
Abstract
We evaluated the efficacy of 670 G HCL on changes in HbA1c and continuous glucose monitor (CGM)-based glucose metrics at 3 and 6 months between five adults with T1D with gastroparesis and nine age-, sex-, and diabetes duration-matched T1D without gastroparesis. At baseline, there were no differences in age, gender, diabetes duration, and total daily insulin requirement between two groups. Median duration of gastroparesis diagnosis was 4.3 years (interquartile range [IQR]: 3.7, 5.9 years). Reduction in HbA1c [difference in HbA1c from baseline to 6 months, median (IQR): 0.3% (0.3%, 0.3%) vs. 0.5% (0.3%, 0.9%); P = 0.20] and CGM time spent in normoglycemia at 6 months [median (IQR): 73% (68%, 80%) vs. 67% (64%, 74%); P = 0.24] were not different between the groups. HCL has similar efficacy in glucose control in adults with T1D with gastroparesis and appears to be safe in this population.
Introduction
Diabetic gastroparesis is a syndrome characterized by delayed gastric emptying in the absence of a mechanical obstruction. 1 Patients with type 1 diabetes (T1D) are 30 times more likely to develop gastroparesis than the general population and estimated prevalence is about 5%. 2 –4 Gastroparesis is associated with higher risk of severe hypoglycemia and higher HbA1c levels than in patients with T1D without gastroparesis. 2–3 In addition to suboptimal glycemic control, it increases the risk of nutritional deficiencies, hospitalization, and depression, 2,3 and thus decreases the quality of life. 2,3
Insulin pump therapy with the use of longer active insulin time and smart bolus features such as extended/divided boluses has been suggested to improve glycemic control in T1D. 3 Current FDA-approved hybrid closed-loop system (HCL, Medtronic MiniMed® 670G) improves glucose control and reduces time spent in hypoglycemia in patients with T1D. 5 However, there are no clinical studies evaluating HCL systems in patients with gastroparesis. We conducted a study to evaluate the efficacy of HCL on glycemic control in adults with T1D and gastroparesis compared to adults with T1D without gastroparesis.
Methods
This retrospective study included adults (age >18 years) with T1D using insulin pump and continuous glucose monitoring (CGM) system for at least 3 months, which transitioned to Medtronic MiniMed 670G HCL system at the Barbara Davis Center for Diabetes. Pregnant patients with T1D were excluded. Adults with T1D and gastroparesis were identified from electronic medical records based on ICD-10 codes and then verified by reviewing medical chart notes and supporting laboratory evidences. Gastroparesis was verified further by a documentation of gastric emptying study. Identified adults with T1D and gastroparesis were asked questions to assess gastroparesis symptoms using validated Gastroparesis Cardinal Symptom Index (GCSI). 6 Patients were asked to rank each of nine symptoms (nausea, retching, vomiting, stomach fullness, inability to finish a normal-sized meal, feeling excessively full after meals, loss of appetite, bloating, and the abdomen appearing visibly larger) using a Likert scale of 0 (none) to 5 (very severe). Age-, sex-, and diabetes duration frequency-matched adults with T1D without a diagnosis of gastroparesis, who transitioned to HCL during the same time period, were used as controls. Patient characteristics and details of diabetes management were collected with chart review. Insulin pump and CGM data at baseline (3 months before start of HCL), and after 3- and 6-month use of HCL were retrieved from Carelink software and full CGM data set was used for analysis. CGM time spent in range (TIR), hypoglycemia, and hyperglycemia were defined as the percentage of time spent between 70 and 180 mg/dL, <70 mg/dL, and >180 mg/dL as recommended by the International Consensus. 7 We analyzed change in HbA1c and CGM metrics such as TIR and time below and above range at 3- and 6-month use of HCL in adults with T1D and gastroparesis compared to adults with T1D and no gastroparesis for efficacy and safety outcomes. Colorado Multiple Institutional Review Board approved this study.
Statistical methods
Summary statistics were presented as median and interquartile range (IQR) for continuous data and as count and proportion (%) for categorical data. The differences in HbA1c between baseline and 3 months and baseline and 6 months were tested with Wilcoxon signed rank tests, separately for the gastroparesis and control groups. Differences in HbA1c at each time point between gastroparesis and control groups were calculated using Wilcoxon rank sum tests. Wilcoxon signed rank and Wilcoxon rank sum tests were also used to test for differences in percent time in range between time points and between groups, respectively. Differences between baseline characteristics and changes in diabetic measurements were also compared between groups using Wilcoxon rank sum tests. R version 3.5.1 was used for all analysis. All statistical tests were two sided with P < 0.05 considered statistically significant.
Results
Five adults with T1D and gastroparesis and nine adults with T1D and no gastroparesis (control) were included in this study. There were no differences in age, gender, diabetes duration, HbA1c, average total daily basal and bolus insulin requirement, active insulin time, or carbohydrate ratio between two groups (Table 1). Median duration of gastroparesis diagnosis was 4.3 years (IQR: 3.7, 5.9) and median GCSI score at baseline was 23.5 (IQR: 17, 27.3). All, except one, T1D patients with gastroparesis were on motility agents. There was a nonsignificant reduction in HbA1c in the gastroparesis group and significant reduction in HbA1c in the control group at 3 months (P = 0.14 and P = 0.04, respectively) and 6 months of HCL use (P = 0.10 and P = 0.06, respectively) compared to baseline. However, the reduction in HbA1c between the groups was similar (Fig. 1). There was no difference in reduction in glycemic variability as measured by coefficient of variation in both groups at 6 months compared to baseline (data not shown). Overall, median CGM glucose at baseline in the gastroparesis and control group was 167.6 mg/dL (IQR: 157.8, 191.7) and 173.8 mg/dL (161.2, 188.7), which was reduced to 150 mg/dL (148.9, 156.2) and 159.1 (147.1, 168.0) after 6 months of HCL use, respectively. The differences in CGM-based TIR, hypoglycemia, and hyperglycemia between two groups are shown in Table 2. No severe hypoglycemia requiring hospitalization was reported in the gastroparesis patients. Despite improvement in glycemic control, there was no significant change in GCSI over 6 months in adults with T1D and gastroparesis (median 23.5 vs. 18.0, P = 1.0). Change in carbohydrate ratio and active insulin time was similar between the groups. Similarly, there was no difference in change in total daily basal insulin dose (median decrease in basal by 1 vs. 1 unit, P = 0.95), bolus insulin dose (median increase in bolus by 1 vs. 3 units, P = 0.18), and change in weight (median increase in bodyweight by 2 vs. 0 kg, P = 1.0) between patients with gastroparesis and patients without gastroparesis at 6 months compared to baseline (Supplementary Table S1). Of five patients with gastroparesis, two reported taking boluses before meals and two reported taking bolus at the time or after meals. Regarding usefulness of 670G HCL on diabetes control on the scale of 1–10 (1 is not useful at all and 10 is extremely useful), patients reported mean score of 5.8.
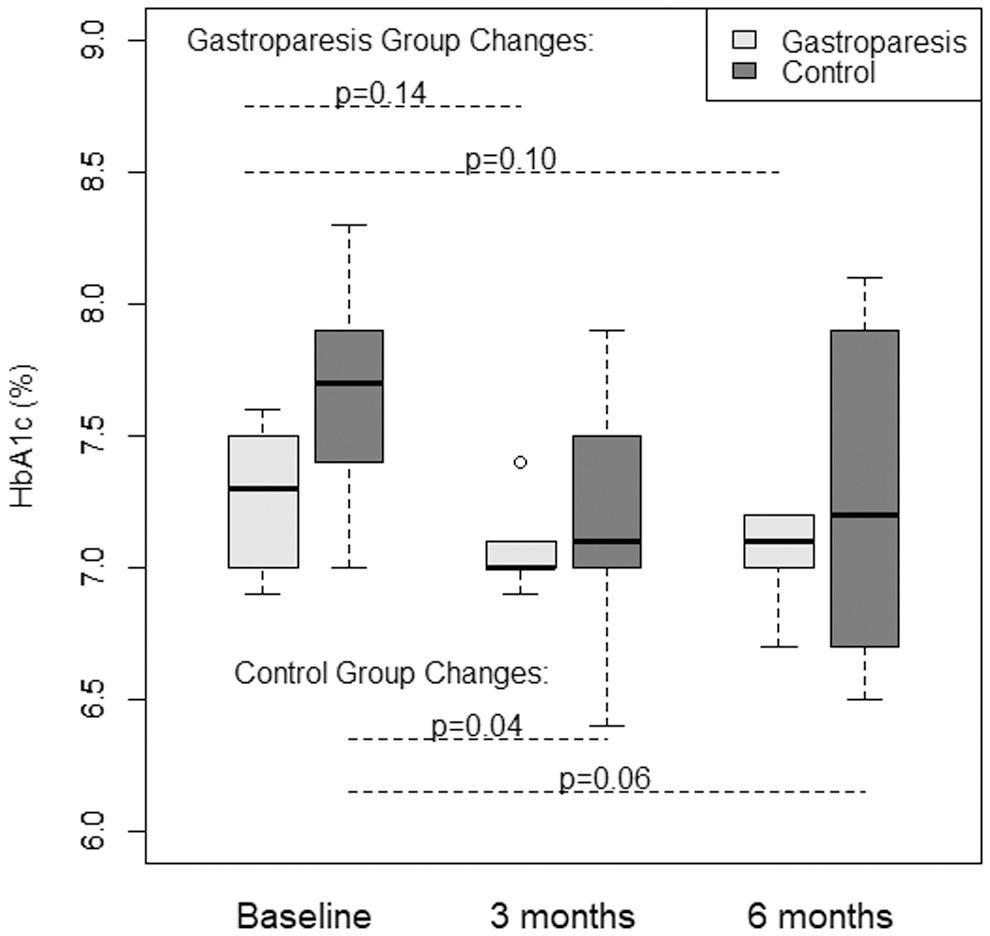
Change in HbA1c in adults with type 1 diabetes with and without gastroparesis over 6 months of hybrid closed-loop system.
Baseline Characteristics of Adults with Type 1 Diabetes With and Without Gastroparesis
Data presented as n (%) or median (IQR).
IQR, interquartile range; T1D, type 1 diabetes.
Change in Time Spent in Normoglycemia, Hypoglycemia, and Hyperglycemia Between Two Groups Over 6-Month Use of Hybrid Closed-Loop System
Data presented as median (IQR).
#Continuous glucose monitor data for 3 months before initiating 670G were considered baseline data.
Wilcoxon signed rank test.
Discussion
Diabetes gastroparesis may result in poor glycemic control along with increased risk of hypoglycemia due to a mismatch between food absorption and insulin action. 2 Patients often use different methods to overcome this timing problem such as using agents to improve gastric motility, delaying insulin administration, or using bolus extension features of subcutaneous continuous insulin infusion systems. 3 However, despite all these efforts, gastroparesis causes significant decrease in quality of life and increase in glucose variability. 1 –4 Studies have suggested that adding GLP-1 analogs to the closed-loop system improves the postprandial glycemic controls in people with T1D due to delayed gastric emptying. 8 Therefore, closed-loop system should be safe and effective in T1D patients with gastroparesis.
In our study, we found that glucose control with HCL use in patients with gastroparesis was not significantly different compared to patients without gastroparesis. Both groups had better HbA1c and improvement in TIR, while utilizing the HCL to control their diabetes. However, differences in HbA1c and TIR over 6 months were not significant in the gastroparesis group, possibly due to small sample size. The initiation of HCL system requires adjustment of two variables, active insulin time and insulin to carbohydrate ratio, to optimize glycemic control while in automode. 9 The changes in these two variables (reduction in active insulin time by 1 h and reduction in carbohydrate ratio by 2–3 g) were similar between the groups, suggesting that adults with T1D and gastroparesis require similar changes in pump settings compared to patients without gastroparesis during HCL initiation.
To our knowledge, this is the first study evaluating efficacy of HCL in adults with gastroparesis and T1D. However, the small sample size, single center, and retrospective study design are major limitations. Most of our patients with gastroparesis were on motility agent and therefore, confounding effect of these drugs on improvement on glycemic control cannot be ruled out. Changes in A1c in previous studies using Medtronic HCL were mainly due to improvement in overnight glucose control. 5 In this study, we did not analyze whether improvement in glycemic control was mainly due to overnight control or postprandial control, which requires further evaluation in future research. The findings of our study with 670G, which uses ePID algorithm, may not be applicable with other closed-loop systems, and therefore, the findings should be interpreted with caution. Larger patient population across a multitude of clinical sites would be warranted to prove the findings of this preliminary study. If HCL is proven to be just as effective in those with gastroparesis, the mental burden of living with not only T1D but also this complication may be alleviated with use of an automated insulin delivery system.
In summary, there is no difference in glycemic control with HCL in adult T1D patients with gastroparesis compared to patients without gastroparesis and appears to be safe in this population. Further research should explore the benefits of HCL systems in the improvement of glycemic control, gastroparesis symptoms, and quality of life in T1D.
Footnotes
Authors' Contributions
V.N.S. conceptualized the study, reviewed data, and edited the article. H.K.A. and N.S. collected the data, and H.K.A., N.S., and H.A. wrote the first draft. L.P. and K.C. analyzed the data. All authors have reviewed and finalized the article before submission. V.N.S. is the guarantor of the work and has full access to the data.
Author Disclosure Statement
V.N.S.' employer (University of Colorado) has received research support from Sanofi US, Dexcom, Inc., NovoNordisk, EyeNuk, National Institute of Health (NIAMS), and Center for Women' Health Research at the University of Colorado. V.N.S. had received honoraria through the University of Colorado from Sanofi US and Dexcom, Inc. for work as an advisory board member. H.K.A. received research support from Mankind, Senseonics, REMD and Eli Lilly. H.K.A. received honoraria through University of Colorado from Sanofi US for work as an advisory board member. H.K., N.S., L.P., and K.C. report no conflict of interests.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.