
Abstract
Background:
Pregnant women with diabetes are identified as being more vulnerable to the severe effects of COVID-19 and advised to stringently follow social distancing measures. Here, we review the management of diabetes in pregnancy before and during the lockdown.
Methods:
Majority of antenatal diabetes and obstetric visits are provided remotely, with pregnant women attending hospital clinics only for essential ultrasound scans and labor and delivery. Online resources for supporting women planning pregnancy and for self-management of pregnant women with type 1 diabetes (T1D) using intermittent or continuous glucose monitoring are provided. Retinal screening procedures, intrapartum care, and the varying impact of lockdown on maternal glycemic control are considered. Alternative screening procedures for diagnosing hyperglycemia during pregnancy and gestational diabetes mellitus (GDM) are discussed. Case histories describe the remote initiation of insulin pump therapy and automated insulin delivery in T1D pregnancy.
Results:
Initial feedback suggests that video consultations are well received and that the patient experiences for women requiring face-to-face visits are greatly improved. As the pandemic eases, formal evaluation of remote models of diabetes education and technology implementation, including women's views, will be important.
Conclusions:
Research and audit activities will resume and we will find new ways for supporting pregnant women with diabetes to choose their preferred glucose monitoring and insulin delivery.
Introduction
4-Weeks before lockdown
Like many Diabetes Technology and Therapeutics readers, I attended the Madrid ATTD conference (February 19–22, 2020), prepared last minute slides, held dawn to dusk meetings with academic and industry colleagues, exercised outdoors in the parque Jaun Carlos 1, and shared tapas with friends at the Mercado-de-San-Miguel. Two weeks later, I gave what will almost certainly be my last “live” oral presentation at the Royal College of Obstetrics and Gynaecologists (RCOG London March 6). There were a small handful of “coronavirus” cancellations, half the audience were physically present, and the remainder by video-link.
The U.K. government advice was to keep calm and carry on (singing Happy Birthday two times during frequent daily handwashing) and life was still almost “normal,” although empty tables at central London restaurants was an early warning. Another unexpected warning came that same day, when Diabetes United Kingdom announced the cancellation of its annual professional conference. This prompt intervention served as a crucial wake-up call for diabetes health care professionals. Suddenly, there was no need to prepare posters and slide presentations, but unexpected breathing space to start to absorb the implications of the emerging coronavirus pandemic literature,
1
and widely shared online articles (
We had a short interlude to connect with colleagues in Italy and Spain, time for some initial panic and disbelief, “can we cope” telephone calls with trusted colleagues, and crucially time to plan for a rapid redesign of our clinical diabetes services. Pregnant women, especially women in their third trimester, and those with underlying health conditions, were considered vulnerable to COVID-19. On March 12, we nervously bid farewell to our clinical colleagues required to “shield” or self-isolate and completed (possibly our last ever) traditional face-to-face antenatal diabetes clinic.
By mid-March, maternity clinics with hitherto little or no IT infrastructure were literally transformed overnight into technology hubs, with secure National Health Service (NHS) (Attend Anywhere) video consultation services. We scrambled to amalgamate, review, update, and share online teaching materials for patients and health care professionals; an early coping mechanism, just as important for ourselves as for our patients. Colleagues in self-isolation focused on updating emergency guidelines for hypoglycemia, management of illness (sick-day rules), and avoidance of diabetic ketoacidosis (DKA), aiming to minimize unnecessary emergency department or hospital attendances. Webinars were shared to support day-to-day self-management of pregnant women with type 1 diabetes (T1D) using intermittent or continuous glucose monitoring (CGM).
Graphic designers gave their time freely to vastly improve our written (Pregnancy Top Tips; Supplementary Data) patient education materials. Resources were freely shared and rapidly disseminated via regional clinical networks and the National Pregnancy in Diabetes (NPID) audit infrastructure, which covers all NHS antenatal diabetes services throughout England and Wales (
Methods and Results
During lockdown
By March 23, when the U.K. government advice escalated to “Stay Home, Protect the NHS, Save lives” lockdown and social distancing procedures, the new-normal of remote antenatal clinics, video consultations, and working from home were in place. Early casualties of the coronavirus pandemic were women planning for pregnancy and attending prepregnancy care clinics, who were advised to maintain stable glycemia but also to restart safe, effective contraception. This advice was less because of concerns about the potential teratogenicity of COVID-19 exposure during early pregnancy (although data are still limited) and more for logistical reasons until normal antenatal diabetes services are reinstated. Those attending prepregnancy clinics and (hopefully most women with diabetes of reproductive years) were signposted to online resources or an interactive pregnancy planning tool.
Another coronavirus casualty was the NHS plan to make real-time CGM available to all pregnant women with T1D, which would have been rolled out from April 1, 2020
Essential ultrasound scans and retinal screening procedures
As pregnant women with diabetes were identified as being more vulnerable to the severe effects of COVID-19 and advised to stringently follow social distancing measures, they were now staying home except for essential excursions for food, health care, and health reasons. The public transport restrictions together with social distancing measures made clinic attendances logistically challenging for women without private transportation. Ultrasound scans were limited to “essential scans”; meaning an early viability scan (7–8 weeks), dating scan (12 weeks), anatomy scan (20 weeks), and growth scans at 28, 32, and 36 weeks (with many avoiding the 32-week scan during the pandemic peak). Some antenatal clinics continued face-face appointments for women attending ultrasound appointments, others (including mine), advised that women attend only for essential scans, blood pressure, and urinalysis, with subsequent telephone or video consultations, usually on the same day. Online peer support materials were promoted and specific advice for CGM use during early, mid, and late gestation (Table 1).
On Line Resources for Managing Diabetes in Pregnancy
Includes patient facing videos about what GDM means for antenatal care, how to do an insulin injection, hypos and low blood sugar, managing GDM in labor and after delivery, the benefits of skin-to-skin, early expressing of breast milk.
CGM, continuous glucose monitoring; GDM, gestational diabetes.
Retinal screening services were targeted at the highest risk women (proliferative and previously treated proliferative retinopathy, preproliferative retinopathy, or maculopathy, those without retinal screening in past 2 years).
Glycemia during lockdown
The impact of COVID-19 on antenatal glucose control will need to be carefully evaluated. Anecdotally, many women with T1D benefitted from the additional time to focus on their diabetes self-management during the lockdown (Figure 1). Others identified as “key workers” (delivery drivers, supermarket or care home assistants) including some women with T1D in their third trimester, were required to continue working for financial reasons, or were busy combining remote working with home schooling responsibilities. Women with mental health conditions and difficult social or family circumstances (including some who lost family members during the pandemic) struggled to prioritize day-to-day diabetes self-management and/or to access psychological support services. Not surprisingly, and in keeping with the higher COVID-19 mortality rates in economically disadvantaged groups (55 vs. 25/100,000), despite the use of modern technology some pregnant women struggled more than others (Fig. 1). The frequency of multidisciplinary (diabetes and obstetric) video consultations is typically 4-weekly for women with optimal diabetes self-management skills who are achieving the recommended glucose control targets (CGM time in range 3.5–7.8 mmol/L [63–140 mg/dL] of >70%, time above range [>7.8 mmol/L or 140 mg/dL] <25%, and time below range [<3.5 mmol/L or 63 mg/dL] of <4%). 2 These have been performed in the hospital antenatal clinic setting allowing joint consultation and decision making between obstetric and diabetes teams. Additional once or twice weekly telephone or email remote diabetes contacts are offered as required to women unable to achieve target glucose levels. Despite the many benefits of remote working for patients and health care professionals, there are ongoing concerns about how to support pregnant women who may be experiencing domestic abuse during the lockdown. New code phrases such as “my urine smells strange” were introduced and are now interpreted as a plea for help during telephone or video consultations.
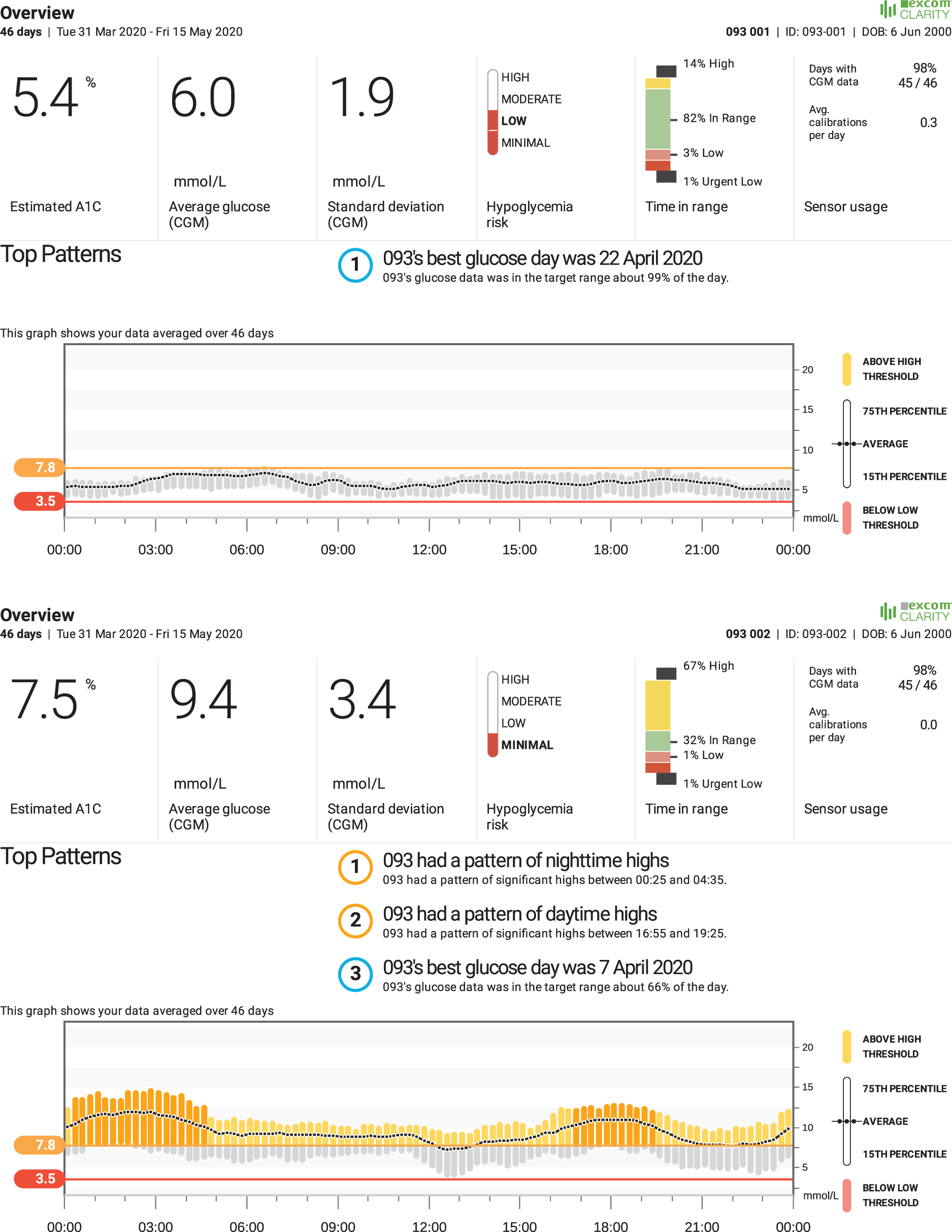
Glucose profiles of pregnant women with T1D women with easier (above) and more challenging (below) lockdown circumstances. T1D, type 1 diabetes. Courtesy of Elizabeth Turner, Diabetes midwife, on behalf of the Norfolk and Norwich University Hospital NHS Trust antenatal diabetes team, Norwich, UK.
There were also some technological successes during lockdown. A 20-year-old primiparous woman with long duration T1D was referred from another hospital at 24 weeks gestation with severe hypoglycemia. She had not engaged with diabetes self-management throughout her teenage years with insulin pump therapy previously withdrawn and replaced by an ultra-long acting basal insulin analog (degludec). Her pregnancy was unplanned with an HbA1c level of 130 mmol/mol (14.0%) at pregnancy confirmation, which had fallen to 75 mmol/mol (9.0%) by 24 weeks gestation. She had frequent daily and nocturnal hypoglycemia events, which persisted after replacing her Freestyle Libre with real-time CGM (Dexcom G6). She completed online insulin pump training (
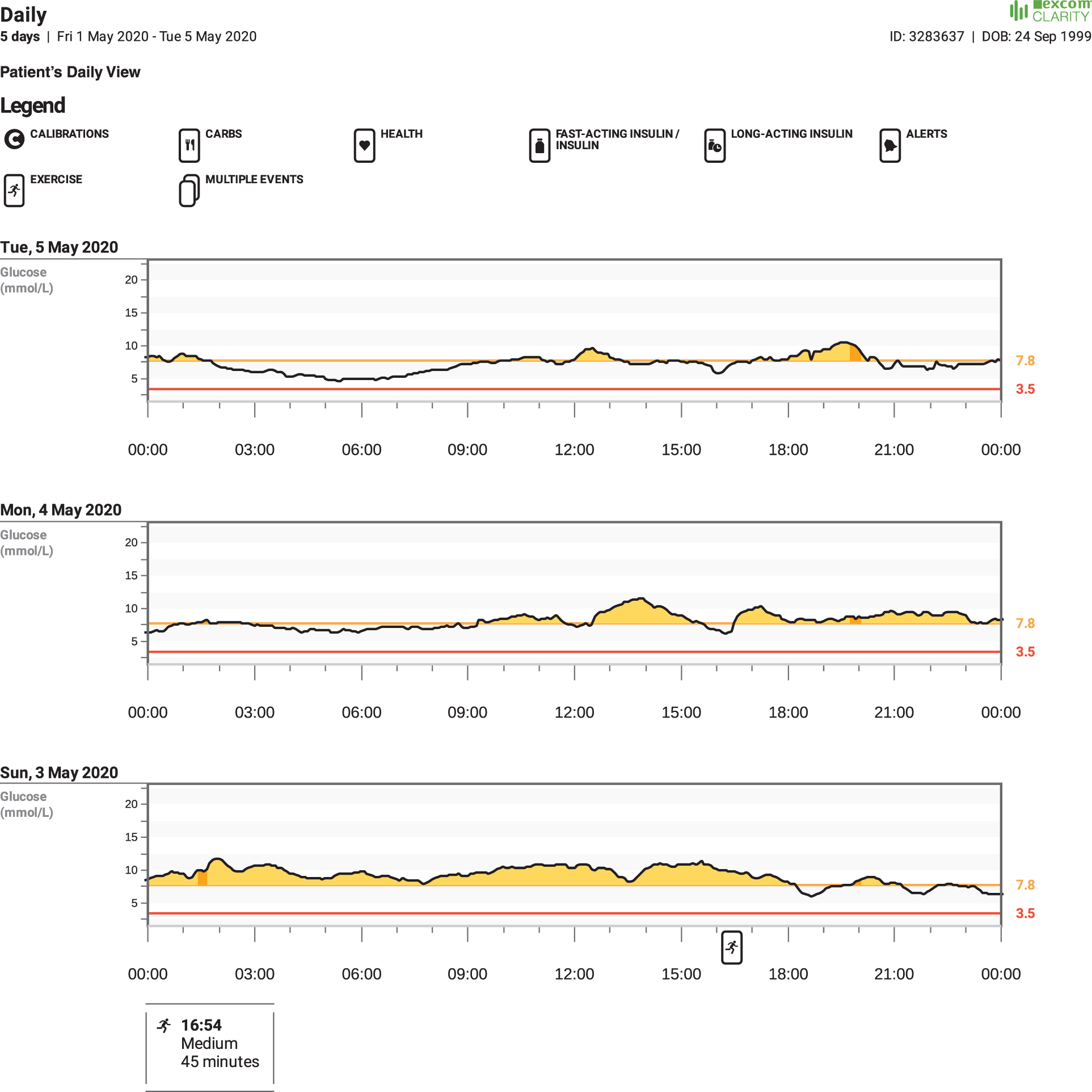
A remote pump start for severe maternal hypoglycemia during lockdown. Courtesy of Caroline Byrne, Diabetes Nurse Specialist, on behalf of the Cambridge University Hospital NHS Foundation Trust antenatal diabetes team, Cambridge, UK.

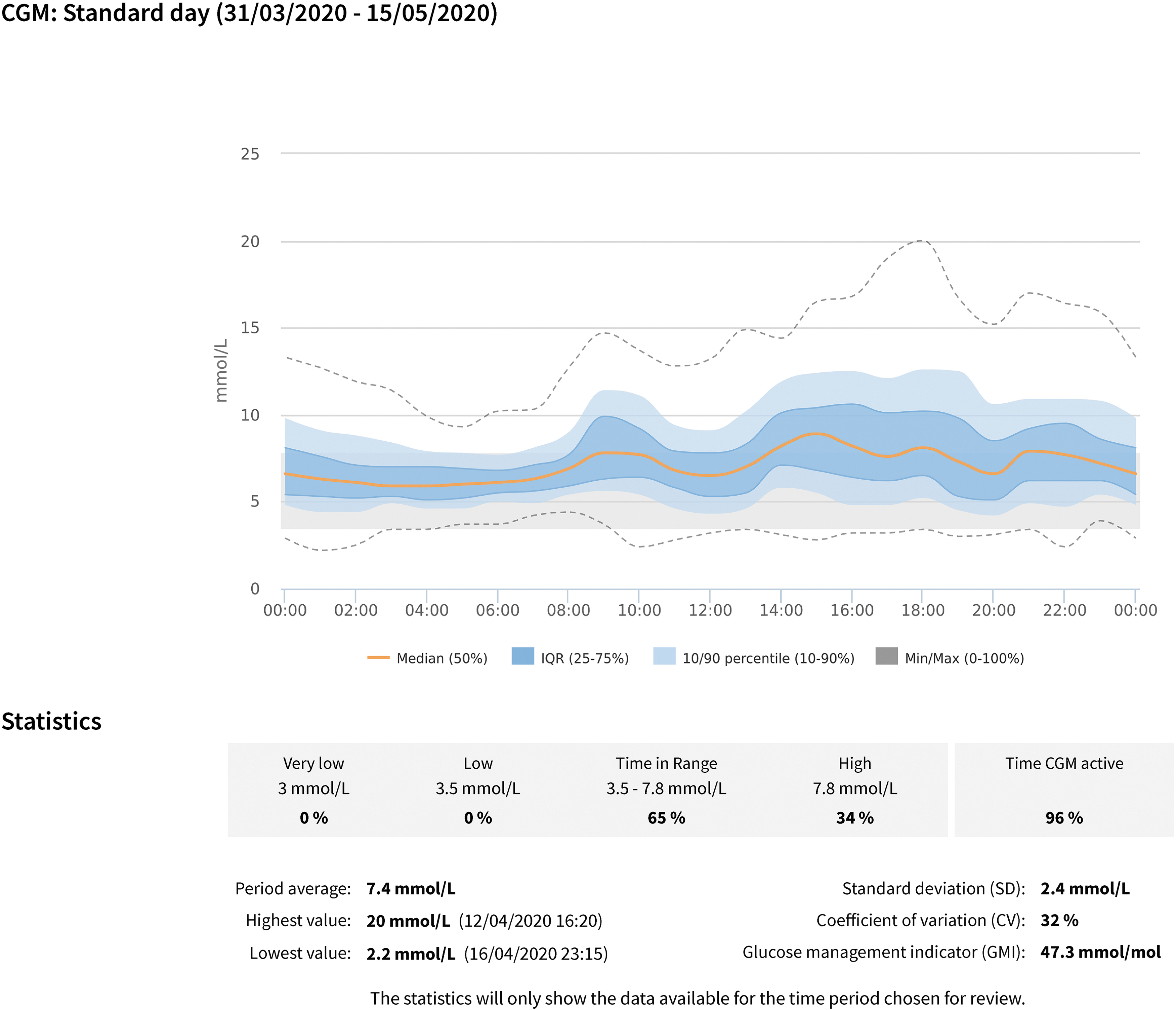
A remote closed loop start using the CamAPS FX app during lockdown. Courtesy of Josephine Rosier, Diabetes research nurse, on behalf of the Ipswich Hospital NHS Trust antenatal diabetes team, Ipswich, UK.
Gestational diabetes
With staff shortages due to self-isolation, illness, or redeployment, our clinical capacity for managing large numbers of pregnant women with gestational diabetes (GDM) and milder forms of hyperglycemia was substantially reduced. Women's concerns about attending a potentially unnecessary oral glucose tolerance test (OGTT), of which 90-95% are negative alongside public transport limitations, and laboratory social distancing measures made routine OGTTs, difficult to implement. Before the pandemic, approximately half of all women with risk factors for GDM, did not have an OGTT performed in routine care settings. 3 OGTT testing was least likely to be performed in women with higher BMI, and from higher risk ethnic groups. Strikingly, among women with pregnancies resulting in a stillbirth, an OGTT was performed in only one-third (38%) of women with known GDM risk factors, meaning that unscreened women had were at increased risk for stillbirth than women with a GDM diagnosis. 4 To avoid further exacerbating health care inequalities during the pandemic we proposed a pragmatic screening strategy, incorporated with routine antenatal care blood testing at 12- and 28-weeks gestation. 5 This involved measuring HbA1c and random plasma glucose (RPG) on all women with risk factors for GDM (previous GDM, BMI >30 kg/m2, high risk ethnic group, family history of diabetes, and previous macrosomic baby >4.5 kg) at the first antenatal “booking” (12 weeks) visit.
Women with HbA1c ≥48 mmol/mol (6.5%) or RPG ≥11.1 mmol/L are managed as having diabetes. Those with HbA1c 41–47 mmol/mol (5.9%–6.4%) or RPG 9–11.0 mmol/L are managed as having early GDM. Women with HbA1c <41 mmol/mol and RPG <9 mmol/L at booking are retested at 28 weeks, with repeat HbA1c and fasting (if possible) or random glucose performed. Women with a fasting plasma glucose (FPG) ≥5.6 mmol/L, HbA1c ≥39 mmol/mol (5.7%), or RPG ≥9 mmol/L are managed as having GDM. All women are advised that the COVID-19 testing procedures do not exclude GDM and that they should follow a healthy eating plan throughout pregnancy. Although intended to reduce the number of GDM diagnoses during the pandemic, our antenatal clinic experienced more “COVID-GDM” diagnoses during April than for all of February and March combined, with many who would not have previously been tested until 24–28 weeks gestation now diagnosed at booking.
Inpatient management of pregnant women with diabetes
The use of antenatal steroids for fetal lung maturation was prioritized for women who were expected to deliver before 34-weeks gestation. After 34-weeks gestation, steroids were withheld on the basis that the benefit to the baby at this gestation would not justify the risk to the woman associated with hospital admission. 4
Pregnant women have continued to deliver their babies in hospital settings with minimal disruption. The use of birthing pools during labor should be avoided in confirmed or suspected cases of COVID-19, given the potential risk of infection via feces. As there is limited availability of fast-track COVID-19 swabs on admission for delivery for every pregnant woman whether or not they have symptoms, this has limited access to birthing pools
Traditional midwifery topics such as support for skin to skin contact for colostrum harvesting for management of neonatal hypoglycemia continue in online formats. Except in the sickest women with COVID-19 infections (i.e., those requiring respiratory support or intensive care admission), the benefits of breast feeding outweigh any potential transmission risks. The Baby Friendly Initiative from UNICEF provides advice and support for women who are having difficulty accessing formula milk. The postnatal wards have benefitted from more bed space and fewer visitors, allowing a more restful postpartum experience than usual. Access to postnatal long acting reversible contraception such as implants or intrauterine contraceptive devices is limited so postpartum medroxyprogesterone (Depo-Provera) injections are offered, if applicable, before hospital discharge, providing 12-weeks of contraceptive cover.
Discussion and Conclusions
Unlocking and the new post lockdown normal
At the time of writing (May 6, 2020), the United Kingdom has had over 200,000 confirmed COVID-19 cases with a death toll exceeding 30,000 lives and expected to rise. The daily death toll remains high (>650 deaths), but we have “reached the plateau,” and are starting to plan for essential economic “unlocking.” The prospects of ensuring adequate supplies of an effective vaccine are still remote meaning that some social distancing measures will remain in place for the next 12–18 months. In 6–8 weeks, maternity services have transitioned from face-to-face to remote working, with home blood pressure monitoring and virtual training for self-monitoring of blood glucose and intermittent or CGM rapidly becoming the “new-normal.”
The patient experiences for women requiring face-face visits are greatly improved; “I was the only one in the waiting room, in and out in no time.” Our video consultation skills have improved and these are well received by women “the videoing clip makes a very human difference to women, their partners, and families. For many this will positively impact their health and wellbeing, and bonding. We all know the importance of this for the future health of the child.” Given these positive experiences (shared by women and health care teams alike) it is hard to imagine that we will return to traditional face-face antenatal clinics. As diabetes health care teams become increasingly confident with remote glucose monitoring, and insulin pump and automated insulin delivery systems become more user friendly, it is likely that online training will complement and perhaps replace face-face training.
There are several reports of the role of virtual care in this issue of Diabetes Technology and Therapeutics for new onset patients with T1D, 6 managing diabetic ketoacidosis virtually and avoiding hospital admissions 7 and effectively managing inpatient glucose control remotely. 8 Many nonprofit organizations like Helmsley Trust rose to the occasion. 9 For pregnant women, face-face antenatal clinic visits will be prioritized for those having ultrasound scans. As the pandemic eases, formal evaluation of remote models of diabetes education and technology implementation, including women's views, will be important. Research and audit activities will resume and we will find new ways for supporting pregnant women with diabetes to choose their preferred glucose monitoring and insulin delivery.
Footnotes
Acknowledgments
Many thanks to colleagues at the Diabetes Technology Network (DTN-UK) for developing and sharing online resources and multidisciplinary diabetes in pregnancy teams at Cambridge University Hospital NHS Foundation Trust, Cambridge UK, Norfolk and Norwich University Hospital NHS Trust, Norwich UK and East Suffolk, and North Essex Hospital NHS Foundation Trust, Ipswich, UK.
Author Disclosure Statement
H.R.M. has received honoraria for speaking engagements from Medtronic, Roche, Novo Nordisk, Eli-Lilly and is a member of the Medtronic European Advisory Board.
Funding Information
H.R.M. is supported by Tommy's charity.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.