
Abstract
Background:
Continuous glucose monitoring (CGM) systems are widely and increasingly used in diabetes self-management and in the context of clinic visits. However, access to CGM data during visits can be challenging. Clinic inefficiencies can restrict the time available for patient education, and the inability to integrate CGM data into electronic health record (EHR) systems can result in data being lost. In this study, we describe our institution's approach to integrating CGM data directly into the EHR through a partnership with a CGM device manufacturer and without a third-party data aggregation/data visualization platform.
Methods:
We interviewed key stakeholders with the hospital Information Technology Department, the Division of Pediatric Endocrinology, and a CGM device manufacturer. A collaborative, human-centered design approach was used to define the workflow. Health Level 7 (HL7) standards were used to build all data exchanges.
Results:
In collaboration with all parties, we created a simple network architecture design for both account linkage and data acquisition. The system uses the standard, computerized, physician order entry interface available in the EHR for both processes. Data acquisition occurs in real time, and customized reports are displayed within the results section of the EHR. The entire process is Health Insurance Portability and Accountability Act (HIPAA) compliant and meets all security requirements.
Conclusions:
Building scalable data integration using HL7 standards is possible and allows real-time access to CGM data within the diabetes provider's existing workflow and can occur with or without the patient present. This may lead to improved clinical outcomes, increased efficiency, and new revenue opportunities by documenting CGM data capture and review.
Introduction
The prevalence of diabetes is increasing, with an estimated 387 million people reported to have diabetes worldwide in 2014, of which type 1 diabetes (T1D) accounts for between 5% and 10%. 1 Over 10% of deaths in the United States are at least partially attributable to diabetes-related complications, 2 and most of these are attributable to high blood glucose. 3 Inadequate blood glucose control, including hypo- or hyperglycemia, results in life-threatening vascular and cardiac complications such as stroke, heart disease, vision loss, and kidney disease. 4
Particularly in T1D, where daily administration of insulin to maintain blood sugar levels is required, frequent blood glucose monitoring is a critical part of daily diabetes management. With the advances of FDA-approved, continuous glucose monitoring (CGM) devices, we have gained more in-depth knowledge of fluctuations in blood glucose levels with alerting alarms of extremes of hypo- and hyperglycemia. 5 –7 The robust data, trend identification, and predictions provided by modern CGM devices assist patients and providers in making adjustments in therapeutic protocols and provide guidance to modify patients' diet and lifestyle. 5 CGM has the potential to improve glycemic control by providing real-time feedback to those with diabetes and those involved in their care. 7
Accessing CGM data during clinic appointments can be challenging and may disrupt clinical workflow, resulting in limited time for patient education on self-management. These limitations can be addressed by offering direct integration of CGM data into the electronic health record (EHR) using available consumer technology. 8,9 The advantages of CGM data integration include accurate clinical evaluation, longitudinal view of disease progression, and efficacy of treatment plan outside of clinic visits. Unfortunately, most attempts at EHR-CGM data integration have required significant effort and custom data interfaces. 10,11 Recently, at least one group has had success in addressing this issue using widely available consumer technology. 9 Others have used third-party data aggregators to collect and visualize patient data. 12 In this study, we present a third approach to this problem: a partnership with the CGM device manufacturer to exchange CGM data directly from the manufacturer's cloud with our hospital EHR. We will describe the process to establish the scalable automated integration of home-based CGM data into the EHR to improve health care provider workflow and enable better remote care.
Methods
Project genesis and goals
In 2017, a major CGM device manufacturer (Dexcom, San Diego) collaborated with the Children's Hospital Los Angeles (CHLA) Research Institute to develop a novel data integration project. A committee of corporate and institutional stakeholders, including Dexcom, the Research Institute, the Center for Innovation, the Information Technology (IT) Department, and the Division of Endocrinology, was established. This committee conducted a needs assessment, defined mutual goals, created the scope of work, and established a timeline. Several educational events for the broader clinical community were hosted to provide visibility to the project and create opportunities for additional feedback.
Needs assessment
Two meetings were convened to understand the current clinical workflows around CGM data in the T1D clinic. The main goals were to map the entire process, identify pain points, and seek out opportunities for optimization. The first meeting was targeted at clinical endocrinologists and the second was targeted at medical assistants, nurses, and administrative staff. Clinic process flows and meeting summaries were developed and then presented back to the groups for verification of accuracy.
New architecture development
Once the process was understood, representatives from Departments of Endocrinology and IT, Dexcom, and the Center for Innovation held an ideation session to propose how the process might be different if CGM data were integrated into the medical record. The group also defined what type of data they would want to see in the EHR. Once the ideal process was defined, the technical teams worked together to propose an architecture that would enable that process. To manage the secure exchange of data between Dexcom and CHLA, an integration engine (Redox, Madison, WI) was put in place to standardize and normalize the data from both partners.
Governance and approvals
Because this project involved the exchange of protected health information (PHI) between a third party and our institution, it required several layers of review and approvals. The original proposal was presented to and approved by the Data Governance Task Force, which reviews all projects where patient data are shared outside our institution. With their approval, the Information Security and Architecture Review Board performed an in-depth review of the technical proposal. With the final technical architecture in place and all data elements defined, Legal and Compliance reviewed the contract governing the partnership between Dexcom and CHLA. Redox was required to complete an extensive information security assessment to verify that their data exchange platform was compliant. All EHR modifications required review and approval by the Change Control Review Board before implementation.
Dexcom CGM and Clarity
Clarity is Dexcom's HIPAA-compliant (Health Insurance Portability and Accountability Act), cloud-based, CGM data storage and visualization platform. Patients can upload their own CGM data to individual Clarity accounts by either episodically connecting their receiver to a computer or automatically from a mobile application running on a connected smart device. Clarity also allows patients to grant access to their CGM data to specific health care providers. Provider accounts within Clarity allow clinicians to view data from patients who have granted them access. Clarity allows physicians to generate eight different reports in increments of 7–90 days.
At the time of this project, there were two Dexcom CGM models compatible with Clarity: the G4 Platinum and the G5 CGM system. 13,14 In both devices, the patient wears an interstitial glucose sensor that is connected to a transmitter. The transmitter then sends data either to a receiver or wirelessly through Bluetooth to a Dexcom mobile application installed on a smart device. Dexcom mobile applications allow the patients to view and share their CGM data with family members and health care providers. 15
Results
Needs assessment and current state definition
Our needs assessment resulted in a comprehensive map of the current CGM clinical workflow at our institution (Fig. 1).

Five-step historical workflow for CGM data review during clinic appointments at Children's Hospital Los Angeles. CGM, continuous glucose monitoring; EHR, electronic health record.
Briefly, when a patient arrives at the clinic and checks in for the diabetes appointment, a clinic staff member (registered nurse or medical assistant) logs in to Clarity. If recent data are available, the staff member prints out all eight Clarity reports of the most recent 14–30 days of data and hands them to the provider. If the patient has not been uploading their data to Clarity, the staff member will take the patient's receiver (all patients are instructed to bring their receivers to the clinic as backup), connect it to a clinic computer, upload the patient's data to generate the report, and then hand it to the provider. The provider reviews the paper report, initials it, reviews the results with the patient during the visit, and then keeps the report until she is done writing her note for the day. Once all documentation is complete, the provider returns the report to the front office staff to have it scanned into the medical record.
Our clinicians and staff identified multiple inefficiencies in the existing system, including the time required by clinical staff to access Clarity and generate reports, the use of static paper reports, the need for clinicians to log into the system again if they want to review additional data, the time lag between the day of the appointment and the availability of the scanned report, and the fact that reports can get lost and never make it into the EHR.
Ideal state definition and architecture design
Our core group of clinicians met and provided the following requirements for any minimum viable product: Minimize the number of systems/platforms needed to be accessed by staff and providers. Work within existing systems. Clinicians should be able to access data at any time. No paper reports. Minimize workload on front office staff.
From a technical aspect, it became clear that the process needed to be divided into two discrete tasks: linking EHR and CGM data and requesting and viewing CGM data.
Each of these tasks generated unique concerns. For data linkage, it would be necessary to develop a mechanism for Dexcom to obtain consent from the patient to share their Clarity data directly with our institution. In terms of CGM data, the prospect of ingesting up to 4032 individual data points representing 14 days before each clinic visit was deemed out of scope for this project. Alternative methods for receiving, storing, and visualizing that amount of data inside the EHR would need to be developed. The proposed solution was to develop a custom Clarity report designed by our clinicians that could be requested at any time directly through the EHR. The custom report was a combination of the eight available Clarity reports, including the ambulatory glucose profile 16 –18 representing data from the most recent 14 days (Fig. 2 and Supplementary Fig. S1). The details of the Clarity reports have been listed in Supplementary Data—Clarity report description. The manufacturer also has several online resources to help clinicians understand and interpret the Clarity reports. 19
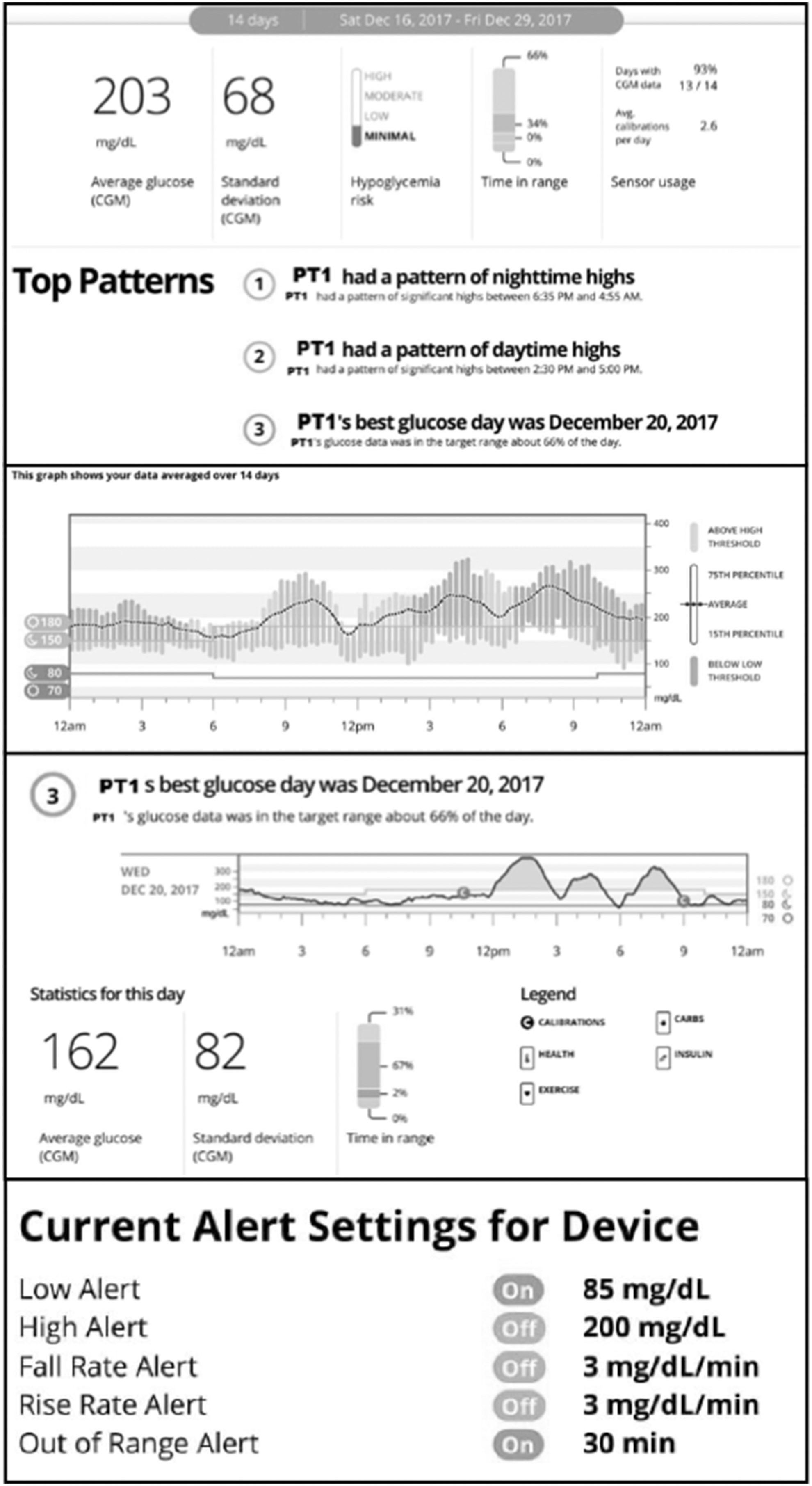
Composite of sample sections of the Clarity report available in electronic health records.
Based on user requirements, and previously mentioned concerns, the technical teams proposed use of the computerized, physician order entry (CPOE) module of our institution's Cerner EHR as the main tool for both tasks. A staff member could enter an order to link accounts, which generates a request for the family to give consent to access their data. Once access is granted, a second order for CGM reports can be entered as often as necessary.
Account linkage
We developed a CPOE order that generated an account linkage request, delivered to Dexcom as a Health Level 7 (HL7) ORU (Observation Result) message through a third-party integration engine (Redox, Madison, WI). Once the request is received, Dexcom sent a HIPAA authorization request for account linkage to the patient (or their guardian, as applicable) through email. For added security, this request expires after 30 days. Depending on the status of the consent, Dexcom generates a variety of update messages to the clinician, including “Request received,” “Authorization requested,” “Authorization granted,” “Authorization denied,” and “Request expired, please resubmit.” These messages are sent to our institution through the HL7 Medical Document Management (MDM) interface (Fig. 3). Once the patient has consented to data sharing, clinicians are able to request data.
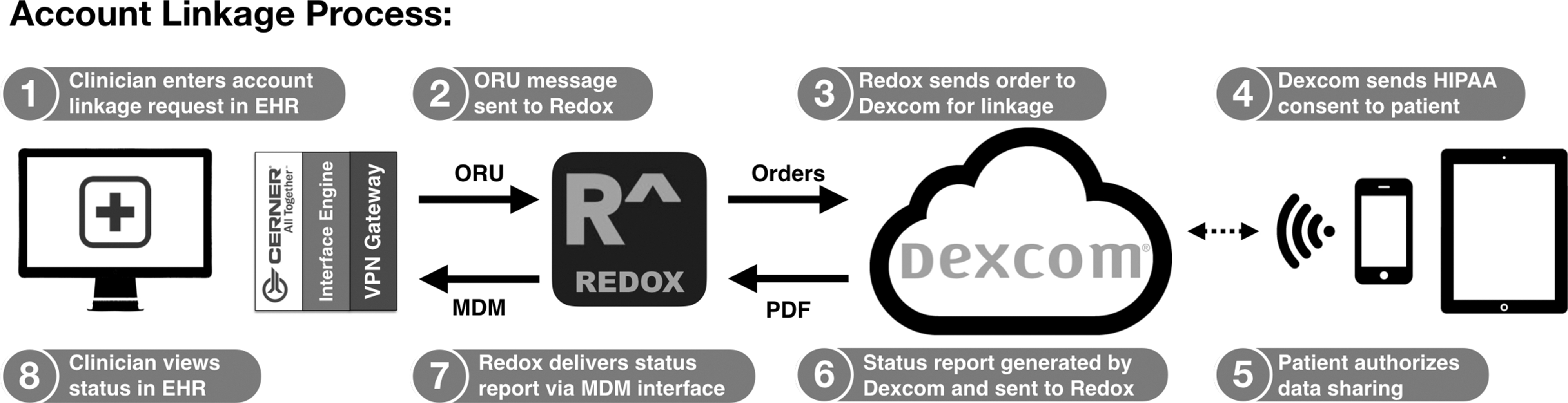
Eight-step workflow for linking Clarity accounts with the EHRs; ORU, HIPAA, MDM, PDF. EHR, electronic health record; HIPAA, Health Insurance Portability and Accountability Act; MDM, medical document management; ORU, observation result; PDF, portable document format.
Data request
A second CPOE order that generates a CGM data request was developed, which is delivered to Dexcom as an HL7 ORU message through Redox (Fig. 4). The data request order cannot be placed until consent has been received. The data request order triggers Dexcom to generate a Clarity report and deliver it as a PDF to our institution through the HL7 MDM interface. The report is then associated with the patient's Cerner account and is viewable by the clinician in the Results section of the EHR.
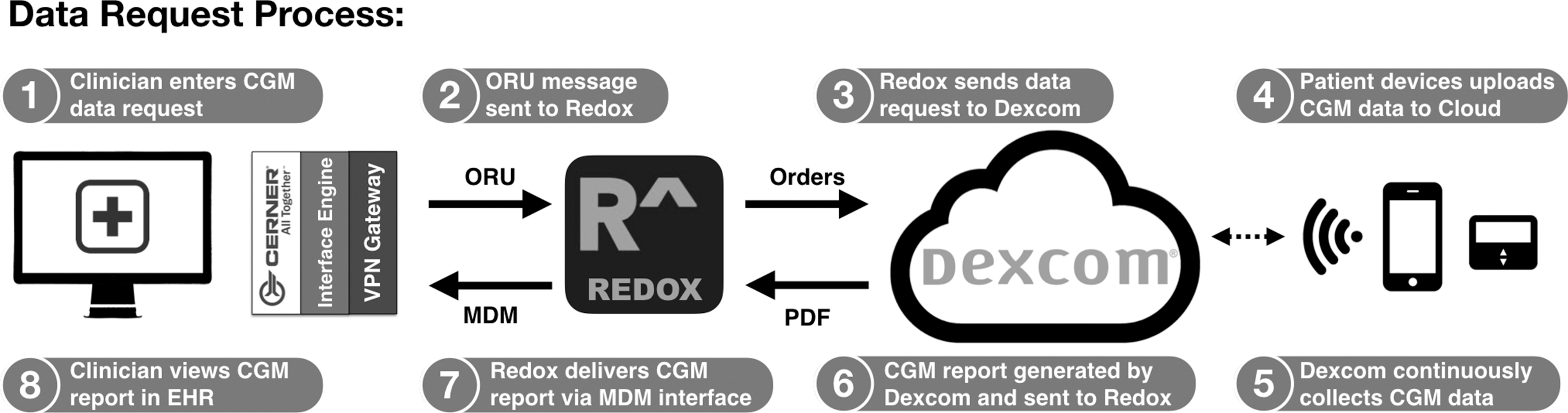
Eight-step workflow for managing EHR-based requests for CGM reports; ORU, MDM, PDF.
Implementation and workflow
Before going live, one provider (J.R.) tested the system with five patients to ensure proper connectivity at each step of both processes. Once all components of the system had been built out, tested, and placed into production environments, all staff in the Division of Endocrinology received a 1-h overview of the new process (Fig. 5), along with clinician training on new CPOE orders. Clinicians then began entering account linkage orders for their patients with Dexcom devices. In the first 2 months, 136 account linkages were requested, representing approximately one-third of eligible patients with Dexcom devices. One hundred five patients provided consent, the remaining 31 patients did not reply within 30 days, resulting in new consent orders being placed. No patients declined to provide consent. After the initial pilot period, a formal workflow was implemented: for all patients who receive a CGM device for the first time, the consent order is placed by the diabetes education team that teaches the patient and family how to use the CGM device. For existing patients with CGM, the consent order is placed by the provider at the next clinical encounter. Data request orders are placed by the clinical staff on the day of the patient appointment before the patient being seen by the provider so that the results are already in the EHR during the visit. Providers also place data request orders during phone and telehealth interactions with patients as needed.

Revised workflow for CGM data acquisition and in-clinic review; EHR.
Discussion
To our knowledge, this is the first collaboration of its kind. Before this project, no CGM device manufacturer in the United States had made patient device data available for ingestion directly into the EHR. Dexcom has previously partnered with other academic institutions to make their data more accessible to clinicians. In 2016, Kumar et al. 9 described their efforts to integrate CGM data into the Epic EHR (Epic, Verona, WI) using the Apple Health Kit (Apple, Cupertino, CA) and the Epic MyChart patient portal to allow patients to push CGM data into their chart. This straightforward approach used existing technology and required very little customization, making it an accessible solution to health systems that have similar systems in place. However, the Apple Health Kit does not interact with all EHRs and excludes patients who have Android and other devices. Furthermore, some institutions are still weary of partnerships with consumer data and technology companies such as Apple, Facebook, and Google. Alternatively, Wong et al. 12 described using third-party data aggregators such as Tidepool to collect and centralize data from multiple devices, including CGM devices, insulin pumps, glucometers, and commercially available smart devices such as fitness trackers and scales. Platforms such as Tidepool and Glooko make large amounts of data available, but do not integrate into the EHR by default, requiring a separate workflow. Both Tidepool and Glooko have developed application program interfaces for EHR integration, 20 –23 which can be powerful tools for patient management, but implementation still requires significant institutional buy-in, data use agreements, and internal IT resources.
There are several innovative aspects of this project. First, the nature of the collaboration between an academic center, a CGM device manufacturer, and a third-party integration engine to share PHI has not been previously described in the literature. Second, the technical architecture was developed to respond to a specific set of needs defined by clinical users. This type of user-centered design is common in user interface/user experience (UI/UX) work, but is less commonly reported for the more technical aspects of data exchange, where legal, compliance, and technical limitations tend to define what is possible. Third, we developed a workflow that does not require the clinician to access a second platform to review CGM data; it is now incorporated into their existing EHR workflow. Simplifying and streamlining workflows are critical aspects of modern health care systems, in which clinicians spend more than 50% of their time in the EHR. 24,25 Although not measured during this study, Mullen et al. demonstrated that optimizing diabetes device data protocols in clinical settings can result in significant time savings. 26 Finally, the use of HL7 standards was an important aspect of this project. Interoperability standards increase the likelihood of replication and dissemination and, as such, were a key consideration in the architecture design.
There are limitations to our approach, and we did not address all the inefficiencies of the original paper-based workflow. Currently, we only receive reports and not structured data, meaning it cannot be trended or visualized natively in the EHR. If providers want to explore data more granularly beyond what is available in the report, they still need to log in to Clarity. It also means that there is no mechanism to flag abnormal results, or provide normal ranges, beyond what is included in the report. The report itself contains 14 days of data, which is the commonly used interval by our clinicians, but there are situations in which a clinician may want to review a different time window, in which case they are required to go to Clarity. We are currently addressing this by building in a date feature into the order to allow the provider to request any range of data. The report is also limited by the fact that patient CGM data are not always uploaded regularly into Clarity. Therefore, while access to the Dexcom cloud is real time, it is limited by the user's data upload frequency. A related limitation is that the system pulls the most recent 14 days of data along with the dates, but there is no mechanism to notify the provider that the patient has not uploaded data recently (e.g., the only data in Clarity are from 2 months ago). The second limitation is that the data are pulled, rather than pushed, requiring a member of the clinical staff to initiate the request. This makes CGM data review an active process rather than a passive one like most other result reviews in the EHR. A third limitation is that our solution only addresses one manufacturer, replicating this process for the other manufacturers of CGM devices will require new agreements and, depending on their technical capacities, a different mechanism for data exchange. That being said Dexcom has begun several partnerships around the country to implement similar systems. Other CGM device manufacturers have already started working with our team to use the same mechanism for data exchange.
Finally, as the first project of its kind, this effort required a high level of institutional buy-in and commitment to obtain all the necessary approvals and have the relevant IT resources dedicated to this effort. Our hope is that by disseminating our results, making our data architecture diagrams public, and sharing Cerner Command Language (CCL) scripting, it will be much easier for other institutions to follow suit.
We estimated that this project generated ∼$40,000 work of billable hours from the various teams that participated. While that number may seem large, for perspective, it is less than a 0.5 FTE of an EHR analyst. No cost data were available from the other collaborators. We have not yet measured the impact of this new mechanism on clinic throughput, provider satisfaction, patient satisfaction, revenue cycle, or patient outcomes. One cost-related consideration is that incorporating CGM data directly into the EHR creates new opportunities for both meaningful use of the EHR 25 and charge capture. In the United States, 95,251 is the Current Procedural Terminology (CPT) code for the review and interpretation of at least 72 h of CGM data. 27 This code is covered by many public and private payers, can be billed once a month, and does not require a face-to-face encounter, facilitating adoption of financially viable, remote patient monitoring paradigms for diabetes. Providers can bill this code for reviewing patient data on the same day of either on-call or in-person visit (i.e., simultaneously with an evaluation and management code) or when the patient is not present (e.g., in response to a patient call to report any symptoms or complications, and the provider reviews CGM data to make decisions about the treatment plan). By incorporating CGM data in the EHR, it may be easier to generate the necessary documentation to bill for CPT 95251. For example, we are exploring adding a feature to the workflow that prompts the clinician to complete the documentation template necessary to describe the CGM data review, generate patient recommendations, and bill for CPT 95251. Providers should discuss the use of any new CPT code with their institutional revenue cycle management and compliance teams.
Next steps
We have identified several key next steps for our ongoing collaboration. First, we are adding an option for the physician to define the dates of the report in the data request order. This will allow clinicians to generate reports of different lengths (14, 30, and 90 days) and from any time frame. We are also actively working with all our partners to define a unified troubleshooting script and decision tree to provide support to our staff and clinicians who encounter difficulties with the system. Finally, we are exploring options for importing discrete CGM data into the EHR, as well as mechanisms to visualize them natively in the EHR, or with an EHR integrated software such as Tableau (Tableau, Seattle, WA).
Conclusions
Building scalable data integration using HL7 standards is possible and allows real-time access to CGM data within the diabetes provider's existing workflow. Better data access may lead to improved clinical outcomes, increased efficiency, and new revenue opportunities by documenting CGM data capture and review.
Footnotes
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Food and Drug Administration.
Poster Presentation
The study was presented at The Pediatric Academic Societies (PAS) Meeting in 2018. J.E. and J.R: Integrating Continuous Glucose Monitoring Data in the Electronic Medical Record: Proof of Concept. Presented at PAS, Toronto, Canada, April 26th–May 6th, 2018.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this article was supported by the Food and Drug Administration under award number P50FD006425 (PI: J.E.) for The West Coast Consortium for Technology & Innovation in Pediatrics.
Supplementary Material
Supplementary Data
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.