
Abstract
Background:
Timing of insulin administration in persons using multiple daily injections (MDI) is self-reported. New technology enabling tracking and logging of insulin doses, combined with continuous glucose monitoring (CGM), may provide insight into the relationship between insulin administration and glucose levels.
Methods:
We performed a prospective observational study using Bluetooth-enabled pen caps, along with CGM, in participants with type 1 diabetes (T1D) on MDI to objectively assess the relationship between the timing of insulin administration and its impact on pre- and postprandial glucose levels for a 2-week period.
Results:
We evaluated 50 participants (age 40.3 ± 19 years; A1c 8.2% ± 1.5%, duration of T1D 20 ± 15 years). Thirty-seven percent of total boluses resulted in persistent hyperglycemia (glucose >180 mg/dL 3 h postprandially), while 10% resulted in clinically significant hypoglycemia (glucose <55 mg/dL 3 h postprandially) on CGM. Preprandial glucose levels at the time of the bolus did not correlate with postprandial glucose levels. Late boluses, defined as a rise in glucose of ≥50 mg/dL before a bolus, were seen two times/patient/week. Missed boluses, defined as a rise in glucose of ≥50 mg/dL without a bolus within 2 h, occurred 17 times/patient/week. Late and missed boluses were associated with worse glycemic control (A1c; R 2 = 0.1, P = 0.02; R 2 = 0.1, P = 0.02).
Conclusions:
The use of Bluetooth-enabled pen caps, with CGM, in persons with T1D on MDI can illustrate the relationship between insulin bolus timing and postprandial glucose. These data may help clinicians and patients understand the impact of timing of insulin doses on glucose levels and glycemic control.
Introduction
Postprandial glucose excursions, in addition to fasting glucose levels, represent one of the two major determinants of achieving good glucose control. Limiting meal-related hyperglycemia, without inducing late postprandial hypoglycemia, is one of the primary objectives of insulin therapy in people with type 1 diabetes (T1D). 1 Continuous glucose monitoring (CGM) has been efficacious in improving glycemic control in people with T1D using multiple daily injections (MDI) in randomized controlled studies. 2,3 However, recent data also show that this success may not translate to real-world clinical settings. 4 Thus, more information on insulin administration and associated glucose patterns is needed to improve diabetes self-management in people with T1D on MDI.
Optimal coverage of postprandial glucose usually requires an injection of bolus insulin before eating a meal. 5 However, thus far, timing of insulin injection is self-reported by patients on MDI and the information on missed or delayed boluses, is not known.
The aim of this study is to use Bluetooth pen caps (Gocap®) and CGM to objectively assess the relationship between the timing of insulin administration and preprandial and postprandial glucose levels in adults with T1D on MDI. We also assessed the impact of late and missed meal-time boluses on glycemic control.
Methods
This prospective, observational study was conducted at the Joslin Diabetes Center in Boston, MA, after receiving approval from the Institutional Review Board. Two populations, young adults (ages 18–35 years) and older adults (ages ≥65 years), with T1D on MDI were recruited for this study. We chose two age groups, one younger and one older, to identify different age-related challenges to glucose control and insulin administration. All participants enrolled in the study were established patients at the Joslin Diabetes Center with ample previous education regarding insulin administration, dose adjustments, and carbohydrate counting, per Joslin standards of care. 6 Exclusion criteria included allergies to tape/adhesive used for CGM sensors, acetaminophen use, gastroparesis, and visual or cognitive impairment that interferes with self-administration of insulin. After providing written informed consent, demographic and medical information was collected using a questionnaire. All participants completed the Hypoglycemia Fear Survey-II (HFS-II) to assess behaviors and worries regarding hypoglycemia. 7 A1c was measured by venous blood test. The study participants were provided with Lantus® and Apidra®-SoloSTAR insulin pens, and Common Sensing, Inc. Gocap Bluetooth-enabled pen caps that fit on the end of the insulin pens. They also received a smartphone, with the Gocap application, for the duration of the study. The insulin pen cap works in conjunction with a smartphone application. The cap registers the position of the insulin pen plunger and automatically sends confirmation of dose and time of delivery to a smartphone app that sends data to a study web portal through a study-provided account. Study participants were blinded to the data on the app. The study staff monitored the web portal on a weekly basis to ensure that participants were utilizing the device appropriately. The data collected from the Bluetooth-enabled pen cap were sent to a web portal through a study-provided account.
The participants continued on their usual insulin regimen during the study. If participants used basal insulin other than Lantus, they were switched to Lantus for the duration of the study, after receiving permission from their diabetes specialists. Similarly, if they used meal-time insulin other than Apidra, they were switched to Apidra for the duration of the study. Participants who used syringes for insulin self-administration were trained in the use of insulin pens.
A masked CGM (Dexcom® G4) was worn for the 14 days (two 7-day sensors) of the study with twice-daily calibrations according to the manufacturer labels. CGM sensors were inserted by the participant. The participant was educated on the proper calibrations and troubleshooting techniques while wearing the CGM. Education was also provided on how to change the CGM sensor after 7 days of wear. The CGM was mailed back to the Joslin Diabetes Center by the participant in a prepaid FedEx envelope after 2 weeks of wear. Participants who were already using their own Dexcom CGM continued using their device in real-time and were provided with sensors for the 14-day collection period, and CGM data were downloaded from their personal device. We also analyzed the data to assess the impact of real-time CGM use on primary outcomes.
The time recorded by the Bluetooth pen cap defined the time of the bolus, and thus, preprandial glucose, and the time 3 h after the recorded bolus defined postprandial glucose. Stable glucose was defined as continuous readings ≥95 mg/dL without an increase in glucose of ≥50 mg/dL for at least 30 min. We used this cutoff to avoid the erroneous labeling of rising glucose, which could be secondary to the treatment of a hypoglycemic episode. A bolus was considered an on-time preprandial bolus when it was administered while the CGM reading was stable. A bolus was deemed a late preprandial bolus when it was administered after a rise in glucose of ≥50 mg/dL, following stable glucose. A bolus was deemed a missed preprandial bolus when a rise in glucose of ≥50 mg/dL was noted, without a bolus within 2 h from start of the rise. We considered all boluses given on time or late as totaling 100%, while missed boluses were not counted in the “total boluses,” as they were not given. Thus, the number of missed bolus is reported as an absolute number, rather than a percentage.
Time windows for bolus insulin were created as breakfast (6 am–11 am), lunch (11 am–4 pm), dinner (4 pm–10 pm), and overnight (10 pm–6 am). Participants were grouped based on the percentage of their boluses resulting in postprandial glucose levels >180 mg/dL: ≥30%, ≥50%, or ≥70%.
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range) while categorical variables are presented as n (%). Student's t-test was used to compare means of continuous variables between real-time CGM use (user vs. nonuser). Generalized linear models were used to estimate effect sizes (β-coefficients, P-values, and R 2) for the associations between continuous variables. The effect size (β-coefficient) indicates the magnitude of change in the outcome that corresponds to a 1 unit increase in the independent variable. Statistical significance level was set at P < 0.05. All analyses were done using the SAS statistical analysis package (version 9.4; SAS Institute, Inc., Cary, NC).
Results
We recruited 50 participants for this study (36 younger and 14 older). The average age was 40 ± 19 years and 45% were female. Average A1c was 8.2% ± 1.5% and 36% were real-time CGM users. On average, 20 meal-time boluses per participant were reported/week, with 19 categorized as on time and 1 as late. Participants missed an average of 17 boluses per week. On average, the total number of bolus events per week per participant was 37, combining on-time, late, and missed boluses. Characteristics of the participants as a whole group, as well as by age, are shown in Table 1. The two age groups did not differ in the number of missed or delayed boluses.
Characteristics for All Participants
CGM, continuous glucose monitoring; DM, diabetes.
Table 2 shows the mean (%) and SD of preprandial and 3-h postprandial glucose levels using CGM data reported in four categories: <55, 55–70, 70–180, and >180 mg/dL. 8 Regardless of postprandial glucose levels, the glucose values preprandially were <70 mg/dL 6.8% of the time, between 70 and 180 mg/dL 37.8% of the time, and >180 mg/dL 55.4% of the time. At 3 h postprandial, regardless of preprandial glucose levels, the values were <55 mg/dL 10.6% of the time, 55–70 mg/dL 3.6% of the time, 70–180 mg/dL 49.2% of the time, and >180 mg/dL 36.6% of the time (Table 2).
Percentage of Boluses Classified by Preprandial and Postprandial Glucose Levels
The proportion of all boluses (% mean ± SD) are categorized based on preprandial glucose levels (row) as well as their postprandial result (column).
SD, standard deviation.
Table 3 shows the details of late and missed boluses. Late boluses represented 8% of total boluses and were observed at many different time points throughout the day (Table 3). The percent of late boluses was inversely correlated with total time in range (β = −0.82, P = 0.02, R 2 = 0.11), but did not correlate with total time <70 mg/dL (P = 0.34). The percentage of late boluses was positively correlated with the percentage of postprandial glucose levels >180 mg/dL (β = 0.75, P = 0.04, R 2 = 0.08), which was more pronounced in the younger cohort than the older cohort (β = 1.22, P = 0.01, R 2 = 0.18; β = 0.06, P = 0.91, R 2 = 0.001, respectively). The percentage of late boluses did not correlate with HFS-II score. (P = 0.4) The average percent of late boluses did not differ by real-time CGM use (P = 0.44).
Late and Missed Boluses by Time of Day
IQR, interquartile range.
Missed boluses also occurred throughout the day. Four missed boluses per week per participant occurred between the hours of 6–11 am (breakfast), 11 am to 4 pm (lunch), and 10 pm to 6 am (overnight), while an average of six missed boluses per week per participant occurred between 4 pm and 10 pm (dinner) (Table 3). The average number of total missed boluses per week did not differ by real-time CGM use (16.6/week in CGM users vs. 17/week in non-users, P = 0.79) and was not associated with HFS-II score (P = 0.22) in this cohort. The total number of missed boluses per week was negatively correlated with time in range (70–180 mg/dL; β = −2.03, P < 0.0001, R 2 = 0.34) and was positively correlated with A1c (β = 0.10, P = 0.01, R 2 = 0.13).
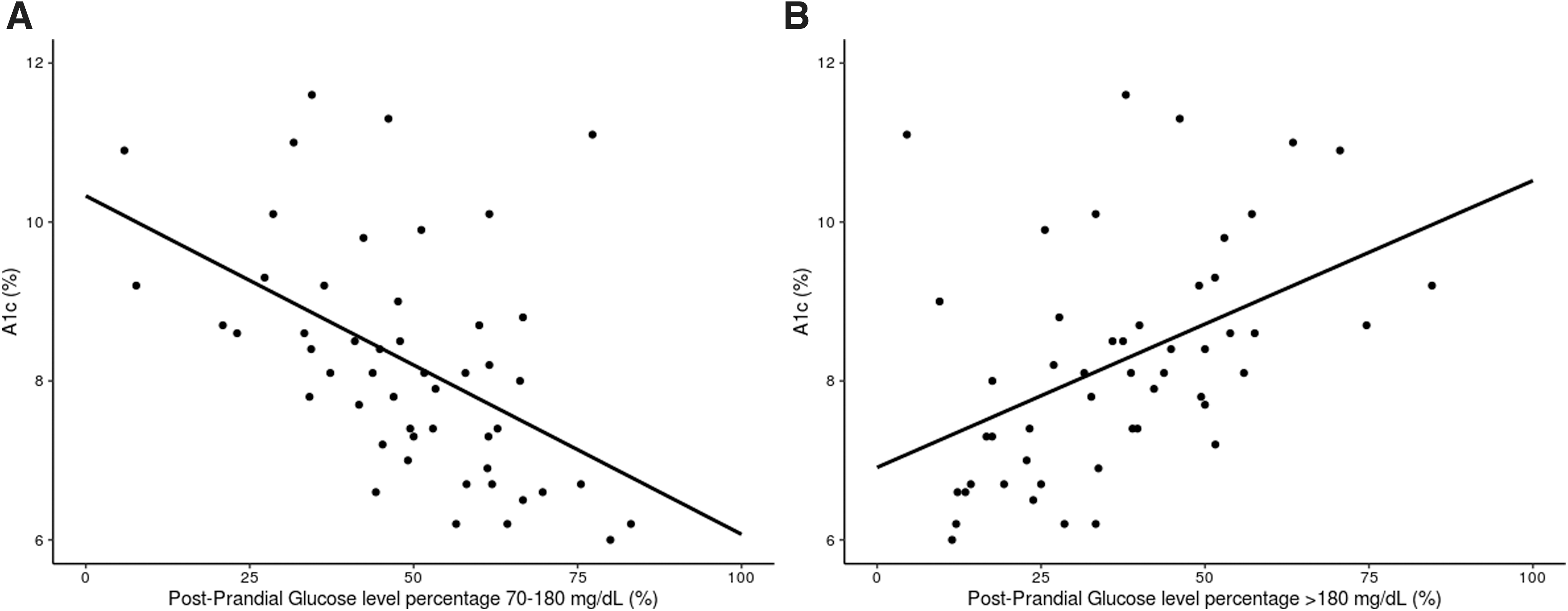
Next, we analyzed the frequency of 3-h postprandial CGM values >180 mg/dL at different levels of glycemic control (A1c). The results are shown in Table 4. We found that ≥30% of boluses resulted in postprandial glucose >180 mg/dL in 31 participants, ≥50% of the boluses resulted in postprandial glucose >180 mg/dL in 13 participants, and ≥70% of boluses resulted in postprandial glucose >180 mg/dL in 3 participants. Glucose control measured by A1c was negatively correlated with the percent of boluses resulting in postprandial glucose levels between 70 and 180 mg/dL (β = −0.04, P = 0.002, R 2 = 0.25) and positively correlated with the percent of boluses resulting in postprandial glucose >180 mg/dL (β = 0.04, P = 0.001, R 2 = 0.20) (Fig. 1). However, in participants who had ≥30% of their boluses resulting in postprandial glucose >180 mg/dL, A1c levels varied from <7.5% to >9% (Table 4). Out of 31 participants who had ≥30% of boluses resulting in postprandial glucose >180 mg/dL, 5 subjects or 16% had A1c <7.5%; 16 subjects or 52% had A1c 7.6%–8.9%, and 10 subjects or 32% had A1c ≥9% (Table 4).
Number of Participants with Boluses Resulting in 3-H Postprandial Continuous Glucose Monitoring Glucose Values >180 mg/dL at Least 30%, 50%, or 70% of the Time at Different Levels of Glycemic Control (A1c %)
The distribution of postprandial glucose levels differed with the use of real-time CGM. Compared to non-CGM users, real-time CGM users had a significantly lower percentage of postprandial clinically significant hypoglycemia (glucose <55 mg/dL), whether preprandial glucose was <70 mg/dL (real-time CGM = 2.1% vs. non-CGM = 5.5%, P = 0.01) or >180 mg/dL (real-time CGM = 2.2% vs. non-CGM = 5.1%, P = 0.002).
Next, we assessed the relationship between HFS-II score and pre- and postprandial glucose levels. The participants with a higher number of boluses with preprandial glucose levels >180 mg/dL had a higher score on the HFS-II, especially the subscore scale for behavior (β = 0.11, P = 0.09, R 2 = 0.07). The participants with a higher frequency of both preprandial and postprandial glucose levels >180 mg/dL, showed a trend for higher total scores on the HFS-II (β = 0.12, P = 0.11, R 2 = 0.06).
Discussion
We used a novel technology, Bluetooth-enabled insulin pen cap in combination with CGM, to illustrate the relationship between meal-time insulin boluses and preprandial and postprandial glucose levels in people with T1D on MDI. Although this method of analysis is common in individuals using insulin pumps, our study is the first to report these data in participants with T1D using MDI.
We recently showed that the use of Bluetooth-enabled pen cap technology can objectively assess adherence to insulin dosing and timing. 9 In the current study, we analyzed the timing of insulin administration and its relationship with glycemic excursions related to meals. Overall, this cohort of patients on MDI with T1D showed a high percentage of preprandial and postprandial glucose levels that were outside of the recommended goal of 70–180 mg/dL.
Interestingly, although a high percentage of elevated postprandial glucose levels (>180 mg/dL) was seen among all participants (37% of boluses), only a subgroup of 10% of participants consistently (>50% of the time) had preprandial and postprandial glucose levels >180 mg/dL. In the latter subgroup, insulin to carbohydrate ratios or sliding scale doses may have been inadequate. However, the high frequency of elevated postprandial glucose levels in the overall cohort suggests a multitude of contributing factors playing a role in meal dose and insulin response. For example, in recent years, we have learned that high-fat meals can result in a delayed blood glucose rise that can occur as late as 4 to 5 h after the meal, and high protein intake can also increase the incidence of delayed postprandial glucose rise. 10,11 The strong correlation observed in our data between late boluses and postprandial glucose levels >180 mg/dL, especially in the younger cohort, may be due to a greater consumption of high fat meals in this age group. Further studies are needed to determine this relationship in these populations.
In addition, we found that people with a higher HFS-II subscore tended to have higher percentage of boluses leading to high postprandial glucose levels >180 mg/dL, suggesting that fear of hypoglycemia, and the resulting behavior to mitigate hypoglycemia, may also interfere with glucose control. 12
Late and missed boluses were captured throughout the 24 h. Timing of insulin administration is important, as previous studies have shown that administration of rapid-acting insulin 15–20 min before meals results in a 30% lower postprandial glucose level and lower rate of hypoglycemia. 5 Several studies of people with T1D have also shown that a delay in bolus until after the meal may result in poorer glucose control, 13 –15 and diabetic ketoacidosis. 16 In our study, the percentage of late boluses was lower compared to other studies in the literature that used self-reported late boluses. This could be partly related to the definition we used to define late boluses in our study. The percentage of late boluses was not related to increased risk of hypoglycemia in our study, which is consistent with data in the literature. 17 However, in our study, both late and missed boluses were associated with poorer glycemic control.
The distribution of late and missed boluses over the 24 h was greater in the late afternoon and evening. This pattern could be attributed to a lack of focus and an increasing number of competing demands that may arise throughout the day. Thus far in the literature, distribution of late and missed boluses over the 24 h and potential causes have not been studied.
In our cohort, glucose levels pre- and postprandially were frequently out of range among all the participants, independent of A1c level. In addition, glucose levels postprandially were frequently out of range, independent of preprandial levels. However, as expected, participants with a higher percentage of boluses resulting in postprandial glucose levels >180 mg/dL had a higher A1c. When we evaluated preprandial and postprandial glucose levels by A1c category, we found that 16% of participants with good glycemic control (A1c <7.5%) had at least 30% of their boluses result in postprandial glucose levels >180 mg/dL, suggesting that other factors (i.e., composition of the meal, high and low glycemic index), rather than just the timing and amount of the insulin bolus, may need to be taken into consideration when educating patients. 1
This study has important limitations that should be acknowledged, including that it is a small, observational study, and we did not collect information on type of meal, exercise, or other factors that could have influenced postprandial glucose levels. We did not ask participants to provide this information to reduce the chance of biased adherence. In addition, we included participants who were naive to CGM, who subsequently wore a masked CGM, as well as those using real-time CGM. We showed that real-time CGM use did not impact postprandial hyperglycemia, as shown by a similar percentage of boluses resulting in postprandial glucose levels >180 mg/dL in both real-time CGM users and nonusers. The only significant difference between real-time CGM users and nonusers was seen as a significant reduction in boluses resulting in postprandial glucose levels <55 mg/dL in real-time CGM users. These data suggest the benefits of real-time CGM utilization to mitigate postprandial clinically significant hypoglycemia in people using MDI. However, further education around meal-time insulin doses and meal composition may be needed to improve glycemic outcomes in real-time CGM users.
In summary, the use of Bluetooth-enabled insulin pen caps along with CGM in persons with T1D on MDI can illustrate the relationship between timing of insulin boluses and postprandial glucose. These data may help clinicians and patients to understand the impact of timing of meal-time insulin on glucose levels, and lead to better strategies for improving glycemic control. Future larger intervention studies are needed to assess the cause of elevated postprandial glucose levels and to confirm whether the use of Bluetooth insulin pen technology can help improve preprandial and postprandial glucose levels with the development of educational tools.
Footnotes
Acknowledgments
We acknowledge support by the Joslin Clinical Research Center and thank its philanthropic donors. The funding source had no role in design or conduct of the study; collection, management, analyses, and interpretation of the data; or preparation and decision to submit article for publication.
Authors' Contributions
Dr. Toschi had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis. Study concept and design: M.M., C.S., and E.T. Data acquisition, analysis, and interpretation: E.T., C.S., J.M.G., T.G., A.A,-C., S.C., A.B.D., and M.M. Drafting of the article: E.T., C.S., J.M.G., A.A.-C., A.B.D., and M.M. Critical revision of the article of important intellectual content: M.M., C.S., and E.T.
Author Disclosure Statement
M.M. consultant for Sanofi and Lilly. All other authors have no conflicts of interest relevant to this article.
Funding Information
This study was supported by an investigator-initiated grant from Common Sensing, Inc., in collaboration with Sanofi and Dexcom.