
Abstract
Background:
Hybrid closed-loop systems may offer improved HbA1c levels, more time-in-range, and less hypoglycemia than alternative treatment strategies. However, it is unclear if glycemic improvements offset this technology's higher acquisition costs. Among adults with type 1 diabetes in Australia, we sought to evaluate the cost-effectiveness of a hybrid closed-loop system in comparison with the current standard of care, comprising insulin injections and capillary glucose testing.
Methods:
Cost-effectiveness analysis was performed using decision analysis in combination with a Markov model to simulate disease progression in a cohort of adults with type 1 diabetes and compare the downstream health and economic consequences of hybrid closed-loop therapy versus current standard of care. Transition probabilities and utilities were sourced from published studies. Costs were considered from the perspective of the Australian health care system. A lifetime horizon was considered, with annual discount rates of 5% applied to future costs and outcomes. Uncertainty was assessed with probabilistic and deterministic sensitivity analyses.
Results:
Use of a hybrid closed-loop system resulted in an incremental cost-effectiveness ratio of Australian dollars (AUD) 37,767 per quality-adjusted life year (QALY) gained. This is below the traditionally cited willingness to pay a threshold of $50,000 per QALY gained in the Australian setting. Sensitivity analyses that varied baseline glycemic control, treatment effects, technology costs, age, discount rates, and time horizon indicated the results to be robust.
Conclusions:
For adults with type 1 diabetes, hybrid closed-loop therapy is likely to be cost-effective compared with multiple daily injections and capillary glucose testing in Australia.
Introduction
Management of type 1 diabetes is complex. The complications of unstable blood glucose levels are multisystem and lead to significant morbidity, mortality, and health care costs. 1,2 Furthermore, while newer health technologies are being developed to improve glycemic control, it is unclear if these devices are cost-effective.
The value of intensive glycemic control has been established through landmark clinical trials such as the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) study that demonstrated lower HbA1c reduced vascular complications. 3 However, intensive management strategies targeting HbA1c values less than 7.0% (53 mmol/mol) have been limited by increased frequency of hypoglycemia. 3 –6 In an attempt to simultaneously reduce HbA1c and minimize the burden of hypoglycemia, hybrid closed-loop systems have been developed and may offer glycemic advantages over other management strategies. 7,8
In Australia, the economic burden of type 1 diabetes is estimated to be in excess of $570 million (Australian dollars [AUD]) per annum, which mirrors the international experience. 1,9 –14 The costs of diabetes not only comprise treatment, vascular complications, ambulance visits, and hospital attendances, but also indirect costs of reduced productivity. While health technologies offer the potential for improved outcomes, access is not equitable due to high acquisition costs and limited funding. 8,15 –17 The current standard of care in most settings remains multiple daily injections (MDI) with self-monitoring of capillary blood glucose (SMBG), 8,13,18 being the least expensive treatment strategy with the broadest penetrance. Despite Australia's universal health care system, at the time of writing insulin pumps cost $7,362–$9,025 (AUD) and among adults are accessed by those who can afford supplementary private health care insurance or completely self-fund. 15,19 In addition, the retail cost of continuous glucose monitoring (CGM) is estimated to exceed $5,000 (AUD) per year, but most adults with type 1 diabetes do not receive subsidy or have the costs of CGM covered by private health care insurance. 15,20
A recent network meta-analysis has reported that integrated insulin pump and CGM systems with low-glucose suspend or hybrid closed-loop algorithms reduced HbA1c by 0.87% (9.5 mmol/mol; 95% predictive interval 0.12–1.63 [1.3–17.8 mmol/mol]) compared with MDI with SMBG. 21 However, it is unclear if the cost of funding these devices would be offset by the projected long-term reductions in complications. We thus performed a cost-effectiveness analysis to compare a hybrid closed-loop system to MDI and SMBG among adults with type 1 diabetes over a lifetime horizon, from the perspective of the Australian health care system.
Materials and Methods
Simulation cohort and treatment effects
The model was populated with a hypothetical sample of 1000 individuals profiled largely on adult subjects with type 1 diabetes from the Australian National Diabetes Audit (ANDA). 22 Diabetes centers, including primary care and community-based centers across Australia, voluntarily participate in ANDA as an annual cross-sectional benchmarking activity comprising data from adult and pediatric patients with diabetes (type 1 and 2). The simulation cohort was 18 years of age with no vascular complications and diabetes duration of 10 years at baseline. Rates of severe and nonsevere hypoglycemia for individuals using MDI and SMBG were drawn from large cohort studies. 23,24 One severe hypoglycemic event (requiring third-party assistance) per person-year was modeled among the predicted ∼80% of the population with normal hypoglycemia awareness, and six events per person-year in the presence of hypoglycemia unawareness. 23 –27 Treatment effects for hybrid closed-loop therapy in terms of HbA1c reduction were conservatively extrapolated from a randomized-controlled trial (RCT) comparing a hybrid closed-loop system with sensor-augmented pump therapy. 28 Rates of severe hypoglycemia were assumed to be reduced by 95%, and reduction of nonsevere hypoglycemia was modeled from a 53% relative reduction in time below range. 29 A detailed profile of the simulation cohort and treatment effects are provided in Tables 1 and 2 and the Supplementary Table S1.
Characteristics of the Base-Case
HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Treatment Effects and Utilities Used in Analysis
Model description and outcomes
The Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement was followed throughout. 32 A decision analytic Markov model with annual cycles was developed to assess the cost-effectiveness of a hybrid closed-loop system versus MDI with SMBG among adults with type 1 diabetes (Fig. 1). A simulation cohort with type 1 diabetes and no vascular complications populated the model at baseline. The possible health states were as follows: no complications, only microvascular complications, only macrovascular complications, both microvascular and macrovascular complications, and death. Complications of diabetes comprised diabetic retinopathy, sight-threatening diabetic retinopathy, blindness, diabetic nephropathy, diabetic foot ulcers, lower extremity amputations, acute myocardial infarction (AMI), unstable angina, stroke, and congestive heart failure (CHF). Health states, including microvascular complications, were further subdivided based on the presence of microalbuminuria, macroalbuminuria, or end-stage kidney disease (ESKD). Nephropathy could progress directly from microalbuminuria or macroalbuminuria to ESKD or death from renal causes. Regression of nephropathy or retinopathy was not modeled directly. Macrovascular complications were subdivided into primary or recurrent events. The interrelated nature of complications was reflected by altering transition probabilities for all health states based on the shared risk factor of HbA1c, and incorporating renal health states as part of annual cardiovascular risk prediction. Mortality was modeled for cardiovascular disease (CVD), renal causes, as well as “other causes.” Individuals in the simulation cohort continued to cycle through the model until death or age 100 years.

Structure of the cost-effectiveness model. Solid lines represent nonfatal transitions and dashed lines represent transitions to death. Macrovascular cx* (complications) may represent the first macrovascular event or a recurrent event depending on the order of transitions through health states. Only microalbuminuria, macroalbuminuria, or ESKD could lead to renal death. ESKD, end-stage kidney disease.
The cost perspective was that of the Australian health care system. All costs and outcomes were discounted by 5% annually based on guidelines by the Australian Government Department of Health, 33 and the primary outcome of interest was the incremental cost-effectiveness ratio (ICER) in terms of cost per quality-adjusted life year (QALY) gained.
Transition probabilities and mortality risk
Transition probabilities were derived from published sources to simulate disease progression (Table 3). The most contemporary published data available were sought and age-specific all-cause mortality was drawn from published Australian data for people with type 1 diabetes. 38
Annualized Costs Used in Analysis
Assumed variance of 25% above and below the mean. Costs reported in 2019 in Australian dollars.
The treatment effect of hybrid closed-loop therapy on HbA1c determined the difference in transition probabilities between treatment groups for all vascular complications. Rates of severe and nonsevere hypoglycemia per person-year were modeled to reflect the possibility of having multiple hypoglycemic events in a year rather than annual transition probabilities. To predict the annual probability of the first macrovascular event, “The Steno Type 1 Risk Engine” model was used and involved the variables of age, sex, diabetes duration, systolic blood pressure, low-density lipoprotein cholesterol, HbA1c, presence or absence of microalbuminuria or macroalbuminuria, estimated glomerular filtration rate (eGFR) above or below 40 mL/min/1.73 m2, smoking status, and participation in regular exercise. 30 eGFR was assumed to be >40 mL/min/1.73 m2 unless patients transitioned to ESKD. Recurrent cardiovascular events had to be preceded by a cardiovascular event at least 1 year earlier, and renal death could only occur in the presence of renal pathology arising at least 1 year prior. To predict the probability of recurrent events, the results of “A new model for 5-year risk of CVD in Type 1 diabetes” were annualized. 39 This cardiovascular risk prediction model includes variables of age, diabetes duration, HbA1c, systolic blood pressure, total cholesterol to high-density lipoprotein cholesterol ratio, smoking status, presence or absence of macroalbuminuria, and the presence of a previous event. A random number was generated to determine patient sex, smoking status, and participation in regular exercise within the cardiovascular risk prediction models. Patients were assumed to be male, smokers, and physically inactive when the random numbers generated were less than the estimated cohort-specific probabilities for each variable included in Table 1. Results from the DCCT/EDIC study were utilized to predict the proportion of events comprising AMI, stroke, or CHF. 40 Because cardiovascular risk prediction models generated a composite of fatal and nonfatal events, case-fatality data were utilized to derive mortality rates for AMI, stroke, and CHF. Angina and lower extremity amputations were assumed to be nonfatal. Because cardiovascular and renal mortality rates were modeled separately in relation to glycemic control, these causes of death were subtracted from Australian estimates of all-cause mortality to avoid double counting. 38
Costs and utilities
All costs were reported in 2019 AUD with any adjustment for inflation/deflation using the health consumer price index. 41 Costs were sourced from the largest Australian cost of illness study comprising 2200 people with type 1 diabetes randomly selected from an Australian diabetes register (National Diabetes Services Scheme [NDSS]). 9 Direct health care costs related to any public or private health service visit and use of medications (Table 3). Data sources for the cost of illness study included Medicare Benefits Schedule and Australian Medical Association fees, Pharmaceutical Benefits Scheme prices for reimbursed drugs, Pharmacy Direct prices for nonreimbursed drugs, National Diabetes Service Scheme database, National Cost Data Collection, and Cost Report Round 6 using AR-DRG 4.2 classifications. 9 For severe hypoglycemia, an Australian economic evaluation was utilized that comprised costs for ambulance callout, hospital admission, accident and emergency visit, glucagon injection, and follow-up visits. 37 Nonsevere hypoglycemia were assumed to have no associated costs, but an annual disutility was applied to these events.
Regarding intervention costs, the analysis included only incremental costs of a hybrid closed-loop system over MDI with SMBG therapy. The only commercially available hybrid closed-loop system in Australia at the time of writing comprised the MiniMed™ 670G (Medtronic), infusion sets, reservoirs, batteries, Guardian™ Sensor 3 (Medtronic), transmitter, and transmitter charger. Twice-daily capillary glucose testing was assumed for calibration when using the hybrid closed-loop system compared with eight tests per day for MDI and SMBG. Sensitivity analyses considered other brands of insulin pumps and CGM sensors (Table 4 and Supplementary Table S2).
Deterministic Scenario Analyses
CGM, continuous glucose monitoring; ICER, incremental cost-effectiveness ratio.
Utilities and costs for the model health states were drawn from the same Australian cost of illness study described above. 9 Participants completed the standardized EuroQOL five-dimension questionnaire (EQ-5D), with results presented for people with type 1 diabetes and no complications, with only microvascular complications, with only macrovascular complications, or both microvascular and macrovascular complications. 9 Annual disutilities of −0.0475 and −0.0041 were utilized for severe and nonsevere hypoglycemia, respectively. 31 Disutility data for hypoglycemia were derived as the average of daytime and nocturnal events from a large Canadian time trade-off survey. 31
Sensitivity analyses
Probabilistic and deterministic sensitivity analyses were undertaken to assess the impact of uncertainty and ascertain key determinants of cost-effectiveness. Probabilistic sensitivity analyses were undertaken with 10,000 iterations to simultaneously account for uncertainty across multiple input parameters. Additional scenario analyses were undertaken to explore model assumptions that comprised the following: reducing discount rates for future costs and benefits to 3.5% and 1.5%; halving the cost or number of capillary glucose tests used in standard care; halving the cost of hybrid closed-loop systems; assuming costs of hybrid closed-loop systems related to the t:slim X2™ or mylife™ YpsoPump® insulin pump paired with Dexcom G5® CGM; assuming no cost for insulin pumps; assuming 25% reduction in the treatment effect on nonsevere hypoglycemia; assuming twice as many episodes of severe hypoglycemia per person in the first year of hybrid closed-loop therapy; assuming treatment effect on severe hypoglycemia was reduced to 60% or 50%; assuming no treatment effect on severe hypoglycemia; assuming no treatment effect on HbA1c; assuming baseline HbA1c was 7.0% (53 mmol/mol); reducing the time horizon to 20 years; assuming the simulation cohort was aged 40 years at baseline instead of 18 years; and assuming that the hybrid closed-loop therapy commenced at age 40 or 50 years (Table 4). Microsoft Excel (Microsoft Corporation, Redmond, WA) and @risk version 7.6 (Palisade Corporation, Ithaca, NY) were used for the economic analyses.
Results
Relative to MDI and SMBG, use of a hybrid closed-loop system was associated with gains of 0.079 (discounted) years of life and 3.724 (discounted) QALYs per person over a lifetime, at a net cost (discounted) of $133,800 (AUD). Over 10,000 simulations, hybrid closed-loop systems were associated with a mean (95% confidence interval [CI]) ICER of $37,767 (95% CI $20,035–$64,393) per QALY gained (Fig. 2). At a willingness-to-pay threshold of $50,000 per QALY gained, 86% of simulations predicted the hybrid closed-loop system to be cost-effective (Fig. 2).
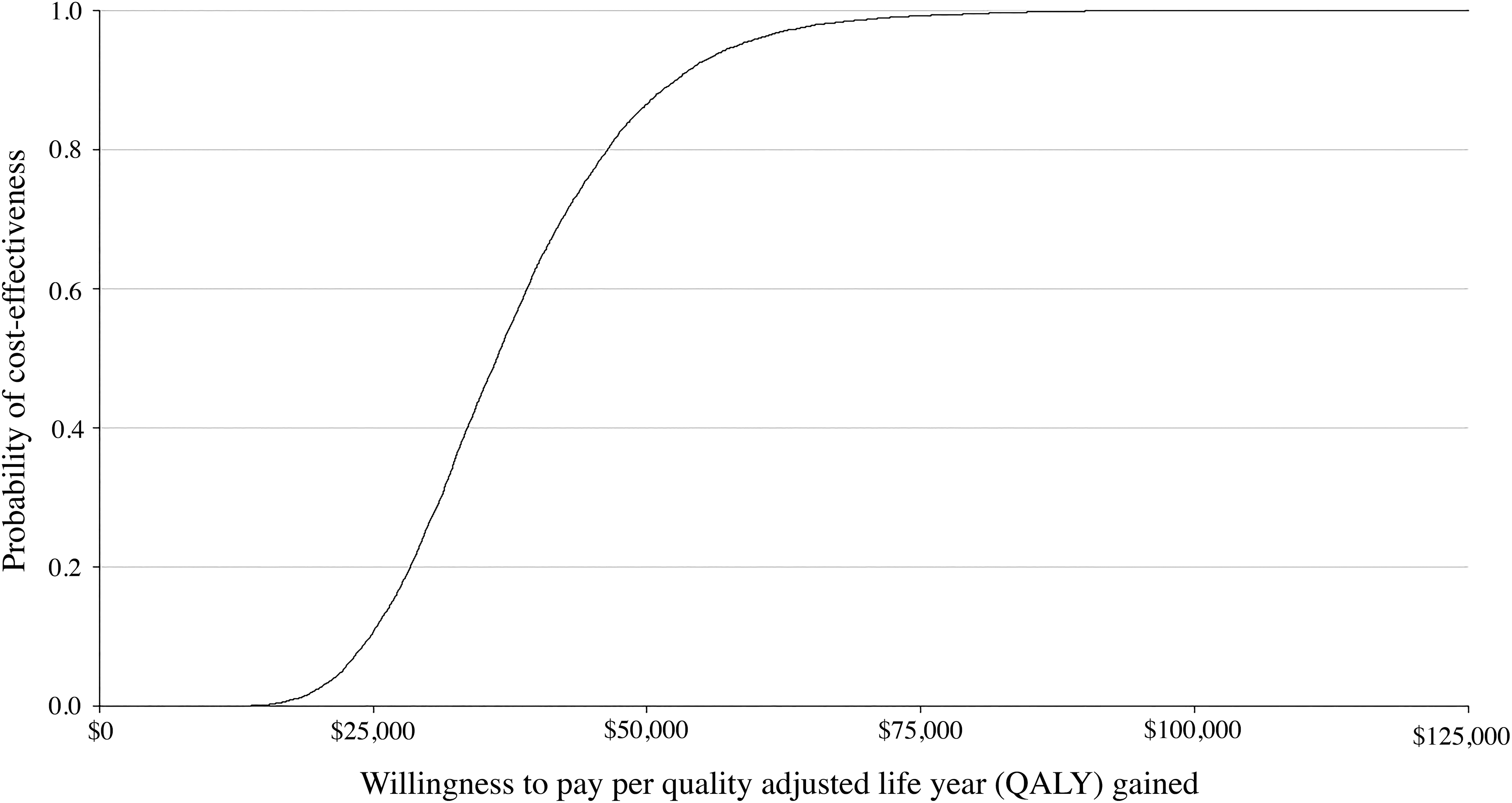
Cost-effectiveness acceptability curve. QALY, quality-adjusted life year.
Sensitivity analyses found that results were most sensitive to the cost of the hybrid closed-loop system, disutility of severe and nonsevere hypoglycemia, and treatment effect on hypoglycemia (Fig. 3). Results of the scenario analyses are included in Table 4. Assuming no treatment effect for severe hypoglycemia increased the ICER to $84,676 per QALY gained, but assuming a doubling of the severe hypoglycemia event rate for the first year using a hybrid closed-loop system and subsequent 95% reduction in rates had minimal impact ($39,375 per QALY gained). Halving the cost of hybrid closed-loop systems reduced the ICER to $10,794 per QALY gained. Assuming costs for Dexcom G6® will be the same as Dexcom G5®, and that t:slim X2™ and mylife™ YpsoPump® insulin pumps will retain similar costs when hybrid closed-loop systems using these brands of technology are commercially available in Australia, ICERs were $42,814 and $41,471 per QALY gained, respectively. Assuming only costs for pump consumables and Dexcom G5®, the ICER was $32,692 per QALY gained. Assuming that hybrid closed-loop therapy was commenced at 40 or 50 years of age, ICERs increased to $38,240 or $40,767 per QALY gained, respectively. Reducing the time horizon to 20 years, reducing discount rates, halving the cost or number of capillary glucose tests in standard care, assuming a baseline HbA1c of 7.0% (53 mmol/mol), or assuming no treatment effect on HbA1c had minimal impact on results.

Probabilistic sensitivity analysis. Black shading indicates where the high value of the parameter has been used, and white shading indicates that the low value of the parameter has been used.
Discussion
Use of a hybrid closed-loop system is likely to be cost-effective among adults with type 1 diabetes in Australia, based on a willingness-to-pay threshold of $50,000 per QALY gained when compared with MDI and SMBG. Furthermore, while people living with type 1 diabetes and higher baseline HbA1c have more to gain from advanced technology, sensitivity analyses indicated that ICERs with a baseline HbA1c of 7.0% (53 mmol/mol) remained below the willingness-to-pay threshold.
Regarding clinical variables, the model was most sensitive to rates of hypoglycemia. From literature searches, the reported incidence of severe hypoglycemia was approximately one event per person/year, but ranged from 0.35 to 4.9 events per person/year. 24 –27,42 Therefore, one event per person/year with normal hypoglycemia awareness was assumed, and a sixfold higher frequency of severe hypoglycemia was modeled for 19.5% of the population with impaired awareness of hypoglycemia. 23 While others have modeled closed-loop or low-glucose suspend systems as preventing all severe hypoglycemia over a lifetime, 43 –49 our model assumed a more conservative 95% reduction. The study by Benhamou et al. found that the hybrid closed-loop therapy group had five severe hypoglycemic episodes relating to human and system error over 24 weeks, compared with three episodes among those using sensor-augmented pump therapy. 29 Sensitivity analysis was therefore performed with twice as many episodes per person with severe hypoglycemia in the first year of hybrid closed-loop therapy compared with MDI and SMBG. While it is unlikely for hypoglycemia rates to double with hybrid closed-loop therapy in the first year, the resultant ICER of $39,375 per QALY gained suggests that even with significant initial deterioration in severe hypoglycemia, hybrid closed-loop systems are likely cost-effective in the long-term.
In addition, recent studies reported that reduction of nonsevere hypoglycemia with hybrid closed-loop therapy varies from 26% to 72%. 28,29,50 –55 Modeling a 53% relative reduction in nonsevere hypoglycemia 29 was therefore considered conservative for our cost-effectiveness analysis. Furthermore, in a sensitivity analysis that reduced the treatment effect for nonsevere hypoglycemia by 25%, hybrid closed-loop therapy remained cost-effective with a mean ICER of $42,039 per QALY gained.
While severe and nonsevere hypoglycemias were important clinical determinants of cost-effectiveness, results were most sensitive to the acquisition costs of technology. Indeed, CGM contributes to 54%–62% of the total annual costs of hybrid closed-loop systems. To explore the impact of acquisition costs further, different brands of technology in the hybrid closed-loop system were considered. The costs of different brands were based on listed retail prices of current-generation pumps and CGM systems, although costs for all brands of pump consumables were assumed to be equivalent to Medtronic because other brands' websites only reported subsidized costs to consumers. Actual costs to the government may be different when updated devices with closed-loop functionality become commercially available in Australia. Therefore, our results do not directly compare the different hybrid closed-loop systems, nor were analyses completed to assess for statistical significance of any differences between brands. Since all hybrid closed-loop systems were associated with ICERs below the willingness-to-pay threshold, it is our cautious conclusion that all these systems would likely be cost-effective if funded in Australia.
Sensitivity analyses were also performed regarding age and diabetes duration, given their important impact on cardiovascular risk. Assuming the baseline simulation cohort was 40 years of age with no vascular complications and that diabetes duration was 10 years had minimal impact on ICERs. Additional sensitivity analyses found that hybrid closed-loop therapy remained cost-effective despite slightly higher ICERs when the baseline simulation cohort was 18 years of age but hybrid closed-loop therapy was commenced at age 40 or 50 years. Furthermore, hybrid closed-loop therapy was cost-effective even over a time horizon of 20 years. This likely relates to reduced hypoglycemia, associated costs, and improved quality of life having a larger impact on cost-effectiveness than vascular complications over this shorter time-period. Together with our base-case findings, sensitivity analyses highlight the importance of minimizing exposure to dysglycemia by initiating hybrid closed-loop therapy as early as possible and not restricting funding to only younger age groups.
Regarding strengths of our economic evaluation, the CHEERS recommendations were followed and an expert multidisciplinary team was involved for model development and appraisal of face validity. 32 Costs and utilities were sourced primarily from Australia's largest cost of illness study regarding diabetes. 9 Furthermore, no industry support was provided as part of our research and we provide sensitivity analyses regarding multiple brands of technology.
We also acknowledge limitations of the available data sources and model assumptions. First, in common with almost all economic evaluations, long-term outcomes were projected from short-term clinical data. In the absence of RCTs investigating hybrid closed-loop systems compared with MDI and SMBG, conservative estimates of treatment effect on HbA1c and hypoglycemia were utilized based on the available data comparing these systems to insulin pumps or sensor-augmented pump therapy. The utilization of generalized costs for modeled health states rather than costs for individual complications was another limitation. Furthermore, the modeled treatment effects were not specific to any closed-loop algorithm, although for the base-case, retail prices were utilized for the only commercially available hybrid closed-loop system in Australia (Medtronic MiniMed™ 670G).
Uncertainty was addressed through deterministic and probabilistic sensitivity analyses. Variability of the ICER was reflected by 95% confidence intervals in the base-case, and the probability of cost-effectiveness was presented as a cost-effectiveness acceptability curve. Deterministic analyses demonstrated which key input parameters impacted variation of the ICER, however, additional confidence intervals could not be provided.
Finally, not all scenarios relevant to clinical practice could be adequately addressed through sensitivity analyses. For example, models are currently unable to fully capture the impact of personal preference for technology as part of the treatment effect, or the economic impact of ceasing and changing technology types over a lifetime in the absence of relevant data sources.
There have been very few economic evaluations regarding hybrid closed-loop therapy. One study suggested that hybrid closed-loop systems were cost-effective in comparison with the already expensive comparator of insulin pump therapy with SMBG in Sweden. 43 However, we believe ours is the first cost-effectiveness analysis of a hybrid closed-loop system in comparison with the standard of care comprising MDI with SMBG. Prior economic evaluations of diabetes management technologies reported that key determinants of cost-effectiveness usually comprise worse baseline glycemic control and larger treatment effects. 56 Therefore, our finding that hybrid closed-loop therapy remained cost-effective compared with MDI and SMBG in sensitivity analyses with baseline HbA1c of 7.0% (53 mmol/mol), no treatment effect on HbA1c, or only conservative improvements in hypoglycemia support our base-case findings.
Conclusions
Hybrid closed-loop systems are likely cost-effective when compared with the current standard of care by reducing HbA1c and the incidence of hypoglycemia among adults with type 1 diabetes in Australia.
Footnotes
Author Contributions
A.P., D.L., and S.Z. conceived the study. A.P., D.L., E.Z., G.S., S.Z., and Z.A. designed the study. A.P. created the model with multidisciplinary input from A.E., D.L., E.Z., G.S., S.Z., and Z.A. A.P. wrote the first draft of the article. A.P., A.E., D.L., E.Z., G.S., S.Z., and Z.A. interpreted the data and contributed to the writing of the final version of the article. All authors agreed with the results and conclusions of the article. S.Z. is the guarantor and affirms that the article is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Author Disclosure Statement
A.P., A.E., G.S., and Z.A. report no conflicts of interest.
All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare no support from any organization for the submitted work. Outside the submitted work, E.Z. has received grants from Amgen, AstraZeneca, Pfizer, and Shire, and has received personal fees from Pfizer. D.L. has received grants from AstraZeneca, Pfizer, AbbVie, and Bristol Myer Squibb, and has received personal fees from AstraZeneca, Astellas, and Bayer outside the submitted work. S.Z. reports participation in advisory boards, expert committees, or educational meetings outside the submitted work on behalf of Monash University for Boehringer-Ingelheim, Eli Lilly, Sanofi, AstraZeneca, Novo Nordisk, and MSD Australia (payment to institution). There are no other relationships or activities that could appear to have influenced the submitted work.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.