
Abstract
Background:
Continuous glucose monitoring (CGM) has a beneficial impact on diabetes control; however, its utilization within people with diabetes remains low. The success of CGM requires cluster of cognitive skills and executive functions (EF). We speculated that participants with high EF would be more adherent to CGM use.
Materials and Methods:
The study population included 85 children and adolescents between 5 and 18 years old being followed for type 1 diabetes. Participants and their parents completed three questionnaires—“Behavior Rating Inventory of Executive Function” (BRIEF), CGM satisfaction, and a questionnaire assessing reasons for discontinuing CGM use.
Results:
Sixty-one participants used CGM on a regular basis and 24 discontinued use. Adherent participants were significantly younger than participants with nonadherence to CGM (P = 0.011). No significant differences were found between gender, diabetes duration, or HbA1c. Females adhering to CGM had a significantly higher “organization of environment” skill than those with nonadherence to CGM (P = 0.023). Also, adherent participants older than 14 years had a higher “organization of environment” skill than participants with nonadherence to CGM (P = 0.032). No difference was found between the groups in other EF domains. Alarm fatigue was found to be the main reason for discontinuing CGM.
Conclusions:
Given the interplay between CGM adherence and EF, it is recommended that people with diabetes should receive training by a multidisciplinary team, including psychological counseling, before CGM use and thus preparing them to cope with the demands of CGM and to avoid false expectations.
Introduction
The potential benefits of continuous glucose monitoring (CGM) are well established in the literature. A meta-analysis demonstrated improved glycemic control, a lower HbA1c, and fewer hypoglycemic events among adults using CGM. 1 In the pediatric group, CGM usage was associated with lower HbA1c and fewer diabetes-related emergency visits. 2,3 Glycemic control was closely correlated with the level of adherence to sensor use. 4 –6 Children who used CGM on a near daily basis had a greater reduction in HbA1c and spent more time within range than children with less frequent use.
Despite the recognized benefits of CGM, overall device usage rates remain low. The type 1 diabetes (T1D) Exchange Survey reported a recent increase in CGM usage during 2016–2018, 37% of children (6–12 years), 24% of adolescents (13–18 years), and 22% of young adults (18–26 years) used CGM, a fourfold increase to previous years (2010–2012). Despite this, a deterioration in glycemic control was noted between these two time periods, particularly among teens and emerging adults. 7,8 A similar trend was reported by the DPV German/Austrian registry with 19% of the participants using CGM in 2016. 9
Many patients who started using CGM subsequently discontinued its use; 41% in the T1D Exchange Survey and 21% of adolescents and 20% of children in the JDRF Multicenter Study. 4 In reality, it is likely that CGM adherence is lower than reported in the abovementioned studies.
The reason for poor CGM adherence is not clearly understood. 10,11
Ideal CGM adherence depends on both the patients' and their families' organizational capacity. Proper management of daily tasks such as dietary intake, exercise, blood glucose monitoring, and insulin administration is vital. 12 Efficient completion of these tasks relies on a set of cognitive skills incorporated under the umbrella of executive functions (EF), including planning, problem-solving, organization, working memory, and behavioral self-regulation.
Competence in EF may have a significant impact on adherence to treatment and management of diabetes. Several studies have found a correlation between EF, as measured by questionnaires, and treatment adherence among adolescents with type 1 diabetes mellitus (T1DM); 13,14 however, no study has yet explored the relationship between EF and the specific adherence to CGM.
This study aimed to investigate the hypothesis that children with higher levels of EF have improved CGM adherence. Reasons for discontinuing CGM usage were also explored.
Materials and Methods
A single-center retrospective study design was utilized. The study cohort comprised 85 T1D participants aged 5–18 years undergoing regular follow-up at the Schneider Children Medical Center between December 1st 2015 and July 31st 2017. Participants were recruited if they had used CGM for at least 1 month. Those using CGM exclusively for a clinical study were excluded so to represent everyday life. Demographic and clinical data were collected from electronic records, including adherence or nonadherence to CGM. Nonadherence to CGM was defined by complete discontinuation of CGM during the month before the clinical visit.
Assessment of EF and CGM use was derived from the questionnaires listed below; surveys were completed by both the parent and the participant at a single routine clinic visit.
(1) Behavior Rating Inventory of Executive Function (BRIEF) questionnaire: Consisting of 86 parent-reported responses that evaluates the domains of executive functioning (goal setting, organization, working memory, and so forth). It uses 3-point Likert scale, in which parents express the frequency of the child's behavior (never occurred, sometimes occurred, or occurred often). Reliability of the BRIEF has been established (0.80–0.98) for both clinical and normative samples. It has been validated with other measures of behavioral and attentional functioning. 15
(2) CGM satisfaction (CGM-SAT) questionnaire comprised 37 statements relating to CGM use, satisfaction, and influence on diabetes management. A 5-point Likert scale is used, in which the responder rates their level of agreement with each statement. Overall scores range from 37 to 185, with a higher score indicating greater degree of satisfaction with CGM. 16
(3) A structured questionnaire assessing patient expectations of CGM as well as reasons for discontinuing CGM use when relevant.
The study was approved by the Institutional Review Board Committee of Rabin Medical Center. Informed consent was obtained by all participants or by their parents.
Statistical analysis
The Mann–Whitney U test was used for the analysis of skewed distribution. Independent samples t-test was used for normally distributed data. Data were analyzed using SPSS version 23.0.
Results
The study cohort consisted of 85 participants, of which 41 (48%) were males. The median age was 13.4 years (interquartile range [IQR]: 10.7–15.5). Median HbA1c was 7.8% (62 nmol/mol), and the duration of diabetes was 5.1 years (IQR: 3.2–7.5).
Among this cohort, 61 (72%) participants were defined as adherent to CGM use (group 1) and 24 participants (28%) had lower adherence to CGM (group 2).
CGM devices that were used by cohort participants included 39 (46%) Minimed EnliteTM (Medtronic, Northridge, CA), 29 (34%) Freestyle Navigator® II CGM (Abbott Diabetes Care, Alameda, CA), and 17 (20%) Dexcom G4 Platinum (Dexcom, Inc., San Diego, CA). The Medtronic Minimed Paradigm Veo pump was the only pump connected to a CGM (Minimed Enlite).
Baseline characteristics of the two groups are presented in Table 1. There were no significant differences in gender, parental education, glycated hemoglobin, (A1C) or duration of diabetes between the groups.
Baseline Characteristics—Adherent Versus Participants with Nonadherence to Continuous Glucose Monitoring
A1C, glycated hemoglobin; CGM, continuous glucose monitoring; IQR, interquartile range; N.S., no significant differences.
Adherence to CGM was inversely correlated with age (P = 0.011); the median age in group 1 (13.0 years, IQR: 9.3–15.0) was significantly lower than in group 2 (15.1 years [IQR: 13.3–16.1]).
EF as explored by the BRIEF questionnaire
No significant association was found between any single EFs as measured by BRIEF and adherence to CGM. Subgroup analysis by age (Table 2) demonstrated that adherent participants 14 years of age and older had a significantly stronger “organization of environment” skill than those who discontinue CGM use (47.6 ± 9.4 vs. 54 ± 7.8, P = 0.032). In a subgroup analysis by gender (Table 3), a statistically significant association was found between adherence and “organization of environment” scale among females (45.4 ± 8.6 vs. 51.9 ± 9.3, P = 0.023). Moreover, females with difficulties in planning skill were less adherent to CGM compared to those with better planning skills (52.1 ± 10.2 vs. 46.1 ± 5.8, P = 0.059).
Executive Functions by Adherence to Continuous Glucose Monitoring, Stratified by Age Groups (5–14 and 14–18)
Executive Functions by Adherence to Continuous Glucose Monitoring, Stratified by Gender
CGM-SAT as explored by the CGM-SAT questionnaire
CGM-SAT scores were correlated with adherence to CGM for both genders (mean ± standard deviation) (82.6 ± 22.6 vs. 108.6 ± 20.1 and 85.5 ± 20.5 vs. 108.0 ± 10.6 in males and females respectively, [P < 0.001 for each]). These correlations were seen with both hassles and benefits subscale scores (P < 0.001 for each). Responses in CGM-SAT questionnaire which differed the most between the two groups included: “It is more of a bother than useful”, “there were too many unjustified alarms”, “it is complicated to operate”, and “it interferes with sleep”.
Expectations from CGM use as explored by the third questionnaire
Most participants expected that CGM would allow for fewer blood glucose checks (average 4.6 in a scale from 1 to 5) and that their diabetes control would improve with CGM (average 4.4 in a scale from 1 to 5).
Reasons for discontinuation of CGM
The main reasons for CGM discontinuation were as follows: “too many alarms” (54%), “inconvenience with wearing two devices on the body” (50%), and “failure to meet expectations” (38%) (Fig. 1).
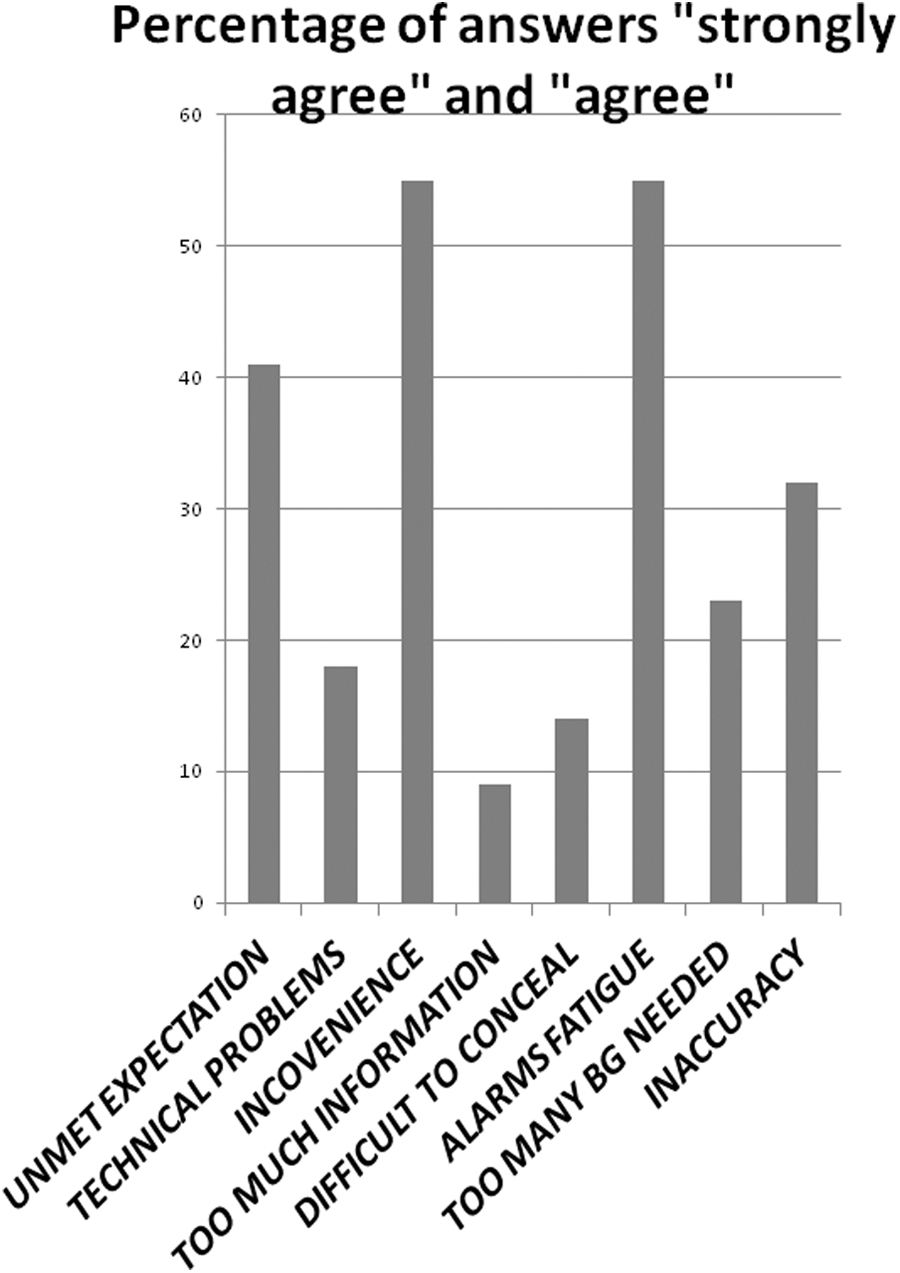
Reasons for discontinuation of continuous glucose monitoring.
Discussion
In the present study, we found that a stronger “organization of environment” skill was associated with greater adherence to CGM in the age group older than 14 years (P = 0.032).
This skill encompasses one's ability to organize their everyday environment, including work and living areas, such as desks and closets. 15 People who have difficulties in this area often have problems in managing their diabetes. Their overall level of functioning is inefficient, often misplacing objects such as the glucometer, CGM receiver, insulin vials, or sticks. This challenge is accentuated with concurrent use of an insulin pump, 17 with patients being overwhelmed by the use of multiple devices on a daily basis, a factor which is likely to lead to CGM discontinuation.
The association between “organization of environment” and adherence to CGM was not significant in the younger cohort, children <14 years old, as opposed to adolescents. We speculate that as younger participants are primarily dependent on a primary caregiver, a parent, difficulties in a child's EF would not influence CGM adherence.
When stratified by gender, the skill of “organization of materials” was stronger in females adhering to CGM (P = 0.023). Planning skills were also superior among females who were adherent to CGM, however, this difference did not reach statistical significance (P = 0.059). These associations were not found in the male cohort.
Planning skills encompass one's ability to anticipate future events, implement goals and take appropriate steps before performing an activity. 15 The planning skill plays a fundamental role in the management of CGM in people with diabetes, being essential for sensor insertion and calibration, taping and changing of sensors, responding to CGM alerts, as well as for insulin administration, inserting the insulin pump, taping it, replacing insulin tubing equipment, and so forth.
No significant associations were found between global executive composite index, behavioral regulation index (BRI), metacognition index (MCI), or any other EF scale with adherence to CGM. These findings differ from the literature. Bagner et al. demonstrated a significant relationship between BRI of EF and adherence to CGM in a cohort of 130 children with T1DM. 18 In contrast, Miller et al. did not establish an association between the MCI of EF with adherence to CGM or with glycemic control. 14 In Graziano et al., 19 an examination of an adolescent cohort subgroup analysis revealed improved adherence to diabetes management among males with greater cognitive flexibility, attentional control, and goal setting. In contrast, this association was seen among females in our study population.
A recent study examined the relationship between child EF, as well as parental EF with adherence to diabetes treatment, and the level of glycemic control. This study found significant consistent interaction between child EF and parental EF. Mainly, patient EF problems were related to treatment adherence and glycemic control, especially in older children and less related to parental EF. 20 None of the aforementioned works investigated the associations between EFs and adherence to CGM.
In our study, adherence to CGM use was inversely correlated with age (P = 0.011). These results are in accordance with those found by Rachmiel et al. who reported that consistent CGM users were younger than intermittent users. 21 De Bock et al. found that age was the only predictor of adherence to CGM use. 22 Multicenter and larger registry studies showed glycemic control to be consistently worse among adolescents; 4,7,9 nonadherence to treatment regimens such as CGM may be a likely culprit. This pattern of patient compliance is obvious in the adolescent population suffering from other chronic diseases. 23,24
Our study showed a significant positive association between CGM-SAT score and adherence to CGM (P < 0.001). Similar results were reported in the JDRF study, in which CGM-SAT was higher in participants using CGM consistently. 25,26 We speculated that participants with less frequent CGM use may be more displeased by multiple CGM sensor alarms, whereas compliant participants may likely derive greater benefits than disadvantages from CGM use. 27
The abovementioned findings emphasize the necessity for comprehensive education regarding CGM as well as evaluation of EF before CGM use, thus allowing patients to develop realistic expectations.
The most frequent reasons for discontinuing CGM in our study included alarm fatigue, the inconvenience of wearing the sensor, and failure to meet the participant's expectations. Possible reasons for nonadherence among adolescents, as reported both in our study and in the literature, include a problem with body image and interference with sports and other activities. 28 –30 Rachmiel et al. 21 found that pain, inaccuracy, and frustration with device alerts were the main reasons for discontinuing CGM.
Technology is changing at a rapid pace, and since the completion of the current study, CGM technology has progressed. Some of the current available CGM devices do not need calibration, they are more compact, and sensor insertion is easier, all of which improve user experience. These improvements may account for the dramatic increase in CGM use in the pediatric Exchange T1D cohort from 7% in 2010–2012 to 30% in 2016–2018. 8 It is quite possible that the inconvenience of CGM use will lessen with advancements in CGM equipment. Thus, future reasons for nonadherence might be different from the current study's results.
The treating medical team should also contribute to improve CGM adherence by coping with the reason for discontinuing CGM of “failure to meet the patient's expectations”. CGM demands more comprehensive education before use, demanding extra workload on the treating team, explaining to the patients and their families the advantages and disadvantages of CGM, aiming to achieve realistic expectations. 31 People with diabetes must be taught how to use CGM technology, how to set the alarms gradually, and to adjust them according to frequency of hyper- and hypoglycemia events, allowing optimization of CGM benefits and therefore optimizing patient satisfaction. Unrealistic expectations will only add to the burden carried by adolescents with difficulties in planning skills.
The intensive preparation program before CGM use should include appropriate psychological counseling and support, particularly since psychological difficulties may be part of the reason for discontinuing CGM.
Our study has several limitations. First, it is retrospective in nature, with participants having to recall the reasons for discontinuing CGM. Parental assessment took place on average 19.8 ± 12.3 months after discontinuing CGM. This may lead to recall bias with parents answering the questionnaires based on the child's current outlook rather than on their attitude at the time of discontinuation. Second, the BRIEF questionnaire, which is intended to be completed by parents, may less accurately evaluate the participant's EF, particularly that of adolescents.
Third, this study was observational in nature and thus the two groups were not equal in size. In addition, our study was not designed to assess the influence of CGM use on glycemic control.
Study strengths included the participants themselves, all of which were part of diverse ethnic, gender, and age groups, although being treated in a single medical center at the same time period. In Israel, every patient with T1D younger than 18 years of age with documented hypoglycemic events (four events below 70 mg/dL for children younger than 8 years and two events below 50 mg/dL for older patients) receives financial reimbursement by the government for CGM use. As it is nationally reimbursed, health disparities and socioeconomic bias are not expected. This study assessed real-life adherence and did not include any intervention by the study team. It has an advantage over a structured study, in which continued structural support may influence adherence.
In conclusion, adherence to CGM was related to the EF skill of “organization of environment” in adolescents and among females. Given that psychological difficulties may be part of the reasons for discontinuing CGM, these results emphasize the need for an intensive preparation program by the treating team before CGM initiation. This education should aim to provide the patient and his family with the necessary knowledge and skills as well as the psychological support to avoid false expectations. An effective program may increase adherence to CGM and improve diabetes management and control.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.