
Abstract
Background:
To compare the impact of two sodium–glucose cotransporter 2 (SGLT2) inhibitors, tofogliflozin and ipragliflozin, on hypoglycemia in patients with type 2 diabetes mellitus (T2DM), treated with sulfonylureas.
Methods:
Thirty patients with T2DM were allocated to treatment with either 20 mg/day tofogliflozin or 50 mg/day ipragliflozin and underwent continuous glucose monitoring (CGM) for 5 days at three times in a crossover manner.
Results:
The percent time spent at glucose <70 mg/dL per 24 h was 0.48, 2.77, and 0.06%, before treatment with SGLT2 inhibitors and treatment with ipragliflozin and tofogliflozin, respectively (P = 0.1135, difference between SGLT2 inhibitors). The addition of either ipragliflozin or tofogliflozin to sulfonylureas markedly and significantly improved other CGM-derived parameters, including average plasma glucose, standard deviation of glucose, mean postprandial glucose excursion, percent time with glucose >140, >180 mg/dL, and >200 mg/dL, area over the curve <70, area under the curve >140, >180, and >200, and maximum and minimum plasma glucose. However, there were no significant differences in these parameters between the two SGLT2 inhibitors.
Conclusions:
Based on the CGM, the addition of tofogliflozin to sulfonylureas tended to decrease the percent time spent in hypoglycemia in T2DM patients. The addition of SGLT2 inhibitors to sulfonylureas improved the average glucose level and reduced glucose fluctuations without increasing the time in hypoglycemia.
Introduction
Anumber of large-scale clinical studies, such as the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) 1 and the Action to Control Cardiovascular Risk in Diabetes (ACCORD) 2 trials, have demonstrated that strict glycemic control through intensive insulin therapy, contrary to expectations, increases mortality rate, based on increased incidence of hypoglycemic episodes and weight gain.
The reactive hyperemia index (RHI) is an index of endothelial function that reflects early arteriosclerosis; and is measured noninvasively with the EndoPAT. We reported previously that RHI does not correlate with mean blood glucose levels measured by glycated hemoglobin A1c (HbA1c) levels or by continuous glucose monitoring (CGM). 3 Our results, however, showed significant correlation between RHI and time in hypoglycemia and time at blood glucose level of ≥200 mg/dL, based on CGM, as well as CGM markers of fluctuations in blood glucose level, including standard deviation (SD), mean amplitude of glycemic excursion (MAGE), and mean postprandial glucose excursion (MPPGE). 3
It was concluded that avoidance of hypoglycemia and large fluctuations in blood glucose levels is an important aspect of treatment of diabetes mellitus and prevention of diabetes-related macroangiopathy.
Sodium–glucose cotransporter 2 (SGLT2) inhibitors exhibit pleiotropic effects in patients with type 2 diabetes mellitus (T2DM). For example, they stabilize blood glucose levels as well as reduce body weight and/or visceral fat, reduce blood pressure, improve lipid levels (e.g., reduce triglyceride and increase high-density lipoprotein cholesterol levels), lower uric acid level, minimize insulin resistance, and ameliorate fatty liver.
The Empagliflozin Cardiovascular Outcome Event Trial (EMPA-REG OUTCOME) 4 and the Canagliflozin Cardiovascular Assessment Study (CANVAS) 5 concluded that administration of SGLT2 inhibitors significantly improved the primary endpoint (improvements in three-point major adverse cardiovascular events). Furthermore, the EMPA-REG OUTCOME also showed a reduction in all-cause mortality rate following treatment with SGLT2 inhibitors. 4 The results suggested that these effects are class effects common to SGLT2 inhibitors, thus boosting the use of SGLT2 inhibitors worldwide.
The use of SGLT2 inhibitors is considered to be associated with a relatively low risk of hypoglycemia. This effect is thought to be mediated through the following mechanisms: (1) enhanced glucose production, (2) glucose reabsorption by the residual function of sodium–glucose cotransporter 1 (SGLT1) located downstream of the renal tubules, 6 –8 and (3) transient increase in the concentrations of SGLT2 inhibitors in the gastrointestinal tract. The latter mechanism is based on the observation that although canagliflozin and ipragliflozin are inferior to other SGLT2 inhibitors with regard to their selectivity for SGLT2 over SGLT1, they can inhibit SGLT1 in the gastrointestinal tract. 9 These properties raise the question on whether differences in selectivity for SGLT2 can affect clinical outcome.
In this regard, tofogliflozin, which is 2900 times more selective for SGLT2 than for SGLT1, 10 has the highest selectivity among the SGLT2 inhibitors. In contrast, ipragliflozin is only 860 times more selective for SGLT2 than for SGLT1. Tofogliflozin is already approved in Japan, and ipragliflozin is already approved in Japan and Korea. In the present study, we used CGM to compare the effects of tofogliflozin and ipragliflozin on hypoglycemia in patients with T2DM, particularly those treated with oral sulfonylureas. Our objective was to test whether the more selective drug, tofogliflozin, is better than the less selective drug, ipragliflozin, in reducing the incidence of hypoglycemia in patients treated with sulfonylureas.
Methods
Subjects
The study participants were 30 T2DM patients, ages 20–75 years, who had been treated at study entry with sulfonylurea for ≥7 days, and were hospitalized at the University of Occupational and Environmental Health Japan, Department of Endocrinology, Metabolism and Diabetes between July 2015 and June 2017. We excluded patients treated with insulin, SGLT2 inhibitors, and those with severe liver dysfunction (aspartate aminotransferase >100 IU/L), estimated glomerular filtration rate (eGFR) of <45 mL/min/1.73 m2, body mass index (BMI) <22.0 kg/m2, and those with history of cerebral infarction. Although no exclusion was imposed based on the use of oral glucose-lowering agents other than SGLT2 inhibitors at the time of admission, changes of such agents were prohibited throughout the study.
The study was approved by the ethics review committee of our university. The study was explained in detail to the participants in writing, and written consent was obtained at study enrollment. All biological samples were processed appropriately according to the Declaration of Helsinki. The trial is registered with the University Hospital Medical Information Network (UMIN) (No. UMIN 000018265).
Study design
This study was a randomized-controlled, open-label, and crossover study; 30 subjects were allocated randomly in a 1:1 ratio by the permuted block method to treatment with either 20 mg/day tofogliflozin or 50 mg/day ipragliflozin (Fig. 1). In the tofogliflozin precedence group, tofogliflozin was administered at 20 mg after breakfast from day 6 of admission, withdrawn at day 12, and then replaced from day 14 of admission with 50 mg ipragliflozin. In the ipragliflozin precedence group, ipragliflozin was administered at 50 mg after breakfast on day 6 of admission and continued at the same dose till it was withdrawn on day 12, and then switched from day 14 of admission to 20 mg tofogliflozin. We did not change the dose of sulfonylurea during the study period.
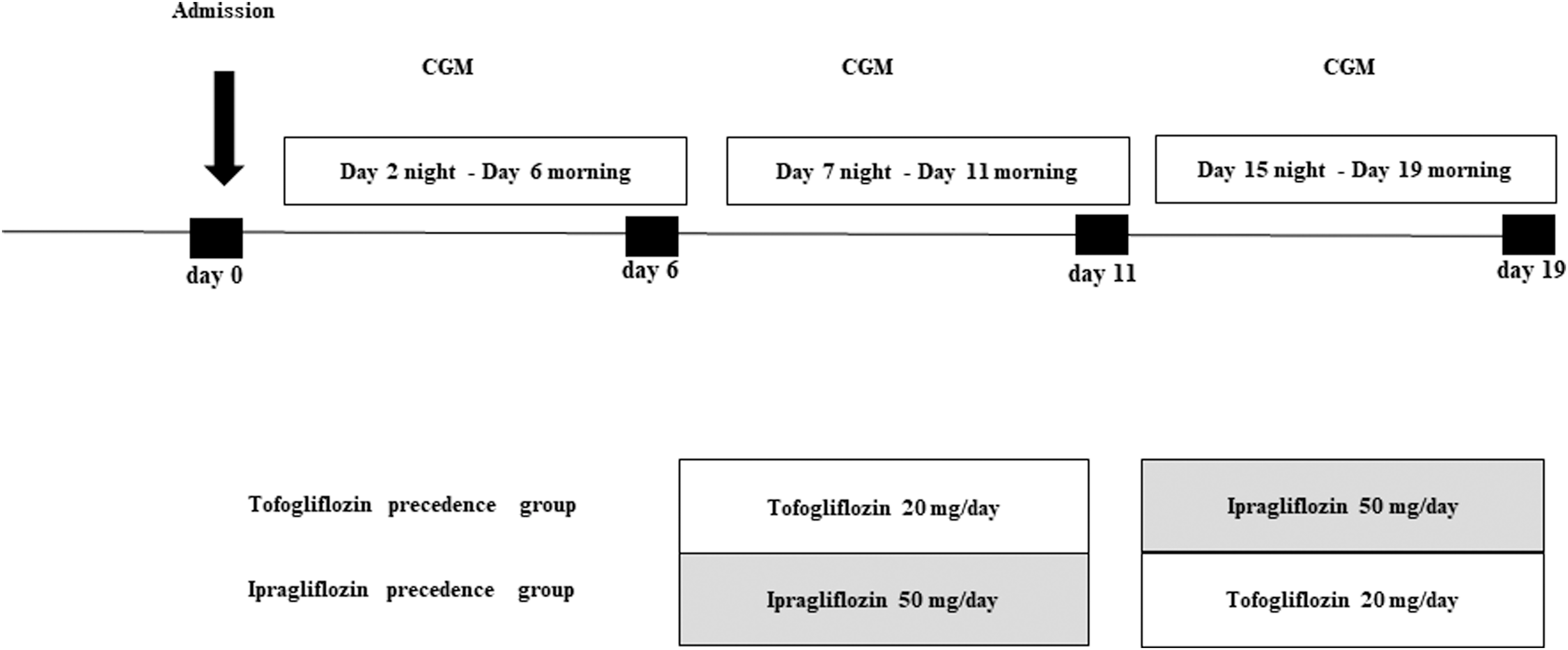
Study design. This study was a randomized-controlled, open-label, and crossover study; type 2 diabetes patients treated with insulin were allocated at random to additional treatment with either 20 mg/day tofogliflozin or 50 mg/day ipragliflozin. In the tofogliflozin precedence group, participants were treated with 20 mg tofogliflozin after breakfast from day 6 of admission till day 12–13, and then switched from day 14 to 50 mg ipragliflozin. In the ipragliflozin precedence group, participants were treated with 50 mg ipragliflozin after breakfast from day 6 of admission till day 12–13, and then switched from day 14 to 20 mg tofogliflozin. We did not change the dose of sulfonylurea during the study period.
All participants wore a CGM (ipro2®; Medtronic, Inc., Fridley, MN) from the night of day 2 of admission for 5 days (pretreatment), from the night of day 7 of admission for 5 days (first SGLT2 inhibitor), and from the night of day 15 of admission for 5 days (second SGLT2 inhibitor). Thus, each patient underwent 5-day CGM three times in a crossover manner. The data used for analysis were obtained on day 4 of CGM to ensure stability. No changes were made to diet or exercise therapy or drugs (except the SGLT2 inhibitors).
The primary outcome measure was the percent time over 24 h with glucose at <70 mg/dL (time <70), as recorded by CGM, under the two SGLT2 inhibitors. The secondary outcome measures were SD of glucose, MPPGE, percent time at glucose >140 mg/dL, percent time at glucose >180 mg/dL, percent time at glucose >200 mg/dL, area over the curve <70, area under the curve (AUC) >140, AUC >180, AUC >200, and maximum and minimum plasma glucose levels, as determined by CGM, and these were compared between the two SGLT2 inhibitors.
Statistical analyses
Patient demographics were summarized using descriptive statistics or contingency tables. The difference between tofogliflozin and ipragliflozin was analyzed using a mixed-effects model with treatment sequence, period and treatment as fixed effects, case as random effects, and baseline values as covariates. The efficacies of pretreatment and tofogliflozin or ipragliflozin within each group were compared using the paired t-test. In all analyses, P < 0.05 was considered statistically significant. All statistical analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC).
Clinical laboratory tests
Blood samples were collected early in the morning after at least 12-h fasting. Urinary C-peptide reactivity levels were measured in 24-h urine samples. Measurement of each parameter was outsourced to SRL Co., Ltd. (Tokyo, Japan) and conducted using standard methods. All samples were stored at −80°C until analysis.
Meal tolerance test
A meal tolerance test (MTT) was performed in all subjects. After at least 12-h fasting, patients underwent an MTT with a test meal. The test meal contained 450 kcal (protein 15.3%, carbohydrate 51.4%, and lipids 33.3%). We measured plasma glucose, proinsulin, insulin, c-peptide, glucagon, active glucagon-like peptide-1, gastric inhibitory polypeptide, and free fatty acid (FFA) at fasting, and after 30, 60, and 120 min of meal ingestion.
Results
Study population characteristics
Table 1 shows the baseline characteristics of the participating patients. Of the 30 participants, 16 were males. The mean age of participants was 54.7 years. The mean duration of diabetes was 8.1 years. Participants were mildly obese, with mean BMI of 29.0 kg/m2. Renal function was normal, with eGFR of 90.9 mL/min/1.73 m2. Laboratory tests on admission showed poor blood glucose control, with mean HbA1c of 9.1%. In addition, the subjects were insulin resistant on average, with a mean homeostasis model assessment as an index of insulin resistance of 3.3 and urine C peptide immunoreactivity level of 112.8 μg/day. Treatment included gliclazide in 21 patients (average dose 33 mg/day), glimepiride in 9 patients (average dose 1.2 mg/day), dipeptidyl peptidase 4 (DPP4) inhibitor in 16 patients, metformin in 9 patients, α-glucosidase inhibitor in 2 patients, and thiazolidine in 1 patient.
Patient Demographics Recorded on Admission
Data are mean ± SD or number (range: minimum–maximum).
α-GI, alpha-glucosidase inhibitor; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DPP4 inhibitor, dipeptidyl peptidase 4 inhibitor; eGFR, estimated glomerular filtration rate; γ-GTP, gamma-glutamyl transpeptidase; HbA1c, glycated hemoglobin A1c; HOMA-IR, homeostasis model assessment as an index of insulin resistance; SD, standard deviation.
Changes in CGM-based glucose parameters
Figure 2 shows the CGM recordings of patients before treatment with SGLT2 inhibitor (Fig. 2A), treatment with tofogliflozin (Fig. 2B) and ipragliflozin (Fig. 2C), in the following: Supplementary Figure S1 shows the CGM recordings of all patients before treatment with SGLT2 inhibitor (Supplementary Fig. S1A), treatment with tofogliflozin (Supplementary Fig. S1B) and ipragliflozin (Supplementary Fig. S1C). Figure 3 shows the mean values of continuous plasma glucose recorded by the CGM for all patients before treatment with SGLT2 inhibitor, and during cotreatment with ipragliflozin and tofogliflozin.

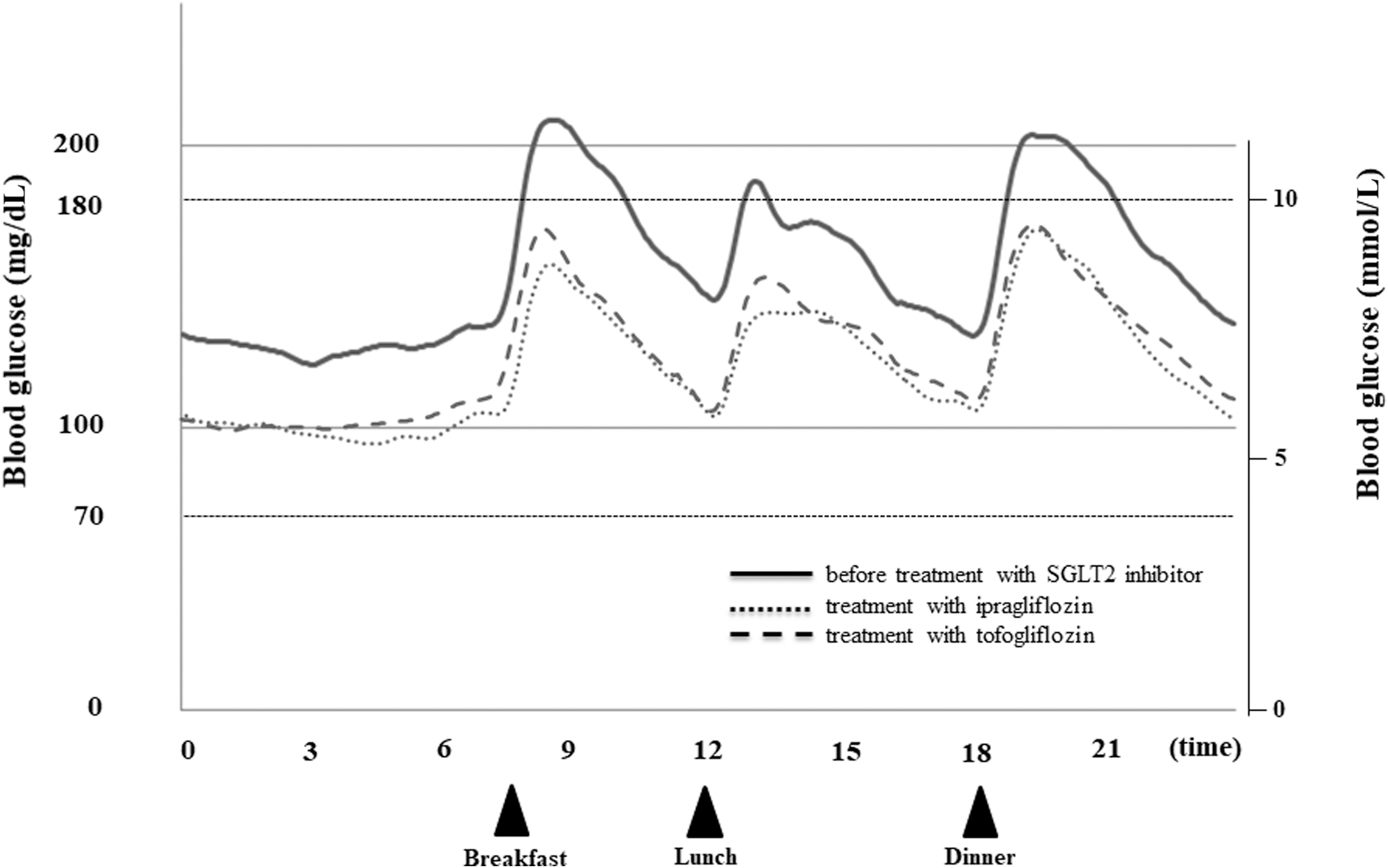
Mean values of continuous plasma glucose levels measured by CGM in all participants before treatment with SGLT2 inhibitor, and during treatment with ipragliflozin and tofogliflozin.
The primary outcome measure (time <70) before treatment with SGLT2 inhibitors was 0.48% and decreased during treatment with tofogliflozin (0.06%) but increased with ipragliflozin (2.77%) (P = 0.1135, difference between the two SGLT2 inhibitors).
With regard to the secondary outcome measures, the area over the curve <70 before treatment with SGLT2 inhibitors and during treatment with ipragliflozin and tofogliflozin was 0.06, 0.30, and 0.004 mg/dL*day, respectively (P = 0.097, difference between the two SGLT2 inhibitors). Other CGM-derived parameters, including average plasma glucose, SD of glucose, MPPGE, percent time with glucose >140, >180, and >200 mg/dL, area over the curve <70, AUC >140, >180, and >200, and maximum and minimum plasma glucose, were markedly and significantly improved during treatment with either ipragliflozin or tofogliflozin; and there were no significant differences in these parameters between the two SGLT2 inhibitors (Table 2).
Changes in Glucose Parameters Detected by Continuous Glucose Monitoring
Data are mean ± SEM.
P values represent the difference in changes from baseline between tofogliflozin and ipragliflozin, by an ANCOVA model with the order of administration, timing of administration, and treatment as fixed effects, case as random effects, and baseline values as covariates. The efficacies of pretreatment and tofogliflozin or ipragliflozin within each group were compared using the paired t-test.
ANCOVA, analysis of covariance; MPPGE, mean postprandial glucose excursion; SEM, standard error of mean.
Changes in total blood ketone bodies and glucose excretion
The mean total blood ketone bodies before treatment with SGLT2 inhibitors were 262 ± 215 μmol/L and increased during treatment with ipragliflozin and tofogliflozin to 508 ± 374 and 548 ± 559 μmol/L, respectively (P = 0.7354, difference between the two SGLT2 inhibitors). Also, the mean glucose excretion before treatment with SGLT2 inhibitors was 7.11 ± 1.79 g/day and increased during treatment with ipragliflozin and tofogliflozin to 43.49 ± 4.02 and 43.01 ± 4.02 g/day, respectively (P = 0.9331, difference between the two SGLT2 inhibitors). There were no significant differences in total blood ketone bodies and glucose excretion between the two SGLT2 inhibitors.
Meal tolerance test
Table 3 shows changes in AUC from 0 to 120 min (AUC0–120) of metabolic parameters recorded during the MTT before and after treatment with SGLT2 inhibitors. The AUC0–120 of plasma glucose, proinsulin, and FFA markedly and significantly improved by treatment with either ipragliflozin or tofogliflozin (AUC0–120 of insulin improved significantly during treatment with tofogliflozin), but there were no significant differences in these parameters between the two SGLT2 inhibitors.
Changes in AUC0–120 of Metabolic Parameters Detected by Meal Tolerance Test
Data are mean ± SEM.
P values represent the difference in change from baseline between tofogliflozin and ipragliflozin, by an ANCOVA model with the order of administration, timing of administration, and treatment as fixed effects, case as random effects, and baseline values as covariates. The efficacies of pretreatment and tofogliflozin or ipragliflozin within each group were compared using the paired t-test.
AUC, area under the curve; AUC0–120, AUC from 0 to 120 min; FFA, free fatty acid; GIP, gastric inhibitory polypeptide; GLP-1, glucagon-like peptide-1.
Safety
No serious side effects were observed during the study period. Hypoglycemia developed in two cases (blood glucose level: 60, 61 mg/dL) before the addition of SGLT2 inhibitor, two cases (59, 67 mg/dL) treated with tofogliflozin and five cases (40, 41, 57, 61, 63 mg/dL) treated with ipragliflozin. However, severe hypoglycemia associated with disturbance of consciousness or requiring medical intervention did not occur.
Discussion
The results of the present study showed that in patients with T2DM treated with sulfonylureas, the addition of either SGLT2 inhibitor improved and stabilized blood glucose levels, without increasing the frequency of hypoglycemic episodes. The present study investigated whether the difference between tofogliflozin and ipragliflozin in their selectivity for SGLT2 can explain their effectiveness in reducing the incidence of hypoglycemia in patients treated with sulfonylurea. The results showed no significant difference between the two inhibitors, although the percent time spent in hypoglycemia tended to be lower with tofogliflozin, which has higher selectivity for SGLT2, than ipragliflozin. Furthermore, although there were no significant differences in hypoglycemia-associated parameters, hypoglycemia was occasionally more frequent during the night and before each meal in patients on ipragliflozin than in those cotreated with tofogliflozin (Fig. 2).
Hypoglycemia was observed in two cases before treatment with SGLT2 inhibitors, in two cases with tofogliflozin, and in five cases with ipragliflozin in this study. In the tofogliflozin group, both patients had hypoglycemia when using the second drug, which is more likely to cause hypoglycemia. On the contrary, two patients in the ipragliflozin group had hypoglycemia despite using the first drug. Although the two patients had hypoglycemia with ipragliflozin as the first drug, there was no hypoglycemia when using tofogliflozin as the second drug. Thus, it may be a possibility of the difference of selectivity for SGLT2.
In their experimental study, Nagata et al. 12 reported that phlorizin (PHZ), but not tofogliflozin, enhanced urinary glucose excretion during hypoglycemic episodes and further aggravated hypoglycemia. In the same study, normoglycemic rats were administered SGLT2 inhibitors of different selectivity (e.g., tofogliflozin 400 ng/mL or PHZ 1333 ng/mL) to examine their effects on urinary glucose excretion, intrinsic gluconeogenic capacity, and blood glucose levels. The results showed that under hypoglycemic conditions induced by the glucose clamp technique, tofogliflozin neither inhibited glucose reabsorption nor increased urinary glucose excretion. 11
Our previous CGM-based study that assessed the early effects of treatment with SGLT2 inhibitors on blood glucose levels in T2DM patients showed a close correlation between urinary glucose excretion level after administration of SGLT2 inhibitor and the lowest blood glucose level. 12 Considered together, the above results point to a mechanism of action of SGLT2 inhibitors that fine tunes the level of urinary glucose excretion in the presence of low blood glucose levels.
Several studies have used CGM to investigate the effects of SGLT2 inhibitors in patients with T2DM treated with insulin. However, to our knowledge, there are no studies that have used CGM to evaluate the effects of different of SGLT2 inhibitors in patients with T2DM treated with sulfonylureas. In a study using CGM, Takeishi et al. 13 investigated the effects of 20 mg tofogliflozin and 50 mg ipragliflozin in T2DM patients treated with 300 U/mL insulin glargine. They found that the control of mean blood glucose level, MAGE, and SD was better with tofogliflozin compared with ipragliflozin. Furthermore, they reported that tofogliflozin was associated with significantly fewer hypoglycemic episodes, particularly nocturnal episodes, and ascribed this to its shorter half-life relative ipragliflozin. 14 In the present study, we analyzed the percent time at blood glucose level <70 mg/dL during the night (0:00–6:00 a.m.) and tofogliflozin tended to reduce it between the two SGLT2 inhibitors (P = 0.1080, baseline 1.86%, ipragliflozin 8.02%, tofogliflozin 0.01%).
Overall, our results showed no significant difference between the two SGLT2 inhibitors. SGLT2 inhibitors are considered to pose relatively low risk of hypoglycemia. Evidence from experimental and clinical studies on T2DM suggests that while SGLT1 located downstream of renal tubules enhances glucose reabsorption, SGLT2 inhibitors enhance gluconeogenesis in the liver through increased serum levels of glucagon. 14 –16
In a recent clinical study, Okajima et al. 17 used CGM to dissect nocturnal hypoglycemia in patients with T2DM who were on basal–bolus insulin (BBI) therapy, and treated additionally with 50 mg ipragliflozin (an SGLT2 inhibitor) and/or 20 mg teneligliptin (a DPP4 inhibitor), alone or in combination. Their study showed that the percent time at blood glucose level <70 mg/dL during the night (0:00–8:00 a.m.) was significantly lower in the BBI+IPR group than in the BBI+teneligliptin group. Their results suggest that SGLT2 inhibitors may increase the risk of hypoglycemia when used in combination with DPP4 inhibitors and metformin, known to inhibit gluconeogenesis in the liver.
To examine this issue in our patients, we conducted a subanalysis of hypoglycemia in 16 patients who received DPP4 inhibitors. The results showed that the percent time at glucose level <70 mg/dL (between SGLT2 inhibitors: P = 0.1118, baseline 0%, ipragliflozin 4.99%, tofogliflozin 0.07%) and the area over the curve <70 (between SGLT2 inhibitors: P = 0.0631, baseline 0 mg/dL*day, ipragliflozin 0.56 mg/dL*day, tofogliflozin 0.01 mg/dL*day) tended to be lower in patients treated with tofogliflozin. We also analyzed the low blood glucose index (between SGLT2 inhibitors: P = 0.1040, baseline 0.49, ipragliflozin 1.87, tofogliflozin 0.89) and percent time with blood glucose <54 mg/dL (between SGLT2 inhibitors: P = 0.1910, baseline 0%, ipragliflozin 0.41%, tofogliflozin 0.01%) using the data of all patients. While the analysis showed comparable effects for tofogliflozin and ipragliflozin on the above parameters, the time at severe hypoglycemia tended to be lower in patients treated with tofogliflozin.
The most important limitation of the present study is the small sample size (30 patients), although we used a crossover study design. Furthermore, the lack of significant differences in hypoglycemia could be explained by the following methodological aspects of the study: (1) sulfonylureas were used in our subjects at low doses, which are recommended to prevent hypoglycemia; (2) many patients used gliclazide, which has a short half-life; and (3) the incidence of hypoglycemia was very low in our patients, even before the addition of SGLT2 inhibitors. This study needs to be repeated in the future in patients with T2DM treated with long half-life sulfonylureas.
In conclusion, based on the data collected through CGM, the present study demonstrated that the addition of tofogliflozin to sulfonylureas for treatment of T2DM tended to reduce the time spent in hypoglycemia. On the contrary, the addition of SGLT2 inhibitors to sulfonylureas in the same patients improved the average glucose level and reduced glucose fluctuations without increasing the time in hypoglycemia.
Footnotes
Acknowledgments
This study was supported by a grant from Kowa Company, Ltd., and a representative from the firm participated in reviewing the final article. However, the authors declare full responsibility for the study design, conduct, data collection, statistical analysis, and drafting of the article.
Author Disclosure Statement
Y.O. has received lecture fees from AstraZeneca, MSD, Ono, Mitsubishi Tanabe, Bayer, Novo Nordisk, Eli Lilly, Boehringer Ingelheim, and Takeda. Y.T. has received consulting fees, lecture fees, and/or honoraria from Daiichi-Sankyo, Astellas, Pfizer, Mitsubishi Tanabe, Bristol-Myers, Chugai, YL Biologics, Eli Lilly, Sanofi, Janssen, and UCB, and has received research grants from Mitsubishi-Tanabe, Takeda, Bristol-Myers, Chugai, Astellas, AbbVie, MSD, Daiichi-Sankyo, Pfizer, Kyowa-Kirin, Eisai, and Ono. A.K., M.S., Y.G., T.O., M.N., and K.T. declare no conflict of interest.
Supplementary Material
Supplementary Fig. S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.