
Abstract
Aims:
We evaluated the real-life efficacy and safety of empagliflozin in combination with optimized insulin therapy in patients with type 1 diabetes (T1D).
Methods:
This was a prospective study, including 27 patients with T1D treated with insulin therapy to whom empagliflozin was added according to an off-label protocol approved for use in clinical practice. The primary end point was the change in HbA1c 52 weeks after the addition of empagliflozin to insulin therapy. Blood pressure (BP), weight, and safety were also assessed.
Results:
At week 52, the addition of empagliflozin significantly reduced HbA1c from 8.0% ± 0.7% to 7.2% ± 0.8% (P < 0.001). The mean percentage of time in range for capillary glucose monitoring increased from 50% to 62% (P = 0.008) in parallel to a −0.08 IU/(kg·day) reduction in insulin requirements (P = 0.031). There was also a reduction in the body weight (−8 kg) and in systolic BP from 134 to 127 mmHg (P < 0.001). The most commonly reported adverse events were genitourinary infections (10 episodes in 52 weeks of follow-up). One patient developed an episode of mild diabetic ketoacidosis that motivated empagliflozin withdrawal. No severe hypoglycemic events were registered.
Conclusions:
Our results suggested that the use of empagliflozin following a strict off-label protocol may represent an effective and safe option in real life among patients with T1D, improving metabolic control, and ameliorating some cardiovascular risk factors.
Introduction
Nowadays treatment of type 1 diabetes (T1D) consists almost exclusively of intensified insulin therapy, a practice that associates secondary effects such as weight gain and hypoglycemic episodes. 1 Although other pharmacological therapies have been studied, none of them has been proved to be effective and safe. 2 –6 Moreover, the increasing prevalence of cardiovascular morbidity in patients with T1D highlights the need of novel therapeutic strategies that may offer beneficial effects in this respect.
Sodium-glucose transporter type 2 inhibitors (SGLT2i) are a family of oral antidiabetic drugs approved for T2D. 7 –9 The inhibition of SGLT2 results in glycosuria and osmotic diuresis. These drugs show pleiotropic effects such as weight loss, decrease in blood pressure (BP), and a reduction in glomerular hyperfiltration or albuminuria. 10 The insulin-independent mechanism of action makes them a potential therapeutic option for patients with T1D. In addition, randomized controlled trials evaluating the efficacy and safety of several SGLT2i in patients T1D have been published. These studies have demonstrated beneficial results in glycemic control as well as an acceptable safety. 11 –23 The most severe adverse event associated to the use of these drugs is diabetic ketoacidosis (DKA). 8,24 Although DKA has been reported in both T2D and T1D patients, the risk of DKA seems to be higher in the latter.
Despite the increasing evidence published lately about the use of SGLT2i in patients with T1D, the efficacy and safety for the treatment with SLGT2i in patients with T1D at the routine clinical practice setting have not been previously demonstrated. We aimed to evaluate the efficacy and safety of the use of empagliflozin in patients with T1D in addition to intensive insulin therapy following a strict off-label protocol for use in clinical practice.
Methods
Study design and selection of participants
From April 1, 2016 to December 31, 2017, we conducted an observational prospective study, including 27 patients with T1D and suboptimal glycemic control despite intensive insulin therapy. Patients were selected at the Diabetes Unit from Hospital Universitario Ramón y Cajal, Madrid, Spain. The off-label protocol was approved by the Commission of Pharmacy of this hospital. Among SGLT2i, we chose empagliflozin since this drug had the larger amount of published evidence obtained from patients with T1D. 11,17,25 –27
The study protocol conformed to the ethical guidelines of the Declaration of Helsinki, and it was approved by the local ethics committee (protocol 297/17). Patients were informed of the possible benefits and adverse events of the treatment and signed a written informed consent form before starting treatment with empagliflozin. The inclusion criteria were (1) diagnosis of T1D according to American Diabetes Association (ADA) criteria, 6 (2) insufficient metabolic control defined by a HbA1c level ≥7.5% but <9%, and/or (3) previous use of intensive insulin treatment.
Exclusion criteria were (1) poor adherence to medical follow-up; (2) previous treatment with SLGT2i; (3) chronic renal disease, renal transplantation, or renal replacement therapy; (4) ongoing pregnancy; (5) other types of diabetes; and (6) contraindications to the use of empagliflozin.
Clinical, anthropometric, and biochemical variables
We reviewed the medical history and recorded parameters related to T1D and cardiovascular risk factors. Microvascular complications included any diabetes mellitus-related eye disease; neuropathy, including any diabetes mellitus-related neurological complication; and nephropathy, including any diabetes mellitus-related kidney disease. Macrovascular complications consisted of a history of cardiovascular disease. The smoking status was also recorded. Current smoking was defined as having smoked cigarettes during the 30 days preceding the survey. Individuals who had smoked regularly but were not current smokers were considered past smokers. Only individuals who had never smoked were considered as nonsmokers. We also recorded the total insulin dose and distribution of basal/bolus insulin, as well as glycemic control variables derived from self-monitoring capillary glucose (SMCG), including percentage of time in the 70–180 mg/dL circulating glucose range, percentage of time in hypoglycemia (<70 mg/dL), and time in hyperglycemia (>180 mg/dL). 28
Patients were submitted to a complete anthropometric evaluation that included weight and height, and they were classified according to their BMI. Systolic BP, diastolic BP, mean BP, and heart rate were also measured. A fasting blood sample and urine collection served for the analytical assessment of renal function [creatinine and estimated glomerular filtration rate (MDRD-4)], serum lipids and HbA1c, and to measure the urinary albumin–to–creatinine ratio, respectively. The type and frequency of adverse events (severe hypoglycemic events, genitourinary infections [GIs], respiratory infections, positive ketonemia or ketonuria, DKA, withdrawal/discontinuation of treatment and reason, and other adverse events) were also registered.
Off-label protocol of use of empagliflozin in patients with T1D
According to the approved off-label protocol, patients started empagliflozin (initial dose of 5 mg/day) and decreased concomitantly the basal insulin dose by 10%. We made sure that patients committed to capillary blood glucose monitoring (by SMCG at least six times/day) during the treatment with empagliflozin, as well as to capillary ketonic bodies monitoring during the empagliflozin dose titration phase (including the following week after starting or increasing the dose). When the 5 mg daily dose of empagliflozin was tolerated for at least 1 week, the dose was increased to 10 mg/day. Ketone body monitoring was stopped after 14 days of treatment with empagliflozin, when a stable dose was achieved, and only in cases where the patient has showed an adequate tolerance without any incidents during the titration phase. In case of elevation of ketone bodies (>0.6 nM in capillary blood), the patient discontinued empagliflozin treatment and proceed with the management of positive ketonemia.
At inclusion, all patients completed a preplanned education training provided by qualified diabetes educators, with information about how to recognize signs and symptoms of DKA; how and when monitor blood ketone levels and what actions to take for elevated ketonemia (hydration, carbohydrate intake, and insulin administration). Patients were encouraged to determine blood or urine ketone bodies in every possible DKA triggering situation throughout the study (changes in diet, activity, or insulin dose as well as for concomitant events such as infection, dehydration, surgery, injury, or pump occlusion/malfunction). Treatment was started and supervised by an experienced practitioner in diabetes (L.N.-C.).
Medicals visits were programmed at 1, 3, 6, and 12 months after starting empagliflozin. At every visit, physical examinations were performed and SMCG and capillary HbA1c measurements were registered. Blood samples were obtained at the initial visit and after 6 and 12 months of empagliflozin use.
Statistical analysis
Qualitative variables are represented as counts and percentages. Continuous variables are expressed as mean ± SD or median (interquartile range) as appropriate. Normality of continuous variables was ensured by applying logarithmic transformations or by applying a two-step transformation method, 29 and it was checked using the Kolmogorov–Smirnov test. We applied nonparametric tests to variables remained skewed even after transformation. We used univariate repeated measures general linear models to compare the means at baseline and after 12, 24, and 52 weeks. We performed both intention-to-treat and per protocol analysis. Three of the 27 patients withdrew treatment with empagliflozin and were excluded from per protocol analysis (Fig. 1). For both intention-to-treat and per protocol analysis, the last observation was carried forward as a method of imputing missing data. Data were available for 89% of all visits for systolic BP, 89% for diastolic BP, 89% for body weight and anthropometric measures, 81% for SMCG and 89% for total doses of insulin. Statistical significance was set at the P < 0.05 level. We used SPSS Statistics 23.0 (IBM, NY) to perform the statistical analysis. SigmaPlot™ (SSI, San Jose, CA) was used to draw the figures.
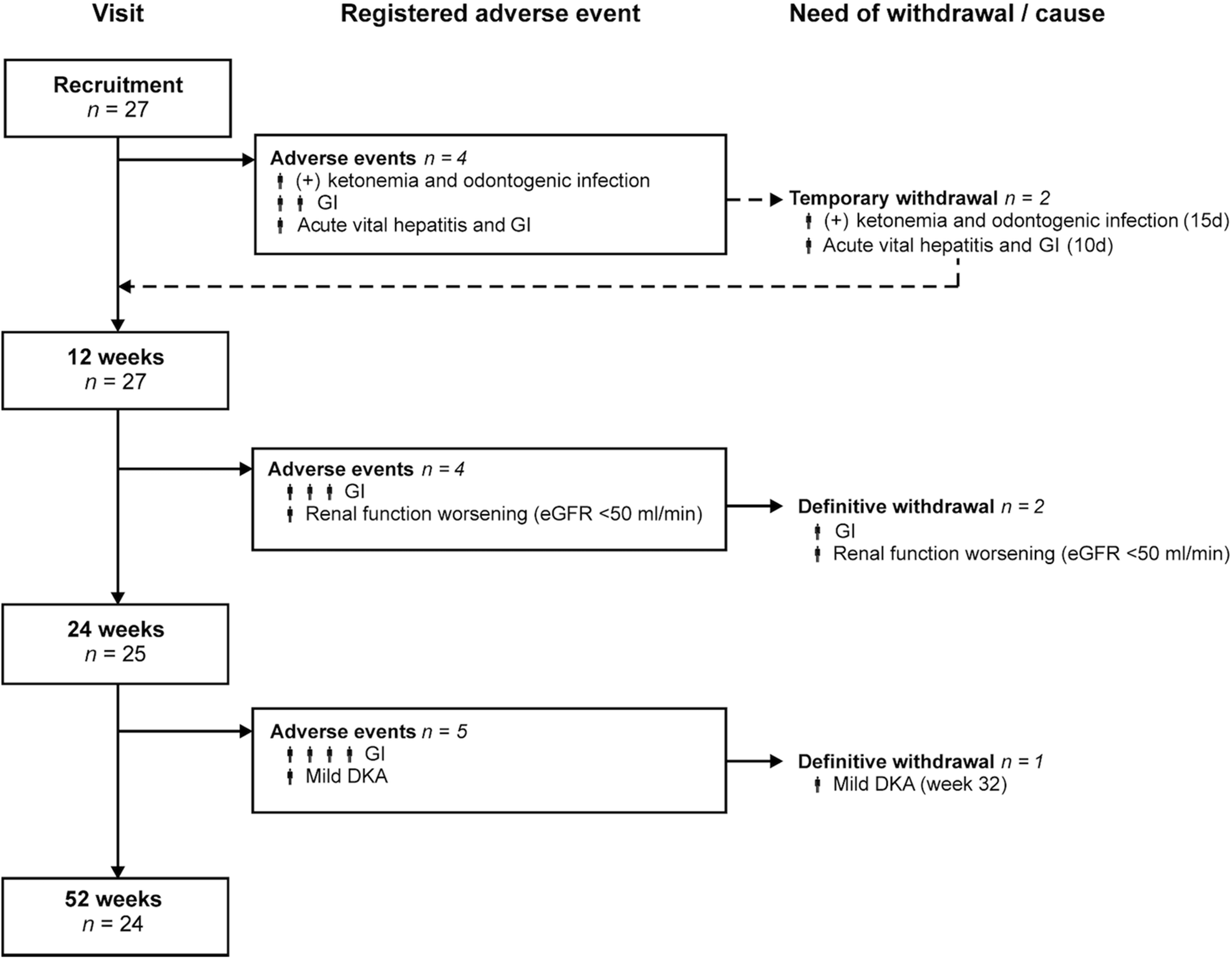
Flowchart representing number of patients who entered the study and at each visit, registered adverse events, time of occurrence, and need of withdrawal of empagliflozin. For temporary withdrawal, the time lapse during which the drug was withdrawn is given in brackets (days). DKA, diabetic ketoacidosis; eGFR, estimated glomerular filtration rate; GI, genitourinary infection; n, number of patients.
Results
A total al 27 patients (13 men and 14 women) with T1D entered the study. Their mean age was 45 ± 12 years. Mean duration of diabetes was 23 ± 12 years. Most patients used multiple insulin dose injections (82%), whereas the remainder used continuous insulin infusion devices. At baseline, the mean insulin dose of study subjects was 0.62 ± 0.22 IU/(kg·day). Nineteen patients had a total insulin dose >0.5 IU/(kg·day). Ten (37%) patients had evidence of microangiopathy and three (11%) had macroangiopathy. Nine (33%) patients had hypertension, whereas 16 (59%) had obesity. Five (19%) patients were receiving metformin in addition to insulin, and nine (33%) had suffered at least one episode of DKA. Their baseline HbA1c was 8.0% ± 0.7% and their BMI was 32 ± 4 kg/m2 (26 out of 27 patients had a BMI >27 kg/m2).
During treatment with empagliflozin the patients showed a statistically significant improvement in glycemic control variables, (Fig. 2), including a decrease in HbA1c—already observed after 12 weeks of treatment that persisted after 24 and 52 weeks—and an improvement in indexes of glycemic variability (measured by SMBG) such an increase in the percentage of time in range and a reduction in the percentage of time in hyperglycemia. Besides, we observed a near significant tendency toward a decrease in the coefficient of variation in the first 24 weeks (per protocol analysis, P = 0.206; intention-to-treat analysis, P = 0.127).
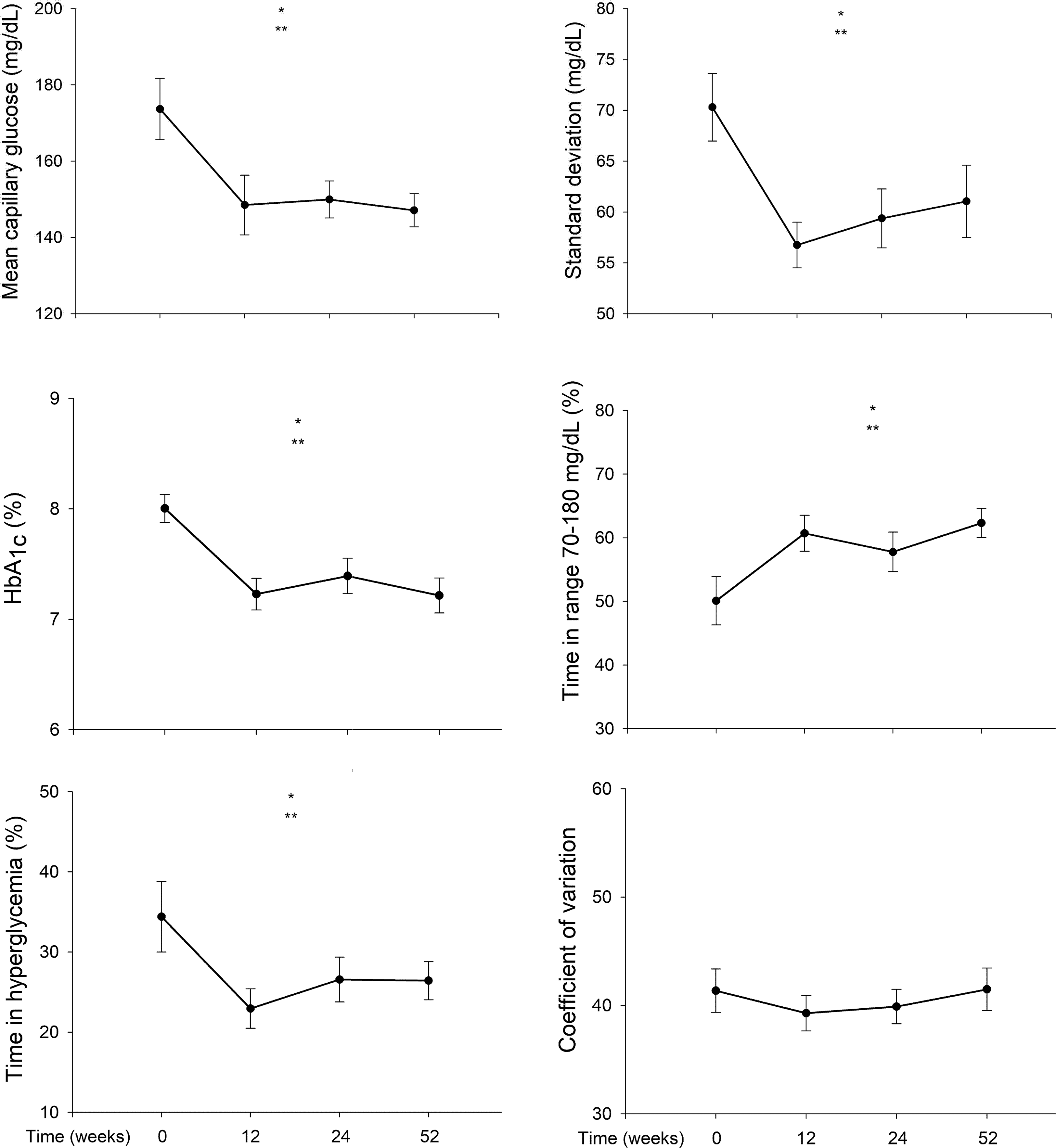
Changes in indexes of metabolic control during empagliflozin administration in patients with type 1 diabetes, including mean capillary glucose (left upper panel), standard deviation (right upper panel), HbA1c levels (left medium panel), time in range (right medium panel), time in hyperglycemia (left bottom panel), and coefficient of variation (right bottom panel) at 0, 12, 24, and 52 weeks. Data are means ± SEM of the analysis per protocol. *P < 0.05 for per protocol analysis. **P < 0.05 for intention-to-treat analysis.
Regarding anthropometric variables, we observed an improvement in systolic BP and a reduction in body weight (Table 1), with the mean BMI being in the overweight range after 52 weeks of treatment (Table 1). Total daily insulin requirements decreased significantly at the expense of both basal and bolus insulin that decreased similarly (Table 1). There were no statistically significant changes in uric acid, total cholesterol, low- or high-density lipoprotein cholesterol, and triglyceride levels (data not shown).
Anthropometric Parameters, Glycemic Control Variables, and Laboratory Parameters at Baseline and 12, 24, and 52 Weeks After Starting the Treatment with Empagliflozin (n = 27)
Bold italic form show a significant P value.
Data are means ± SEM of the intention-to-treat analysis. n (%): number of patients (percentage) included for per protocol analysis in each variable.
Excluding outliers.
P value is given for per protocol analysis (*) and intention-to-treat analysis (**).
The flowchart (Fig. 1) describes the registered adverse events, time of occurrence, and need of withdrawal of empagliflozin. The most common adverse events reported were GIs, including low urinary tract infections and candidiasis (10 episodes during the 52 weeks observation period). In one case the drug had to be withdrawn definitively because of recurrent infections. In two patients, the drug had to be temporarily discontinued due to the development of acute viral hepatitis in the first case, and due to the presence of positive ketonemia secondary to odontogenic infection in the second one. The drug was reintroduced later without any other complication in these patients. No severe hypoglycemic events were registered. We did not observe an increase in percentage of time in hypoglycemia after starting empagliflozin or found significant differences in renal function safety parameters (Table 1). In one case the drug was definitively discontinued after 24 weeks of administration because of the decreased estimated glomerular filtration rate <50 mL/min due to excessive diuretic therapy. Also, we observed a statistically significant increase in the hematocrit (per protocol: 43% ± 5% to 46% ± 5% after 52 weeks, P = 0.012; intention-to-treat analysis: 43% ± 4% to 45% ± 5% after 52 weeks, P = 0.008).
During the 52-week period of the study, we registered one event of mild DKA that occurred after 32 weeks of empagliflozin administration. The patient was a 43-year-old man on continuous subcutaneous insulin infusion (CSII), with a long history of diabetes and a HbA1c level of 7.5% before entering the study. As comorbidities, he had a nonproliferative diabetic retinopathy, nephropathy consisting of albuminuria <300 mg/g creatinine with normal glomerular filtration rate, and hypertension. His BMI was 31.5 kg/m2 at inclusion. The patient had shown an excellent response to empagliflozin, with a decrease in his total insulin dose from 72 to 47 IU/day, a weight loss of 9 kg, and a decrease in HbA1c of 0.5% after 6 months of treatment. As probable triggering factors, we recognized insulin pump failure and alcohol consumption. The patient had been in hyperglycemia for >12 h before reporting to the emergency room (ER), and although he administered correction insulin doses using his CSII, he had not monitored ketone bodies as it was specified in our protocol. Laboratory evaluation in the ER displayed a blood glucose level of 212 mg/dL, a capillary β-hydroxybutyrate concentration of 3 mM, a serum bicarbonate of 22.5 mM, an arterial pH of 7.27, with a normal venous lactate level. The patient was treated with intravenous fluids, insulin, and glucose, and the DKA solved in <24 h with any further complication. Finally, empagliflozin was definitively discontinued and the patient was discharged home without any further negative consequences.
Discussion
Our present results suggest that real-life treatment of patients with T1D with empagliflozin in addition to insulin therapy, when following a strict protocol, improves glycemic control and has beneficial effects of cardiovascular risk factor, while showing an acceptable safety profile.
Current estimations indicate that up to 75% of individuals with T1D do not reach glycemic control objectives (HbA1c <7.0%) or, even if reaching them, their glycemic variability is large enough to put them at risk for the development of microvascular complications. 6 Limited options for the treatment of T1D together with the insulin-independent mechanism of action of SGLT2i turn these drugs into potential therapeutic alternatives for these patients. Initial phase 2 trials conducted with SGLT2i in patients with T1D, despite short follow-up periods, showed beneficial effects, including a reduction in mean blood glucose, glycemic variability, total insulin dose, and body weight. 11 –18,26–28 Phase 3 randomized controlled trials with larger sample sizes and longer follow-up periods were published afterward, demonstrating similar efficacy end points without increasing the frequency of hypoglycaemia. 19 –23,26,31 –34 Likewise, parameters of glycemic variability obtained from SMCG or continuous glucose monitoring system (CGM) seemed to improve in T1D patients who were on treatment with SGLT2i. 9,23,33,34 –36 However, real-life experience with these drugs in patients with T1D followed at their usual clinical practice has not been reported to the best of our knowledge.
Our experience showed that the use of empagliflozin, following approved, strict, and standardized off-label protocol, resulted into an improvement in glycemic control consisting of a decrease in HbA1c, a reduction in glycemic variability and a decrease in the total insulin daily dose. Other beneficial effects such as weight loss or decrease in systolic BP were also observed. These results complement those of previous randomized clinical trials in patients with T1D, even though the patients in our study had higher BMI and more prevalent obesity than those included in phase 3 studies. 21 –23 Of note, selection bias toward inclusion of patients with larger weight in our present study may explain why our results were even better than those observed in with industry-driven randomized clinical trials. 9,25,27,36,37
Regarding safety, our real-life experience resembles that of clinical trials, with GI usually mild, being the most frequent adverse events. 36,38,39 Similarly, GIs were the most frequent adverse events with only one patient requiring empagliflozin definitive discontinuation. Hypoglycemia has been another common secondary effect of SGLT2i in patients with T1D that usually resulted from inappropriate adjustment of insulin doses and not from a drug class effect. 13,21,22,30 Following our off-label protocol, patients in this study reduced by 10% their basal insulin doses when starting on empagliflozin and further gradual adjustments were carried out as needed. As a result, we did not find an increase of time in hypoglycemia nor registered any severe hypoglycemic event.
Only one the 27 patients with T1D treated with empagliflozin in our series developed DKA. In this case, DKA was hyperglycemic and not euglycemic and was related to probable insulin pump failure. The reported incidence of DKA in the literature varies; phase 3 studies described incidences between 1% and 6%, but in these trials very few patients experienced an intercurrent illness during the study and strict measures for prevention of DKA were applied. 11,13,16,19 –23,25,32,34,36,40 Chen et al. 41 presented a meta-analysis of 10 trials, including 581 patients with T1D and showed an increased incidence of DKA in patients treated with SGLT2i against placebo, documenting 16 DKA events. Similar results were confirmed by a larger meta-analysis of 14 studies, including 4591 patients. 9 In most of the cases of SGLT2i-related DKA reported in the literature there were recognizable triggering factors, suggesting that this condition might be predictable and potentially prevented. 42 These triggering factors include abrupt or excessive decreases in insulin doses, insulin omission, major surgery, infection, reduction of water or food intake, and low-carb diets or an increase in physical activity. 25,43 Furthermore, the balance between glucagon and insulin may be particularly critical in patients with SGLT2i-related DKA. SGLT2i appears to be associated with an increase in glucagon levels by means of urinary glucose losses, and directly, by stimulating pancreatic alpha cells. That hyperglucagonemia would induce lipolysis and ketogenesis. 42 –45 As well, SGLT2i might decrease ketone body clearance contributing to the development of DKA. 24,46,47
Our interest in developing an off-label protocol for the real-life use of SGLT2i in T1D patients was to establish clear indications for the use of SGLT2i in these diabetic patients and to ensure strict standards for ketone body monitoring, insulin therapy adjustment and dose titration in the clinical setting. The National Institute of Health and Care Excellence (NICE) recently published guidelines on the issue suggest restricting the use of dapagliflozin to poorly controlled patients with T1D presenting with a BMI >27 kg/m2 and a total insulin dose >0.5 IU/(kg·day) (
Our subsequent results confirm the efficacy and safety of such a protocol at least for the 1-year duration of the study. According to our experience, we might suggest that patients with T1D who may obtain the greater advantage of SGLT2i are those who (1) have not achieved appropriated targets of glycemic control for their age, duration of diabetes, and comorbidities; (2) are compliant and committed to the strict follow-up required; (3) are able and willing to monitor blood or urine ketone bodies at the beginning of SGLT2i treatment, when increasing its dose, in situations that increase the risk of ketogenesis, or when persistent hyperglycemia occurs; (4) have adequate knowledge of the measures needed for the correct management of mild ketosis; (5) have a moderate cardiovascular risk because of weight excess or hypertension; and (6) have no history of recent or multiple DKA nor an eating disorder.
In addition, other authors suggested that physicians attending T1D patients must have a low threshold for withdrawal of SGLT2i in case of intercurrent illness, and that the awareness of the occurrence of euglycemic DKA by primary care and emergency departments must be enforced. 8,46 Physical stress, abdominal pain, vomiting, fasting, increased physical activity, alcohol intake, or fever are among the reasons for monitoring ketone bodies in these patients, regardless of their actual blood glucose levels. Recently, Garg et al. 46 published updated recommendations for the management of mild ketosis/ketoacidosis in T1D patients on SGLT2i treatment, highlighting the importance of symptoms recognition.
Nevertheless, we are aware of certain limitations of our study, including (1) the absence of a control group, (2) its small sample size, (3) the time of follow-up limited to 1 year, and (4) a selection bias favoring the inclusion of T1D patients who may benefit the most from SGLT2i such as those with weight excess. Regarding its possible strengths, we wish to underline that our study was conducted at a clinical setting, warranting the applicability of the off-label protocol of empagliflozin addition to insulin regimens during follow-up intervals usually recommended for the routine management of T1D. Anyway, larger studies in terms of sample size and more prolonged follow-up are needed to establish definitively the profile of patients with T1D who may benefit the most from SGLT2i coadministration with insulin, as well as the precise indications and the safety of such a therapeutic approach in this setting.
Conclusion
The addition of empagliflozin to insulin following a strict off-label protocol might be effective and safe in patients with T1D who have suboptimal glycemic control, and it may in turn show a beneficial impact on cardiovascular risk factors in these patients. The benefits of such therapeutic approach should be carefully balanced against the potential risks on an individual basis, to minimize the possibility of potentially severe complications.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.