
Abstract
Although insulin delivery devices are widely used by the patients, there is a paucity of published guidelines to help professionals manage their patients in insulin therapies. To provide simple and easily implementable guidelines to health care physicians on the choice of insulin delivery devices in routine clinical practice, experts in diabetes gathered together and discussed the recommendations at the National insulin Summit 2018. An ideal insulin delivery device should accurately deliver the prescribed dose of insulin and be easy to use. Recommendations are: (1) insulin should be initiated by using an insulin device if the patient seems to discontinue insulin therapy. (2) Pen devices offer accurate dosing than a syringe and vial and are associated with cost savings in the long term. (3) Switching over from syringes and vial to disposable pen devices improves adherence. (4) FlexPen® offers better accuracy, and it requires lower dose force and injection force than SoloStar® and KwikPen® (5). Durable delivery pens such as NovoPen® 4 maintain accuracy and low dose force compared with vials and syringes. (6) One pen should be used by only one patient. (7) Regular counseling on the proper use of the pen device is required regularly. This consensus-based recommendation is a useful reference tool for health care practitioners to initiate insulin therapy in patients with diabetes by using the appropriate insulin pen device.
Introduction
Diabetes mellitus is a worldwide epidemic disease. Management of diabetes demands a safe convenient and economic therapy. The goals of diabetes therapy are to ensure effective glycaemic control with low risk of hypoglycemia in the short term and to prevent chronic complications in the long term. One of the greatest medical breakthroughs of all time was the discovery of insulin by Frederick Banting and Charles Best in 1921–22. 1 With the introduction of insulin, a significant improvement was seen and patients were able to achieve better glycemic control.
However, both patients and physicians may be reluctant to initiate insulin therapy due to pain associated with insulin injections using vial and syringes and other factors. 2 Insulin injection using a syringe is time-consuming, cumbersome, inconvenient, and painful. It is also associated with a high risk of dosage errors. 3 In addition, adherence to insulin therapy is low because of drawbacks associated with insulin injections using syringes. 4
To overcome the disadvantages of insulin injection, insulin pen devices were developed to improve the patient's convenience and ease of use. 3 They have several benefits over the traditional vial-and-syringe method of insulin delivery such as less pain, improved compliance, and better glycemic control, which lead to improved patient outcomes. 5,6
Materials and Methods
An expert panel consisting of endocrinologists met to develop consensus on choice of insulin delivery devices in routine clinical practices in insulin-treated patients with diabetes in the Indian setting. The panel analyzed published data (Table 1) and real-world evidences, and it provided recommendations. The final proposed consensus-based recommendations were collectively recorded in easily implementable steps, without any bias and in an as much possible unambiguous language. The proposed consensus planned to provide practical guidance for physicians and general practitioners in India in terms of (1) choice of the right insulin delivery device, (2) choice of the right disposable device, (3) choice of the right durable device, and (4) practical considerations while using an insulin delivery device (Fig. 1). Among insulin delivery devices, consensus was generated for insulin pens only.
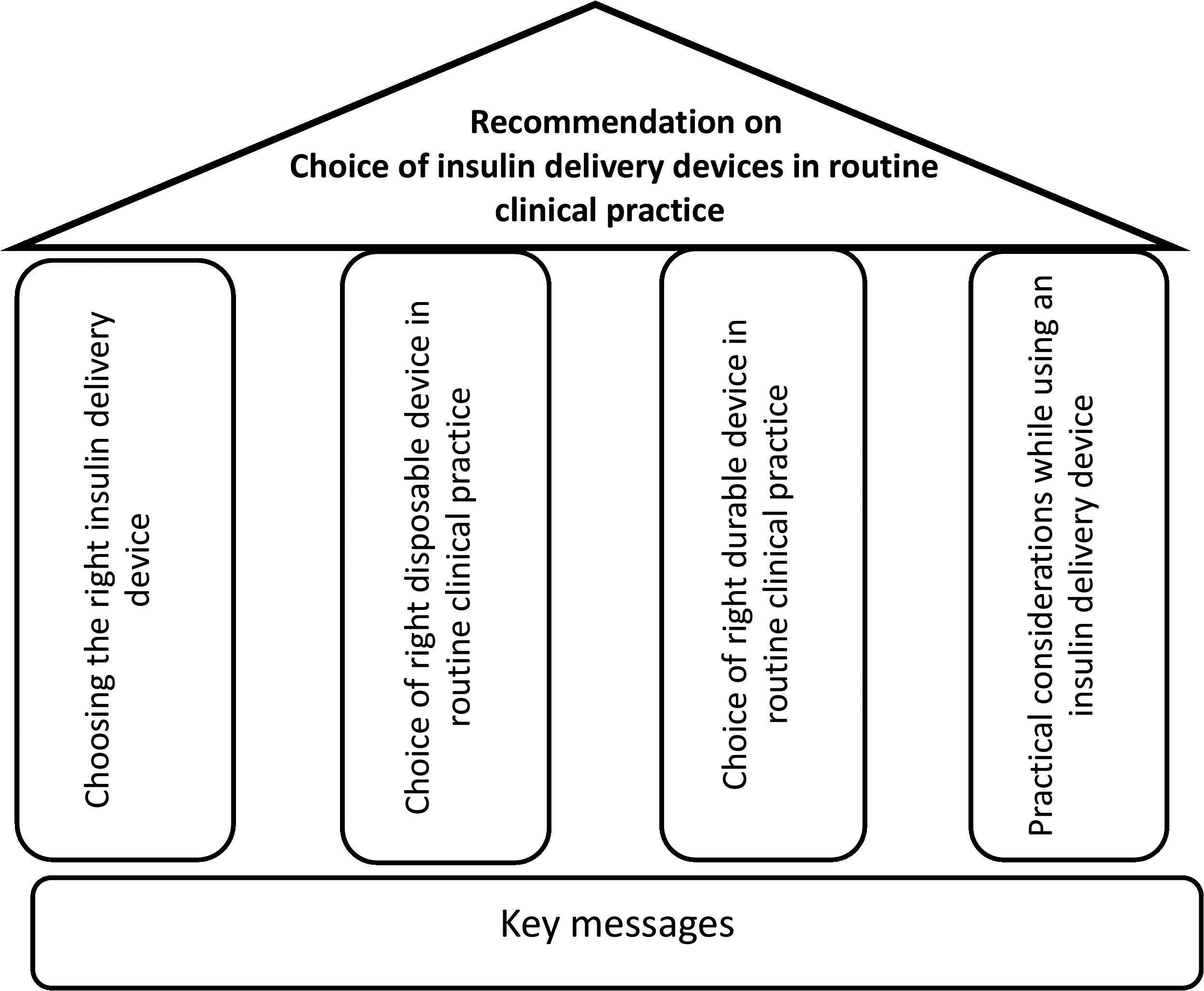
Framework of consensus recommendation.
Details of Randomized Controlled Trials Conducted in Various Countries
T2DM, type 2 diabetes mellitus.
Types of insulin delivery pens
There are two types of insulin pens: reusable (durable) and prefilled (disposable) pens. Reusable pens require an insulin cartridge to be inserted into the pen's delivery chamber. In such devices, types of insulin can be changed without a need to buy another pen if a type of insulin is changed. It may be more economical than prefilled pens. Reusable pens are durable and easy to use. Risk of infection can be minimized if an insulin pen is not used by more than one individual, even if the pen needle is changed because sharing of insulin pens can result in the transmission of blood-borne pathogens, hepatitis viruses, or human immunodeficiency virus. 7
Prefilled pens contain a built-in single-use insulin cartridge. Such devices do not require loading by the patient. Therefore, they are easy and convenient to use. These durable and lightweight devices are particularly useful in patients who have difficulty handling the cartridges. 8
Factors to be considered while prescribing insulin delivery device
The selection of an insulin delivery device depends on the insulin regimen of the patient, their lifestyle, and their preferences. Patient adherence is better where the device causes the least disruption to the patient's day-to-day life. The factors to be considered while selecting a pen are given in Table 2. 8
Factors to Be Considered While Prescribing an Insulin Delivery Device
An ideal insulin delivery device
An insulin delivery device should have the following characteristics: Accurate in delivering the prescribed dose of insulin Ease of use (less dose force and confirmation of delivery of dose) Less painful delivery of insulin Should alleviate the social stigma of using insulin delivery devices Should be easy to learn the technique Improve patient adherence to therapy Should provide better glycemic control Reduce the risk of hypoglycemia Should be stable in the Indian climate
For visually impaired diabetes patients, an ideal insulin delivery device should have the following properties:
It should have sufficient thickness so that it is easy for gripping.
The housing should have markings that make the use of an insulin pen easy for blind or visually impaired patients and to help prevent confusion with other insulin pens that may contain other types of insulin.
Audible and tactile feedback to select the units of insulin.
If possible acoustic or tactile reminders of the time and the amount of the most recent insulin injection.
Easily readable display for the visually impaired.
An ideal delivery device can improve adherence to insulin therapy. Selecting the right insulin pen device for the right patient is important to overcome insulin barriers among patients.
The need for guidelines
There are various international guidelines for recommendation about insulin pens. 9 Forum for Injection Technique and Therapy Expert Recommendations for Best Practice, 2017 mentions about insulin injection techniques. 10 One market research survey from emerging countries such as Brazil, China, Egypt, India, and Malaysia provides insights from people with diabetes into usage characteristic of 3–4 different reusable insulin pens available and to observe their preference for usage of pens. Although insulin pen devices are used widely in India, there are no guidelines available on them. 11 Therefore, there is a need for developing guidelines on the selection of right insulin pen devices for India also.
Expert recommendation 1: choosing the right insulin delivery device
Evidence from two studies shows that patients with type 2 diabetes mellitus (T2DM) who initiated treatment or switched to treatment with a pen device are more adherent to insulin therapy than patients who use a vial and syringe (Fig. 1). 12,13 Adherence (measured by the proportion of days covered) among patients initiated with insulin delivery devices was 54.6% compared with 45.2% among patients initiated with vial and syringe. 12 Adherence (measured by the medication possession ratio) among patients switching from a vial and syringe to a pen device was 69% compared with 62% among patients switched over to vials and syringe. 13
Pen device users are less likely to discontinue treatment. 14 –16 The risk of treatment discontinuation among insulin-naive patients initiated insulin therapy (n = 1876) with a pen was 38% lower than in patients using a vial and syringe over 1 year. 14 Among elderly insulin-naive patients initiated treatment with a pen (n = 3172), the risk of treatment discontinuation was 58% lower than in the vial and syringe cohort over 1 year. 15 In another study, the risk of discontinuation among insulin-naive patients initiated insulin therapy (n = 1466) with a pen device was 10.5% lower than in patients using a vial and syringe over 1 year. 16
A retrospective analysis of a United States database demonstrated that among 1308 patients with T2DM initiated with insulin therapy significantly more pen users continued with insulin treatment than vial and syringe users (58.4% vs. 51.4%, respectively; P = 0.011). Also, significantly more pen users continued with insulin treatment for a longer duration than vial and syringe users (314 vs. 299 days, respectively; P = 0.001). 17
Multiple studies found that patients initiated with insulin therapy using pen devices achieved significantly lower glycated hemoglobin (HbA1c) levels than vial and syringe users after 1 year (Fig. 2). 16 –18
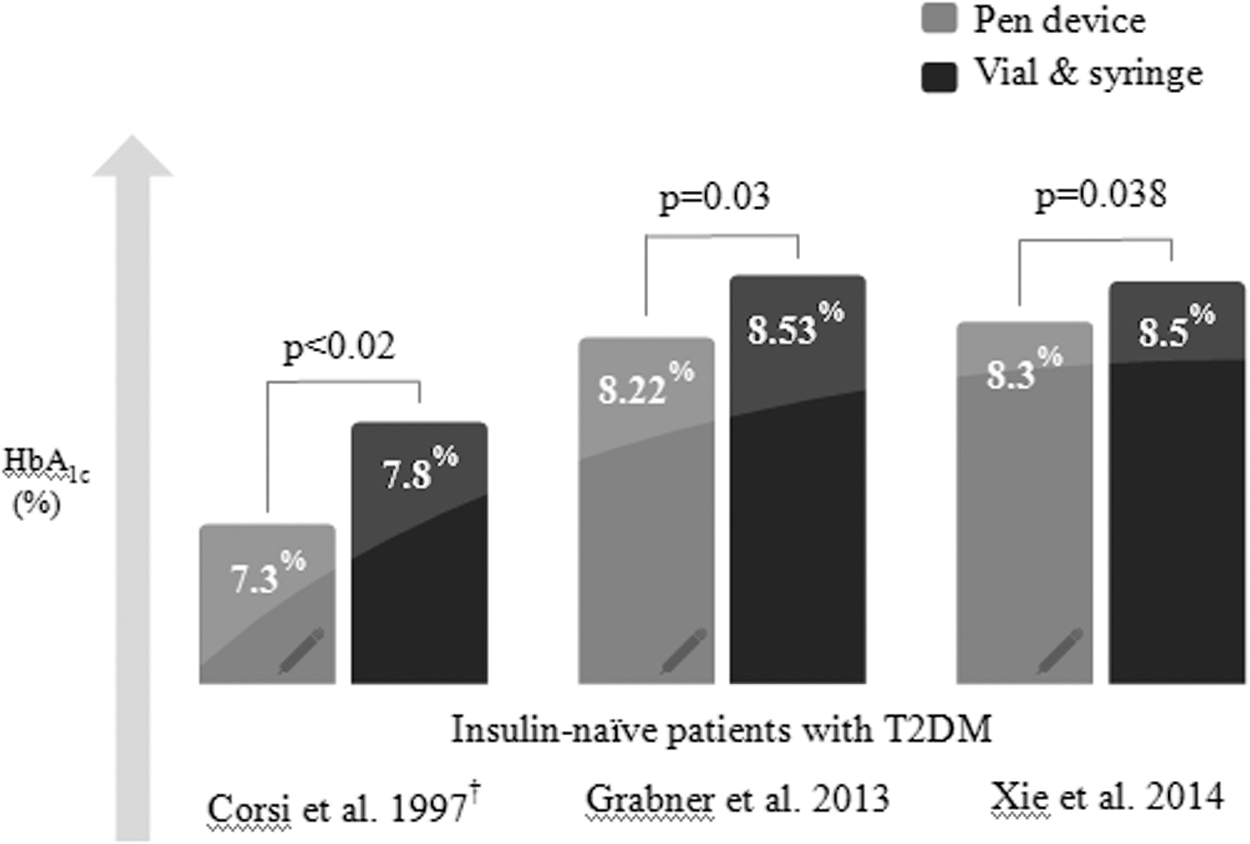
HbA1c levels among patients initiated with a pen versus a vial and syringe.
The risk of hypoglycemic events was lower among patients initiated insulin therapy with pens than vial and syringe. The risk of hypoglycemia among insulin-naive T2DM patients initiated insulin therapy with pens was 5.7% compared with 7.8% in those with vials and syringe. Among patients aged ≥65 years, it was 8.6% versus 10.4%. Pen device users experienced 64% fewer hypoglycemic events after conversion from a vial and syringe. 13,17,19
Two studies evaluating the accuracy of insulin dose with pen devices found that they offer accurate insulin dosing. In one of the studies, 39 out of 40 patients were confident in achieving dose accuracy with a pen device. 20,21
Nurses are the first health care professionals to interact with patients. They are involved in training, education, and motivation of diabetes patients about insulin use and in achieving treatment goals. A study comparing nurses' perceptions and satisfaction with the use of insulin pen devices versus vial and syringes for insulin delivery reported that pen devices decrease the risk of needle stick injuries and giving the wrong insulin dose. In addition, 98% of nurses felt that the insulin device saves time to prepare and administer insulin compared with 38% of nurses who used a vial and syringe. 22
A cost-effectiveness model among patients with diabetes demonstrated that over 5 years patients gain 3.18 and 3.17 quality-adjusted life years with a pen and a vial and syringe, respectively. 23 Patients with T1DM or T2DM in Taiwan who completed the 36-Item Short-Form Health Survey (SF-36) reported significantly greater improvements in general health status scores with a pen device than with a vial and syringe. 24 These two studies concluded that pen devices improve health status and are considered cost-effective. 23,24
Pen users reported fewer diabetes-related hospitalizations than vial and syringe users. Patients with T2DM who initiated therapy with a pen device required 4.8% fewer diabetes-related hospitalizations over 1 year than those using a vial and syringe. 17 After the initiation of insulin therapy, adherent and nonadherent pen users had significantly lower hospitalization rates than adherent and nonadherent vial and syringe users. 25 Pen users also had a fewer emergency department and physician visits. 13
Among T2D patients using a pen device, 90% agreed that they can draw and dispense insulin with less nursing assistance. 26 Of 33 physicians treating patients with T1DM or T2DM, 73% believed that it takes less time to initiate therapy with a pen than a vial and syringe, 88% believed that it takes less time to teach patients to use a pen than a vial and syringe, and 97% consider insulin therapy via a pen device better overall than a vial and syringe. 27
Pen devices are associated with decreased daily insulin consumption. Insulin-naive patients who initiate insulin therapy with a pen device had lower daily insulin consumption over 1 year but a higher treatment adherence, compared with those who initiate therapy with a vial and syringe. 19
In patients with T1DM in Ireland, 95% of patients preferred an insulin pen device to a vial and syringe. 28 In diabetes patients >60 years in Italy, 90% of patients preferred the insulin pen to a vial and syringe. 3 In a cross-over study in Morocco among patients with T2DM, 89.5% preferred pens to vials and syringes. 24 Among patients with T1DM or T2DM in Italy, the United States, and Ireland: 3,28,29
88% of patients considered pens faster to use
85% of patients perceived pens to be more discreet
74% of patients found pens easier to use
81% of patients believed pens offer more flexibility.
In a study assessing injection pain, pen device users reported that they experience no pain during insulin injection compared with 26.7% of vial and syringe users. 30 In children with diabetes, 95% preferred administering insulin with a pen device than with a vial and syringe, for reasons related to ease of use, convenience, and dose accuracy. 31
Based on these reports, recommendations on choosing the right insulin delivery device were made.
Recommendations
The highest discontinuation of insulin therapy occurs in the first 12 weeks. Hence, initiation of insulin therapy should be done with a device in which the patient is least likely to discontinue during this period.
Pen devices increase treatment adherence and continuation compared with vials and syringes
Pen devices offer clinical and safety benefits compared with vials and syringes
Pen devices are preferred due to better accuracy and less variability in dosing
Pen devices are associated with cost savings in the long term due to less risk of hypoglycemia and associated emergency hospital visits.
Expert recommendation 2: choice of a right disposable device in routine clinical practice
A list of available disposable pens is mentioned in Table 3 and Figure 1. Disposable insulin delivery devices are indicated for short-term use in newly detected severe hyperglycemia, insulin initiation and hospitalization, pregnancy, elderly, patients with visual disturbances/dexterity problems, and patients undergoing surgeries.
List of Disposable Pens
Several studies have demonstrated the superior accuracy of FlexPen® to other prefilled insulin injection pens at high, medium, and low doses. In a study comparing the dose accuracy of FlexPen with a vial and syringe, FlexPen was significantly more accurate than a vial and syringe. The delivered mean dose was significantly closer to the intended insulin dose of 10 IU with FlexPen than with a syringe and vial. With the vial and syringe method, the mean dose delivered was significantly higher than that delivered by the insulin therapy-naive Healthcare Professionals group, who had no previous experience with insulin injections (P < 0.001). There was also a wider variation in the size of doses delivered with a vial and syringe compared with FlexPen. 32
Next-Generation FlexPen was designed to improve patient perception and is as accurate as FlexPen. A study compared the accuracy of Next-Generation FlexPen versus SoloStar®. Next-Generation FlexPen was significantly more accurate than SoloStar for delivering 10 and 30 IU of insulin. With Next-Generation FlexPen, the mean (±standard deviation) from the intended dose at 10 IU was 1.63% (±0.84%). This was significantly lower than the mean deviation with SoloStar (2.11% ± 0.92%; P < 0.001). 32 A study compared the dose force with Next-Generation FlexPen with SoloStar and KwikPen®. At injection speeds of 3.3, 5.0, and 8.3 mm/s, the mean dose force was 5.7, 8.2, and 12.7 N, respectively, with Next-Generation FlexPen, which was 15%–22% lower than the dose force with SoloStar fitted with the same needle (6.7, 10.4, and 16.3 N, respectively; P < 0.05) and 37%–41% lower than the dose force with KwikPen fitted with the same needle (9.1, 13.1, and 21.6 N, respectively; P < 0.05). 33
Analysis of claims database of patients with type 2 diabetes switching from human or analogue insulin injection (vial/syringe) to a prefilled insulin analogue pen showed significantly higher adherence when using FlexPen compared with a vial and syringe. 13 A survey was conducted to assess patient perception of usability, safety, and convenience of Next-Generation FlexPen and the ease of attaching NovoTwist and NovoFine® needles. A 35-item questionnaire was completed by patients with type 1 or type 2 diabetes. Overall, 89% of patients rated Next Generation FlexPen as the most convenient pen to use (P < 0.001 compared with FlexPen), and 84% of patients rated it as the simplest pen to use (P < 0.001 compared with FlexPen). It instilled more trust and confidence than FlexPen in 50% of patients, and 48% had no preference. 34
FlexTouch® was accurate for the delivery of 1, 40, and 80 U insulin detemir and insulin aspart. FlexTouch was significantly more accurate for the delivery of 1 U of insulin detemir and insulin aspart versus SoloStar for the delivery of insulin glargine (1.14 ± 0.22 U, range 0.49–1.39 U, P < 0.0001). FlexTouch had consistent accuracy when delivering 1, 40, and 80 IU as demonstrated through the repetitive test results, and demonstrated by relatively low standard deviations. 35 The injection force of FlexTouch was 65%, 76%, and 82% lower than KwikPen at 4, 6, and 8 mm/s, respectively (P < 0.0001), and 62%, 73%, and 81% lower than SoloStar at 4, 6, and 8 mm/s, respectively (P < 0.0001). 36
Three multicenter, open-label, usability studies were conducted in people with type 1 or 2 diabetes (outpatients) and in physicians and nurses in a crossover design. Considerably more people with diabetes and health care professionals chose FlexTouch (83%–91%) as easier to use than SoloStar (9%) and KwikPen (4%). More people with diabetes and health care professionals felt “very confident” or “rather confident” that they/their patient would control blood sugar levels by using FlexTouch than using SoloStar or KwikPen. FlexTouch was rated higher than the other devices on the 5-point scale (P < 0.001 Wilcoxon signed rank tests). 36 –38
In another study, a significantly higher proportion of people with diabetes and HCPs had more confidence in correct and complete dose delivery with FlexTouch Tresiba® 100 U/mL (68.8%) and FlexTouch Tresiba 200 U/mL (71.9%), than with SoloStar (<6%; P < 0.001). 39 Patients and HCPs preferred FlexTouch to SoloStar or KwikPen for ease of learning to use. 40 Considerably more people with diabetes and health care professionals would recommend FlexTouch (83%–91%) to others than would recommend SoloStar (8%) or KwikPen (6%), and these differences were statistically significant (P < 0.001). 36 –38 The majority of patients, with dexterity or a visual impairment, preferred FlexTouch to InnoLet®. 39 A randomized, multicenter, open-label, crossover study compared FlexTouch and FlexPen in insulin-treated pen-naive patients with type 1 or T2DM for 12 weeks. Glycemic control achieved with FlexTouch was comparable to that with FlexPen. More patients (68%) preferred FlexTouch device over FlexPen. In addition, most subjects found FlexTouch® easier to use (64% [144/226]), easier to inject the insulin dose (65% [148/227]), and easier to push for injection (69% [155/226]). 41
Recommendations
Disposable devices are more accurate than a vial and syringe
Adherence is significantly better after switching to disposable delivery devices from a vial and syringe
Among disposable devices
○ FlexPen significantly better accuracy than SoloStar
○ FlexPen has a significantly lower dose force than SoloStar and KwikPen
○ FlexTouch has a lower injection force than other prefilled pens
Expert recommendation 3: choice of a right durable device in routine clinical practice
Many durable devices are available (Table 4) for use (Fig. 1). Durable insulin devices are simple outside but complicated inside. 42
List of Durable Insulin Devices Available
NovoPen® 4 (Novo Nordisk) has been designed to make insulin injections even simpler, with features such as a four-times larger dose setting window, an easy-to-read dose scale, less force required to inject, metallic body, child lock facility, and an end-of-dose confirmation click. Doses with NovoPen 4 can be set from 1 to 60 U in 1-U increments and doses are most accurate. 42
A study assessed simulated 5-year use of NovoPen 4 without insulin cartridge. It involved 5475 automatic injections by the robot (corresponding to three injections per day for 5 years). Dosing included removal and replacement of the cap. Dose accuracy also tested the following storage without cartridge, under hot, cold, and humid conditions and freefall from 1.5 m onto various surfaces. There was no significant difference in the dose accuracy of the NovoPen 4 before and after 5 years of simulated use. Exposure to variations in temperature and humidity and freefall did not affect the dose accuracy. 43
Another study showed the highest accuracy of dosing with NovoPen 4 compared with ClikSTAR® or Luxura®. The mean dose delivered by ClikSTAR or Luxura was less than the expected 30 U and significantly less than the mean dose delivered by NovoPen 4. There was no significant difference in dose delivery with NovoPen 4 (30.04 U) from the expected mean. NovoPen 4 had the greatest variance in laboratory testing but the least in the simulated clinical setting. 44 Ease of fitting cartridge, dose setting, and dose delivery of NovoPen 4 were better than ClikSTAR, HumaPen® Luxura, Itango®, and Biosulin® Pen. NovoPen 4 required the least force followed by ClikSTAR and Itango. HumaPen Luxura required an injection force approximately twice that of other pens. 45 Handling and acceptance of NovoPen 4 was superior compared with HumaPen Ergo and Optipen® Pro in patients and health care professionals. 46
More than 90% of patients rated performing different tasks on NovoPen 4 as very easy/easy. In addition, more than 96% of patients found NovoPen 4 very/convenient for everyday handling, and because of its weight and size, appropriate to use in public. Patients felt significantly greater satisfaction after using NovoPen 4 for 12 weeks compared with their previous use of NovoPen 3 or other insulin delivery devices. 47 NovoPen 4 was quick and simple to use, lasted longer even under extreme conditions, and delivered accurate insulin for a long time. It has an end-of-dose click for patient convenience. It is useful for elderly diabetes patients with visual and/or physical dexterity impairments.
Recommendations
Patients can be started on durable devices or shifted from other devices
Durable delivery devices maintain accuracy and low dose force compared with vials and syringes
A larger window for dose selection, lesser dose force, durability, and end of dose click makes NovoPen 4 a preferred durable delivery device
Expert recommendation 4: practical considerations while using an insulin pen device
Self-management is an inevitable task for patients living with diabetes (Fig. 1). The process of injecting insulin involves several tasks such as measuring blood glucose, assessing the timing of insulin injections relative to meals, and self-injecting insulin. During each injection, the process of assembling and dosing the insulin must be meticulously carried out to ensure the proper delivery of insulin. Incorrect injection technique will lead to poor glycemic control due to mismatch of peak insulin effect and maximal glucose load. Hence, the injection technique is critical to the therapeutic success of insulin. 48
Improper use or reuse of needles may lead to undesirable consequences, including pain with bleeding and bruising, breaking off and lodging under the skin, contamination, dosage inaccuracy, and lipohypertrophy. Insulin pen cartridges can become contaminated, and pathogens are transmitted if multiple patients use a pen. Needle reuse causes damage to the tip of the needle, needles bend, and the silicone lubricant coating of the needles is also lost. All these contribute to more and increase pain during injection. Therefore, the needle should not be reused. 49
The needle in the insulin pen should be removed and disposed of safely immediately after injection. The needle should not be left attached to the pen to prevent the entry of the air into the cartridge as well as leakage of the medication, which can affect subsequent dose accuracy. 49
Besides an appropriate selection of insulin devices, the needle, its length and gauge are critical. Pen needles are available in 4, 5, 6, and 8 mm sizes and are of 32, 31, and 30G. 48 The frequency of painful injections and bleeding increases with an increased needle gauge. Thin-wall technology is used to manufacture needles with the same outer diameter, but a relatively large inner diameter. This allows improved insulin flow, reducing injection time and injection force. 50
NovoFine 32G 4 mm has been designed and engineered to reduce the risk of needle breakage and bending. Needle glue tower protects the cannula from breakage, and cannula design improves bending resistance. It also minimizes pain and risk of intramuscular injection. In a study, injection with a 32G needle was associated with reduced frequency of pain and bleeding compared with thicker needles (27, 28, 30, and 31G). Most patients were able to inject with a 4-mm needle without making a skin fold in the thigh. It also reduced the risk of penetrating underlying muscle with a 4-mm needle and caused less trauma and discomfort. 9,51 –53 A multicenter open-label, single-arm study in patients with diabetes (n = 92) using insulin pens for 2 weeks each with standard needles and thin-wall needles showed that patients experienced less pain, skin irritation and bleeding with thin-wall needles compared with standard needles. 50
A few accessories are available to improve the comfort of insulin injection such as automatic injectors, needle-free injectors, devices for magnification, insulin ports, cooler bags, needle safety guards, and dosing aids. In automatic injectors, a loaded syringe is placed into the device. The tip is placed against the skin, and the button is pressed to automatically deliver the needle through the skin sight-unseen. 54 Needle-Free Injector is an all-stainless-steel, semiportable device, without a needle, so that needle phobia is avoided. It was used in vaccination programs from the 1950s and discontinued by the 1990s because of cross-contamination issues. 55 Devices for magnification are a clear plastic tube that fits over the barrel of a syringe, magnifying its markings by 2 × . 56
Insulin ports are a patch-like device that reduces the number of times that needle injections are necessary. The cannula is inserted into the skin at an angle of 20–45° with a needle as the guide. Injections are made into a plastic tube that is attached flat against the skin. The port must be replaced at least every 3 days. 56 Cooler bags are used to keep insulin cool and safe. It contains ice packs. It should be kept in a refrigerator for 6–8 h until it becomes solid and reused. Needle safety guards are attachments that fit over the cap of an insulin vial, creating a barrier that protects the hand holding the vial from accidental needle sticks. Dosing aids allow a blind or visually impaired person to fill a syringe with the desired amount of insulin. A syringe is placed in Count-a-Dose so that the needle is inserted into an insulin bottle, located in the device's bottle holder. With each click of a dial, a unit of insulin is drawn. 57
Recommendations
One patient—one device
Use a sterile, new needle for each injection
Thin-walled needles are associated with less pain, skin irritation, and bleeding compared with standard needles
When a patient is newly initiated with a pen device, a backup 100 IU syringe should be provided to use in case of device failure
The patient should be regularly counseled on the proper usage of delivery devices
Summary
This expert panel-based consensus provides a simple and implementable guideline for physicians and patients to select ideal insulin pen device in accordance with new research findings, recent advances in pen manufacturing, and updated international guidelines The recommendations include use of insulin pens in case the patient is not continuing insulin therapy, accurate dosing provided by pen devices, improving patient adherence, lower dose and injection force, and single patient use. The current consensus has been developed with due consideration to the Indian context based on experience and common therapy practices in India. The final proposed consensus-based recommendations were collectively recorded in easily implementable steps, without any bias and in an as much possible unambiguous language.
Recommendations regarding insulin pen devices provided in this consensus statement emphasize:
Insulin should be initiated by using an insulin device if the patient seems to discontinue insulin therapy.
Pen devices offer accurate dosing than a syringe and vial and are associated with cost savings in the long term.
Switching over from syringes and vials to disposable delivery devices improves adherence.
FlexPen offers better accuracy, requires lower dose force and injection force than SoloStar and KwikPen.
Durable delivery devices such as NovoPen 4 maintain accuracy and low dose force compared with vials and syringes.
One device should be used by only one patient.
Regular counseling on proper use of delivery device is required regularly.
Footnotes
Acknowledgments
All the named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given final approval for the version to be published. The authors thank the following members of the expert group committee for their comments and suggestions during the work shop: Dr. Balaji, Dr. Augraj Uprety, Dr. Ritesh Kalwar, Dr. K. Tamilarasan, Dr. Bijaya Krishna Prajapati, Dr. Bimalendu Chaterjee, Dr. Shalinder Sharma, Dr. Maithili L. Lad, Dr. Soumya Sengupta, Dr. Ajay Kumar S., Dr. Satisha Naik, Dr. Kingshuk Dutta, Dr. Joseph K. Joseph, Dr. Shrikant Jategaonkar, Dr. Joshy K. Cheriyan, Dr. Shiva Shankar, Dr. Subrata Biswas, Dr. Indrajit Paul, Dr. Balraj Gupta, Dr. Satyendra Misra, Dr. C.H. Ravikanth, Dr. Sunil Kohli, Dr. Shailndra Dixit, Dr. Deepak Agarwal, Dr. S. Sen Gupta, and Dr. Dibakar Sinha. The authors thank the organizers of the 12th National Insulin Summit for supporting the conduct of the consensus meeting.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors thank Dr. Punit Srivastava of Mediception Science Pvt. Ltd. for providing medical writing support in the preparation of this article, funded by Novo Nordisk, India.