
Abstract
Background:
The Stay at Home order in Colorado and The Stay Safe at Home order in California during COVID-19 pandemic have forced a majority of the endocrinologists/diabetologists to adapt to providing diabetes care remotely through telehealth. This may provide increased access to diabetes health care in certain settings. However, health care disparities continue to challenge availability of diabetes technologies for underprivileged communities. We report our experience with two patients providing diabetes care effectively and preventing hospital admissions by using telehealth.
Methods:
Two adult patients with type 1 diabetes (T1D): one new onset and the other one with established T1D are presented where telehealth facilitated by Clarity Software and the “Share” feature with the use of Dexcom G6 continuous glucose monitoring (CGM) for management of diabetic ketosis and hyperglycemia.
Results:
Both patients were managed effectively virtually despite higher risk of diabetic ketoacidosis (DKA). Shared glucose data through CGM facilitated frequent insulin dose adjustments, increased fluid and carbohydrate intake, and prevented hospital admissions in both cases. In the case of new onset patient with T1D, most of the education was done remotely by certified diabetes care and education specialists.
Conclusion:
Acute diabetes complication like DKA increases morbidity and mortality in addition to adding cost to the health care system. The current pandemic of COVID-19 has allowed newer ways (with the help of newer technologies) to manage high-risk patients with T1D and DKA through telehealth and may result in lasting benefits to people with T1D.
Introduction
Significant health care disparities exist between underserved individuals with type 1 diabetes (T1D) compared with those who are more affluent. 1 HbA1C levels are higher, 2 use of technology is lower, 3 and hospitalization rates for diabetic ketoacidosis (DKA) are increased. 4 This high-risk population seems particularly vulnerable to suffering from a loss of access to health care and life-sustaining insulin therapy in the midst of a health care system struggling to contain a global pandemic. However, at least anecdotally, in some circumstances people with T1D may be receiving better care, not worse.
Los Angeles County + USC Medical Center, located in one of the poorer parts of Los Angeles and is among the largest public hospitals in the United States. It is the major single provider of health care in Los Angeles County, the most populous county in the country. The endocrine fellows, who consult on inpatients with DKA, routinely see multiple cases due to lack of insulin and access to health care. To get a sense of how badly COVID-19, with clinic disruptions and loss of jobs for many, was impacting our community of patients with T1D, the endocrine fellows were queried as to how many patients with pre-existing diabetes they were managing who were admitted for DKA. The shocking answer was “none.” They said they had admitted patients with new onset T1D and several with T2D in DKA from SARS-CoV-2 infections, 5 but none with pre-existing T1D. The last case admitted to the hospital was 6 weeks prior when a patient with T1D went into DKA because he ran out of pump supplies while in jail.
This finding leads to an analysis of why. Part of the answer may be how our outpatient health care system, like many others, has changed nearly overnight from a system where patients come physically into clinic to one that relies on telemedicine. At our site, the Roybal Comprehensive Health Center, telemedicine occurs without video images and consists of scheduled telephone calls by health care providers. Our long-standing clinic for people with T1D and those with T2D on U500 insulin is still held weekly, with providers in clinic and patients largely managed remotely. Patients, many at home due to the “Stay Safe at Home” directive, are unusually receptive to our phone calls. No longer do they need to take three buses to come into clinic or take a morning off from work. The “no show” rate has dropped to an unheard of 9% low. Patients do not have to come in to pick up their medications monthly, as they now have a 3-month supply shipped to their homes, with a year's worth of refills.
Instead of waiting months between appointments, our patients are now “seen” every week or two—as often as needed to manage their diabetes. Expanded access to health care and treatment is changing the care we provide. Thanks to a combination of county and grant funding we offer telehealth along with diabetes educators, registered dietitians, social workers, pharmacists, and others. The weak link is technology. Patients rarely have continuous glucose monitors (CGMs), although those who do allow us to manage their diabetes through cloud-based programs that is incredibly useful, as described in the cases hereunder. Most have to figure out how to find their glucose levels in their meter memories and read them out to us, which is often problematic. Although we can obtain some individuals' sensors and pumps through MediCal (Medicaid), the process is difficult and refills intermittently as health plans change distributors, leaving patients with discontinuous access to the tools they need. Most device companies do not offer meaningful discounts for underserved patients. Despite a multiyear-long effort, made by our Department of Health Services Endocrinology Work Group, we cannot get traction for the county supplying our patients with CGM devices due to the cost associated with doing so.
Methods and Results
To illustrate the essential nature of diabetes technology in dealing with this pandemic, two cases illustrate this point. In both cases the patients received free accessible CGM systems rather than having to go through the process of insurance verification.
The first is a 21-year-old student with T1D, home from college because his school had closed due to COVID-19. Upon arrival in Los Angeles he self-quarantined and after several days he developed a fever, cough, body pain, a loss of taste, and smell, as well as marked reduction in appetite. His blood glucose levels started to rise and the patient, who is on an insulin pump but not on a sensor, felt too weak and nauseated to drink fluids. His urine ketones were strongly positive. Based on a presumptive diagnosis of COVID-19, his mother tried to minimize direct contact but wanted to help her son. A friend with T1D dropped off unused sensors and a transmitter. He was given antiemetics, his fluid consumption increased, and he gave small frequent doses of rapid-acting insulin while his mother and his diabetes team remotely monitored his glucose levels. By the next afternoon, his ketones were gone and he recovered without needing to physically interact with a health care system or break his quarantine.
The second case is a 26-year-old woman who presented with symptoms of diabetes insipidus nearly 6 years ago. Imaging of the brain showed a suprasellar tumor that was resected surgically and found to be germ cell germinoma. Histology showed the tumor to be cancerous and thus she went through radiation and chemotherapy. In addition, she had irregular and scanty menstrual cycles for 6 months along with symptoms of hypothyroidism and hypocortisol state. She was diagnosed with panhypopituitarism and has been receiving replacement hormones: desmopressin, prednisone, levothyroxine, and a low-dose estrogen and progesterone patch for the past >5 years.
Now in mid-April 2020, she presented with worsening polyuria and increased water intake. Since she had diabetes insipidus, the dose of desmopressin was increased significantly. However, her symptoms of polyuria and polydipsia continued and the symptoms were associated with weight loss. Finally, the blood glucose was checked and it was found to be very high (>500 mg/dL), and other laboratory work showed elevated beta-hydroxybutyric acid levels with nearly normal pH and a slightly elevated anion gap. She was referred to the Barbara Davis Center (BDC) for further care for the new onset T1D. Because of the COVID-19 pandemic, the decision was made to manage her new onset diabetes associated with hyperglycemia and ketosis on an out-patient basis through telehealth. On day 1, she was seen in the clinic briefly to give her basic education and provide all the insulin and technology needed for her diabetes management remotely.
She was provided with a CGM system (from the Adult Clinic of the BDC to avoid a delay in getting it through the insurance and to facilitate effective telehealth for her ongoing diabetes management). During the in-clinic visit, she was initiated on the CGM and was taught how to change the sensor every 10 days. She was not provided with a glucose meter or strips and was initiated on multiple daily injections with basal and prandial rapid-acting insulin. Since she had ketosis with very high glucose values (Fig. 1A) with only 13% of the glucose readings in the target range (time in range [TIR]) (70–180 mg/dL), she was given rapid-acting insulin (insulin lispro) on a sliding scale frequently every 30 min for the next 3 h along with a dose of basal insulin. The rest of her new onset education (e.g., carbohydrate counting, insulin dose adjustments for exercise, and alcohol etc.) was conducted virtually by a certified diabetes educator (certified diabetes care and education specialists [CDCES]) through telehealth over the next 2 days.
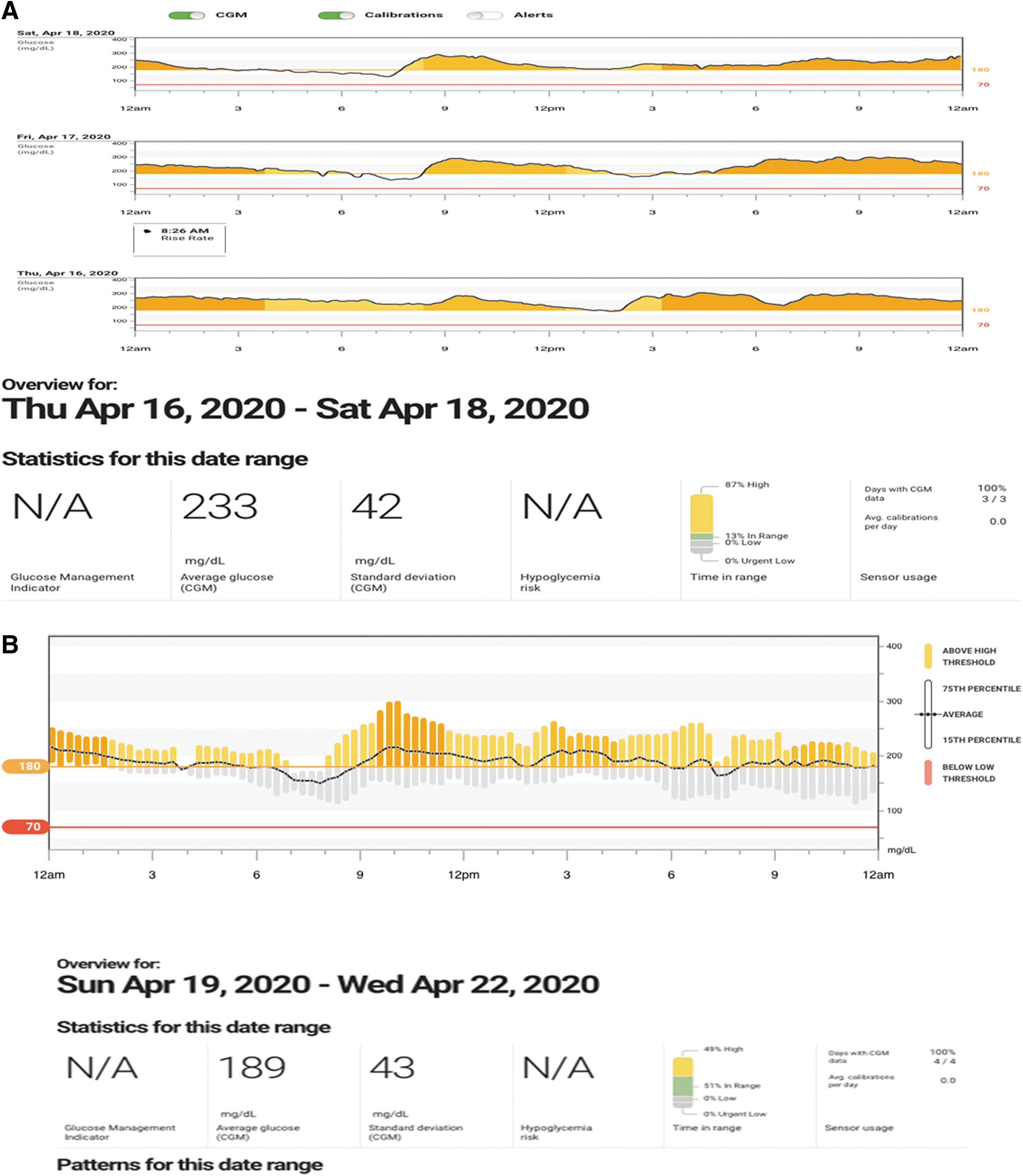

The physician followed her every day through telehealth for the next 7 days to adjust her insulin dose and thereafter she was followed by the CDCES periodically. After day 6, her glucose values were significantly lower, mostly in 150–200's (Fig. 1B) with TIR at 51% and 0% time below range (TBR). Most recent glucose values in the past 5 days (day 7–12 after the diagnosis) are in the normal range with one episode of minor hypoglycemia (Fig. 1C). More than 90% of the glucose readings are now in the target range with 0% in TBR. Her symptoms of polyuria subsided after day 3 of insulin initiation and the dose of desmopressin was reduced to the pre-T1D diagnosis. She is continuing her other replacement hormone treatments in the same dosages from the pre-T1D diagnosis. Her 2-week telehealth visit is scheduled in 3 days (April 29, 2020).
Discussion and Conclusions
COVID-19 has forced dramatic changes to our delivery of health care, some of which improve access and outcomes for our patients with diabetes. We recently reported managing diabetes remotely especially in new onset patients with T1D during this pandemic. 6 If these measures continue after the pandemic is over, they could evolve to provide significant improvements for patients.
Access to insulin, technology, and diabetes health care providers is vital to the health and survival of people with T1D. Perhaps now is the time to document the role technology can play, coupled with telehealth, to convince payors and policy makers of the lasting benefits for this high-risk population.
One issue that came up periodically during the first few days after new onset diagnosis was nonavailability of the glucose data for the past 3 h to the provider and thus patients had to be asked to read out the last few glucose readings from their smart phone. We communicated this concern to the Food and Drug Administration (FDA) about 2 weeks ago and we believe the FDA cleared the hurdle and allowed for the last 3-h data to be made available to the provider or others where the data are being shared. However, to date, this has not been resolved due to regulatory updates needed by the device manufacturer. This is particularly important as we help keep people safe and out of the hospital during these unprecedented times during a global pandemic.
Footnotes
Acknowledgments
The authors thank the clinical and research staff at the Roybal Comprehensive Health Center and the Barbara Diabetes Center, as well as the Los Angeles Department of Health Services Endocrinology Work Group.
Author Disclosure Statement
A.L.P. participates on an advisory board for Abbott Diabetes Care, Boehringer Ingelheim, Eli Lilly and Company, Livongo, MannKind, Merck, Novo Nordisk, Sanofi, and Pendulum Therapeutics; has research support from Dexcom and vTv Therapeutics, and has devices donated from Abbott Diabetes Care; and is in the speaker's bureau of Novo Nordisk; and has stock options in Mellitus Health, Omada Health, Stability Health, Pendulum Therapeutics, and Livongo. S.G. receives advisory boards consulting fees from Medtronic, Roche, Merck, Lexicon, Novo-Nordisk, Sanofi, Mannkind, Senseonics, Stability Health, Zealand, Inc., and Eli Lilly and CO; receives research grants from Eli Lilly, Novo-Nordisk, Merck, Lexicon, Medtronic, Dario, NCI, T1D Exchange, NIDDK, JDRF, Animas, Dexcom. and Sanofi; has no stocks in any device or pharmaceutical company; and all research grants, travel, and honoraria were received through University of Colorado Denver.
Funding Information
Our research in underserved regions of Los Angeles is, in part, funded through grants from the Leona M. and Harry B. Helmsley Charitable Trust.