
Abstract
Background:
Along with increased usage of continuous glucose monitors, flash glucose monitors, and patch pumps by patients with diabetes, the frequency of skin reactions has also increased. Skin irritation and itching can be annoying to users. However, more serious contact allergies to one or more components of the adhesives or plastic material of the housing of the devices can become lifelong. Redness and itchiness are so strong that patients can no longer use a particular system. In August 2017, a major culprit allergen, isobornyl acrylate (IBOA), was identified for these more serious reactions.
Objectives:
Our objective was to evaluate IBOA content in different medical products.
Methods:
The plastic material used for the housing of the Freestyle Libre (n = 3), Dexcom G6 (n = 3), and Enlite (n = 4) was analyzed for IBOA content by gas chromatography–mass spectrometry. Adhesives of the different systems were also analyzed.
Results:
IBOA was found in the housings of Freestyle Libre and Enlite sensor, but not in the Dexcom G6.
Conclusions:
Patients with an IBOA allergy should consider switching to a medical product without IBOA. Furthermore, removal of IBOA from devices that contact the skin is encouraged.
Introduction
Skin reactions to externally applied diabetes products have become more common with the increased usage of these systems for treatment of patients with diabetes. Some months after market launch of the Freestyle Libre glucose monitoring system (Abbott, Chicago, IL), skin reactions with this system were described. 1 Several subsequent reports described skin reactions with this system 2 –5 ; however, in most of these studies, it was not differentiated between irritative and contact allergic skin lesions. 4,5 In adults, such device-related skin reactions are even associated with an increased patient scoring on the generic questionnaire Problem Areas in Diabetes on having problem areas in diabetes. 6 Although more common, skin irritations do not occur with every wear or with the same intensity. Patients notice redness and sometimes itching. Irritation is usually due to individual and physical factors. 7 Individual factors may be the age or a predisposition to dry skin. Physical factors are due to the long skin occlusion under a sensor, sweating, or damaging the epidermis by rapidly tearing off the adhesive.
Allergic contact dermatitis (ACD) is less common, but of a greater clinical significance. ACD may be due to substances contained in the adhesives of the medical products or the plastic materials that are used for housing of the technical components themselves. This means that one or more allergens that are in the given medical product itself and/or the adhesive leads to an allergic type 4 contact allergy reaction. 8 It can take several weeks or even months until such a contact allergy develops; however, once the patient is sensitized to an allergen, this reaction remains likely lifelong and appears with every contact within a short period of time after another exposure. 9 Allergic skin reactions are mostly of stronger intensity than skin irritations. In case of Freestyle Libre, it occurs under the system and is so pronounced, that the system has to be removed after only a few hours or days. Redness and blistering appear, often with yellowish exudate (Fig. 1). In addition to the long exposure time and skin barrier disorders, predisposition factors for the development of this contact allergy relate to the amount and allergenic potency of one or more allergens. The patch test is according to the American Academy of Allergy, Asthma, and Immunology, “the gold standard for contact allergen identification.” 9
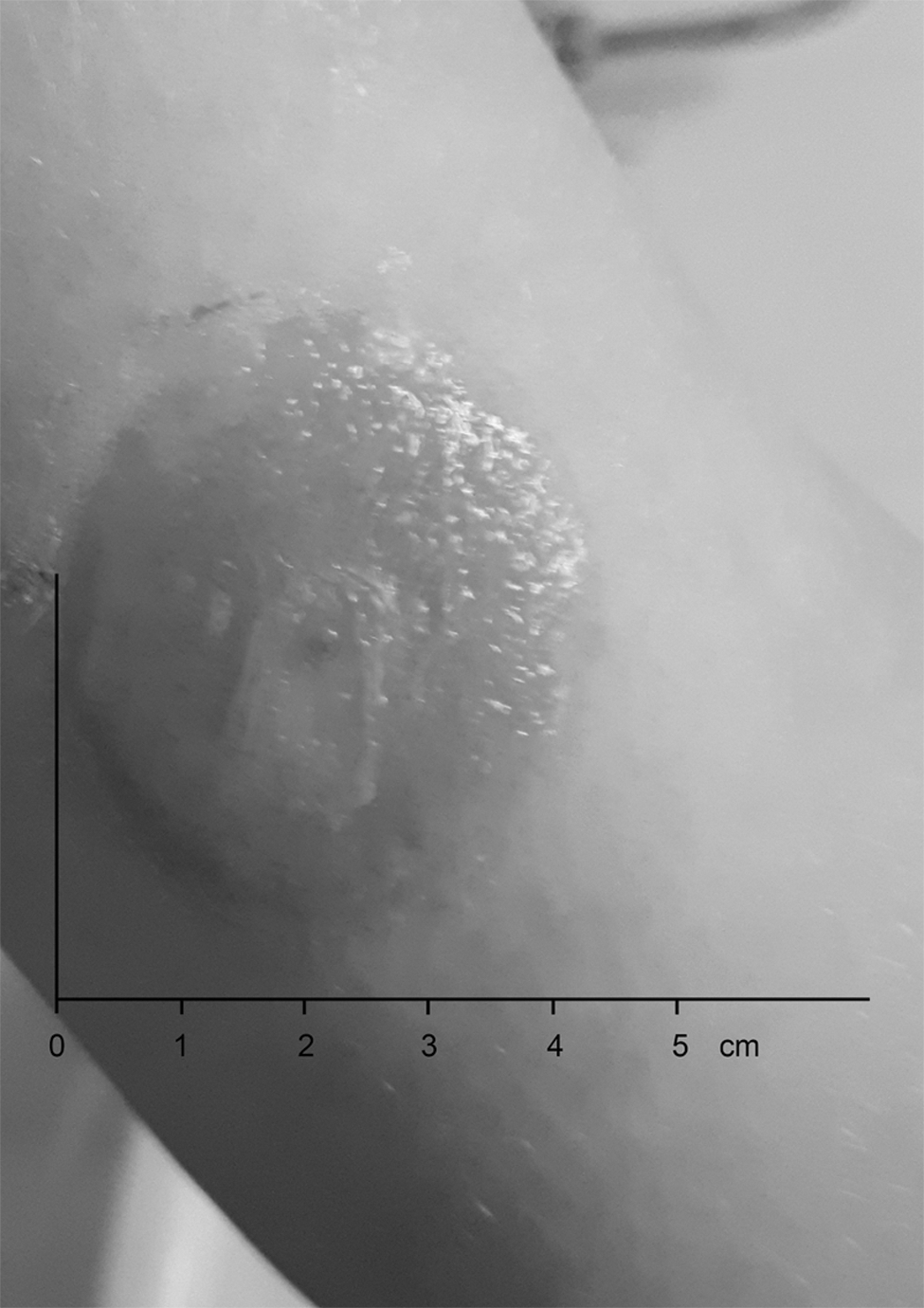
Allergic skin reaction of a boy after usage of Freestyle first generation.
Reports of allergic skin reactions to medical devices for the treatment of diabetes were unusual before 2017. In 1995, two patients with diabetes were described that showed allergic reactions to the adhesives of the infusion set of their insulin pump. 10 Isobornyl acrylate (IBOA) was identified to be one of the components contained in the UV-cured glue used to fix the infusion set needle to its plastic stand. In 2016, the case of a child was published developing ACD toward a Dexcom G4 CGM. 11 A skin sensitivity patch test revealed a positive reaction to hydroxycyanoacrylate, which was present in the intermediate layer of the kit. Two other adults in whom the ACD was caused by 2-ethyl cyanoacrylate contained in their Dexcom G4 were also described. 12 The manufacturer eliminated exposure that might trigger a skin reaction from the intermediate adhesive layer by attaching the CGM system to the adhesive using a thermic ultrasound technique. 13
The major allergen generating reactions to the Freestyle Libre system was unknown until the summer of 2017 when a group of Belgian and Swedish dermatologists showed that in 12 of 13 of their affected patients with ACD, this was induced by IBOA. 3 In a subsequent study, we tested IBOA 0.1% with a boy with a known ACD induced by wearing the Freestyle Libre. There was a positive skin reaction after 48 and 72 h in the patch test. 4 However, the two original adhesives ([1] skin adhesive and [2] thin layer glue that sticks the sensor to the skin adhesive) that were provided by the manufacturer of these (Adhesive Research, Glen Rock, PA) did not show a positive skin reaction. Thus, our assumption was that IBOA may originate from the plastic material of the Freestyle Libre itself and subsequently diffuse through the plaster to the skin; at least in some patients the outline of the skin reactions is that of the housing of the Freestyle Libre and not that of the adhesive. IBOA could also be detected by gas chromatography (GC) in the housing of the patch pump Omnipod, but—like the Freestyle Libre—not in the adhesive that sticks the pump to the skin. 14,15 In contrast, it was reported that the housing of the Dexcom G5 and its adhesive are free from IBOA and are well tolerated by patients who are allergic to Freestyle Libre and IBOA. 16
At present, no good estimations are available about how many patients suffer from ACD after IBOA sensibilization. This is, in part, due to the fact that ACD occurs typically after months of usage of the Freestyle Libre, even years later. In most clinical studies - which have a too short study duration - it was not differentiated between skin reactions that were simple irritations and real ACD. 5,6 A systematic evaluation of skin reactions, especially ACD, is missing.
The aim of our study was to estimate the IBOA content of a number of medical products that are applied to the skin for diabetes therapy.
Material and Methods
The IBOA content of different CGM systems (Freestyle Libre [Abbott]; G6 [LOT 5249363; Dexcom, Inc., San Diego, CA]; Enlite [sensor LOT D138P, transmitter LOT GT6066295M; Medtronic, Dublin, Ireland]) was measured.
Sample preparation
The adhesives of the CGM systems were manually removed from the housings. The CGM systems (Freestyle Libre (n = 3), Dexcom G6 (n = 3), and Enlite sensor (n = 4) were transferred into weighing bottles (45 mL, 60 × 30 mm; neoLab, Heidelberg, Germany). Six milliliter of methanol (GC Ultra Grade, RATISOLV® ≥99.9%, Roth, Karlsruhe, Germany) was added to immerse the bottom side (dermal contact side) of the systems in a solvent level of ∼2 mm. This corresponds to immersed areas of ∼9.0 cm2 (Freestyle Libre), 7.0 cm2 (Dexcom G6), and 2.8 cm2 (Enlite). As internal standard caffeine (CF) solution (0.01 mg/mL) (HPLC ≥99.0%, Sigma-Aldrich, St. Louis, United States) was added. After 3 days incubation of the systems in the dark at room temperature, the IBOA content in the methanol (eluates) were analyzed (see Analytic procedure) by GC–mass spectrometry (GC/MS).
Water (LC-MS-Grade, ROTISOLV®; Roth) elutions were carried out as described previously. For GC/MS analysis, water samples previously were extracted one time with ethyl acetate (LC-MS-Grade, ROTISOLV ≥99.9%) (1:1 v/v). To optimize layer separation, the samples were centrifuged at 2800 rpm for 10 min. 17
The same technical procedure was conducted on pieces of the adhesives of the CGM systems (the adhesive of the Freestyle Libre was supplied by Adhesive Research; skin plaster n = 3 and transparent glue layer that fixes the sensor to the skin adhesive n = 3; Dexcom G6 (n = 3) and Enlite (n = 1).
Analytic procedure
The analysis of the eluates was performed on a Finnigan Trace GC ultra gas chromatograph connected to a DSQ mass spectrometer (Thermo Electron, Dreieich, Germany). A J&W VF-5ms capillary column (length 30 m, inner diameter 0.25 mm; coating 0.25 μm; Agilent, Böblingen, Germany) was used as the capillary column for gas chromatographic separation. Helium 5.0 was used as carrier gas at a constant flow rate of 1 mL/min. The temperature of the transfer line was 250°C. For sample analysis, 1 μL each was injected in splitless mode (splitless time 1 min, split flow 50 mL/min). For capillary transfer, the programmable temperature vaporizing inlet was heated from 30°C to 320°C (14.5°C/s) and finally held for 5 min at this temperature. The GC oven was initially heated isothermally at 50°C for 2 min, then increased to 280°C (25°C/min), and finally remained for 5 min at this temperature. The MS was operated in the electron impact mode at 70 eV (ion source temperature: 240°C). Samples were recorded in full scan mode (m/z 50–600).
Identification of IBOA was achieved by comparing the mass spectra and retention time with those of the reference standard IBOA (Merck, Darmstadt, Germany). For the reference standard IBOA, a calibration was performed. Resulting limit of quantification (LOQ) for IBOA in water (ethyl acetate extract) was 0.20 μg/mL and LOQ for IBOA in methanol was 0.10 μg/mL. The quantity of identified IBOA was calculated by correlating its characteristic mass peak (m/z 55) area to the corresponding predetermined calibration curve (internal standard CF). An example chromatogram of Freestyle Libre is shown in Figure 2.
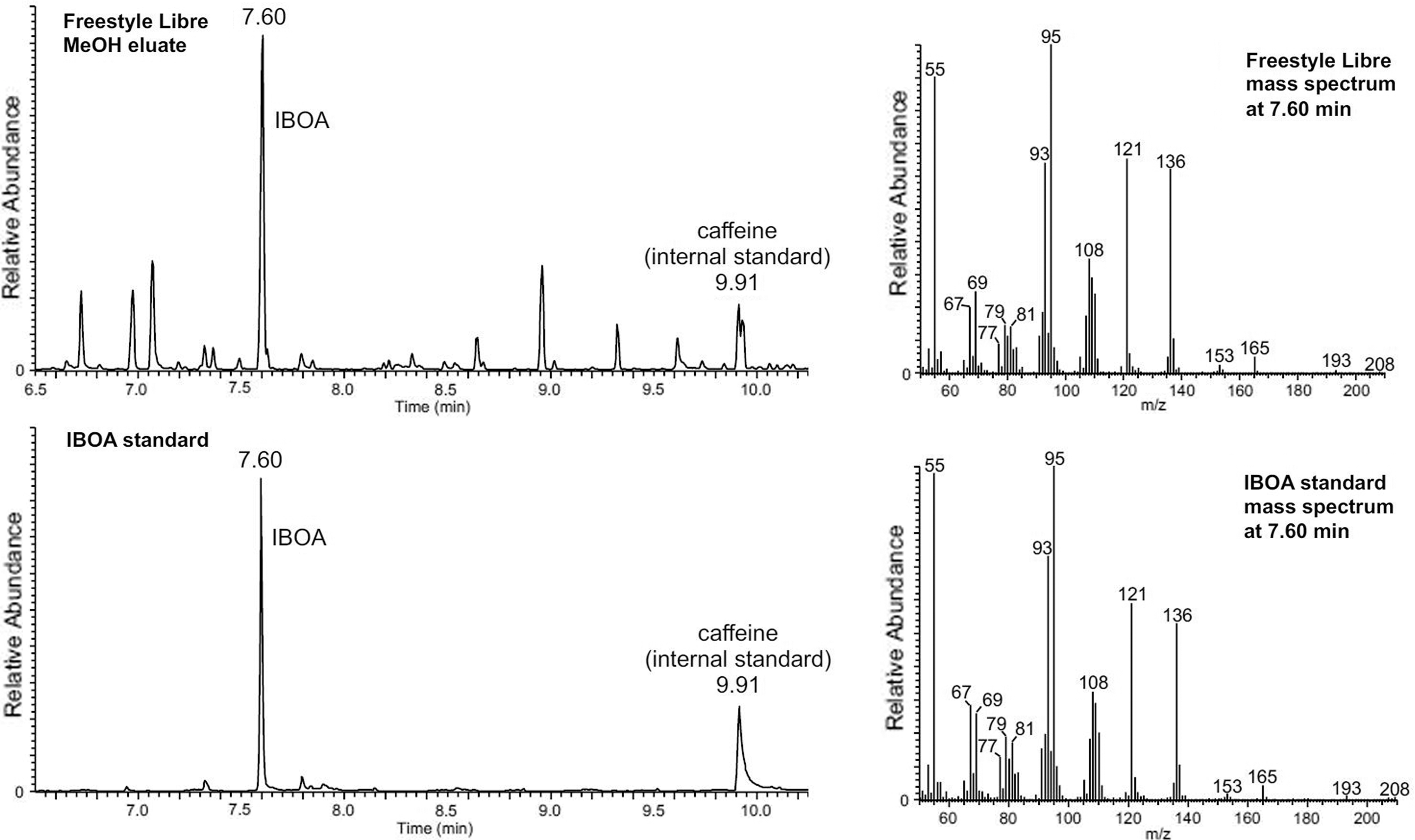
Example chromatograms of Freestyle Libre methanol eluate (above) in compression with IBOA reference standard (below). Retention time of IBOA in standard (below) and sample (above) was 7.60 min. Corresponding mass spectra of sample and standard yielded identical patterns.
Results
In the water eluates of all CGM systems—including the adhesives—no IBOA (<LOQ) could be detected; however, at least in some of the methanol eluates of the CGM systems, it could be detected (Table 1). In case of the Freestyle Libre, 2.64 μg/mL with a standard deviation (SD) of 0.36 μg/mL of IBOA (3 days, methanol) corresponds to a dose/area of ∼0.29 μg/cm2 per mL (immersed surface area). In both types of adhesives of the Freestyle Libre, no IBOA (<LOQ) was found. In the methanol eluates of Dexcom G6 sensors and its adhesives, no IBOA was detected. With the Enlite CGM system, IBOA was found both in the methanol eluates of the sensor (1.11 μg/mL with a SD of 0.12 μg/mL corresponds to a dose/area of ∼0.40 μg/cm2 per mL [immersed surface area]) and the adhesive (0.26 μg/mL), but not in the eluates of the transmitter.
The Isobornyl Acrylate Content in the Housing and Adhesives of Different Medical Devices Used for Continuous Glucose Monitoring in Patients with Diabetes Was Analyzed by GC/Mass Spectrometer After 3 Days Elution in Methanol and Water (Control)
CGM, continuous glucose monitoring; FL, Freestyle Libre; LOQ, limit of quantification.
Discussion
IBOA is an acrylate used widely in the automobile industry for UV and weather protection. 18 In safety data sheets, it is classified as an irritant for skin and eyes. In August 2013, Christoffers et al. carried out a study with various acrylates and concluded that IBOA does not have to be included in the skin patch test. 19 However, data obtained in this study revealed that IBOA is detectable in the housing of the Freestyle Libre and the Enlite sensor and the adhesive of Enlite. This suggests that an ever increasing number of patients with diabetes are being exposed to IBOA for longer periods of time. We recommend that IBOA be included in skin patch tests for evaluating the sensitivity of a given patient to this substance. In this context, it is of interest to know that IBOA 0.1% will become available as a commercial test substance sometime in the middle of 2019.
This study confirms the finding of IBOA in the housing of the Freestyle Libre, and also finds that smaller amounts of IBOA can be detected in the Enlite CGM system and in its corresponding adhesive. In the Dexcom G6 and its plaster, no IBOA could be measured; a finding that confirms former measurements of the G5. 16 A limitation of our study is that the measurements were not performed in a “blinded manner.” Our measurement results should be confirmed by measurements of samples from a larger number of devices.
Once a patient is sensitized to an allergen, future contacts with this substance triggers a reaction again, commonly known as a memory response. So it is most likely that patients will have it for the rest of their life. 9
So, once a patient is allergic to IBOA, this contact allergy lasts surely for the rest of his or her life and he or she also may be at risk to develop cross-allergic reactions to other acrylates. This should be avoided at all costs. Cross-reactions mean that patients can also react toward other materials and adhesives that contain structures that are chemically similar, which might be used for other medical reasons to such patients. IBOA has a very special branched structure and fortunately may be not so much at risk to develop cross allergies; however, it has a high allergenic potency itself.
In case of the Freestyle Libre, a relevant amount of IBOA seems to be present. In view of the large number of users of this CGM system (>1.5 million on a worldwide basis), it is hoped that the manufacturer comes along with an IBOA-free version soon. IBOA appears to be the major allergen with this CGM system. Recently, another relevant allergen was identified in the housing of the Freestyle Libre, called N,N-dimethylacrylamide. 20 It is worth considering as well the acrylates of the adhesive or other acrylates contained in the housing. Some patients appear to develop ACD toward these substances.
Patients with an IBOA allergy should avoid contact to this allergen; however, most patients do not want to give up their CGM system due to the benefits they have by using it; therefore, they do everything to be able to continue using, for example, the Freestyle Libre. Patients first tried to fix special skin plates under their sensors, yet most constructions did not appear to work over a longer period, or glucose concentrations were not accurately being measured in the same skin compartment due to a change in the depth of the needle tip of the sensor. Good experience was reported with some hydrocolloid-based thicker adhesives/plates, for example, blister plasters. 21 Such constructions do work not only in patients with an IBOA allergy but also in patients who have other severe skin reactions (Fig. 3).

Addition of hydrocolloid-based adhesives/plates in a patient with an IBOA allergy, preventing allergens from migrating into the skin from the sensor set and thus decreasing allergic contact dermatitis symptoms. IBOA, isobornyl acrylate.
In conclusion, the acrylate IBOA was detectable in the housings/adhesives of some CGM systems and a patch pump (X), but not in all. In view of the severity of allergic skin reactions and the potential clinical consequences, the manufacturer should develop IBOA-free housings and adhesives.
Footnotes
Author Disclosure Statement
No competing financial interests exist.