
Abstract
Objectives:
The objective of this population-based study was to identify factors associated with insulin pump therapy initiation in adults with insulin-requiring diabetes in France in 2015.
Method:
People with insulin-requiring diabetes and their characteristics were identified from the national health data system. Factors associated with insulin pump therapy initiation were identified by logistic regression analysis.
Results:
The study focused on 614,913 adults with diabetes treated by multiple daily injections before 2015: 4083 of them initiated insulin pump therapy during the year (71% of them had type 1 diabetes, T1D). Factors associated with insulin pump therapy initiation were the number of consultations with an endocrinologist within the past 2 years (2 vs. 0, odds ratio [OR] = 1.5, P < 0.01), the presence of a chronic cardiovascular or neurovascular disease (OR = 1.6 for T1D, OR = 1.3 for type 2 diabetes [T2D], P < 0.01) and treatment with antidepressants/anxiolytics (OR = 1.2 for T1D, OR = 1.4 for T2D, P < 0.01). The other determinants were female gender (OR = 1.5, P < 0.01) and history of hospitalization for acute metabolic complications (OR = 1.14, P < 0.01) in T1D. Factors associated with less insulin pump therapy initiation were age, duration of diabetes, end-stage renal disease, and social deprivation (OR = 0.662, P < 0.01, T1D only).
Conclusion:
Predictive factors of insulin pump therapy initiation in people with insulin-requiring diabetes in 2015 in France were globally consistent with clinical practice guidelines. Age, male gender, and social deprivation are still associated with a lower rate of insulin pump therapy initiation in adults with T1D.
Introduction
Five percent of the population covered by the French national health insurance general scheme and local mutualist section (LMS), that is, 2.9 million people (calculation based on national health data system) received drug treatment for diabetes in 2016. This treatment represented 15% of all reimbursed expenditure of people with diabetes (whether related to diabetes or not) paid by these compulsory health insurance schemes in 2012, that is, €19 billion. According to a study conducted by the French national health insurance, 1 25% of people treated with diabetes medication are treated with insulin and this proportion increased by 2 percentage points between 2012 and 2015.
In this context, also marked by the arrival of new products (medications and medical devices), often presented as being innovative and actually more expensive, it seemed important to further our knowledge concerning the use of insulin therapy in France. This is an essential prerequisite to propose actions designed to improve the quality of management and follow-up of people with insulin-requiring diabetes, as well as the efficacy of the expenditure in this field.
According to Système National des Données de Santé (SNDS) [National Health Data System] data, the prevalence of insulin pump therapy among general scheme beneficiaries with diabetes was 3.4% in 2015, with a prevalence of 8.4% in the subgroup of people with type 1 diabetes (T1D). In 2017, this prevalence was 21% of all health insurance scheme beneficiaries with T1D (unpublished French health insurance data).
Many studies have compared the efficacy of external insulin pump therapy and multiple daily injections (MDI), and have demonstrated improvement of blood glucose control in favor of insulin pump therapy. 2 –6 In people with T1D, not only insulin pump therapy is associated with a decreased incidence of hypoglycemia, but also lower HbA1c levels compared with patients treated with MDI. 7 –10 However, other studies have found no differences in glycemic control and highlight the primary importance of patient choice. 11 Insulin pump therapy is used less often in people with type 2 diabetes (T2D) requiring insulin, although several studies have demonstrated the efficacy of this device in terms of reduction of HbA1c levels. 3,4,10,12,13 Moreover, use of an external insulin pump also allows greater flexibility and freedom of the patient's lifestyle compared with MDI. 14
Few studies have been conducted in France to identify the determinants of the choice between these two modalities of insulin therapy. This study tried to address this issue by using the SNDS, one of the largest medical administrative databases in the world, comprising all reimbursement data for the French population. The comprehensive nature of the data allows studies on management strategies concerning specific diseases such as diabetes.
Methods
Data
The French health care system is a social insurance system. Public insurance is compulsory and covers the resident population; it is financed by employee and employer contributions and taxation. This public insurance is supplemented by a private complementary insurance system. 15 The data used in this study combined office care reimbursement data, public and private hospitalization data, cash benefits, and certain individual clinical and sociodemographic data concerning the beneficiaries reimbursed for these various forms of health care. 16
These data consist of unsampled French administrative data. The SNDS covers almost the whole French population and not simply population subgroups. The Caisse Nationale d'Assurance Maladie has used these data to develop medical algorithms that can be used to characterize the health status of national health insurance general scheme beneficiaries. These algorithms are based on hospitalizations, drugs dispensed, and long-term diseases scheme, the so-called French Affection de Longue Durée (ALD) [long-term disease] scheme. ALD status allows the management of patients with a chronic disease requiring long-term and particularly expensive treatment. A list established by decree allows for co-payment exemption (100% reimbursement) for health care related to the disease indicated on this ALD list. This medicalized analysis allows a summary description of the management of various diseases. Main diagnoses (MD), related diagnoses (RD), or associated diagnoses (AD) of hospital stays, ALD diagnoses and drugs are used in most of the algorithms used to constitute disease groups.
Identification of the study population
The study was conducted on data concerning general scheme beneficiaries (including SLM), living in France (overseas departments and regions [DROM] and metropolitan France) with at least one health care reimbursement in 2015. People with insulin-requiring diabetes were identified in 2015 and health care utilization data were extracted from the database since 2006.
People with diabetes for whom diabetes medications were dispensed at least three times in 2014 or 2015 (or dispensed at least twice when at least one large pack was dispensed), or with ALD diabetes co-payment exemption in 2015 or who had been hospitalized for diabetes or a complication of diabetes in 2014 or 2015 were selected. Diabetes medications were class Anatomical Therapeutic Chemical (ATC) Classification A10 drugs (drugs used in diabetes).
People with insulin-requiring diabetes were defined as the population of interest. This population was composed of people to whom insulin had been dispensed at least three times on different dates in 2015. Women hospitalized for gestational diabetes in 2015 were excluded from the study.
As people with type 1 (T1D) or type 2 (T2D) insulin-requiring diabetes have very different characteristics, these two types of patients, therefore, had to be distinguished. Based on an expert opinion and on a previous publication, we have chosen an age criterion to distinguish the two types of diabetes. 17 A person satisfying at least one of the following conditions was considered to have T1D: <45 years in 2015, <45 years at the time of first dispensing of insulin, or <45 years at the time of granting ALD status for diabetes. A person was considered to have T2D, when he/she was at least 45 years old in 2015 and did not satisfy the age criterion for the date of first dispensing of insulin and ALD status for diabetes. On the basis of these criteria, we obtained 160,000 T1D patients and 470,000 T2D patients. People treated by implantable insulin pump were excluded from the study because they present very specific characteristics and because of their small numbers (14 newly treated individuals in 2015). 18
Finally, people were also distinguished according to the modality of insulin administration: individuals initiating external insulin pump therapy versus individuals treated exclusively with MDI on the basis of the medical devices reimbursed for the period 2006–2017.
In summary, people with insulin-requiring diabetes were initially identified. Among these people, T1D and T2D patients were distinguished according to the criteria defined earlier. Two subgroups were then created within each of these two groups, according to the modality of insulin administration (external insulin pump and MDI) and these two subgroups constituted the study population (Fig. 1).
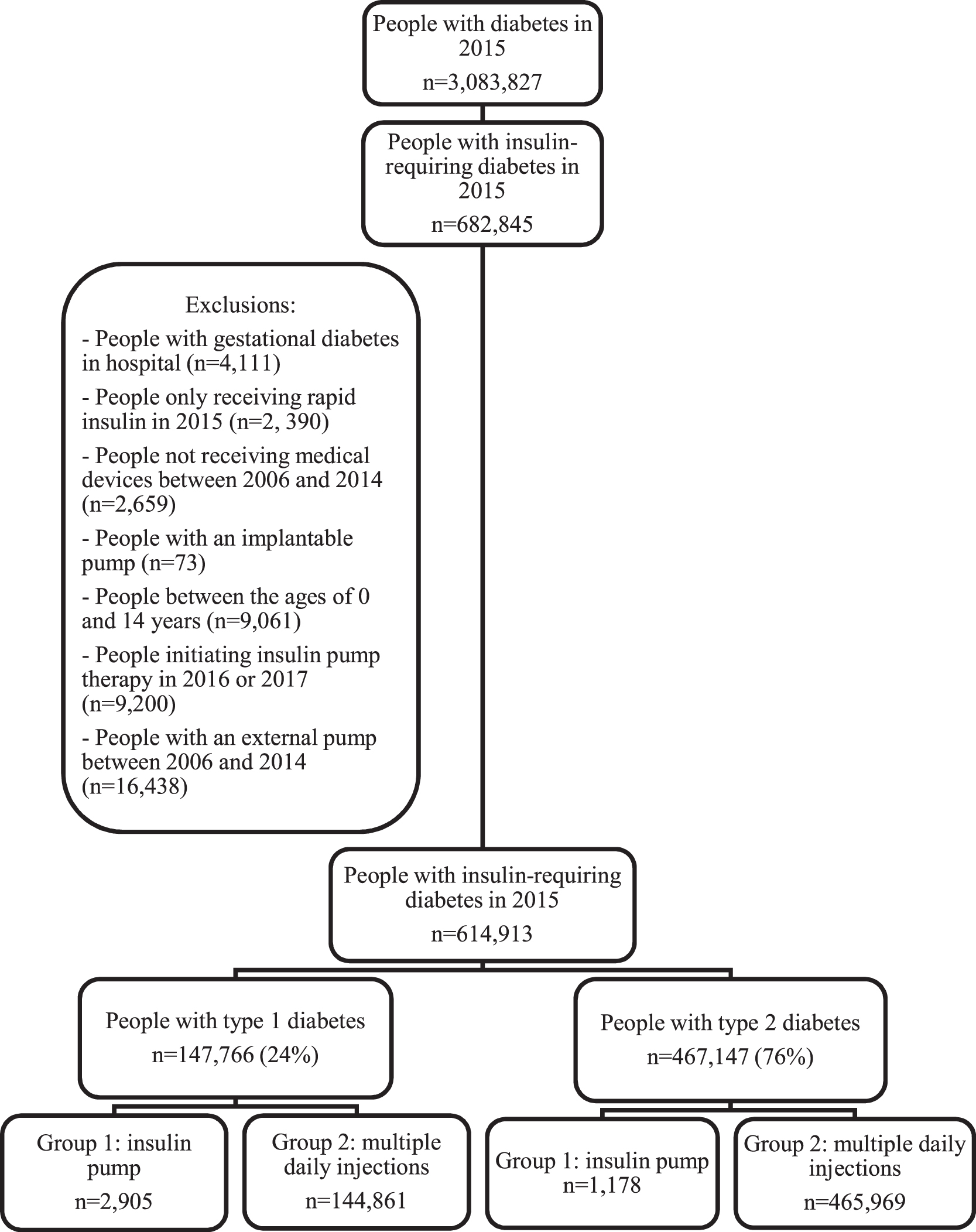
Study population flowchart.
Statistical analysis
The purpose of this study was to identify factors associated with initiation of insulin pump therapy by means of logistic regression analysis. The variable to be explained was the initiation of insulin pump therapy in 2015 versus MDI continuation. The following explanatory variables were introduced into the model: age (various age-groups according to the type of diabetes), gender, universal complementary health insurance (CMU-c) plan for people <60 years, social deprivation index, region of residence, reimbursable expenditure in 2014, frequency of endocrinologist consultations during the 2 years before initiation of insulin pump therapy or other medical devices, duration of diabetes and/or insulin therapy (according to the type of diabetes considered), and presence of comorbidities (chronic cardiovascular and neurovascular diseases in 2015, history of acute metabolic complications, end-stage renal disease, and mental illness and/or use of antidepressants/anxiolytics). Low-income people ≥60 years are generally eligible for a voucher plan for the purchase of complementary health insurance (ACS), as their income is slightly higher than the CMU-c income threshold.
The SNDS comprises only limited individual sociodemographic characteristics. However, we used a social deprivation index and the CMU-c variable as proxies for socioeconomic status. The social deprivation index is calculated for the town of residence and is constructed from data concerning taxable income, the proportion of people with a baccalaureate or higher degree, the proportion of manual workers and unemployed people in the working population. 19 The CMU-c is a free universal complementary health insurance plan designed to facilitate access to care of low-income people regularly and stably living in France. 15,20 The “frequency of endocrinologist consultations” variable was calculated from office visits, outpatient department visits, and consultations during hospitalization for diabetes or a complication of diabetes.
To assess variables related to comorbidities of diabetes, a history of acute metabolic complications included diabetic coma, ketoacidosis, drug-induced hypoglycemia without coma, and other types of hypoglycemia was identified by ICD-10 codes. Mental illness was defined by medical algorithms as psychotic, neurotic and mood disorders, manic and bipolar disorders, depression and other mood disorders, mental deficiency, addictive disorders, behavioral and emotional disorders with onset usually occurring in childhood and adolescence and other mental illnesses. Mental illness was identified by ALD or hospitalization diagnoses. The use of antidepressants/anxiolytics was defined by at least three dispensings of these drugs in 2015.
The association between external insulin pump therapy and explanatory factors is presented in the form of crude and adjusted odds ratios.
A linear regression model was used to determine a possible correlation between the incidence of initiation of insulin pump therapy in the T1D population and the density of endocrinologists by department.
Finally, a sensitivity analysis was conducted on people initiating insulin pump therapy in 2015 to confirm the validity of the criteria used to distinguish between T1D and T2D.
SAS software version 9.4 was used for statistical analysis.
Results
Description of the study population
The flowchart describing selection of the study population from SNDS data is presented in Figure 1. The characteristics of the study population are presented in Tables 1 and 2.
Age Distribution in People Initiating Insulin Pump Therapy Versus People Staying Under Multiple Daily Injections, by Type of Diabetes
For each age-group: number of patients and percentage of the study group (pump initiation or multiple daily injections) are given.
T1D, type 1 diabetes; T2D, type 2 diabetes.
Descriptive Statistics of the Characteristics of Patients Treated by Insulin Pump Versus Multiple Daily Injections
Interpretation: 45.3% of people with T1D initiating treatment with insulin pump were men.
CMU-c: public complementary health insurance for French resident with low income.
Frequency of endocrinologist consultations during the 2 years preceding initiation of insulin pump therapy or during the 2 years preceding the first dispensing of medical devices in 2015.
In 2015, 2905 people with T1D initiated external insulin pump therapy versus 1178 people with T2D.
People with T1D initiating insulin pump therapy in 2015, compared with those continuing to be treated with MDI, were predominantly women (55%), younger (37 years vs. 46 years), less frequently CMU-c beneficiaries (12% vs. 16%), with a shorter mean duration of diabetes (11 years vs. 14 years), and a higher mean number of endocrinologist consultations during the 2 years preceding initiation of insulin pump therapy (3 vs. 2). They presented fewer comorbidities, with the exception of a history of acute metabolic complications (30% vs. 20%).
People with T2D initiating insulin pump therapy in 2015, compared with those continuing MDI, were predominantly men (53%), younger (63 years vs. 72 years), 60% of whom had a history of insulin therapy ranging between 6 and 10 years (vs. 57% for people treated with MDI), a greater number of endocrinologist consultations during the previous 2 years (4 vs. 2), more often presented mental illness or chronic treatment related to mental health, and more often presented a history of acute metabolic complications (13% vs. 10%).
Analysis of factors associated with initiation of insulin pump therapy in 2015
The results of univariate and multivariate analysis of the association between initiation of insulin pump therapy in 2015 and baseline patient characteristics are presented in Table 3.
Probability of Initiation of External Insulin Pump Therapy Versus Multiple Daily Injections (Univariate and Multivariate Analyses)
Interpretation: Women with T1D had a 1.54-fold higher probability of initiating insulin pump therapy compared with men, all other things being equal. * P < 0.05; ** P < 0.01.
Variable not selected at the limit of 5% by the STEPWISE method.
Other variables added to the model were not selected by the STEPWISE method: social deprivation index and acute cardiovascular and neurovascular disease.
CMU-c: public complementary health insurance for French resident with low income.
Frequency of endocrinologist consultations during the 2 years preceding initiation of insulin pump therapy or during the 2 years preceding the first dispensing of medical devices in 2015.
The frequency of endocrinologist consultations during the previous 2 years was positively associated with the probability of initiating insulin pump therapy in 2015. The absence of an endocrinologist consultation during the previous 2 years markedly decreased the probability of initiating insulin pump therapy compared with an individual who had consulted an endocrinologist at least once for the same period, regardless of the type of diabetes. Moreover, a linear relationship was observed between the number of endocrinologist consultations and the probability of initiating insulin pump therapy. In contrast, patients who had not consulted an endocrinologist during the previous 2 years had an 8-fold (T1D) and a 11.5-fold (T2D) lower chance of initiating insulin pump therapy in 2015 than patients who had consulted an endocrinologist at least once (reference category). The first prescriber was a salaried physician in 88% of cases and a private physician in 12% of cases.
The probability of initiating insulin pump therapy decreased with the patient's age, regardless of the type of diabetes. People with T1D between the ages of 15 and 24 years had a 9.5-fold higher probability of initiating insulin pump therapy than people with T1D, who were ≥65 years.
The probability of initiating insulin pump therapy was 1.5-fold higher for women than for men with T1D, but this was not the case for people with T2D, in whom gender was not significantly associated with initiation of insulin pump therapy.
The probability of initiating insulin pump therapy also decreased when diabetes had been diagnosed for >2 years, regardless of the type of diabetes. The odds ratio subsequently remained stable despite the increasing number of years with diabetes.
In contrast with the duration of diabetes, the duration of insulin therapy in people with T2D was a positive predictive factor for initiation of insulin pump therapy. People with T2D who had been treated by insulin for between 6 and 10 years had a 2.2-fold higher probability of initiating insulin pump therapy than people who had been treated by insulin for between 0 and 2 years.
In people with T2D, the presence of antidepressant/anxiolytic treatment with no identified mental illness (ALD or hospitalization diagnosis) was associated with a 1.4-fold higher probability of initiating insulin pump therapy compared with people with no mental illness and no chronic antidepressant/anxiolytic treatment. A less marked effect was observed in people with T1D. In contrast, the presence of an identified mental illness was significantly associated with a lower incidence of initiation of insulin pump therapy among people with T1D.
The presence of a history of chronic cardiovascular or neurovascular disease in people with T1D or T2D was associated with a 1.6- and 1.3-fold higher probability, respectively, of initiating insulin pump therapy versus the absence of cardiovascular or neurovascular disease. In contrast, the presence of end-stage renal disease was a negative predictive factor for initiation of insulin pump therapy in 2015 in people with either T1D or T2D.
In people with T1D, a history of at least one episode of acute metabolic complications (diabetic coma, diabetic ketoacidosis) before 2015 was associated with a 1.1-fold higher probability of initiating insulin pump therapy compared with people with no history of acute metabolic complications.
In terms of socioeconomic variables, the absence of a CMU-c plan among people with T1D was associated with a 1.5-fold higher probability of initiating insulin pump therapy compared with people with CMU-c plan.
Geographic variations in incidence rate
The map of France of the incidence of insulin pump initiation in patients with T1D in 2015, by department, is given in Figure 2 and the France map of the medical density of practitioners specializing in endocrinology and diabetology in 2015 is given in Figure 3.
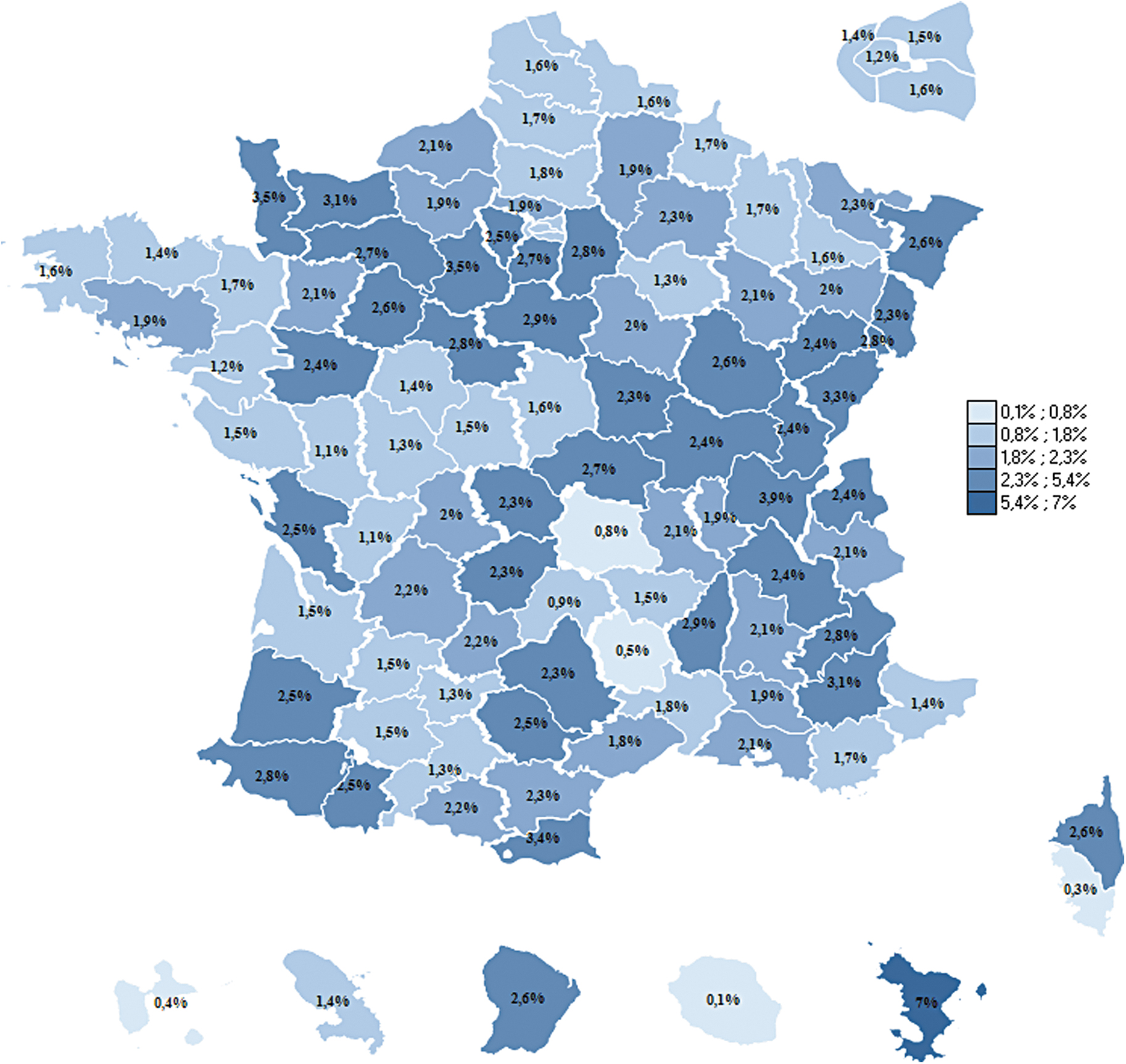
Departmental incidence (%) of initiation of external insulin pump therapy in the T1D population in 2015. T1D, type 1 diabetes.
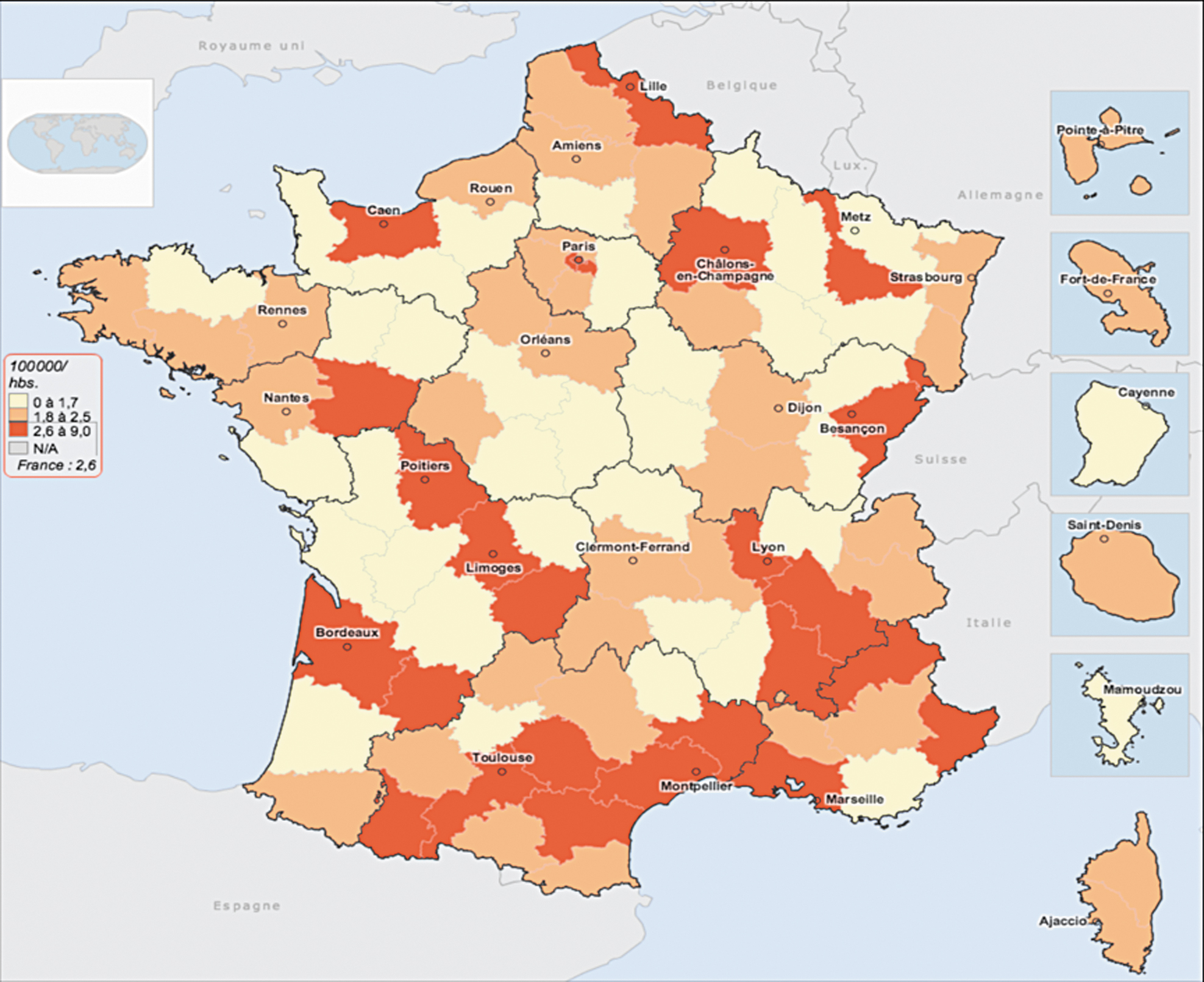
Departmental density of endocrinologists (all types of practice) in France in 2015 (per 100,000 inhabitants) based on Conseil National de l'Ordre des Médecins (French medical board) data (demographie.medecin.fr).
In 2015, the lowest incidence rate was 0.10% (Reunion Island) and the highest incidence rate was 7% (Mayotte). The median incidence was 2.10% and the average incidence 2.05%.
No significant correlation was shown between the incidence rate of insulin pump initiation in the T1D population and the density of endocrinologists in the same department based on a univariate analysis. Similar results were obtained by only taking into account salaried endocrinologists.
Sensitivity analysis
A sensitivity analysis was conducted on people initiating insulin pump therapy in 2015, to confirm the validity of the criteria used to distinguish between T1D and T2D, by considering people to have T1D when they had received insulin during the 2 years following the date of ALD diabetes status. Of the 4083 people initiating insulin pump therapy in 2015, 5% of people initially identified as T2D were reclassified as T1D. Within this group of 5% of reclassified individuals, diabetes medication (in addition to insulin therapy as insulin therapy concerns the all study population) had been dispensed at least once to 82% of these individuals. In one-half of cases, these treatments corresponded to drugs not usually prescribed to people with T1D (sulfonylurea, dipeptidyl peptidase-4 inhibitors, alpha-glucosidase inhibitors, and glinides) and in the other half it corresponded to metformin or glucagon-like peptide 1 analogue, which may in some rare cases be prescribed to patients with T1D. We, therefore, considered the hypothesis that these people truly presented T1D to be unlikely, thereby confirming the criteria used to distinguish between T1D and T2D.
Discussion and Perspectives
Factors associated with insulin pump therapy initiation are consistent with clinical practice guidelines
We used a logistic regression model to analyze the main predictive factors of insulin pump therapy initiation compared with continuation of MDI in people with insulin-requiring diabetes. General scheme (including SLM) beneficiaries with insulin-requiring diabetes in 2015 were identified from SNDS data. This study, based on 615,000 people with insulin-requiring diabetes, demonstrated the following predictive factors for insulin pump therapy initiation (regardless of the type of diabetes): at least one endocrinologist consultation during the 2 years preceding initiation of insulin pump therapy, presence of chronic cardiovascular or neurovascular disease and presence of antidepressant or anxiolytic therapy with no mental illness identified on ALD or hospitalization diagnoses. Two additional predictive factors were identified in people with T1D: female gender and a history of acute metabolic complications. Finally, among people with T2D, a longer history of insulin therapy also appeared to be positively associated with initiation of insulin pump therapy. Factors identified as obstacles to initiation of insulin pump therapy were advanced age, duration of diabetes, end-stage renal disease, mental illness (ALD or hospitalization diagnosis), and CMU-c cover (these last two factors were only significant in people with T1D). Predictive factors for initiation of insulin pump therapy identified in this study, based on recent French data, therefore appear to be consistent with clinical practice guidelines. 2
Regular specialized follow-up in diabetology
In France, the initial prescription of external insulin pump therapy must be established in a specialized “initiating” center satisfying a number of specifications. It is, therefore, consistent that the “frequency of endocrinologist consultations” was positively associated with initiation of insulin pump therapy in people with T1D and T2D. However, our results did not reveal any association between the density of endocrinologists and the incidence of insulin pump therapy initiation in people with T1D (univariate analysis), suggesting that proposal of insulin pump therapy is still highly dependent on the prescribing physician. So, at this level of analysis, endocrinologists concentration in a given zone does not appear to have an effect on insulin pump therapy initiation, but this observation deserves an adjustment on possible confounding factors that was not the objective of this study. For example, decision to consult an endocrinologist was studied by Andrade et al. 21 and showed a marked positive effect of income and a higher probability of consulting when treatment complexity increases.
Age
The second major determinant of insulin pump therapy initiation is the patient's age: initiation of insulin pump therapy decreases with increasing age, both for people with T1D and people with T2D. This result is independent of the duration of diabetes and has also been reported in other studies. 22 –24 One may assume less attractiveness in older patients compared with younger and more active patients. This trend can also be explained by an age-related reduction of autonomy that can be related to the presence of comorbidities that were not considered in the present model (sensory disorders, cognitive disorders, social isolation, etc.).
Inequality between men and women in the T1D population
The study demonstrated an inequality between men and women in terms of initiation of insulin pump therapy, as, according to our results, women are more likely to start an insulin pump than men. A similar gender distribution has been observed in the United Kingdom, Sweden, and Denmark. 22 –24 Several explanations can probably be proposed for this phenomenon. First, in adults with diabetes, insulin pump initiation can concern young women who need strict blood glucose control before conception and then during pregnancy. These periods can justify initiation of insulin pump therapy to rapidly achieve blood glucose targets. 25 . In our study, 16% of women, who initiated insulin pump therapy in 2015 gave birth between 2015 and 2017. Data also suggest that women are more active than men on social media and would, therefore, have greater access to information concerning therapeutic innovation, 26 which could also explain the more frequent use of insulin pump therapy in women with T1D.
Duration of diabetes and insulin therapy
In people with T1D, the duration of diabetes and length of insulin therapy tend to be similar as a consequence of absolute insulin deficiency. The results of our study show that the initiation of insulin pump therapy decreases with duration of the disease, and as the choice for treating diabetes, therefore, appears to occur very early after the diagnosis of diabetes.
In people with T2D, insulin therapy is not the first-line treatment and is generally prescribed several years after onset of the disease. In our study, initiation of insulin pump therapy also decreased with increasing duration of T2D. But, in people with T2D, initiation of insulin pump therapy increased with the duration of insulin therapy, which can be explained by the fact that initiation of insulin therapy in people with T2D usually starts with basal insulin, then, after several months or years, an MDI regimen. This sequential introduction of insulin therapy, therefore, explains why initiation of insulin pump therapy increases with the duration of insulin therapy in people with T2D, as only people with MDI are eligible for an insulin pump.
History of acute metabolic complications
A history of acute metabolic complications of diabetes reflects the difficulty of diabetes management, which is often associated with poorly controlled diabetes and/or more frequent blood glucose variations in people with T1D. These events are rare but can have very serious consequences and they provide an opportunity to review therapeutic management. In 2010, the Société Francophone du Diabète published a consensus statement on the indications for insulin pump therapy. 2 The prevalence of moderate or severe hypoglycemia is considered an indication for insulin pump therapy with a high level of evidence. 8
History of cardiovascular and neurovascular disease
Our results indicate that the presence of a history of chronic cardiovascular or neurovascular disease is associated with a higher probability of initiating insulin pump therapy. Two hypotheses can be proposed to explain this association. The first hypothesis is that of a confounding factor: diabetes control, which was not entered into the multivariate analysis model as this information is not available in the SNDS. It can be assumed that people with a history of cardiovascular or neurovascular disease are also likely to have poorly controlled diabetes, which is why insulin pump therapy is more often proposed to these patients. A second hypothesis is that people with a history of cardiovascular or neurovascular disease are more closely followed and may be more often hospitalized (independently of endocrinology consultations or hospitalizations). This more intensive hospital management could be responsible for this association between cardiovascular or neurovascular disease and the incidence of insulin pump therapy initiation.
Factors limiting initiation of insulin pump therapy
Our results showed that a history of mental illness or end-stage renal disease were factors that limited initiation of insulin pump therapy, which is consistent with the indications and contraindications of insulin pumps. 2 Nevertheless, the use of antidepressants and/or anxiolytics, without a diagnosis of mental illness (ALD or hospitalization), appeared to be a positive predictive factor of insulin pump therapy initiation. This result may appear to be somewhat surprising at first sight, but can be explained by the following hypothesis: insulin pump therapy may be prescribed in an anxious or depressed patient to decrease his/her mental load related to the burden of daily diabetes care and thus improve the patient's quality of life and enable to effectively manage his/her treatment and diabetes. 14
End-stage renal disease is associated with a higher risk of metabolic acidosis and is a theoretical contraindication of insulin pump. 2 But the low rate of insulin pump therapy in these patients can also be explained by the fact that their diabetes is easier to control as a result of the “burnt-out diabetes” phenomenon, 27 as these patients present spontaneous improvement of blood glucose control due to a reduction of their insulin requirements, an alteration of renal gluconeogenesis, and a decrease of carb intake. Insulin pump therapy is, therefore, less commonly proposed to them.
Finally, in terms of social factors, our study showed that CMU-c beneficiaries with T1D had a lower probability of initiating insulin pump therapy than non-CMU-c beneficiaries. Moreover, this association remained significant after adjustment for the number of endocrinologist consultations, which suggests that poorer access to specialist cannot fully explain this disadvantage. Other factors associated with the patient's socioeconomic conditions are probably involved and it can also be assumed that the patient's lower socioeconomic status or lower level of education may influence the prescriber's treatment strategy.
Comparison of the prevalence of insulin pump therapy in people with T1D in Europe
The number of people with T1D treated by external insulin pump in France in 2015 was 16,782, corresponding to a prevalence of 8.4%. However, this prevalence is rapidly increasing, as the estimated prevalence in 2017 was 21% (all insurance schemes). The estimated prevalence of external insulin pump therapy in 2016–2017 was 15.6% in England and 6.7% in Wales, with local variations ranging from 5% to 50%. 22 In Scandinavian countries, the estimated prevalence of external insulin pump therapy was 20% in Sweden in 2015, 24 and between 12% and 31% in Denmark 23 (2014–2015), which again highlights the marked variations between countries and even between regions.
Limitations
The SNDS presents a number of limitations specifically related to its structure, as it was not specifically designed for research purposes, but exclusively for reimbursement of individual health care expenditure based on medical administrative data.
Among the limits, we can cite the absence of biological data or the absence of data concerning the prescriber characteristics. As 88% of insulin pump prescribers are health care professionals working in hospitals or health care institutions, no analysis comprising prescriber characteristics could be performed, as such information is not available in the database. However, we tried to consider certain aspects of health care provision based on the characteristics of the general practitioner, for whom more information was available, even when the general practitioner was not inevitably the physician who initiated treatment. Similar results were obtained whether or not the analysis was adjusted for the general practitioner's characteristics (data not shown).
Another limit is that SNDS data cannot be used to distinguish the type of diabetes. It was decided not to use an algorithm to distinguish between people with T1D and T2D based on ICD-10 codes, as coding modalities can be ambiguous because they were based on the type of treatment and not the type of diabetes before 2015. We, therefore, decided to use an age criterion to limit potential bias related to the quality of ICD-10 coding in the PMSI database. The cutoff of 45 years is debatable (as some cases of T2D can occur before the age of 45 years and some cases of T1D can occur after the age of 45 years). Individuals with diabetes other than type 1 or 2 cannot be identified and are automatically included in one of these two groups.
Finally, concerning prediction variables for insulin pump initiation, diabetic coma, and ketoacidosis are not distinguished (acute metabolic complications). This choice was made due to a low number of events but is probably objectionable as those two events are different.
Conclusion
This study provides new objective data about the profile of people with diabetes treated by insulin pump in France and reveals inequalities that could guide decision-makers concerning the measures to be taken to improve the management of these people. This study was based on recent comprehensive nationwide data, allowing powerful analysis of data concerning people with T1D, who are often poorly represented. The proportion of patients treated by insulin pump therapy in France remains low in view of the many studies demonstrating the efficacy of external insulin pump therapy compared with MDI. However, considerable progress has been made in the treatment of diabetes by insulin pump (insulin pump linked to continuous blood glucose monitoring [transducer], closed loop pumps, “artificial pancreas,” etc.) and the prevalence of T1D patients treated by insulin pump is gradually increasing each year. A growing number of patients will, therefore, eventually benefit from these innovations, which will represent a certain cost for the French health system.
This study, therefore, provides preliminary data concerning the profile of people treated by external insulin pump in France. The results of this study need to be completed by other studies, particularly concerning the intensity of use of insulin pump therapy in practice (intensity, persistence, care pathway, and costs). Such studies would allow decision-makers to consider actions designed to promote insulin pump therapy among both health care professionals and patients.
Footnotes
Authors' Contributions
A.-S.A., C.G.-M., A.F.-C., Y.V., and L.M. designed the study. L.M. and A.-S.A. collected the data. L.M., A.-S.A., and D.V. analyzed the data. L.M., A.-S.A., C.G.-M., and Y.V. wrote the first draft. C.A. wrote particularly the introduction and discussion. Finally, all authors wrote, and contributed to the interpretation of the data, revised critically each versions of draft, and globally participated to the whole aspect of the study. C.A. and C.G.-M. take full responsibility for the study as a whole, including the study design, access to data, and the decision to submit and publish the article.
Data Availability
The data supporting the findings of this study are available from the SNIIRAM/SNDS database. Analyses of the SNIIRAM/SNDS databases have been approved by the French personal data protection agency. Restrictions apply to the availability of these data and may not be publicly available.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project was supported by the French national health insurance.