
Abstract
Background:
The current COVID-19 pandemic provides an incentive to expand considerably the use of telemedicine for high-risk patients with diabetes, and especially for the management of type 1 diabetes (T1D). Telemedicine and digital medicine also offer critically important approaches to improve access, efficacy, efficiency, and cost-effectiveness of medical care for people with diabetes.
Methods:
Two case reports are presented where telemedicine was used effectively and safely after day 1 in person patient education. These aspects of the management of new-onset T1D patients (adult and pediatric) included ongoing diabetes education of the patient and family digitally. The patients used continuous glucose monitoring with commercially available analysis software (Dexcom Clarity and Glooko) to generate ambulatory glucose profiles and interpretive summary reports. The adult subject used multiple daily insulin injections; the pediatric patient used an insulin pump. The subjects were managed using a combination of e-mail, Internet via Zoom, and telephone calls.
Results:
These two cases show the feasibility and effectiveness of use of telemedicine in applications in which we had not used it previously: new-onset diabetes education and insulin dosage management.
Conclusions:
The present case reports illustrate how telemedicine can be used safely and effectively for new-onset T1D training and education for both pediatric and adult patients and their families. The COVID-19 pandemic has acutely stimulated the expansion of the use of telemedicine and digital medicine. We conclude that telemedicine is an effective approach for the management of patients with new-onset T1D.
Introduction
The current COVID-19
The global burden of diabetes continues to increase and is now estimated at 475 million people worldwide. 1 More than 100 million people require insulin therapy for management of their diabetes, including ∼15% antibody positive misdiagnosed patients with type 2 diabetes. 2 Many physicians have noted that there has been a significant and disproportionate increase (100-fold) in the number of health-care system administrators compared to the growth in the number of endocrinologists, physicians, and health-care providers available to care for patients. 3 –6 This growth in “overhead” may be a source of the imbalance between the cost of health care and the number of physicians available to provide care for growing patient populations. As such, physicians are challenged to “do more with less” and thus innovate to provide accessible and cost-effective care for patients.
The lifetime cost for T1D alone in the United States is about $1 trillion (direct medical costs, societal costs, and total income loss) for 1.6 million people, which is approximately $10,000/year per patient. 7 Imagine if similar costs were to apply to the world stage (for 30 million people with T1D), lifetime cost would be ∼$15 trillion. The annual global expenditure related to diabetes now exceeds U.S.$800 billion, of which about $300 billion are spent in the United States, where it is ∼8% of total health-care spending. 8 About $1 billion is spent per year for the care of acute diabetes-related hospital admissions (hypoglycemia and diabetic ketoacidosis [DKA]) in the United States. 9 Costs for the management of long-term complications have continued to increase in large part due to inadequate quality of care for the majority of patients. Most adult patients with all types of diabetes (∼90%) are cared for by primary care physicians or allied health professionals in the United States due to the limited number of trained endocrinologists/diabetologists. 3 –6 However, a larger percentage of children and adolescents with diabetes are treated by pediatric endocrinologists. 6,10 Despite increased use of technologies, the average quality of care of people with insulin-requiring diabetes is inadequate, even in the United States and the Organization for Economic Co-operation and Development (OECD), and is decidedly less satisfactory in the remainder of the world. 11 –13 In the United States, about 35%–40% of patients with T1D are using continuous glucose monitoring (CGM), and about 15% of T2D are using some CGM. 11 –13 This number is likely to grow in the United States and OECD, and CGM is likely to largely replace self-monitoring of blood glucose (SMBG) in the next few years.
The World Health Organization forecasts a current global deficit of approximately 18 million health-care workers. 10 There is a need to improve outcomes and examine the long-term sustainability of resources for the care of patients with diabetes. Hopefully, telehealth and digital diabetes care will better enable health-care providers to reach the millions of people with either type 1 or type 2 diabetes who currently do not achieve the desired level of glycemic control, thereby improving quality of care and reducing societal health-care costs. 10,14 –21
The COVID-19 pandemic has removed many long-standing regulatory burdens to telehealth and created an unprecedented surge in demand for this form of care from both patients and providers. Here, we present two cases (of the 13 seen at BDC in the last 2 weeks) of new-onset T1D management via telehealth, and then we discuss the potential of these COVID-19-associated changes to allow for broader improvements in diabetes care in the long term.
Case 1: Adult Case Presentation
A 20-year-old white male was admitted with DKA on the Western Slopes of Colorado. Despite having a family history of type 1 diabetes, the patient ignored symptoms of polyuria, polydypsia, feeling tired and continued weight loss for 3 months. He presented to the emergency department with very high blood sugar levels and in DKA. He was hospitalized in the intensive care unit for 2 days and thereafter remained an additional day for observation in the hospital. He was then seen as a new-onset T1D patient at the BDC Adult Clinic for day 1 new-onset diabetes education only. Because of the COVID-19 pandemic and Colorado Stay at Home Order, the follow-up visits (every day for 7 days) and 2-week visit were conducted virtually. His initial A1c was 15.0% at the time of the first visit, and all daytime blood glucose values for the past 2 days were >250 mg/dL with a time in range (TIR) of 16% (Fig. 1a). With regard to family history, the patient's maternal uncle had been followed at the BDC for T1D for the previous 31+ years. His mother has also had hypothyroidism for a long time.
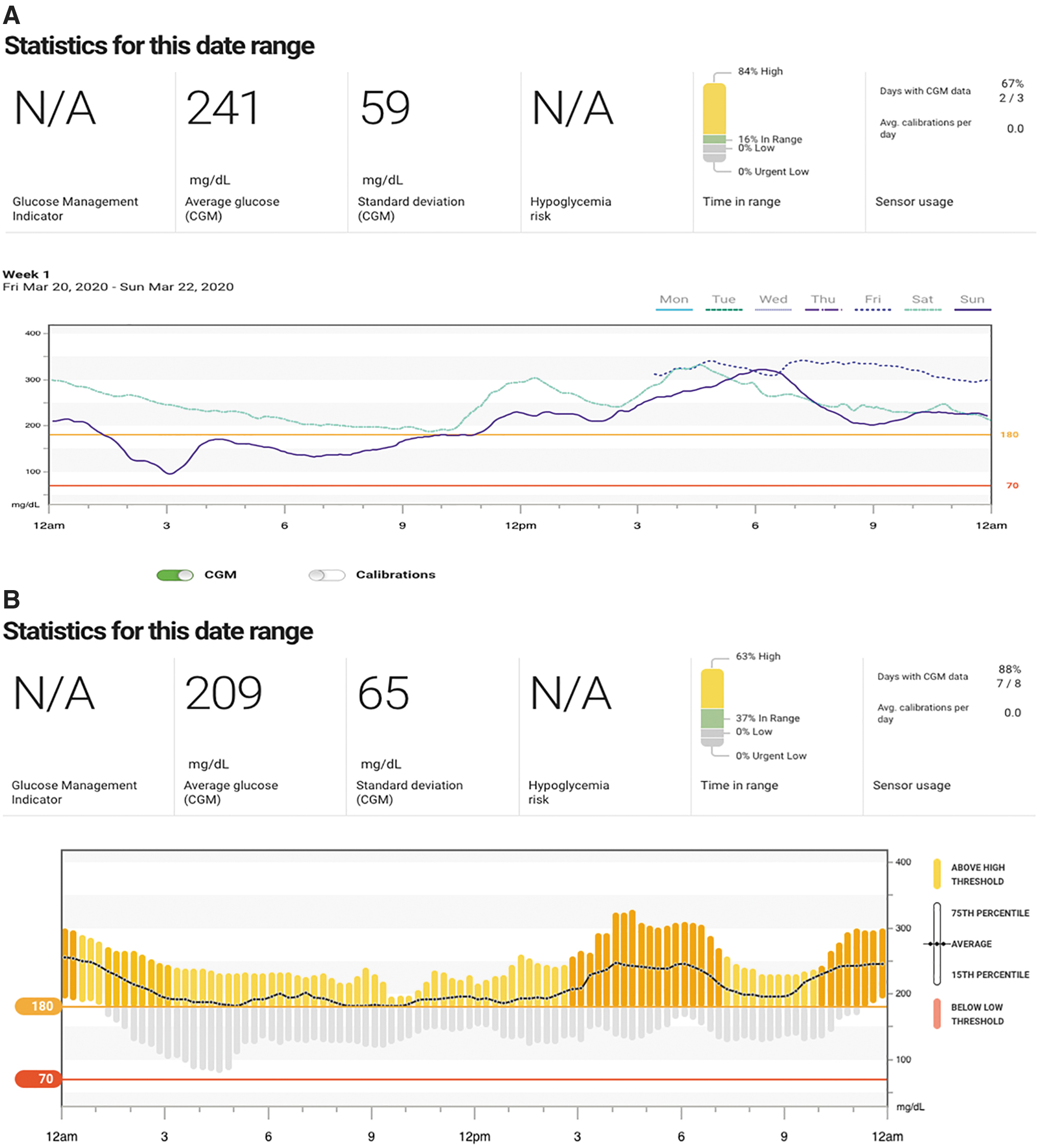
His physical examination was unremarkable when seen at the BDC on day 4 after the diagnosis of T1D. He was started on multiple daily injections with insulin glargine once daily at bedtime and insulin lispro given three times daily before meals. He was also started on CGM with a Dexcom G6 sensor (provided free [to avoid insurance bureaucracy etc.] by the BDC Adult Clinic to facilitate virtual care), and he was asked to share the data using the Clarity® software with his caregivers, so that we could manage his diabetes virtually. His insulin dose was adjusted every day (Fig. 1A) for the next 7 days by the physician based on the Clarity® outputs. 22 –27 In the second week, he was followed periodically through televisits by a certified diabetes educator (CDCES). His 2-week visit through telehealth showed a remarkable improvement in glucose values, with TIR increasing to 37% with no time below range (TBR; Fig. 1B), and his insulin doses were further adjusted. Three weeks later, at the time of this writing, he is clearly in the “honeymoon phase,” with a TIR of 90% with no TBR (Fig. 1C), but he continues to use basal insulin and very small doses of preprandial insulin. His follow-up 1-month telehealth visit is scheduled for the first week of May 2020.
Case 2: Pediatric Case Presentation
A 12-month-old white female, living more than 1 hour away from the nearest hospital in rural Wyoming, presented to the emergency department with a 1-week history of polyuria and polydipsia and 2 days of emesis and decreased energy, in moderate DKA with the following laboratory values: blood glucose 480 mg/dL, sodium 138 mEq/L, potassium 4.9 mEq/L, bicarbonate 8 mEq/L, and HbA1c 7.6%. She was air medevac'd from the regional medical center to Children's Hospital Colorado for medical management and for new-onset T1D education at the BDC.
Due to her age (12 months), weight (10 kg), and distance from our center (>250 miles), the decision was made to start her on an insulin pump (Omnipod Eros) and CGM (Dexcom G6) 23 –28 on the first day of outpatient new-onset diabetes education. The family was taught how to upload the insulin pump data via their home computer with a Glooko™ account linked to the Glooko account at the BDC. 29,30
The CGM was set up on a cell phone carried in a fanny pack worn by the child, with remote monitoring by both parents and with continuous connectivity to the Clarity® software linked to the BDC account. The parents were thus able to respond to real-time alerts via Dexcom Follow while the physician was able to see daily summary data via Dexcom Clarity®. During the first 2 weeks after diagnosis, the mother was instructed to upload the insulin pump in the evening and to e-mail the BDC physician, who provided additional new-onset diabetes education for dosing recommendations. Daily dosing adjustments were made by the physician via phone and/or e-mail using the Clarity®22 and Glooko 29 data.
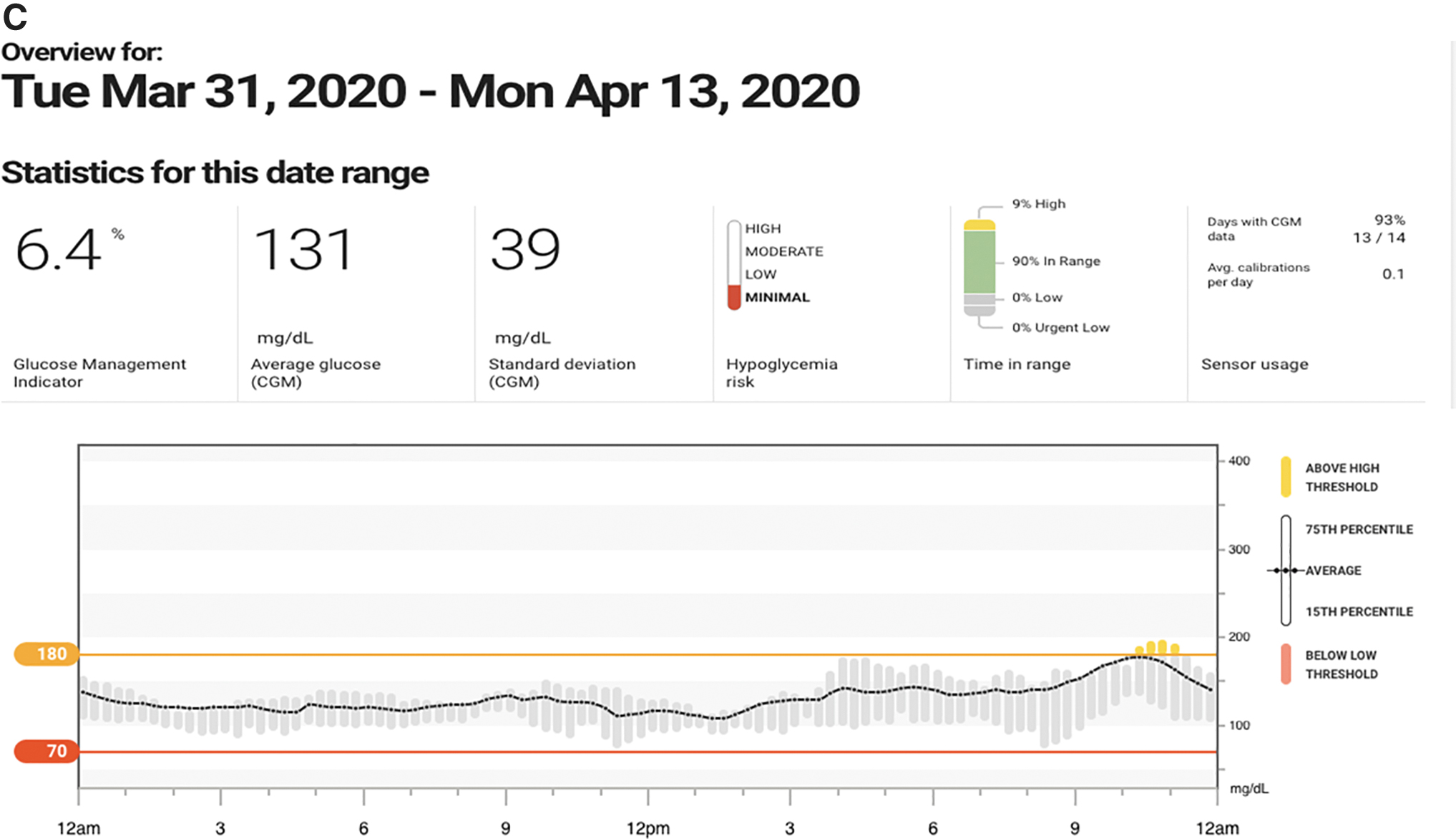
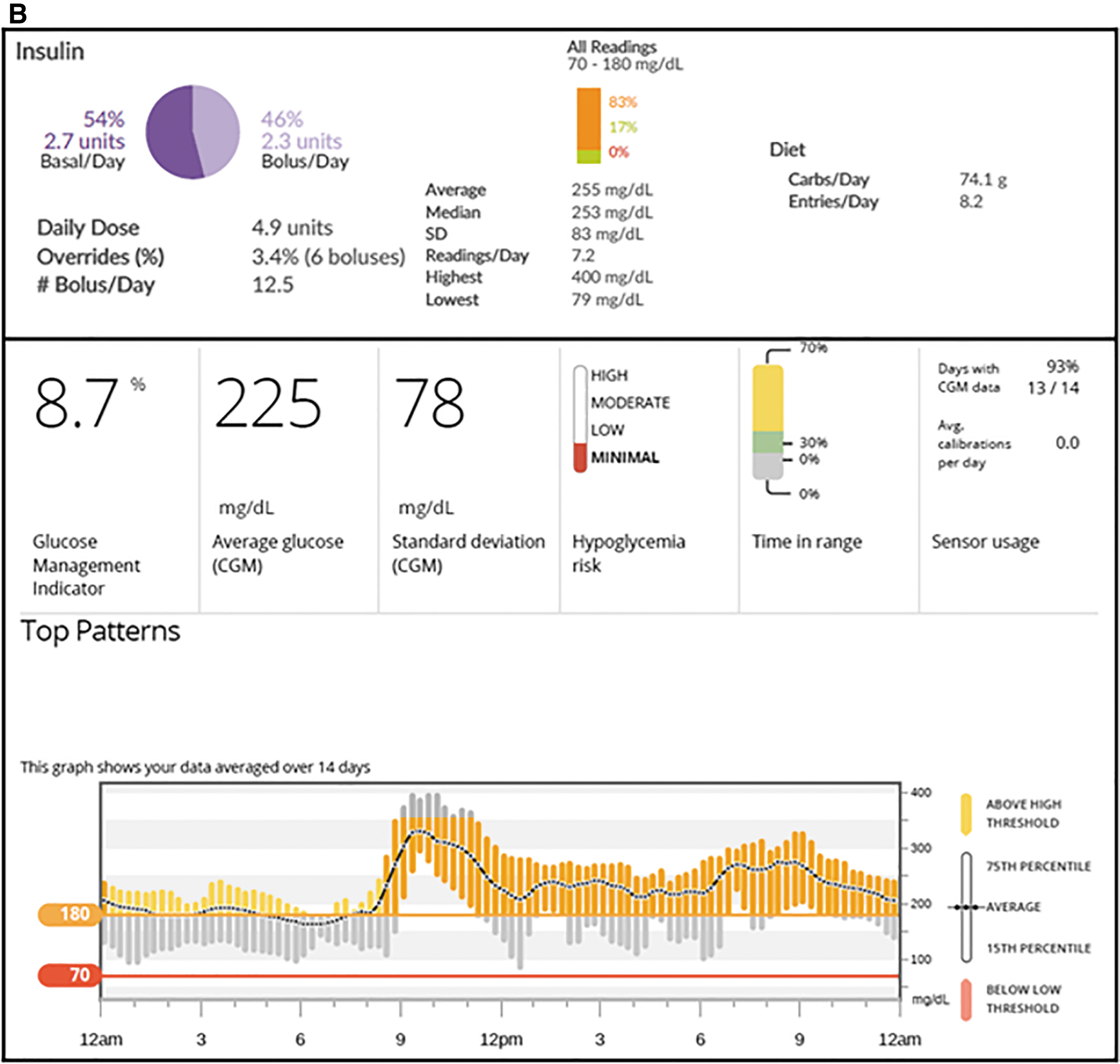
Management of new-onset diabetes in children younger than 2 years of age is focused on avoidance of hypoglycemia. Unpredictable diet and physical activity are major factors requiring gradual titration of insulin dosing. Daily review of the CGM records allows for very specific titration of insulin dosing in new-onset patients, especially those on insulin pumps. Figure 2a displays the CGM tracings for the first day of outpatient therapy at the beginning of new-onset adjustment of insulin doses and for the 14th day of outpatient therapy at the conclusion of the initial remote CGM-based tuning of insulin doses for this patient. Figure 2B displays summary data from the insulin pump and CGM download for the first 2 weeks of outpatient therapy. We show the ambulatory glucose profile (AGP), which is now in standard usage. 22 –28 This 12-month-old was already on a diet including whole milk and solid table foods at the time of presentation. Meal insulin dosing was based on the milk intake combined with a rough estimate of the amount of table food successfully consumed, and insulin was administered postprandially. Large prandial glycemic excursions were seen as a result of the use of post-meal bolusing due to unpredictable diet. The between-meal and overnight glycemic profiles showed significant improvement over the 2-week period. Her follow-up telehealth visits are scheduled.

Telemedicine Under COVID-19
The COVID-19 pandemic has brought telemedicine to the forefront of medical care. During this crisis, telemedicine has emerged as a way for patients to seek care in a way that maintains social distancing and minimizes the risk of virus transmission. Many providers and patients are discovering the benefits of home telemedicine as they are exposed to this method of care. Patients are able to conduct visits from their providers from the comfort of their homes. This is particularly beneficial for children and for patients who experience anxiety in medical situations. The virtual visits also avoid the costs, time, and inconvenience of travel and parking, helping to minimize time away from work and/or school.
T1D care, in particular, is well suited to this form of remote care, as most of the visit is built around a review of data and conversations about therapy. The advancement of continuously connected devices (such as Dexcom G6) allows for the easy flow of data from patient to physician for those using such devices. Device downloading, however, remains the main barrier for many patients who may lack the technical skills or necessary equipment to upload their devices from home prior to visits. This is particularly relevant to the geriatric population, a group that could potentially benefit the most due to challenges with access for face-to-face visits (transportation, issues with walkers, wheelchairs) and risk of infection and associated morbidity and mortality. In a recent meeting in Las Vegas (Consumer Electronics Show—CES, 2020), it was highlighted that a significant contribution from individuals aged ≥50 years amounts to about $8.3 trillion to the U.S. economy. If this group of people constituted a country, it would be the third largest economy after the United States and China. Unfortunately, 25% of people with diabetes (both T1D and T2D) in the United States are in the 6th decade of their lives or later. There are different challenges in managing diabetes in the older population, and thus the technology innovations and digital solutions may need to be individualized by different age groups based on their needs.
The main barrier to home-based telemedicine, however, has been long-standing regulations by institutions and payers (including Centers for Medicare & Medicaid Services [CMS]) limiting the ability of physicians to provide videoconference-based care to patients in their own homes, especially across state lines, which has been a major barrier for large centers such as the BDC and the University of Washington. The rapid increase in the need for continued access to care during the COVID-19 pandemic has resulted in many of these obstacles being rapidly suspended. What many patients and providers have realized is that the necessary infrastructure for a highly desirable method of care—telemedicine—already exists. Regulatory reform allowing for continued access to home telemedicine is needed, and may prove to be one of the long-term benefits of the current crisis.
Discussion
Remote and asynchronous care
Recent advances in technology make it possible to reduce the emphasis on direct (face-to-face/in-person) patient–physician encounters. This can be replaced by more frequent interactions via the Internet, telemedicine, and apps on smartphones, using both synchronous and asynchronous interactions via teleconferencing, telephone, text messaging, and/or e-mail. These systems can provide “just-in-time” training to patients, provide reassurance and emotional support, give advice on when to consult the health-care provider or seek care at an emergency room, and assist the patient in handling common everyday recurring problems. This can and already has greatly expanded the role of CDCES providing education by telemedicine.
Remote monitoring makes it possible to notify physicians and other health-care professionals regarding patients whose condition is deteriorating based on available metrics (e.g., A1C, FPG, glucose profiles [AGP 23 –27 ]) whether obtained by SMBG or CGM, leading to earlier intervention. 13 Direct input of data from CGM, connected insulin pens, 30 –32 and insulin pumps to electronic medical records can and should improve timely utilization of data and clinical outcomes. 33
Is e-health an option only because quality of care is not currently good enough, 11 –21 or does digital health/e-health offer options that traditional health does not? Does it change the paradigm by moving some of the responsibility away from the health-care professional to the patient by empowering the patient with information and decision support?
Of course, there are limitations to telemedicine, the most obvious being the inability to perform a proper physical exam. Some of this can be addressed, such as home blood pressure measurements and the use of video to look at the skin, pump sites, and the feet. Still, it isn't possible to perform a formal exam assessing for mild polyneuropathy and, for older patients, an appropriate cardiovascular exam. Obtaining accurate weight measurements can also be a challenge. It should also be emphasized that screening for diabetic retinopathy has been accomplished with telemedicine for many years. 34
Reorganization of health-care delivery systems
The systems and infrastructure to manage and oversee type 2 diabetes, especially for those individuals not requiring insulin, are quite different from the T1D patient examples presented. The use of telemedicine and digitalized medicine is likely to enable and facilitate major reorganization of systems of health-care delivery, with the potential for considerable reduction of costs with as-yet-unknown effects on quality of care and long-term outcomes. 35 –40 Digitalized medicine could potentially replace or augment the typical visit to the physician's office or clinic at 3- to 6-month intervals by the use of frequent communications with the patient (real-time online, asynchronous, texting, e-mail, telephone, smartphones) driven by artificial intelligence and clinical decision support systems, nurse practitioners, CDCES, primary care physicians, and nurses, with oversight by diabetes specialists using remote monitoring and alert systems. Approaches such as these are in various degrees of development and appear promising, although definitive evaluation of costs and benefits has not been reported. 41 –48
Reimbursement for digital medicine (telemedicine, decision support systems, developing automation and algorithms for guiding patients in real life) is still limited and depends on the country, state, and payer. CMS in the United States recommends reimbursements for telemedicine visits, including facility fees (where the telemedicine visit is being performed; this may not be the case in every state of the United States) based on appropriate documentation. In countries such as France, telemedicine is reimbursed on a limited basis but with a view to providing reimbursement once the value has been established. In Germany, the public body Health Innovation Hub is guiding digital health start-ups in developing objective evidence to evaluate the value of digital innovations to patients and to the health-care system, with the goal of justifying reimbursement at some point in the future. There is definitely a willingness to reimburse digital solutions now more than ever, but the value must be established similar to other health-care modalities such as pharmaceuticals or medical devices. The reimbursement pathway in Germany for digital tools resembles the reimbursement pathway for pharmaceuticals. All health-care interventions compete for the same budget, and therefore all will need to demonstrate cost-effectiveness in order to be granted support from the health-care budget.
Many digital start-up companies face challenges in obtaining reimbursement. Accordingly, they seek different ways to commercialize their innovations. Approaches such as making the technology available at no charge and asking the receiver/health-care system to pay for outcomes achieved is one approach. It removes the risk from the payer, shortens the time spent on developing evidence of value and effect, provides flexibility for changing the digital solution to make it more adaptive and effective, and generates important information and data for the developer. One such example is the recently announced partnership between Livongo and Higi, based on the availability of Smart Health Stations. 41 The purpose is to empower people with chronic conditions, particularly diabetes and hypertension, to live better and healthier lives. These Smart Health Stations are available in pharmacies and will offer ready access to patients and are intended to help motivate them to achieve better health outcomes. Another example is Dario Health, with its user-centric MyDario mobile app, which provides coaching 42 and encourages people to make better decisions. Similar approaches have been used by WellDoc, 43 Bluestar, 44 One Drop, 45 mySugr, 46 and M-Diabetes, 47 among others. 48
A1C, Glucose Management Indicator, and TIR
For three decades, the management of patients with diabetes has been driven largely by monitoring A1C, which correlates well with mean glucose values for the past 3 months. 49 A1C evaluations remain an important validated tool for public health and monitoring long-term complications of diabetes. With the progressive availability of CGM, one can readily calculate the mean glucose and TIR. From the mean glucose, one can calculate an estimate of the predicted A1C, 49 which is now called the Glucose Management Indicator (GMI) to emphasize that it is not a direct A1C measurement per se. 28 This GMI, included in Clarity® and other software, provides an important input, available with even a few days of CGM measurements, without the need to wait for 3 months for the direct measurement of A1C. CGM measurements also provide an estimate of the TIR. TIR is nearly linearly related to A1C based on analysis of data from multiple studies. 50,51 The correlation between TIR and A1C can also be predicted theoretically. 52 Hence, the TIR (and, nearly equivalently, the TAR) can be used as the basis for clinical day-to-day management. 27,28,50,51
Conclusions
Due to the ever-increasing global prevalence and cost of diabetes associated with inadequate availability of health-care providers and access to care, especially in remote places and in emerging economies, the majority of the patients worldwide will require adequate investments in digital health. New diabetes technologies have the promise of improving the quality and duration of life, reducing costs and complications. Several studies have demonstrated the safety, efficacy, and cost effectiveness of this technological revolution. The current COVID-19 pandemic has forced us to reconsider the ways in which effective diabetes management is delivered during these challenging times. The availability of uploaded CGM, pump, and connected pen data has and will facilitate effective diabetes management remotely. To achieve further benefits, extensive studies evaluating the efficacy, safety, cost-effectiveness, long-term acceptance, adherence, use, and outcomes of these technologies are required. While many of the technological opportunities are now becoming available, an improved understanding of patient behaviors and lifestyle choices is needed in order to achieve the full potential for emerging digital health technologies for people with diabetes.
Footnotes
Author Disclosure Statement
S.K.G. received research grants from MannKind Corporation, Eli-Lilly, Novo-Nordisk, Merck, Lexicon, Medtronic, Dario, NCI, T1D Exchange, NIDDK, JDRF, Animas, Dexcom and Sanofi through University of Colorado, received consulting fees for advisory boards from MannKind, Dexcom, Eli-Lilly, Novo-Nordisk, Sanofi, Roche, Merck, Lexicon and Medtronic. G.P.F. conducts research supported by Medtronic, Dexcom, Abbott, Insulet, Tandem, and Lilly. He has served as a speaker, consultant, and/or advisory board member for Medtronic, Dexcom, Abbott, Insulet, Tandem, and Lilly. I.B.H. received research funding from Medtronic and is a consultant for Abbott, Roche, Bigfoot, and Becton Dickinson. D.R. serves as a consultant for Lilly and Better Therapeutics and has previously served as a consultant to Dexcom, Medtronic, Abbott, Roche, Lifescan, and Informed Data Systems.
Funding Information
There was no funding or support for this manuscript.