
Abstract
Background:
Gestational diabetes mellitus (GDM) management using self-monitoring blood glucose (SMBG) does not normalize pregnancy outcomes.
Objective:
We aimed to conduct an observational study to explore if continuous glucose monitoring (CGM) could identify elevated glucose levels not apparent in women with GDM managed using SMBG.
Study Design:
A 7-day masked-CGM (iPro; Medtronic) was performed within 2 weeks of GDM diagnosis, immediately post-GDM education, but before insulin commencement as determined by SMBG. CGM data regarding hyperglycemia (sensor glucose >126 mg/dL [06:00–00:00 h] and >99 mg/dL [00:00–06:00 h] for >10% of time), time with health care professionals, treatment, and pregnancy outcome were collected. Comparisons (Mann–Whitney test) were performed between subjects subsequently commenced on insulin versus those continued with diet and lifestyle measures alone.
Results:
Ninety women of mean (standard deviation) gestational age weeks 27(1) were studied. Those prescribed insulin (n = 34) compared with those managed with diet and lifestyle alone (n = 56) had a greater time in hyperglycemia (P = 0.0001). Of those not prescribed insulin, 35/56 (61%) breached CGM cutoffs between 00:00 and 06:00 h; 11/56 (20%) breached 6.00–00.00 h CGM cutoffs for >10% of the time; and 21/45 (47%) with optimal CGM glucose levels during the daytime spent >10% time in hyperglycemia between 00.00 and 06:00 h. In contrast, SMBG measurements exceeded the clinical targets of <120 mg/dL postdinner in 5.4% and <100 mg/dL fasting in 0% of the subjects.
Conclusions:
CGM provides a more comprehensive assessment of nocturnal hyperglycemia than SMBG and could improve targeting of interventions in GDM. Larger studies to better define CGM targets are required, which once established will inform studies aimed at targeting nocturnal glucose levels.
Introduction
Glycemic management, the focus of gestational diabetes mellitus (GDM) management, reduces adverse fetal outcomes. 1 Insulin therapy is a cornerstone of management when glucose levels remain above target despite diet and lifestyle optimization. The decision to initiate insulin therapy in women with GDM is determined by the health care professional's (HCP) perception of the patient's glycemia following review of self-monitoring blood glucose (SMBG) measurements. However, interventions to optimize glycemia do not normalize outcomes in GDM despite care in accordance with current guidelines. Even with care consistent with current standards, data indicate that 13% of GDM pregnancies result in large for gestation (LGA) babies. 2
We hypothesized that continuous glucose monitoring (CGM) is more comprehensive in its assessment of daily hyperglycemic excursions than SMBG and thus will better inform the need for treatment with insulin aimed at preventing fetal overgrowth. A more effective assessment of glycemia may identify those at greater risk for adverse pregnancy outcomes, enabling more efficient triage and targeted management.
It was our objective to conduct an observational study in women with GDM to identify patterns of hyperglycemia, not apparent with SMBG, using masked-CGM performed shortly after the 24–28-week oral glucose tolerance test (OGTT). We also wished to explore if CGM was more effective than OGTT in predicting subsequent demands during pregnancy on HCP resources, thereby informing a more efficient allocation of limited resources.
Materials and Methods
This was an observational cohort study (ANZCTR:12618000050257) of women diagnosed with GDM between 24 and 28 weeks gestation using IADPSG criteria 3 who were attending two university affiliated Melbourne obstetric centers. The Werribee Mercy Hospital is a regional hospital delivering about 3800 babies each year. The Mercy Hospital for Women is a tertiary center delivering about 5600 babies each year. The study received approval by the Mercy Hospital HREC (ID: 2017-039) on the 10th October 2017 and was conducted in accord with the Declaration of Helsinki. The first subject was consented in December 2017 and the final subject completed the study in March 2019.
All subjects were provided with dietary and lifestyle advice and taught SMBG at the first education session conducted within 2 weeks of GDM diagnosis. Given the time-critical considerations associated with pregnancy and the nature of these interventions, the expectation was that they would be implemented and would have effect immediately (unlike insulin titration which may take some time) in this motivated group.
All SMBG data were available to guide clinical interventions as per institutional protocols. On the same day, following the education session, written informed consent was obtained, and a 7-day CGM (iPro™; Medtronic, Northridge, CA), calibrated by SMBG, was initiated. CGM and glucose meter data (Accu-Chek Guide; Roche Diabetes Care Australia, Bella Vista, NSW, Australia) were uploaded at the end of the monitoring period for analysis. All CGM data were masked to treating clinicians and participants and data from CGM were not used at any stage to guide clinical intervention. Insulin was not initiated in the week immediately following the initial education session when the CGM data were collected.
Women with preexisting diabetes, GDM diagnosed before 24 weeks gestation, or with major medical comorbidities requiring intensive clinical follow-up independent of glycemic control were excluded. Demographic data regarding age, ethnicity, parity, height, weight, and body mass index (BMI) were collected at recruitment. All participants were managed as per the hospitals' standard clinical guidelines to achieve SMBG targets (fasting glucose <100 mg/dL and 2 h postmeal <120 mg/dL). The women had one session for education regarding lifestyle, diet, and glucose monitoring. Education was standardized across the two sites.
All participants were counseled to eat three meals and three snacks and to avoid refined carbohydrates and were advised to walk 10–15 min after each meal. All participants were provided with a diary and requested to record the diet during the week of the CGM. All subjects were requested to monitor at least four times a day and insulin was initiated if they breached the SMBG target approximately three times a week despite diet and lifestyle. Time spent in face-to face interactions with HCPs was collected during each clinic visit. At the end of pregnancy, clinical outcomes, including gestational age at delivery and birthweight, were collected.
Statistics
Continuous variables are presented as median with interquartile range and compared using the Mann–Whitney test. Chi-square test was used to compare the categorical variables. Pearson correlation coefficients were used to quantify associations between CGM parameters and HCP time or OGTT parameters. All analyses were performed using GraphPad Prism Version 8.3 (GraphPad Software, La Jolla, CA). P-values <0.05 were considered significant. For CGM data analysis, glucose targets of <126 mg/dL during the day and <99 mg/dL during the night were used. 4,5 We included participants who had seven consecutive days of data with at least 80% coverage. All CGM values above the thresholds were included in the calculation of the time (in minutes) spent in hyperglycemia during the daytime and the night-time. The CGM data were averaged over 7 days. Daytime was defined as 06:00–00:00 h and night-time as 00:00–06:00 h. 6
Results
CGM data were available for 100 subjects. Ten subjects were excluded because CGM data did not meet the minimum requirements, and 90 subjects (mean ± standard deviation) age 32 ± 4 years; gestational age 27 ± 1 weeks; and BMI 30.2 ± 4.9 kg/m2 at recruitment were included in the analysis (Table 1). None of the subjects was a night shift worker. All subjects recorded their diet during the week of CGM use and their last snack was usually before 21.00 h with none of the subjects reporting their last snack beyond 22.00 h. Thirty-one (34%) were Caucasian; 30 (33%) South Asian; 19 (21%) Southeast Asian; 6 (7%) Middle East; 3 (3%) Samoan; and 1 (1%) African. BMI, fasting OGTT glucose, SMBG, and CGM parameters defining hyperglycemia were greater for the 34 (38%) subjects prescribed insulin (Group 1) compared with the 56 (62%) subjects who managed with diet and lifestyle measures alone (Group 2). As a predictor of future HCP resource utilization, masked-CGM parameters did not correlate with HCP-time spent with the subject, nor did dysglycemia on OGTT. The strongest predictor of HCP-resource utilization was the requirement for insulin, which in turn correlated with multiple CGM parameters and fasting glucose on OGTT (Table 2).
Demographics of All Study Subjects
BMI, body mass index; CGM, continuous glucose monitoring; GMI, Glucose Management Indicator; HCP, health care professional; OGTT, oral glucose tolerance test; SMBG, self-monitoring blood glucose.
Comparison of Subjects Prescribed Insulin and Not Prescribed Insulin
Bolded P-values represent significance of P < 0.05.
In Group 2, 35/56 (61%) of subjects breached the night-time CGM glycemic target for >10% time and 11/56 (20%) breached the daytime target. When CGM data points from all subjects in Group 2 were pooled and analyzed, 20% of these data points during the night-time and 6% during the daytime exceeded the respective CGM cutoffs. Majority of the exposure to hyperglycemia occurred between 00:00 and 03:00 h (Fig. 1). In addition, 21/45 (47%) of the Group 2 subjects with <10% of time in hyperglycemia during the daytime spent >10% time in hyperglycemia between 00.00 and 06:00 h. In contrast, the postevening meal SMBG measurement exceeded the clinical target of <120 mg/dL in 5.4% of the subjects with none exceeding the prebreakfast (fasting) target of <100 mg/dL.
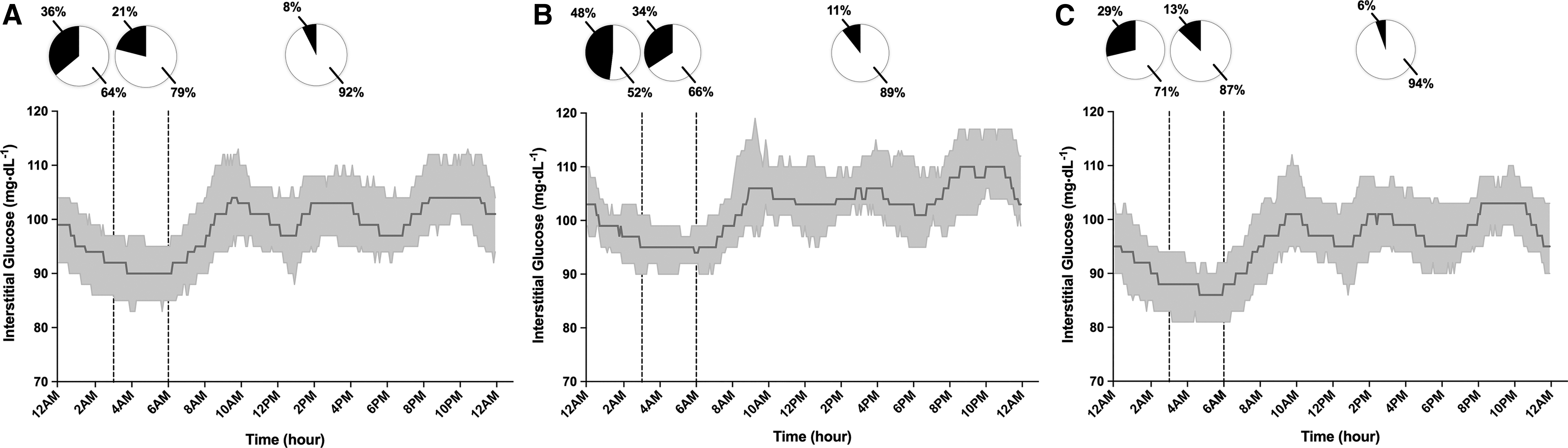
Pooled CGM data points during the daytime (06.00 to 00.00 h), early night-time (00.00–03.00 h) and late night-time (03.00–06.00 h) for:
None of the participants had premature delivery. There were five cases of mild neonatal hypoglycemia. None of these five babies required Neonatal Intenstive Care Unit (NICU) admission; one of these five was LGA. Three of the five mothers of babies with neonatal hypoglycemia required insulin during pregnancy and two required delivery by cesarean section. There were four mothers who suffered a postpartum hemorrhage, all of whom had vaginal deliveries. Two of these four mothers required insulin during pregnancy. One study participant was treated with metformin in addition to insulin. She delivered a LGA baby by cesarean section at 38 weeks.
There were seven (7.8%) LGA babies with 2/7 prescribed insulin. Of the 5/7 mothers with LGA babies who were not prescribed insulin, 3/5 breached the overnight glycemic cutoff >10% of the time. There were no neonatal deaths.
Discussion
Principal findings
Using masked-CGM profiles as a benchmark we evaluated, in a cohort of women with GDM, the clinical decision to initiate insulin therapy by the HCP based upon glucose information provided by SMBG. The masked-CGM data revealed nocturnal hyperglycemia in those who were not commenced on insulin, with 60% of subjects breaching glucose targets overnight for >10% time. The SMBG measurement following the evening meal usually occurred between 7:00pm and 10:00pm and this blood-glucose measurement at a single time-point would have provided only a limited insight into overnight hyperglycemia as would the prebreakfast reading.
This was reflected in our observation that the postdinner and prebreakfast SMBG readings exceeded the therapeutic thresholds in only 5.4% and 0% of readings, respectively, in those women who were not commenced on insulin. In addition, our observation that nocturnal and daytime hyperglycemia correlated poorly implies that SMBG measurements (performed while awake) provide only limited insight into nocturnal glucose elevations. HCP-time spent with their patients is assumed to reflect, in part, the medical team's perception of the patient's glycemic control. These HCP perceptions based upon SMBG readings (as CGM data in this study were not available to the HCP) determined the need to commence insulin, which in turn would have influenced the time devoted to the care of the patient by the HCP team.
The incidence of LGA (8%) was relatively low in our cohort of women compared with the incidence LGA reported in GDM (13%) by others. 2 Contributing factors may have been the exclusion of women with abnormal glucose levels detected in early pregnancy and the relatively mild elevations overall in the subjects' glucose with the 28 week OGTT. It is of interest that five of the seven subjects with LGA babies were not commenced on insulin, and of these, three breached nocturnal glycemic thresholds for >10% of the time.
Results in context
The Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) study found that there is a continuous linear relationship between maternal glucose and newborn adiposity, 7 suggesting that glucose levels in GDM need to be maintained as close as possible to those in healthy women. While an expert group has advised a target range of 63–140 mg/dL for GDM without distinguishing day- versus night-time targets and without a % of time in that range assigned because of lack of data, it should also be recognized that this recommendation represents a consensus of expert opinion rather than the outcome derived from an evidence base. 8
A systematic review of pooled normal pregnancy glucose data from studies conducted in the USA and Europe showed fasting glucose of 70 ± 7 mg/dL, 1 h postprandial glucose of 108 ± 13 mg/dL, 2 h postprandial glucose of 99 ± 10 mg/dL, and 24 h mean of 88 ± 10 mg/dL with little heterogeneity across studies. 4,9 Harmon et al. observed that in healthy normal weight subjects 95% of CGM glucose values were <117 mg/dL during the third trimester with glucose in healthy obese pregnant women about 9 mg/dL higher than normal weight pregnant women in fasting and postprandial states. 5 Given the increased BMI of our cohort, we therefore elected to use the conservative CGM glucose cutoffs <99 mg/dL overnight and <126 mg/dL during the day to ensure that we only classified as hyperglycemic those women who clearly breached the healthy glucose thresholds.
Our observations regarding the incidence of LGA babies in the context of the glycemic cutoffs described above are consistent with the report by Law et al. 10 who used CGM performed at 30–32 weeks' gestation in subjects with GDM and identified significantly higher overnight glucose in mothers of LGA infants.
Clinical implications
CGM provides a unique insight into magnitude and duration of daily glucose fluctuations. We have previously assessed the role of CGM in clinical decision-making in diabetes in pregnancy. 11 Studies have since reported improved neonatal outcomes with the use of CGM in pregnancy with GDM 12 and type 1 diabetes. 13 Our data suggest that the majority of nocturnal hyperglycemia occurs during the first half of the night implying delayed clearance of the evening meal as the major underlying mechanism rather than the diurnal variation in cortisol levels. The impact of bedtime intermediate-acting insulin versus long-acting insulin analogs on nocturnal hyperglycemia in CGM would be worth testing in a future study.
Research implications
We have proposed a set of CGM cutoffs based on previous studies, 4,5,9 with goals set differently for night-time and daytime ranges. Further studies are required to determine the incidence of LGA and other pregnancy-related outcomes in a larger cohort of GDM patients, which would help better define the correct CGM targets. Once these cutoffs have been established, interventions aimed at targeting these nocturnal glucose levels will need to be formally tested against outcomes.
Strengths and limitations
The strength of these data is that a broad spectrum of the obstetric population participated in this study conducted by two public hospitals (tertiary and regional). The protocol mandated that CGM data collection was implemented posteducation provision and before insulin initiation to ensure that the glycemic profiles reflected the impact of any dietary and lifestyle modification aimed at optimizing glycemia before consideration of insulin therapy. Glycemic targets were identical at the two participating centers ensuring that interventions were aligned. The study design whereby the obstetric and diabetes teams were not able to access the traces ensured that the CGM data did not influence clinical decisions. CGM data integrity was ensured by using globally accepted standards 7 applied to determine if the data were suitable for inclusion.
Study weakness includes the small sample size. While we provide comment on LGA, the study was not powered to definitively explore the relationship between CGM and LGA. In addition, we acknowledge that the cutoffs used in ours study are arbitrary and future larger studies will be needed to verify the validity of these CGM cutoffs determining intervention. Also, study sites were well resourced and attached to universities. Therefore, implementation of clinical care, while mainstream, may not be representative of all obstetric centers.
SMBG-based glycemic targets in pregnancy have not been universally agreed upon and the targets used in this study to determine insulin initiation may differ from those used elsewhere. Finally, data collected regarding HCP time spent with the participants was restricted to face to face interactions. We accept that current models of care also incorporate telehealth technologies.
Conclusions
CGM by providing a better assessment of nocturnal hyperglycemia than SMBG may facilitate the triage of patients and effective intervention.
Footnotes
Acknowledgments
We gratefully acknowledge diabetes antenatal care team at Mercy Public Hospitals, particularly Rachel Miller, Anna Peters, Jinyang Jin, and Karen Moulton for their invaluable support in conducting the study. We thank Dr. Robert Vigersky of Medtronic for comments regarding the article. We thank the pregnant women attending Mercy Public Hospitals who participated in the study. Trial Identification Number: ANZCTR:12618000050257 (
Author Disclosure Statement
D.N.O. has received research support from Novo-Nordisk and Medtronic. O.C. serves as the Medical Affairs Director—Medtronic Diabetes EMEA. No other potential conflicts of interest relevant to this article. All other authors report no disclosures.
Funding Information
This investigator-initiated study was supported by funds from Mercy Hospitals with material support Medtronic Australasia Pty. Ltd. The funding bodies had no role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.