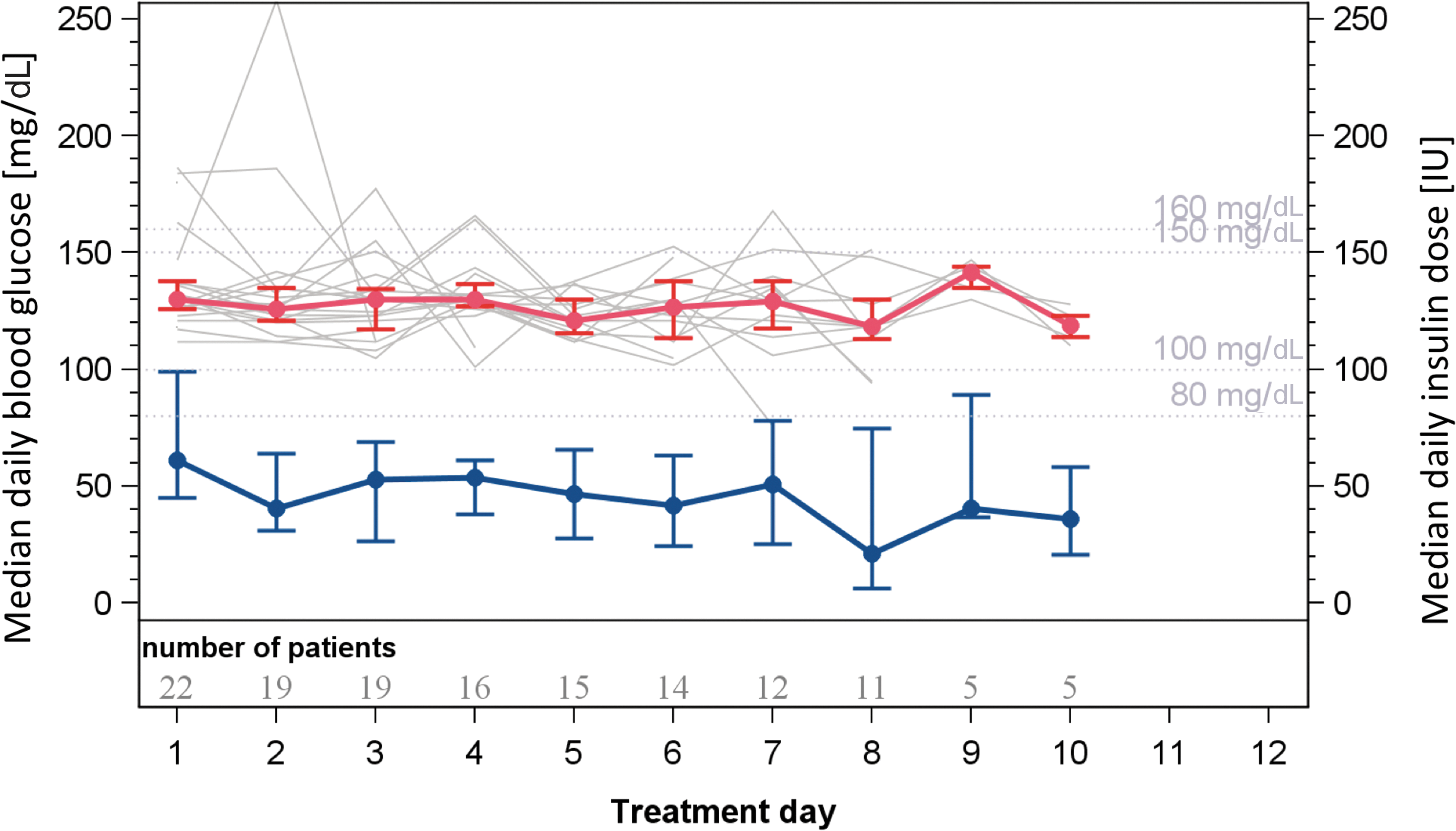
BG and insulin dose over the course of treatment. Data are median daily BG with Q1 and Q3 error bars (red line) as well as individual median daily BG values per subject (gray lines). Median daily insulin dose is indicated in blue. Color images are available online.
Discussion
We report the results of the first clinical trial using the SGCplus system in critically ill patients. In previous studies, only the SGC system without incorporated intra-arterial glucose sensor was used. Our study indicates that the SGCplus system could be safely and efficaciously used for diabetes management in critically ill patients without increasing the risk of hypoglycemia.
Current guidelines on diabetes management for critically ill patients suggest that insulin therapy should be started in case of sustained hyperglycemia (≥180 mg/dL) aiming at a target glucose range of 140–180 mg/dL. More stringent goals (<140 mg/dL) should only be targeted if it can be achieved without relevant hypoglycemia. 6 Target ranges, however, are still under debate and might differ for different patient groups. 7
Frequent BG monitoring was done and continuous intravenous insulin infusion was administered based on validated written or computerized protocols that adjust the infusion rate according to fluctuations in insulin requirements that are recommended in the critical care setting. 2 In the ICU, mainly blood from arterial, venous, or capillary sources is used for glucose measurements. Increasing focus on safe diabetes management has evoked the debate whether the interstitial space as used in diabetes care at home is a feasible site in the critically ill as well. 8 As an alternative to the interstitial space, intravascular (semi-) continuous glucose monitoring has been suggested and explored by various device manufacturers. 9
Sechterberger et al. have compared intra-arterial (GluCath IA-CGM, GluMetrics, Inc.) versus subcutaneous continuous glucose monitoring (FreeStyle Navigator; Abbott Diabetes Care) in eight postoperative cardiac surgery patients in the ICU. 10 Out of 183 data pairs, 85.8% and 84.2% of measurements met ISO 15197:2003 criteria (within 20%). MARD between systems was also comparable (12.3% ± 11.3% vs. 11.1% ± 8.3%).
In contrast, a recent study performing a head-to-head comparison of a subcutaneous (Sentrino® sCGM System, Medtronic) versus intravasal sensor (GlucoClear® iCGM System, Edwards) in 20 cardio-surgical ICU patients has shown superior performance of the intravasal technology (MARD 12.3% vs. 7.2%). 11 With an overall MARD of 5.1 (2.3; 8.4)% and fulfilment of 89.3% of the even stricter ISO 15197:2013 criteria, SGCplus showed a better performance of previously tested systems.
Currently, four electronic decision support systems for insulin titration are available for use in critical care (SGC by B. Braun, GlucoCare by Pronia Medical Systems, Glucommander by Glytec Systems and GlucoStabilizer by Indiana University Health), none of which has incorporated a glucose sensor. A direct comparison of the four systems is impeded as all systems use different target ranges and definitions of hypoglycemia.
For GlucoStabilizer, the target is set at 80–110 mg/dL in the ICU setting. The system used to treat 2398 ICU patients over a period of 18 months. In these patients, 61.0% of BG measurements were in the target range of 80–110 mg/dL and 90.9% were in the wider target range of 60–150 mg/dL. The rate of hypoglycemic episodes (<50 mg/dL) was low: 0.4%. 12 The latest generation of GlucoCare has a set glucose target of 140 mg/dL to allow safe glycemic control while mitigating the risk of hypoglycemia. A mean BG of 146.4 mg/dL and hypoglycemia rates (<70 mg/dL) of 0.04% could be achieved. 13
In a multicenter, randomized controlled trial where ICU patients were randomized to Glucommander versus paper protocol, patients treated by Glucommander had a lower mean BG (103 ± 8.8 mg/dL vs. 117 ± 16.5 mg/dL, P < 0.001) and achieved a higher percentage of BG readings within the target range (71.0% ± 17.0% vs. 51.3% ± 19.7%, P < 0.001). Time to target was shorter for Glucommander compared to standard care (4.8 ± 2.8 h vs. 7.8 ± 9.1 h, P < 0.01). The percentages of patients with more than 1 severe hypoglycemic event (<40 mg/dL) and hypoglycemia (<60 mg/dL) were 3.9% and 42.9% for Glucommander versus 5.6% and 31.9% for standard care (P > 0.1). 14
In our study, time to target (80–150 and 100–160 mg/dL) was faster (111 ± 195 and 135 ± 267 min) and achievement of time in target was comparable and even slightly superior (72% and 84%, respectively). Time in target, however, has to be compared with caution as Glucommander's target range is lower and more stringent (80–120 mg/dL) than the target ranges of SGCplus (80–150 and 100–160 mg/dL). This is also reflected by mean BG achieved by Glucommander (103 ± 8.8 mg/dL) versus SGCplus (141 ± 32 mg/dL). In contrast, more patients were affected by hypoglycemia when treated with Glucommander compared to SGCplus: 3.9% versus 0.0% for severe hypoglycemia (<40 mg/dL) and 31.9% versus 4.5% for nonsevere hypoglycemia (<60 mg/dL vs. <54 mg/dL).
SGC with point-of-care BG determination was tested in a multicenter trial in a total of 508 patients. 5 The median (IQR) time in target (79–150 mg/dL) was 83.0% (68.7–93.1) of time. Four severe (<40 mg/dL) hypoglycemic events occurred (0.01% of all BG measurements); in 0.2% (0–1.4) of the time BG was in the range of 40–77 mg/dL. In patients with BG above target at study start, median time to target was 4.5 h (IQR 2.3–8.3), in 7 (2.3%) patients the target was not achieved. SGC advices on insulin infusion rate were accepted in 99.6% of cases by the users.
Glucose targets in SGCplus are less stringent than in the other systems limiting a direct comparability of results. However, our data reflect results on time in target as seen by Blaha et al. 5 when using SGC without integrated glucose sensor (83% vs. 84% at 80–150 mg/dL for SGC vs. SGCplus, respectively). Hypoglycemia rates are comparably low and acceptance rates for insulin dose suggestions were high in both studies (99.6% vs. 93% for SGC vs. SGCplus, respectively). Minor differences in acceptance rates might be attributed to the only small number of patients included in our study compared to the large-scale study of Blaha et al. (22 patients vs. 508 patients).
As also observed in studies with decision support systems on the general ward, acceptance rates by staff increased over time. 15,16 The introduction of new technology evokes natural skepticism in users often leading to a reduction of insulin doses. As the user gains experience with a new technology, acceptance rates usually increase if the system proved to be safe.
Compared to a historic control group where the local standard infusion protocol was used, SGCplus achieved better glycemic control (178 ± 65 mg/dL vs. 141 ± 32 mg/dL). This is a similar finding as seen with Glucommander where electronic decision support was superior to paper protocols. 14
Glycemic variability has gained importance in recent years as several studies have reported an association of higher glycemic variability with increased ICU mortality. 17 –19 SGCplus use resulted in reduced glycemic variability compared to standard care (standard deviation of glucose: 32 mg/dL vs. 65 mg/dL). This is in line with other electronic insulin dosing algorithms. 14
Larger studies in a broader spectrum of critically ill patients are needed to determine whether glycemic variability is a modifiable risk factor for patients with hyperglycemia. In light of the possibility of reducing glycemic variability and thus the rate of hypoglycemia by means of electronic decision support systems, the question of the optimal target range for glucose control in critically ill patients has to be reappraised. Could critically ill patients benefit from a tight glycemic control after all?
Several limiting factors need to be acknowledged. First, the study was a single-arm study without a prospective control group as the primary aim of the study was to show that SGCplus can be used under routine conditions in critical care. The number of patients included in this pilot was rather small, as 1000 performances of BG measurements was the primary focus to show feasibility of the SGCplus system. Furthermore, the system was only tested in two patient populations (neurosurgical and medical ICU patients) and was compared to a historical cohort. Future studies will thus need to include different patient groups to assess generalizability of results and should evaluate intra-arterial versus CGM-based systems for glucose control with and without formal algorithms for adjustment of insulin doses. 20,21
Conclusions
Data from the study suggest that SGCplus can be safely applied in critically ill patients with hyperglycemia. SGCplus sensor BG data proved to be accurate and can be used for insulin titration. The decision support component proved efficient in steering insulin therapy. Acceptance rates of treatment suggestions were high. Glycemic control was comparable as seen with other titration protocols with low number of hypoglycemic events. 22,23 Future studies will need to prove superiority to current state-of-the-art techniques in a larger set of patients.
Footnotes
Acknowledgments
The authors thank Christian Krainer (Joanneum Research GmbH) for data management and Jutta Claus, (B. Braun) and Sarah Bischof (Medical University of Graz) for data monitoring. Heike Fries (B. Braun) contributed to study planning and design and Georg Tomberger (B. Braun) provided technical support. We want to thank the patients for their participation in the study. Funding: This study was funded by B. Braun Melsungen.
Authors' Contribution
J.K.M., A.C.R., and P.E. drafted the article. J.K.M., V.T.-S., T.A., and J.K.M. designed and performed the study, interpreted data, and contributed to discussions. B.L. and T.A. performed statistical analyses and reviewed the article. M.M., C.M., A.R., and K.E.-R. performed the study. All authors critically revised the article and approved the final version of the article. J.K.M. is the guarantor of this work.
Author Disclosure Statement
J.K.M. is a member in the advisory board of Becton-Dickinson, Boehringer Ingelheim, Eli Lilly, Medtronic, Prediktor SA and Sanofi, and received speaker honoraria from Abbott Diabetes Care, Astra Zeneca, Eli Lilly, Dexcom, Novo Nordisk, Roche Diabetes Care, Sanofi, Servier, and Takeda. P.E. received speaker honoraria from Jazz Pharma. The remaining authors declare no conflict of interest.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.