
Abstract
Background:
To limit the spread of coronavirus disease 2019 (COVID-19), governments have ordered a series of restrictions that may affect glycemic control in individuals with type 1 diabetes mellitus (T1DM), since physical activity (PA) was not allowed outside home.
Methods:
We retrospectively evaluated glycemic control of individuals with T1DM using hybrid closed loop (HCL) system in the period before the SARS-CoV-2 outbreak in Italy (February 10–23, 2020–Time 1), when movements were only reduced (February 24–March 8, 2020–Time 2) and during complete lockdown (March 9–22, 2020–Time 3). Information about regular PA (at least 3 h per week) prior and during the quarantine was collected.
Results:
The study included 13 individuals with a median age of 14.2 years and a good glycemic control at baseline (glucose management indicator of 7%, time in range [TIR] of 68%, time below range [TBR] of 2%). All individuals continued to show good glycemic control throughout the study period. There was an increase in TIR during the study period (+3%) and TIR was significantly higher during Time 3 (72%) than during Time 2 (66%). TBR was significantly lower during Time 3 (1%) both compared with Time 1 and Time 2 (2%). A meaningful variance in TIR at Time 3 between individuals who performed or not PA during quarantine and a significant increase in TIR between Time 2 and Time 3 in individuals both doing PA at baseline and during quarantine was found. At logistic regression, only the presence of PA during quarantine significantly predicted a TIR >70%.
Conclusions:
Glycemic control of T1DM in adolescents using HCL system did not worsen during the restrictions due to COVID-19 pandemics and further improved in those who continued PA during the quarantine. Maintaining regular PA in a safe home environment is an essential strategy for young individuals with T1DM during the COVID-19 crisis.
Introduction
Coronavirus disease 2019 (COVID-19) has aroused worldwide public health concerns in recent days, and when correlated with diabetes, it has initially been reported as the cause of higher mortality in adults. 1,2 However, global but anecdotal reports suggested that children, adolescents, and young adults under the age of 25 years affected by type 1 diabetes mellitus (T1DM) have a disease pattern similar to that of children who do not have diabetes and, as also reported for children in general, are less affected than adults and very rarely require hospitalization. 3 Nevertheless, the International Society for Pediatric and Adolescent Diabetes (ISPAD) emphasized the importance of continued attentiveness to standard diabetes care to avoid the need for hospitalization and emergency or urgent care visits during this period. 3
To hinder and limit the possible spread of COVID-19, some governments have ordered a series of restrictions. The Italian Government imposed the first urgent measures from February 23, 2020, including the suspension of schools, organized sports activities and meetings (while outdoor activities were allowed), 4 and then a national quarantine from March 9, 2020, restricting the movement of the entire population except for necessity. 5 These restrictions may affect glycemic control in individuals with T1DM, since physical activity (PA), which was wholly bound by the law outside individuals' home, is usually recommended to improve glycemic control. 6 It is known that during breaks from school (e.g., holidays), children are physically less active, have much longer screen time, irregular sleep patterns, and less healthy diets. 7 Such negative effects on health could be even worse when children are confined to their homes without outdoor activities and interaction with friends during the outbreak. 8 An expected reduction of exercise and an increase of sedentary behavior could, therefore, have a harmful influence on glycemic control. 6
Since in-person follow-up visits and scheduled checkups have been canceled during COVID-19 pandemics, telemedicine—not requiring physical proximity—is at the moment the only way in many countries to provide health care services for individuals with T1DM and to check glycemic control during this unexpected and out-of-the-ordinary event. 9
This study aimed to evaluate changes in glycemic control and the role of PA at home during this exceptional time in a cohort of individuals with T1DM, using a hybrid closed loop (HCL) system, which allowed us to download detailed data during the televisits through a web-based program.
Methods
We retrospectively evaluated all individuals with T1DM followed at the Diabetes Pediatric Unit of the Institute for Maternal and Child Health “Burlo Garofolo” (a tertiary hospital and research institute that serves as a pediatric referral center for the province of Trieste, Italy) who were using an HCL system (Medtronic MiniMed™ 670G) in auto mode and have made telemedicine visits since March 22, 2020.
We collected data on the age of the patient at the onset, the treatment time of the insulin pump, the time on the HCL system in auto mode, and regular PA before the restriction (Regular PA-Baseline).
We extracted data on glycemic control during the televisits from CareLink™ personal reports, and chose an observation time frame of 2 weeks, since this was the interval between the first Decree-Law of February 23rd (enacting the first emergency provisions) and the Decree-Law of March 8 (establishing the lockdown). We, therefore, evaluated the 2-week period before the SARS-CoV-2 outbreak in Italy (February 10–23, 2020–Time 1), the 2-week period between the 2 Decree-Laws when movements were only reduced (February 24–March 8, 2020–Time 2), and the first 2 weeks of complete lockdown (March 9–22, 2020–Time 3).
During the telemedicine visits, we collected information about PA in the course of restrictions (Times 2 and 3). We defined “regular physical activity” during the quarantine (Regular PA-Quarantine) as an exercise of at least 3 h per week.
Because of the retrospective nature of the study, the existing generic ethic approval and informed consent signed by parents at the disease onset, in which they agree that “clinical data may be used for clinical research purposes, epidemiology, study of pathologies and training, with the objective of improving knowledge, care and prevention,” were used. In addition, all parents were requested to give a specific informed consent for the collection of the data.
All statistical analyses were conducted with Stata/IC 14.2 (StataCorp LLC, College Station). Data are presented as median and interquartile ranges (IQRs). Wilcoxon signed-rank test was performed to check the differences of paired data. Multivariate logistics regressions were carried out to study associations between a dichotomous outcome and one or more independent variables. A P-value <0.05 was considered statistically significant.
Results
This retrospective study included 13 individuals (8 males), with a median age of 14.2 years (IQR 11.4–15.5) and median weight of 53.5 kg (IQR 45–71). The median age at onset was 6.1 years (IQR 2.5–9.0), the median duration of insulin pump therapy was 1.1 years (IQR 0.7–4.7), and the median time spent on HCL auto mode was 3.8 months (IQR 1.5–13.1).
Reference data (Time 1) showed a good glycemic control in these individuals with a median glucose management indicator (GMI) of 7% (IQR 6.9–7.5), a median time in range (TIR, 70–180 mg/dL) of 68% (IQR 60–71), a median time below range (TBR, <70 mg/dL) of 2% (IQR 1–3), a median time above range (TAR, >180 mg/dL) of 28% (IQR 24–39), and a median sensor mean glucose of 155 mg/dL (IQR 152–168), with a median daily insulin dose of 0.9 U/kg per day (IQR 0.8–1.1) and a median of 4.1 g/kg per day of carbohydrates (CHO) intake (IQR 2.9–4.7) (Table 1); they wore the sensor for a median of 93% of the time (IQR 87–96) and used auto mode for a median of 81% of the time (IQR 56–94) (Table 1). Ten individuals (76%) performed a Regular PA-Baseline: three dancing, two skating, one practicing acrobatic gym, one playing basket, one bodybuilding, one doing judo, and one playing volley.
Data on Glycemic Control in the Three Time Intervals
Data are presented as median and interquartile ranges.
P < 0.05 between Time 2 and Time 3.
P < 0.05 between Time 1 and Time 3.
CGM, continuous glucose monitoring; CHO, carbohydrates; GMI, glucose management indicator; HCL, hybrid closed loop; SD, standard deviation; TAR, time above range; TBR, time below range; TIR, time in range.
Glycemic control during quarantine
All individuals continued to show good glycemic control throughout the study period (Table 1). Nonetheless, there was an increase in TIR during the study period (median +3%, IQR −1 to 8), which was higher between Times 2 and 3 (median +3%, IQR 1 to 7) than between Times 1 and 2 (median +1%, IQR −10 to 4) (P = 0.049). The TIR was significantly higher during Time 3 (72%, IQR 68–76) than during Time 2 (66%, IQR 61–70) (P = 0.039) (Fig. 1). TBR was significantly lower during Time 3 (1%, IQR 0–2) compared with both Time 1 (2%, IQR 1–3) (P = 0.041) and Time 2 (2%, IQR 1–3) (P = 0.044) (Fig. 1), whereas TAR did not differ significantly during the study period (Table 1). Time spent in auto mode was higher during Time 3 (93%, IQR 80–96) than during Time 2 (86%, IQR 83–96), although this difference was not statistically significant (Table 1 and Fig. 1). The total daily dose of insulin did not change significantly, as well as the rate of bolus and basal insulin. There was no increase in the number of meals per day, nor of CHO intake. Reservoirs were changed less frequently during Time 3 (median every 3.5 days, IQR 2.3–3.5) than during Time 2 (every 2.8 days, IQR 2.8–3.5) (P = 0.022), although we did not find differences in set changes.

Box plot with the distribution of the percentage of TIR, TBR, and time in auto mode across the three study times (*and § P < 0.05). TBR, time below range; TIR, time in range.
The role of PA at home
During restrictions (Times 2 and 3), three individuals who performed Regular PA-Baseline did not continue any regular exercise, whereas one individual started just during the quarantine. Overall, eight individuals (61%) performed Regular PA-Quarantine: six bodyweight exercise (plus jump rope in two, plus treadmill in one, or plus online dance lesson in one), one exercise bike and yoga, and one racketball and soccer in the garden. The median time of exercise was 3.3 h per week (IQR 3.0–4.0).
TIR was not significantly dissimilar between individuals who performed or not Regular PA-Baseline or Regular PA-Quarantine at Time 1, and there was not a substantial difference in TIR between Time 1 and Time 2 for individuals performing Regular PA-Baseline or Regular PA-Quarantine. A meaningful variance in TIR at Time 3 between individuals who performed or not Regular PA-Quarantine (P = 0.005) and a significant increase in TIR between Time 2 and Time 3 both in individuals doing Regular PA-Baseline (P = 0.043), more evident in individuals performing Regular PA-Quarantine (P = 0.014), was found (Fig. 2).
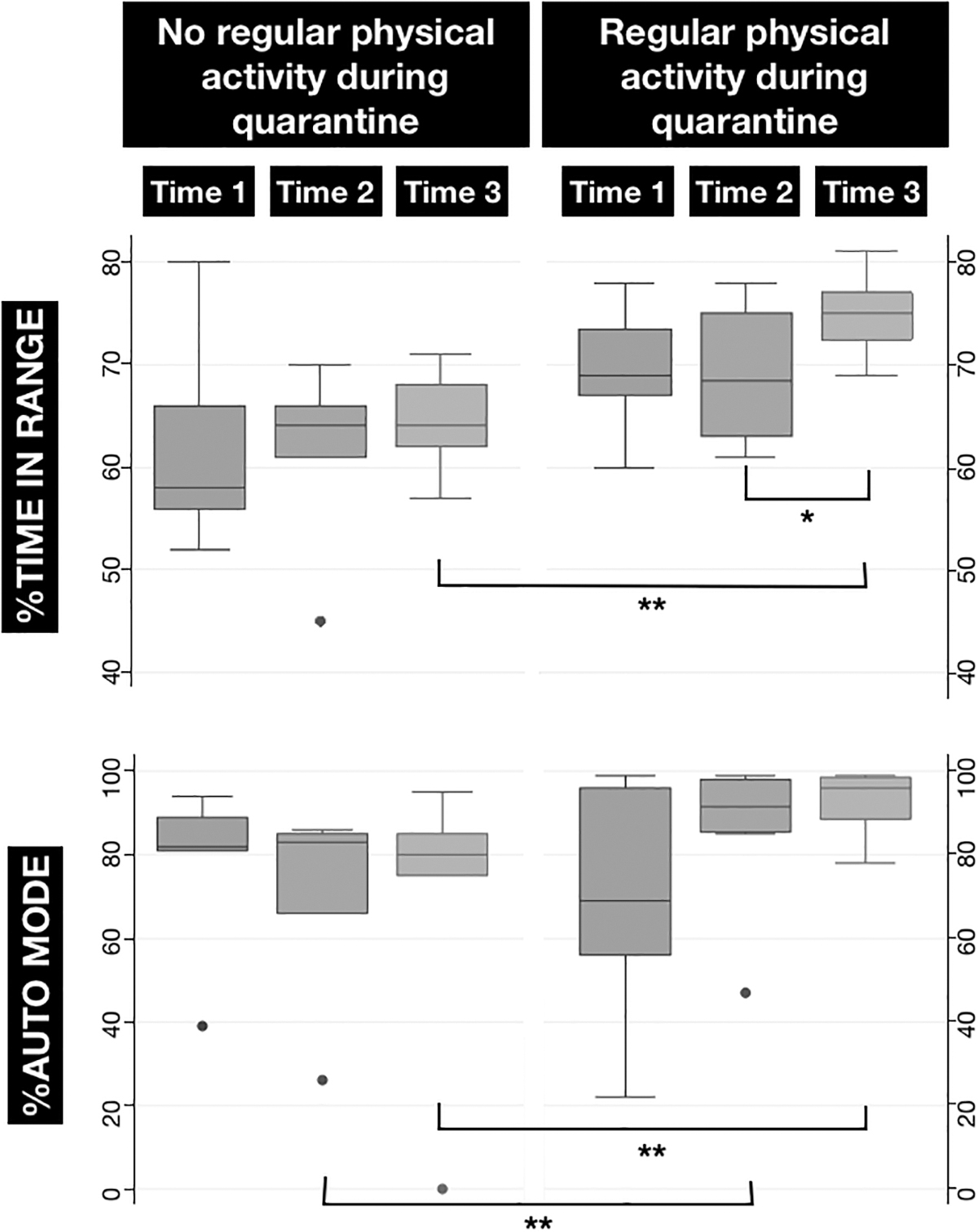
Box plot with the distribution of the percentage of TIR and percentage in auto mode across the study time in the adolescents who performed regular PA at home during quarantine or not (*P < 0.05 between Time 2 and Time 3; **P < 0.05 between the patients who performed Regular PA-Quarantine or not). PA, physical activity.
The percentage of time spent in auto mode was remarkably different both at Time 2 and Time 3 (P = 0.040) between individuals who performed or not Regular PA-Quarantine (Fig. 2).
A logistic regression model, including the percentage of time spent in auto mode and presence of Regular PA-Quarantine, was used to examine associations with TIR >70%, and only the presence of Regular PA-Quarantine significantly predicted a TIR >70% (P = 0.049).
Discussion
In this retrospective study, we analyzed the data of 13 adolescents with T1DM using an HCL system during the restriction of the activities due to COVID-19 pandemics. They showed good glycemic control at baseline (GMI 7%, TIR 68%, TBR 2%, TAR 28%), 10 which did not worsen during the first 2 weeks of restrictions. We did even find an improvement in TIR and TBR in the following 2 weeks of complete lockdown (TIR 72%, TBR 1%), which was particularly significant in those who performed regular PA at baseline and also during quarantine.
Although measures ordered by governments are necessary to fight COVID-19 spread, there are some concerns that prolonged school closure and home confinement might have unintended negative consequences since these efforts to avoid SARS-CoV2 transmission may lead to reduced PA. 6,11 This issue is even more significant for children and adolescents with T1DM since PA is highly recommended and was already identified by Eliot Joslin as one of the three components for blood glucose regulation, along with insulin and diet. The beneficial effect of PA on HbA1c, especially in young individuals, has been extensively investigated, and a recent meta-analysis of PA intervention studies in youth showed an overall effect on HbA1c of −0.85%. 6
The results of this study showed that in adolescents treated with HCL system and with good glycemic control, the quarantine had no pejorative effect.
One explanation for these findings could be the continual presence of parents at home, who could monitor their children during quarantine more closely than usual, and a more regular timetable during the day. The exclusion of the influence of some school and all after-school activities might have reduced stress levels and unpredictability due to multiple and overlapped activities. Eating every meal at home, for instance, can allow a more precise CHO count than meals outside the home, such as in the school canteen, restaurants, and friends' houses.
Another reason can be found in the continuation of the health care professional assistance through telemedicine as it was conducted before the quarantine. The technological development of recent years in the T1DM field has led to an increase in the use of technology, with the possibility of remote access to continuous glucose monitoring systems and insulin pumps data downloaded by individuals comfortably at home. This innovation leads to synergy, the involvement of the children/adolescents and families, sharing of practices that do not require physical presence, and that can be implemented, saving traveling and waiting time. Remarkably, the use of telemedicine already regularly offers a way to be close to individuals with T1DM even from afar. The evidence supporting the use of telemedicine for glycemic control and other clinically relevant outcomes among individuals with T1DM is still insufficient. 12 However, during COVID-19 pandemics, telemedicine is the only way to provide health care services for treatment of T1DM individuals, not requiring physical proximity and allowing download of detailed data through web-based programs. 9
It is noteworthy that those who performed regular PA (both before the quarantine or at home during the quarantine) even improved their metabolic control during the quarantine. Restriction measures for COVID-19 pandemics do not necessarily mean that all forms of PA must be eliminated. In-home PA using various safe, simple, and easily implementable exercises (e.g., bodyweight exercise, jump rope, and online lessons) can help in preserving fitness levels while maintaining social distancing. 11 Especially in the current situation, regular exercise is fundamental not only for glycemic control but also for psychological well-being, since PA reduces stress and anxiety and improves mood and sleep quality. 13,14
According to the Italian guidelines by the Ministry of Health, in line with those of the WHO, children and adolescents aged between 5 and 17 years should exercise at least 60 min per day, moderate to vigorous intensity. Although our individuals were far below this threshold, we proved that some activity is better than none, and more is better than less. 15
The limitations of this study are its single-center nature and the small number of subjects included. However, we believe that this information is valuable for health care professionals caring for children and adolescents during the COVID-19 pandemics and offers real-life data for further research on PA in young HCL users. The use of downloaded data during televisits allowed us to quickly answer to the concerns about glycemic control during this unexpected period.
Conclusions
This study showed that the metabolic control of T1DM in adolescents using the HCL system did not worsen during the restrictions due to COVID-19 pandemics and further improved in those who continued PA during the quarantine.
Maintaining regular PA and routinely exercising in a safe home environment is an essential strategy for healthy living during the COVID-19 crisis, especially for young individuals with T1DM. This may apply also to similar circumstances not related to a pandemic.
Footnotes
Acknowledgment
The authors thank Martina Bradaschia for the English revision of the article.
Authors' Contributions
G.T. designed the research study and wrote the article; V.C., C.C., and E.F. were involved in the clinical care of individuals and contributed to writing the article; L.M. performed the statistical analysis and was a major contributor in writing; and E.B. was a major contributor in writing and revising the article. All authors read and approved the final article.
Author Disclosure Statement
The authors have no conflicts of interest to report and no financial interests to disclose. Besides the authors, no other contributors to the article were identified.
Funding Information
No funding was secured for this study.