
Abstract
Background:
There is limited evidence supporting a replacement interval of infusion sets for continuous subcutaneous insulin infusion (CSII). The aim of this study was to investigate if steel and soft cannula infusion sets can be used in CSII therapy for up to 7 days without negative impact on infusion sites or glycemic control.
Methods:
The insulin infusion sets YpsoPump® Orbit®micro (steel needle) and YpsoPump® Orbit®soft (soft cannula) were each used for up to 7 days by 40 adult subjects with CSII. Each subject used both infusion set types twice. Early replacement reasons were documented and glycemic control was monitored.
Results:
Of 160 inserted insulin infusion sets, 66% were used for 7 days with no obvious difference between steel and soft infusion sets. The mean wearing time was 6.2 ± 1.5 days. Main reasons for early infusion set replacements were occlusions (19%), plaster issues (4%), and accidental pull-out (4%). Comparing glycemic control during day 1–3 and 1–7, mean glucose was 146 ± 21 mg/dL versus 148 ± 18 mg/dL, coefficient of variation was 34% ± 7% versus 33% ± 5%, and insulin dose was 40 ± 11 U versus 41 ± 11 U. Only mild and nonserious infusion site reactions occurred.
Conclusions:
In this study, 7 days indwelling time of insulin infusion sets did not show a clinically relevant impact on glycemic control or insulin requirements and the infectious risk appeared to be low. The replacement interval of infusion sets may be individualized beyond the currently labeled maximum use duration.
Introduction
For patients with type 1 diabetes, continuous subcutaneous insulin infusion (CSII) is a common therapy and represents a concept that is closer to the physiological insulin delivery pattern in healthy people than multiple daily injections. 1 Consequently, CSII has been shown to enable a better glycemic control. 2 However, in addition to an insulin pump, an infusion set, including tubing and a catheter, is required to infuse insulin into the subcutaneous tissue. Infusion sets are commonly regarded as the weak point of insulin pumps and the major counterargument against CSII. 3,4 It is generally recommended to change the infusion set no later than after 2–3 days. The rationale, however, is not to be found in well-designed clinical studies, but rather based on individual case reports, and this recommendation has not been updated since first established in the 1980s. 5,6
Nowadays, especially with regard to the development of closed loop systems, it seems desirable to extend the maximal wearing time. 7 This would not only mean less expenditure of time for users but also less waste and disposal of insulin that remains within the tubing.
Reasons that necessitate an infusion set change are an insufficient delivery or action of insulin, or signs of inflammation at the infusion site, or a subsiding sticking of the plaster. While the status of the latter two is usually obvious to the user, an insufficient insulin delivery might not be noticed immediately. There are different factors that can impede insulin delivery. An occlusion within the tubing or at the catheter tip, which might be caused, for example, by kinking of the cannula or precipitation of insulin, can partially or completely block delivery. In this case, the pump notices the rising pressure within the system and gives an alarm after a certain time. 8 In case of leakage within the system, no alarm will be prompted.
Furthermore, the action of insulin might be impaired by tissue changes due to lipohypertrophy or inflammatory processes. All these events will lead to an insufficient insulin availability and subsequent hyperglycemia. If not counteracted, ketosis and eventually diabetic ketoacidosis, which represents an acute and severe metabolic emergency, may develop. Therefore, it is important that pump users are aware of this risk and know how to handle hyperglycemia. In this context, regular glucose monitoring, either by blood glucose (BG) measurements or continuous glucose monitoring (CGM), is essential.
Unexpected high glucose values that cannot be lowered by applying correction boluses indicate insufficient insulin delivery. In addition, measurement of blood or urine ketones gives information about the current metabolic state and presence of ketones indicates a lack of insulin. If detected early, replacement of the infusion set usually leads to a fast improvement.
Previous studies reported an increase in the risk of infusion site infection, occlusions, and other infusion set issues when using them longer than the recommended 2–3 days. 3,9 –12 However, there are also more recent studies that showed feasibility of a 7-day indwelling time at least in some patients. 13,14
The aim of this study was to investigate whether two infusion sets with either steel or soft cannula can be used for CSII therapy for up to 7 days.
Methods
This was an interventional, open-label, randomized crossover study. The study was performed between October 2018 and February 2019 at the Institut für Diabetes-Technologie, Forschungs- und Entwicklungsgesellschaft mbH an der Universität Ulm, Germany, study sponsor was Ypsomed AG, Burgdorf, Switzerland. The study protocol was approved by the responsible Ethics Committee and the German health authority. The study was registered at
Protocols of similar studies with the same focus that provided well-designed methods were taken into account during the design of the study; many of their procedures and outcome measures were adopted. 13,14
Participants
Adult subjects with type 1 diabetes using CSII for at least 12 months and an HbA1c ≤8.5% were eligible for the study. Exclusion criteria were diabetic ketoacidosis or severe hypoglycemia in the past 3 months; urea, creatinine, alanin-aminotransferase more than three times the upper limit of normal, or thrombocytopenia; pregnancy or lactation period; known severe tape reactions or allergies; known severe nickel allergy; history of frequent catheter abscesses; and serious acute or chronic disease besides diabetes mellitus or an anamnesis that might, in the opinion of the investigator, pose a risk to the subject. All subjects signed informed consent before any study procedures and were included after a screening visit if they fulfilled the eligibility criteria.
After screening, 41 subjects were included in the study. One subject dropped out during the familiarization phase. The subject presented with infusion site inflammation, did not agree to postpone randomization and therefore was discontinued. A total of 40 subjects were randomized to 7-day use of the infusion sets. Of the randomized subjects, 24 were female and 16 were males. The mean age was 49.2 ± 12.5 years and they had diabetes for 26.6 ± 12.8 years with 12.3 ± 7.6 years of CSII therapy. The HbA1c was 7.3% ± 0.7% and the total daily insulin dose 42.3 ± 11.7 U/day. Most subjects (75%) used a soft cannula in their previous therapy and they reported to change the infusion set every 2.8 ± 0.8 days.
Study devices
The two insulin infusion sets YpsoPump® Orbit®micro (steel needle) and YpsoPump® Orbit®soft (soft cannula) (Ypsomed AG, Burgdorf, Switzerland) were used with the mylife™ YpsoPump (Ypsomed AG) and prefilled NovoRapid® PumpCart® cartridges (insulin aspart) (Novo Nordisk A/S, Bagsvaerd, Denmark). Subjects could choose from different catheter lengths (5.5 or 8.5 mm for steel needle and 6 or 9 mm soft cannula) and tubing lengths (60 or 80 cm) and use their preferred infusion sites. An insertion device (Orbit®Inserter, Ypsomed AG) suitable for both infusion sets could be used optionally.
The Dexcom G5™ Mobile system (Dexcom, Inc., San Diego, CA) was used for CGM and the FreeStyle Precision Neo BG and ketone measurement system (Abbott) was used for regular BG and ketone measurements and to calibrate the CGM system. The glucose test strip batch that was used in the study was tested for accuracy in advance using a reduced scale protocol based on ISO 15197:2013, clause 6.3. 15 Accuracy of the used batch was considered adequate with 99% of values within ±15 mg/dL or ±15% of the laboratory comparison method at glucose concentrations <100 or ≥100 mg/dL, respectively.
Procedures
After inclusion, subjects were trained on all study devices and then used them during a familiarization phase of 2–4 weeks to get accustomed to handling of the YpsoPump system and insulin aspart and to be able to adequately calibrate the CGM system and handle CGM data. During this phase, patients were advised to use both infusion set types with equal frequency and to replace them after 2–3 days.
Following the familiarization phase, subjects were randomized to one of two groups that determined the order of infusion set use. Group A started with the steel infusion set and group B started with the soft cannula infusion set. Each infusion set was tested twice in succession. For the following 4 weeks, infusion sets were worn for up to 7 days each while subjects visited the study site weekly (Fig. 1).

Study design.
During visits, infusion sets and CGM sensors were inserted by the subjects under supervision of trained study personnel after site disinfection. Infusion set function was confirmed by monitoring BG levels over the following 2–3 h. Additional fixation of the infusion set was allowed if subjects usually did so. Infusion sets could be replaced if insertion errors were noticed during the first 2–3 h. Subjects then left the study site and tried to wear the infusion set for up to 7 days under daily-life conditions with their usual therapy regimen.
They were allowed to change the infusion set earlier if either an occlusion, or infusion site issues, or adhesive issues occurred that conflicted with further indwelling. An occlusion was defined as either a BG concentration >250 mg/dL for more than 2 h with a failed correction bolus (failure to lower BG by at least 50 mg/dL within 60–90 min), or a blood ketone concentration ≥0.6 mmol/L, or a pump occlusion alarm that could not be solved. Subjects were instructed to measure their BG at least four times a day. In case they noticed a BG >250 mg/dL for more than 2 h, they should measure blood ketone concentration and give a correction bolus. If ketones were positive or the correction bolus failed, an occlusion was suspected and subjects were advised to change the infusion set. In addition, if an occlusion alarm of the pump occurred, subjects were advised to first disconnect the tubing from the catheter and then flush the tubing by giving a bolus. If the occlusion alarm could not be solved, an infusion set change was indicated.
Early infusion set replacements were documented by the subjects by selecting from a list of reasons or describing other reasons. After 7 days, all infusion sets were removed. On the next study site visit, insertion sites were checked, study documentation was reviewed, device data were downloaded and the next infusion set was placed. Occlusions were not supposed to be verified by technical investigations, but for soft catheters, subjects were asked to perform a visual check for kinking after removal. Early replacements due to a suspected occlusion were reviewed by the investigator based on device data and subject documentation and recoded if necessary to achieve a standardized application of the three predefined occlusion criteria. If none of the predefined criteria could be verified, the event was considered an unconfirmed occlusion.
Statistical analysis
The objective of the study was to assess whether the two tested infusion sets can be used for CSII therapy for up to 7 days. It was planned to include 40 subjects to have sufficient data also to evaluate glycemic control over 7-day indwelling when using each type of infusion set two times. Data from the two types of infusion sets and from the two randomization groups were pooled because data were similar between the two types. For each of the inserted infusion sets, indwelling time and, if applicable, reasons for early changes were evaluated.
For infusion sets that were used for the whole 7 days, mean glucose values, coefficient of variation (CV) of glucose values, time in the glucose range of 70–180 mg/dL, and daily insulin doses were calculated for each day after insertion. To evaluate the impact of prolonged indwelling on glycemic control, Spearman correlation was performed. Analysis of variance was used to determine the influence of the individual subject and of the type of infusion set on wearing time. The influence of other factors such as HbA1c or diabetes duration on wearing time was also evaluated using Spearman correlation. Results are presented as number and percentage of infusion sets or mean ± standard deviation.
Results
All of the 40 randomized subjects completed the study as intended; therefore, in total 160 infusion sets (80 steel and 80 soft catheters) were evaluated. Two infusion sets were replaced right after insertion due to insufficient plaster adhesion and not included in the evaluation. The most commonly chosen insertion site was the abdomen (80%) followed by hips (20%) and the insertion device was used in 93% of all insertions.
Of the 160 infusion sets, 105 (66%) were used for the whole 7 days with no significant difference between the steel infusion set (69%) and the soft cannula infusion set (63%) (Fig. 2). After successful insertion, no initial failures within the first 2–3 h were observed. In total, 94% of infusion sets were used for at least 3 days and 82% for at least 5 days. The wearing time averaged 6.2 ± 1.5 days and ranged from 0.8 to 7 days with 97.5% of subjects showing a mean wearing time of 4 days or more. While 10 subjects could use all four infusion sets for the whole 7 days, 1 subject replaced all infusion sets before day 5 due to suspected occlusion (Fig. 3). A significant influence (P = 0.042) of the individual subject on wearing time was found and that can be attributed to this single subject. There was no correlation between wearing time and diabetes duration, CSII duration, insulin demand, or HbA1c.
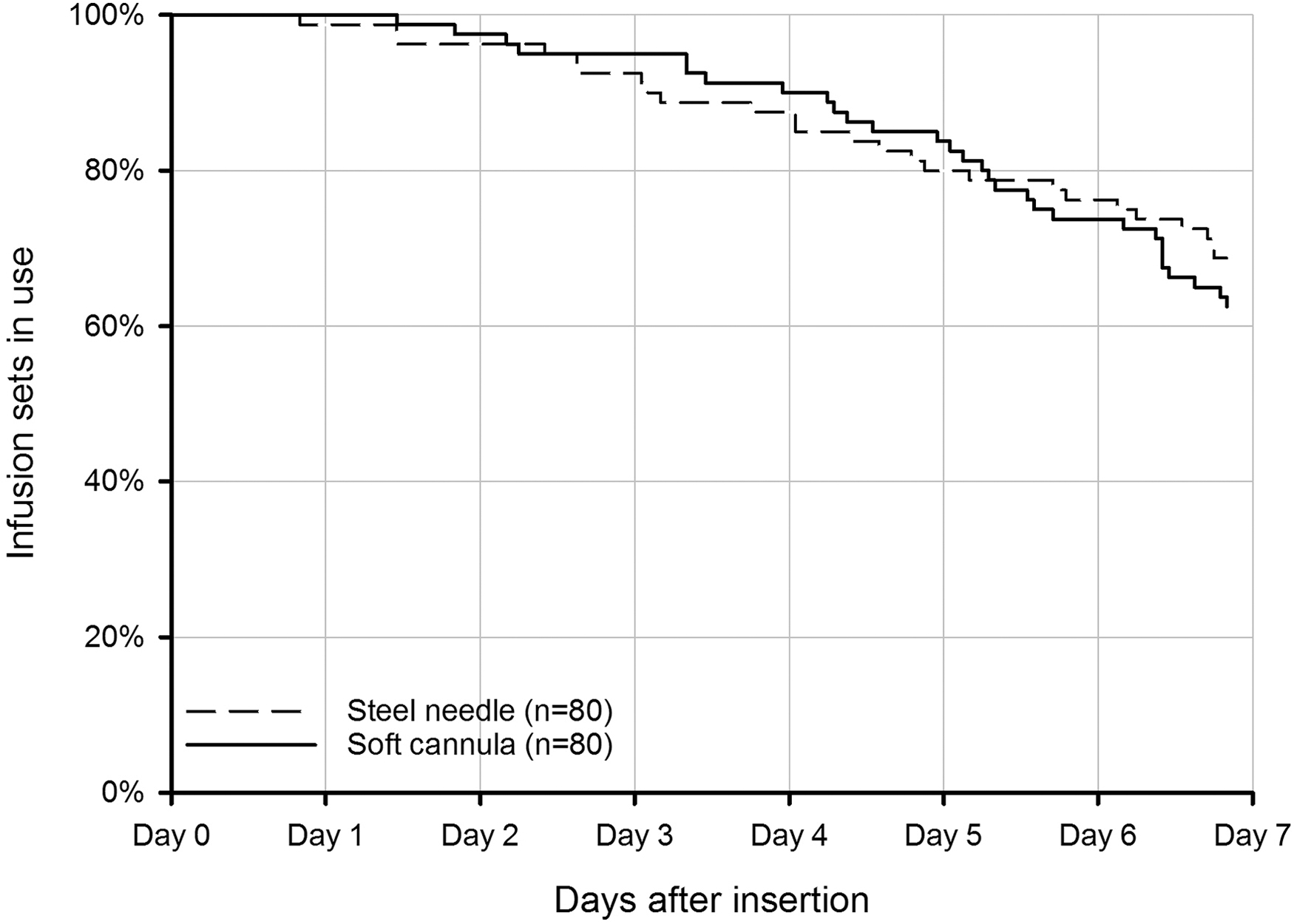
Survival curves for steel needle and soft cannula infusion sets (n = 80 infusion sets each), any early replacement reason.
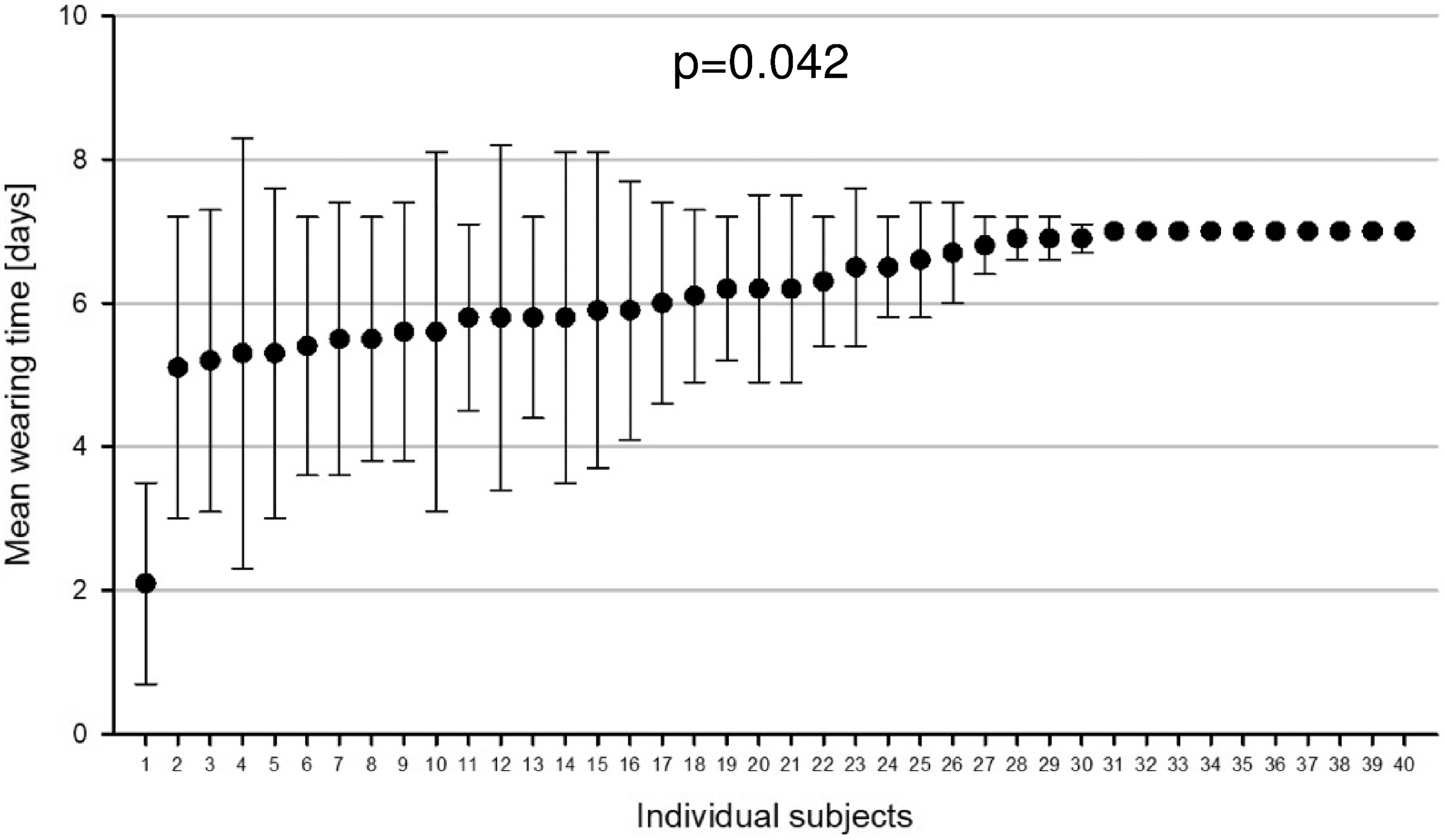
Mean wearing time of four infusion sets per subject. Subjects are arranged by increasing mean wearing time. Antennae show stand deviations.
The main reason for early infusion set replacements were suspected occlusions (n = 30, 19% of infusion sets), characterized by either unexplained hyperglycemia (n = 5) or blood ketones ≥0.6 mmol/L (n = 4) or a pump occlusion alarm (n = 14). For seven further infusion sets, subjects reported an occlusion that could not be confirmed. Occlusions characterized by the predefined criteria occurred in 11 steel (14%) and 12 soft cannula (15%) infusion sets; no kinked cannulas were observed by the study participants during visual examination of the removed infusion set. Other early replacements reasons were, for example, plaster unsticking or rupture (n = 7, 4%), accidental pull-out (n = 6, 4%), blood in the tubing (n = 4, 3%), leakage (n = 3, 2%), and discomfort (n = 3, 2%) (Table 1). No infusion site infection occurred while testing for 7-day indwelling.
Patient-Reported Reasons for Early Infusion Set Replacement
Daily glucose levels were evaluated for infusion sets that were used for the whole 7 days. Mean glucose (Fig. 4A and Supplementary Fig. S1) as well as glycemic variability (Fig. 4B and Supplementary Fig. S1) and time in range (70–180 mg/dL, Table 2) did not show a substantial change over the indwelling time. Mean glucose during the first 3 days was 146 ± 21 and 148 ± 18 mg/dL when considering the whole 7 days of wearing. At the same time, CV was 34% ± 7% versus 33% ± 5%. Mean daily insulin doses over 7-days use were 41 ± 11 U and therefore similar to the demand during the first 3 days (40 ± 11 U) (Fig. 4C and Supplementary Fig. S1). There was no significant correlation between day of wear and mean glucose and daily insulin dose. Glycemic variability seemed to decline over wearing time and time below range tended to decrease (Table 2).
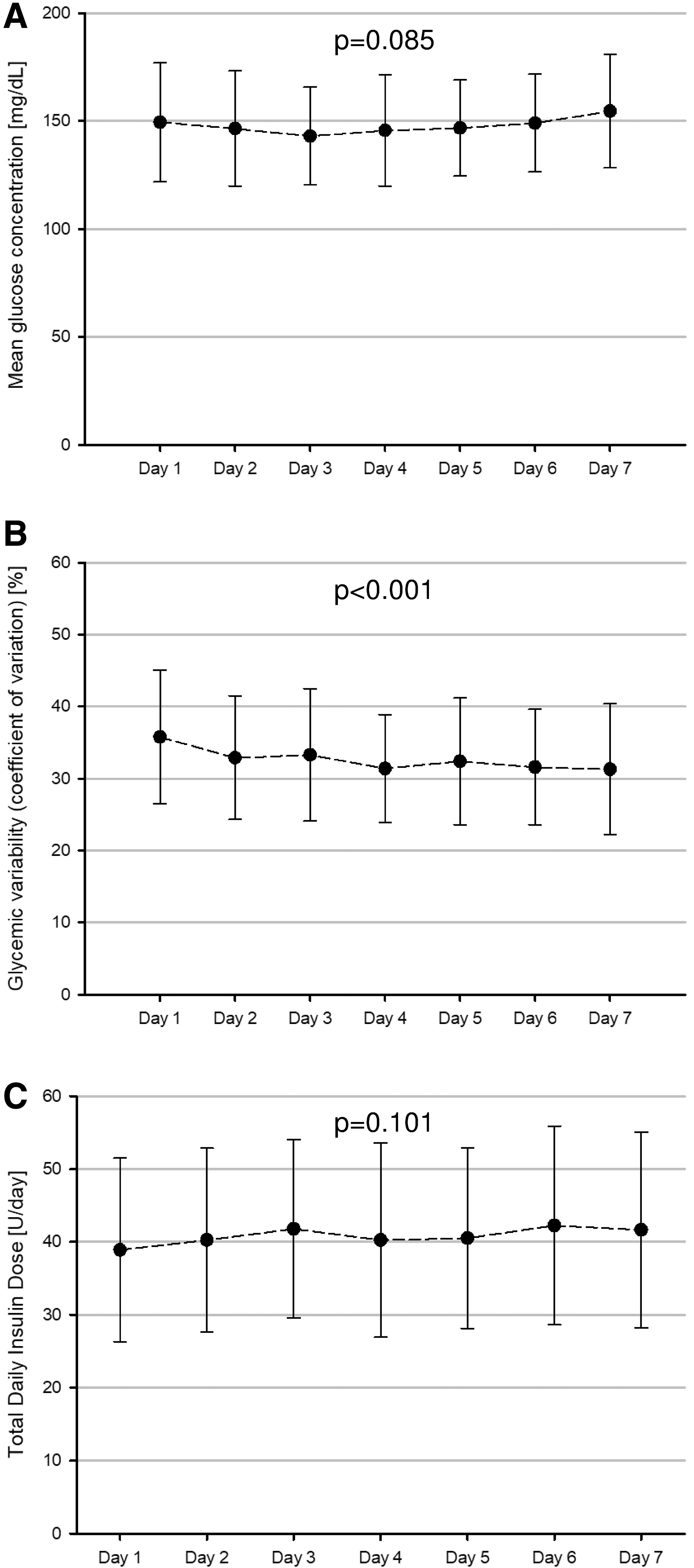
Glycemic control during 7 days use (early replaced infusion sets not included). Data are pooled for both types of infusion sets (n = 105).
Time Spent in Different Glucose Ranges During 7 Days Use (Early Replaced Infusion Sets Not Included)
Data are pooled for both types of infusion sets (n = 105).
One infusion set was replaced because of infusion site discomfort and mild swelling. Other infusion site reactions were limited to mild erythema and only detectable after infusion set removal (n = 16 at the cannula insertion site, n = 4 at the plaster application area). No difference regarding skin reactions was observed between the steel and the soft cannula infusion set. All adverse device effects were nonserious and mild, and resolved without treatment.
Discussion
This study investigated the prolonged indwelling of insulin infusion sets for up to 7 days in experienced CSII patients. The main focuses were to assess (1) the occurrence of occlusions and other infusion set failures or site reactions over 7 days and (2) whether there is any impact of using insulin infusion sets beyond the currently labeled maximum use duration on glycemic control. Regarding the first issue, it was assumed that the main factor limiting appropriate insulin delivery is an occlusion. If not noticed early, insufficient insulin supply leads to elevation of glucose levels. Suspected occlusions occurred in 30 infusion sets and thus were the main reason for early infusion set replacements. For none of the occlusions, subjects reported kinking. No adverse events were associated with occlusion events. The rate of occlusions of 19% was rather low compared to rates of 23%–35% or 30% reported from other studies with prolonged wear time. 13,14 In a previous home use study, including the soft cannula infusion set tested in this study, an occlusion rate of 14% was reported for regular 3 day infusion set use. 16
The strongest reservation concerning prolonged indwelling is glycemic control, because some studies have reported a loss in glycemic control due to a decrease of insulin action. 9,10,14 Clausen et al. studied the effect of Teflon catheter insertion on insulin absorption for 4 days. 17 Insertion leads to tissue trauma, an increase in blood flow, and therefore also an increased speed of insulin absorption within the first 2 days and then returns to baseline. However, there was no effect on peak plasma concentration. In a similar setting, this could not be reproduced with a steel catheter. 18
The present study has the advantage of providing a large dataset of glucose data that allow an evaluation of glycemic control. In subjects who used the infusion set for 7 days, glycemic control was stable as measured by mean glucose, glycemic variability, and time in range variables. Apparent improvements in glycemic variability and time below range are likely to be attributed to CGM performance. It is known that CGM systems are less precise on the first day of wearing, which always was also the first day on infusion set wear in this study. At the same time insulin demand was largely unchanged, at least under consideration of usual day-to-day variations, which means that insulin action was not impaired by prolonged indwelling.
The high 7-day wearing rate of 66% was likely supported by the absence of initial failures during the first hours after insertion except for the two cases of adhesive failures. Reasons might be device properties or study procedures. Other studies report initial failure rates of 9%–15% with kinking of the Teflon catheter as the most common reason. 13,19 Rates of premature infusion set replacements of up to 20% were reported for different infusion sets during regular use. 19,20
No significant differences between the steel and the soft cannula infusion set were observed in this study, neither regarding performance over 7 days nor regarding adverse events. Failure curves were also very similar. Patel et al. also compared steel and Teflon infusion sets in 20 subjects regarding their performance over 7 days, but in a less experienced subject group with slightly poorer glycemic control. 13 They did not observe much difference in the failure rate between the infusion sets as well, but only one-third was used for 7 days. This included an initial failure rate of 15% in Teflon catheters due to kinking. The reported rate of occlusions, or more specifically hyperglycemia with failed correction dose, was 30% and thus twice the rate observed in the present study. They also reported more cases of infection and pain at the infusion site. However, mean glucose and total daily insulin also remained stable over 7 days.
Karlin et al. investigated the effect of lipohypertrophy on infusion set failure in 20 subjects also with an observation time of 7 days. 14 They did not find any influence of lipohypertrophy on infusion set failure and showed a mean wearing time of ∼4 days with 33%–42% 7-day use. Prolonged indwelling time was associated with an increase in mean glucose levels. Similarly, Thethi et al. reported significant increases in mean glucose and total daily insulin dose from day 2 to 5. 9
Schmid et al. and the successor study by Pfützner et al. reported an increased prevalence of infusion site issues after 2–3 days in 12 subjects and 24 subjects, respectively. 10,12 However, the design of these studies did not allow investigating, at which time point an infusion set change was actually indicated. In addition, Schmid et al. observed increasing BG levels with increasing wearing time but as described, the number of cases for longer wearing time was quite low.
In the present study, no infusion site infections occurred during prolonged use and only one infusion set was changed due to discomfort. The low complication rate might be due to thorough preparation of the infusion site, including skin disinfection, but also due to the enrollment of highly motivated and experienced subject. Overall, the skin reactions observed during extended wear were comparable to those observed during regular use and did not require any additional interventions. Tolerance of the cannula and plaster of both infusion sets was thus not impaired by 7-day wear.
Although the wearing time was dependent on the individual subject to some degree, nearly 75% of subjects wore at least one, but not all, of the infusion sets for 7 days. Statistical significance was reached, but this could be attributed to one subject having relatively short wearing times in all infusion sets. Patient-specific factors could not be identified.
This study has some limitations, like the selection of subjects. Subjects that are prone to skin reactions or had a history of catheter abscesses were not included in the study, and all participants were experienced in CSII and familiarized with the used devices. Infusion set application was performed by the subjects themselves, but under supervision and strictly following the instructions for use, including disinfection, thus representing only best case circumstances that may not always be reproducible in daily life. In addition, extra fixation of the adhesive was allowed and was frequently made use of. Therefore, conclusions regarding an average wearing time of the infusion sets without extra fixation are limited. Under certain conditions, such as physical activity or high temperatures or suboptimal initial fixation of the infusion set, decreasing adhesion might terminate wearing time even if insulin delivery and tolerance are still adequate. Another limitation is the use of only one type of insulin because literature indicates that higher occlusion rates might be associated with other insulin analogs. 3,11
This study did not investigate long-term effects of a prolonged indwelling time, including impact on lipohypertrophy and tissue scarring. It is known that both tissue trauma after injection and the lipogenic action of insulin can cause lipohypertrophy. 21 To avoid lipohypertrophy, patients are usually advised to change the infusion site with every infusion set removal. An extended indwelling time of infusion sets does result in fewer needle sticks, but longer insulin action at the same site. In the present study, no signs of lipohypertrophy were observed at the sites where infusion sets were used longer than the recommended time; however, study duration was too short to investigate potential long-term effects. In addition, longer study duration would allow evaluating an impact on HbA1c as well as hypo- and hyperglycemic events.
In conclusion, wearing of insulin infusion sets for up to 7 days may be an individualized option for subjects, who are experienced and well trained in proper infusion set insertion and handling and who regularly monitor glucose levels and know how to respond to hyperglycemia. From a clinical perspective, the currently labeled maximum use duration of insulin infusion sets may be prolonged, but users should replace infusion sets in case of suspected occlusions, plaster unsticking, or infectious signs independent from actual indwelling time.
Footnotes
Acknowledgments
The authors thank the study personnel and all volunteers who participated in that study.
Author Disclosure Statement
G.F. is general manager of the IDT (Institut für Diabetes-Technologie Forschungs- und Entwicklungsgesellschaft mbH an der Universität Ulm, Ulm, Germany), which carries out clinical studies on the evaluation of BG meters and medical devices for diabetes therapy on its own initiative and on behalf of various companies. G.F./IDT have received speakers' honoraria or consulting fees from Abbott, Ascensia, Dexcom, LifeScan, Menarini Diagnostics, Metronom Health, Novo Nordisk, Roche, Sanofi, Sensile and Ypsomed. D.W., E.Z., S.P., and C.H. are employees of the IDT. A.B. is employee of Ypsomed AG, Switzerland.
Funding Information
The study and scientific writing were funded by Ypsomed AG, Switzerland.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.