
Abstract
Introduction:
Hybrid closed-loop systems increase time-in-range (TIR) and reduce glycemic variability. Person-reported outcomes (PROs) are essential to assess the utility of new devices and their impact on quality of life. This article focuses on the PROs for pediatric participants (ages 6–13 years) with type 1 diabetes (T1D) and their parents during a trial using the Tandem Control-IQ system, which was shown to increase TIR and improve other glycemic metrics.
Research Design and Methods:
One hundred and one children 6 to 13 years old with T1D were randomly assigned to closed-loop control (CLC) or sensor-augmented pump (SAP) in a 16-week randomized clinical trial with extension to 28 weeks during which the SAP group crossed over to CLC. Health-related quality of life and treatment satisfaction measures were obtained from children and their parents at baseline, 16 weeks, and 28 weeks.
Results:
Neither the children in the CLC group nor their parents had statistically significant changes in PRO outcomes compared with the SAP group at the end of the 16-week randomized controlled trial and the 28-week extension. Parents in the CLC group reported nonsignificant improvements in some PRO scores when compared with the SAP group at 16 weeks, which were sustained at 28 weeks. Sleep scores for parents improved from “poor sleep quality” to “adequate sleep quality” between baseline and 16 weeks, however, the change in scores was not statistically different between groups.
Conclusions:
Children with T1D who used the Control-IQ system did not experience increased burden compared with those using SAP based on person-reported outcomes from the children and their parents. Clinical Trials Registration: NCT03844789
Introduction
Type 1 diabetes (T1D) requires a significant amount of time and effort to maintain the recommended glycemic targets set forth by the American Diabetes Association. 1 Despite improvements in insulin formulations and methods of insulin administration, only 17% of children with T1D who receive their diabetes management from a trained endocrinologist are able to achieve these goals. 2
The necessity of intensive insulin management for T1D originated from the Diabetes Control and Complications Trial in which there were marked decreases in long-term diabetes complications in those using multiple daily insulin injections and with lower HbA1c levels. 3 Unfortunately, the study also found that the use of intensive insulin therapy resulted in increased frequency of hypoglycemia. Although the frequency of hypoglycemia has decreased with improvements in insulin analogues and delivery systems, hypoglycemia remains a common acute complication of T1D and an area of significant distress for patients and families. 4
Diabetes technology (including insulin pumps, continuous glucose monitors [CGMs], and hybrid closed-loop [HCL] systems) has increased the potential for individuals to increase time-in-range (TIR) 70–180 mg/dL (3.9–10 mM) and lower HbA1c levels while reducing time spent in hypoglycemia. 5 Currently, HCL systems provide the most sophisticated insulin delivery and comprise an insulin pump integrated with a CGM and an embedded algorithm that partially automates insulin delivery in response to sensor glucose levels. Recent studies involving HCL systems have shown significant improvements in glycemic variability. 5 –7
The Tandem t:slim X2 with Control-IQ is one HCL system that was recently approved by the U.S. Food and Drug Administration (FDA) in 2020 for people with diabetes, ages 6 years and over, and has shown significantly improved TIR in comparison with a control group. 5 The Control-IQ system automatically increases preprogrammed basal insulin doses when glucose levels are projected to rise >160 mg/dL (8.9 mM), and decreases preprogrammed doses if glucose levels are projected to fall <112.5 mg/dL (6.25 mM). The system can also deliver automatic correction doses in response to glucose levels >180 mg/dL (10 mM). These automated doses will occur up to once per hour at 60% of the programmed sensitivity factor.
The Control-IQ system has been tested in a randomized controlled trial (RCT) for 16 weeks in children with T1D of ages 6–13 years with favorable glucose outcomes. 8 TIR in the participants using the Control-IQ system increased from 53% ± 17% to 67% ± 10% at 16 weeks compared with 51% ± 16% to 55% ± 13% in a control group using a sensor-augmented pump (SAP), reflecting a reduction in time >180 mg/dL of 2.4 h per day and a reduction in mean glucose of 13 mg/dL. Time in hypoglycemia (<54 mg/dL) was very low in both the Control-IQ and the SAP groups. The difference between treatment groups was especially noticeable during the nighttime (midnight to 6am) when TIR was 80% ± 9% with Control-IQ compared with 54% ± 16% with SAP at 16 weeks.
The closed-loop system was active for a high proportion of the time in most participants (median time in closed loop was 93%). During the 28-week extension, TIR was maintained in the Control-IQ group (66% ± 10%) and increased in the SAP group when the participants switched over to Control-IQ (65% ± 10%). 9
In addition to the glycemic outcomes achieved with diabetes technologies such as HCL systems, person-reported outcomes (PROs) are being recognized as essential components to assessing the utility of new devices. PROs can be useful in determining the reasons for early discontinuation 10 and allow for troubleshooting and focused intervention. PROs are especially important for children and families, as diabetes-related distress is a common occurrence in youth with T1D and their parents. 11 Increased diabetes-related distress and burden play a role in reducing quality of life, diabetes self-management, and the ability to achieve glycemic targets, 12 and this is also true when considering the distress experienced by the parent of a child with diabetes. 13
The purpose of this article is to describe the experience of children with T1D, age 6–13 years, and their parents/caregivers who used the Tandem Control-IQ system (closed-loop control [CLC]) compared with a control (SAP) group in a 16-week RCT with extension up to 28 weeks, specifically related to diabetes device expectations, ease of use, impact on sleep, and fear of hypoglycemia, and quality of life.
Research Design and Methods
The study design consisted of a multicenter unblinded randomized (3:1) trial that was conducted at four pediatric diabetes centers in the United States (described in detail elsewhere). 8 The protocol was approved by a central institutional review board and informed consent was obtained from the parent or guardian and assent was obtained from each patient if applicable. Children between the ages of 6 and 13 years who had T1D for at least 1 year, weighed between 25 and 140 kg, and had a total daily insulin requirement of at least 10 U per day were recruited, along with a parent. The parents completing the surveys were self-selected by the family.
Participants randomized to the CLC group were trained on the use of the Tandem t:slim X2 insulin pump with Control-IQ technology and a Dexcom G6 CGM. Participants randomized to the SAP group used the Dexcom G6 CGM and an insulin pump (either the patient's previous pump or a study provided t:slim X2 with predictive low glucose suspend). The study consisted of a 16-week randomized trial to compare the CLC and SAP groups. At the end of the RCT, the SAP group was given the CLC system to use for an additional 12-week extension phase, while the randomized CLC group continued using the CLC system.
In addition to measuring glycemic outcomes that are reported separately, 8 participants completed quality of life, treatment satisfaction, and other PRO questionnaires at baseline, 16 weeks, and 28 weeks. The questionnaire battery was designed to assess different sources of psychological and behavioral burdens associated with living with and managing pediatric type 1 diabetes (T1D). These included worries and behaviors related to hypoglycemia, emotional distress and stressors associated with diabetes, and negative effects on daily quality of life. The questionnaires were completed online using RedCap (Research Electronic Data Capture, a secure system that is web based and designed for capturing data for research purposes). Parents completed all questionnaires and children completed those that had validated pediatric versions.
Pediatric Hypoglycemia Fear Survey
The Pediatric Hypoglycemia Fear Survey (HFS-II) assesses fear of hypoglycemia and was administered to children and their parents. 14 The survey generates a total score and two subscale scores (behavior and worry). The behavior subscale of both the child and the parent versions has two factors, including a “Maintain High BG” factor that reflects behaviors aimed at keeping glucose levels higher to prevent hypoglycemia and an “Avoidance” factor reflecting other behaviors aimed at preventing hypoglycemia. The worry subscale also has two factors, including a “Helplessness” factor that reflects concerns about the child having a hypoglycemic episode when alone or unable to get treatment and a “Social Consequences” factor that reflects concerns about the child being criticized or negatively evaluated due to hypoglycemia.
The Parent (PHFS) and Child (CHFS) versions include 26 and 25 items, respectively, rated on a 0 (not at all) to 4 (almost always) scale with higher scores indicating more fear. The scores were then scaled to 0 to 100.
The Problem Areas in Diabetes Survey
The Problem Areas in Diabetes (PAID) Survey measures diabetes-related emotional distress and was completed by both parents and children. 15 The parent version has 16 items and the child version has 11 items, which are rated on a 0 (no problem) to 6 (serious problem) scale. Factor analyses have indicated that each version is composed of a single factor. Higher scores reflect higher levels of diabetes-related emotional distress. The scores were then scaled to 0 to 100.
Pediatric quality of life (3.2 Diabetes Module)
The pediatric quality of life (PedsQL) assesses diabetes-specific quality of life. 16 There are separate versions for children and for parents to report their perceptions of their child's quality of life. Both versions have 33 items and 5 subscales identified by factor analysis (diabetes symptoms, treatment barriers, treatment adherence, worry, and communication) rated on a 0 (100%) to 4 (0%) scale with higher scores representing better quality of life.
Insulin Delivery Systems: Perceptions, Ideas, Reflections, and Expectations questionnaire
The Insulin Delivery Systems: Perceptions, Ideas, Reflections, and Expectations (INSPIRE) questionnaire measures user expectations and experience with HCL systems and there are separate versions for children and parents. 17 The INSPIRE questionnaires for children and parents, which were completed at baseline, have 27 and 41 items, respectively, rated on a 0 (strongly disagree) to −4 (strongly agree) point scale, which was then scaled to 0 to 100, with a higher score indicating more positive response. The INSPIRE experience questionnaires for children and parents were completed at 16 weeks and had 17 and 21 items, respectively, rated on the same scale.
Pittsburgh Sleep Quality Index
Parents completed the Pittsburgh Sleep Quality Index (PSQI) that contains 10 questions divided into seven components assessing sleep quality and disturbance over the past month. Individual items are rated on a 0 (no difficulty) to 3 (severe difficulty) scale with higher scores reflecting worse sleep quality. 18 Each component is then added together to yield a total score with a range of 0 to 21, higher scores indicating more difficulties in all components. A total score of >5 is considered an indicator of poor sleep.
Statistical methods
Parent- and participant-reported outcomes were compared between treatment groups at 16 weeks using a linear mixed effect regression model adjusting for baseline outcome, age, prior pump and CGM use, and clinical center (random effect). In an exploratory analysis, paired t-tests were used to evaluate the change in each outcome between baseline and 28 weeks in the CLC group and to evaluate the change in each outcome between 16 and 28 weeks in the SAP group that crossed over to CLC in the extension phase. P-values are two sided and have been adjusted for multiple comparisons to control the false discovery rate using the adaptive Benjamini–Hochberg procedure. 19 Analyses were conducted using SAS software version 9.4 (SAS Institute, Inc., Cary, NC).
Results
A total of 101 (50% female) participants were randomly assigned to either the CLC group (n = 78) or the SAP group (n = 23). Age ranged from 6.48 to 13.99 years (mean 11.2 ± 2.1) and duration of diabetes ranged from 1 to 12 years (mean 5.2 ± 2.8). Baseline HbA1c ranged from 5.7% to 10.1% (mean 7.7 ± 1.0). Insulin pumps were used by 81 participants (80%) and CGM was used by 93 participants (92%) before enrollment.
Parent questionnaires
Results of the parent questionnaire scores for the study are presented in Table 1 and Figure 1. None of the treatment group comparisons at the end of the 16-week RCT met the threshold for statistical significance. PHFS total score changed by −7.7 at 16 weeks among CLC group parents and changed by −3.9 at 16 weeks among SAP group parents (adjusted treatment group difference = −6.0, 95% confidence interval [CI] −12.3 to +0.3, P = 0.07). The change in the total score in the CLC group was reflected in the behavior (−10.8), maintain high BG (−8.1), and social consequences (−4.7) subscales.

Boxplots of parent questionnaires by treatment group and visit*. *The 16- and 28-week timepoints represent the end of the randomized clinical trial and extension phase, respectively. During the extension phase, both treatment groups were using the CLC system. Parent version of the Pediatric Hypoglycemia Fear survey (PHFS Total), 14 Problem Areas in Diabetes Survey (PAID), 15 Pediatric Quality of Life (PedsQL Total), 18 Pittsburgh Sleep Quality Index (PSQI). 18 Dark gray represents Tandem Control-IQ system (CLC) cohort, light gray represents SAP cohort, and striped lines represent SAP cross over to CLC. CLC, closed-loop control; SAP, sensor-augmented pump.
Parent Questionnaires
Model adjusted for corresponding baseline score, age, prior CGM and pump use, and site as a random effect. P-value was adjusted to control the false discovery rate.
In the CLC group, the changes in scores from baseline to 28 weeks were statistically significant for all scores except the PedsQL treatment II subscale.
In the SAP group, there were no statistically significant differences from 16 to 28 weeks.
Higher indicates a worse outcome.
N for the Problem Area in Diabetes Survey (CLC/SAP): Baseline 78/23, 16 weeks 77/22, 28 weeks 78/22.
N for the PSQI (CLC/SAP): Baseline 72/21, 16 weeks 73/20, 28 weeks 74/20.
CGMs, continuous glucose monitors; CI, confidence interval; CLC, closed-loop control; NA, not applicable; PedsQL, Pediatric Quality of Life; PSQI, Pittsburgh Sleep Quality Index; RCT, randomized controlled trial; SAP, sensor-augmented pump.
PAID scores changed by −7.8 at 16 weeks among CLC group parents and changed by −0.9 at 16 weeks among SAP group parents (adjusted treatment group difference = −7.4, 95% CI −15.5 to +0.6, P = 0.08). PedsQL total scores changed by +4.3 in the CLC group at 16 weeks and was unchanged in the SAP group (adjusted treatment group difference = +4.0, 95% CI −1.0 to +9.1, P = 0.13). The treatment group difference for PSQI also was not statistically significant (P = 0.13); however, in the CLC group, the baseline score of 5.8 ± 3.0 indicated a clinically significant disturbance in sleep that decreased to 4.3 ± 2.9 at 16 weeks, indicating an absence of clinical disturbance.
In the extension phase, when the SAP group started using the Control-IQ system, SAP group parents had changes in the scores from 16 to 28 weeks on the maintain high BG subscale of the PHFS, the PAID, the PedsQL, and the PSQI similar to the changes seen in the CLC group during the RCT phase. None of the changes in the SAP group from 16 to 28 weeks were statistically significant (P-values not shown). In the CLC group, which continued to use the system in the extension phase, the scores observed at 16 weeks were similar at 28 weeks. The changes in scores from baseline to 28 weeks in the CLC group were statistically significant at a threshold of 0.05 for all except the PedsQL treatment II subscale.
Child questionnaires
Results of the child questionnaire scores through the duration of the study are presented in Table 2 and Figure 2. There were no statistically significant differences at 16 weeks comparing the CLC and SAP groups. Total CHFS scores changed by −3.7 in the CLC group compared with +1.4 in the SAP group, and worry subscale scores changed by −4.3 in the CLC group compared with +2.3 in the SAP group (P = 0.11 for both). The SAP group had a change of −3.7 and −3.3 for each measure, respectively, when comparing the scores at 16 to 28 weeks (after the SAP group switched to CLC during the extension phase).
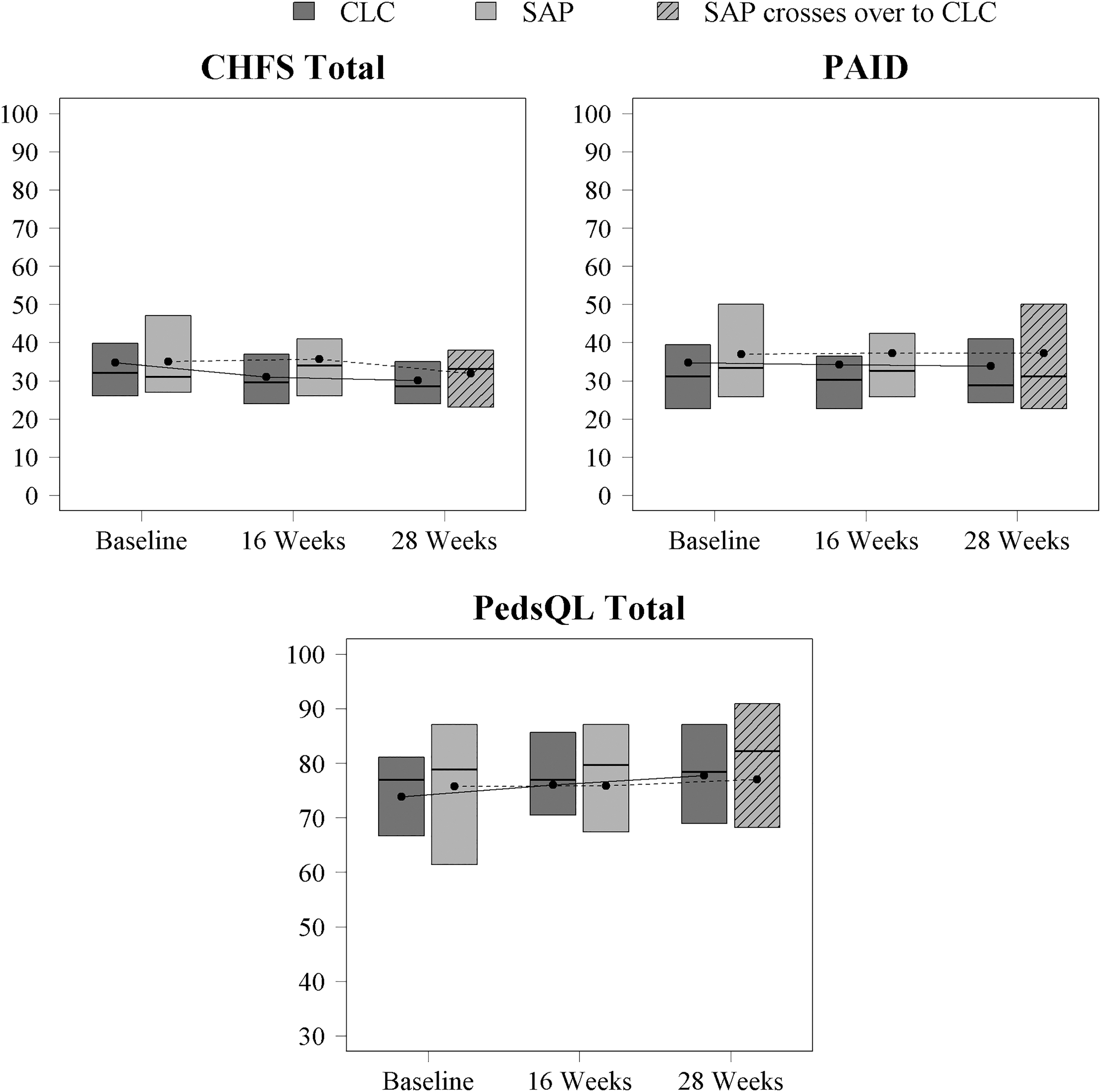
Boxplots of child questionnaires by treatment group and visit*. *The 16- and 28-week timepoints represent the end of the randomized clinical trial and extension phase, respectively. During the extension phase both treatment groups were using the CLC system. Child version of the Pediatric Hypoglycemia Fear Survey (CHFS Total), 14 Problem Areas in Diabetes Survey (PAID), 15 Pediatric Quality of Life (PedsQL Total). 16 Dark gray represents Tandem Control-IQ system (CLC) cohort, light gray represents SAP cohort, and striped lines represent SAP crossover to CLC.
Child Questionnaires
Model adjusted for corresponding baseline score, age, prior CGM and pump use, and site as a random effect. P-value was adjusted to control the false discovery rate.
In the CLC group, the changes in scores from baseline to 28 weeks in the CLC group were statistically significant for the CHFS total score and worry, avoidance, helplessness, and social consequences subscales, and for the PedsQL total score and diabetes and communication subscales.
In the SAP group, there were no statistically significant differences from 16 to 28 weeks.
Higher indicates a worse outcome.
N for maintain high BG subscale of the Fear of Hypoglycemia Survey (CLC/SAP): Baseline 78/23, 16 weeks 77/22, 28 weeks 77/22.
N for social consequences subscale of the Fear of Hypoglycemia Survey (CLC/SAP): Baseline 77/23, 16 weeks 78/22, 28 weeks 77/22.
N for the treatment I subscale of the PedsQL Diabetes Module (CLC/SAP): Baseline 77/23, 16 weeks 78/22, 28 weeks 78/21.
N for the treatment II subscale of the PedsQL Diabetes Module (CLC/SAP): Baseline 77/23, 16 weeks 78/22, 28 weeks 78/22.
N for the worry subscale of the PedsQL Diabetes Module (CLC/SAP): Baseline 76/23, 16 weeks 78/22, 28 weeks 78/22.
N for the communication subscale of the of the PedsQL Diabetes Module (CLC/SAP): Baseline 78/23, 16 weeks 78/22, 28 weeks 78/21.
N for the INSPIRE Survey (CLC/SAP): Baseline 78/23, 16 weeks 76/NA, 28 weeks 77/22.
The changes in scores from baseline to 28 weeks in the CLC group were statistically significant at a threshold of 0.05 for the CHFS total score and worry, avoidance, helplessness, and social consequences subscales, and for the PedsQL total score and diabetes and communication subscales.
Questionnaire scores by child age and baseline HbA1c are given in Supplementary Tables S1 and S2.
Discussion
Use of the Tandem Control-IQ system in children of ages 6–13 years with T1D significantly increased the time spent in the target range of 70–180 mg/dL 8 without increasing the perceived burden on the child or the parents. This was true for the 16-week randomized phase of the study and also for the extension phase. The group using CLC from beginning through extension represented outcomes after 7 months of use of the system, the largest and longest HCL study to date in this age group.
These findings combined with the previously reported high-positive user ratings on the System Usability Scale 9 suggest that the Control-IQ system does not impose additional diabetes care burdens on families that would present potentially serious barriers to the adoption and continuation of system use. These findings are consistent with other studies evaluating psychosocial outcomes for technology use in youth with T1D. 20 –24
Although it was clear that use of the Control-IQ system did not worsen quality of life compared with the use of SAP, there was limited evidence that use of CLC improved these outcomes. There did appear to be improvements in scores in the CLC group on several PRO measures; however, these were not statistically significant when compared with the SAP group. At the end of the 16-week RCT, parents in the CLC group appeared to have reductions in fear of hypoglycemia, including the total score, the behavioral subscale, and maintain high blood glucose factor.
These findings may reflect a decrease in parents' perceived need to keep their child's glucose higher to reduce the risk of hypoglycemia in certain situations, such as when the child is away from them. There was also a decrease in worries about the child being criticized or seen negatively due to the effects of hypoglycemia on behavior, as well as in overall diabetes-related emotional distress as measured by the Problem Area in Diabetes scale. These concepts should be further explored in a study powered to detect subtle differences in PROs.
Although the PSQI scores did not significantly decrease in the CLC group compared with the SAP group, it is important to note that the scores for the CLC parents decreased from 5.8 to 4.3. For the PSQI, a score >5 indicates a clinically significant level of poor sleep. Therefore, the parents in the CLC group improved from a designation of achieving poor sleep quality to adequate sleep quality. This improvement was also maintained in the CLC group after 28 weeks. In addition, the SAP group had a baseline PSQI score of 6.4 ± 3.8 that remained the same at 16 weeks (6.5 ± 3.9) but decreased to 5.4 ± 3.6 by the 28-week extension after switching over to CLC.
These findings support the anecdotal reports that parents of children using HCL systems experience improvement in sleep secondary to a reduction in worries about nocturnal hypoglycemia and nighttime awakenings to check their child's glucose levels. As objective measurements of sleep quality and quantity have only had limited evaluation in HCL system use, the impact of these devices on parental sleep warrants further evaluation since this is a major contributor to overall quality of life and perceived health.
Strengths of this study include a high retention rate for the study participants and a wide range of pediatric participants without limitations based on HbA1c or history of diabetic ketoacidosis (DKA) and hypoglycemia. In addition, this study included a control group allowing for comparison to a system available to the public. The use of an extension phase for this study showed sustainability in the changes associated with the CLC group, indicating a true effect of the system over time.
Limitations also exist for this study and the current analysis. This study was not powered based on the PRO questionnaires; therefore, some of the differences in survey scores may not have reached significance due to small sample size, particularly in the SAP group because of the 3:1 randomization with three subjects on Control-IQ for everyone assigned to the control group. Further research is needed to address health-related quality of life in this population with larger sample sizes.
The study participants likely do not reflect a more generalized population of children with T1D and their parents. The families who participated were likely to be highly engaged with their child's diabetes management and able to readily use advanced diabetes technologies due to previous experience with diabetes devices, including insulin pumps and CGMs. Therefore, adoption and successful use of HCL may present more challenges in families with barriers to engagement with diabetes management and less comfort with use of diabetes technology. The high technology use before entering this study may have had an impact on the ability to detect significant changes in PROs.
This study compared the CLC group with a group of youth using diabetes technology (the SAP group) and, therefore, was not compared with youth not using technology for diabetes management. This may have impacted the ability to find significant changes in PROs as all study participants were using diabetes devices. Although this was the largest study of HCL use in children with T1D, and the longest trial of continued use, more research is clearly needed in more general populations.
When determining the most appropriate insulin regimen for any persons with T1D, it is important to consider the burden placed on the persons and their families as well as the potential benefits. As new technologies are developed, determination of the impact on families will be a key component to the successful use of these devices. For youth with T1D, it is essential that this research includes the parents as they are at the very least involved and often in control of the child's diabetes care. Ultimately, HCL systems have a goal of improving glycemic outcomes while reducing the burden of diabetes management, which, in turn, may improve quality of life, diabetes self-management, and prevention of long-term complications from T1D. The results of this study showed that the Tandem Control-IQ system was successful in improving glycemic outcomes without increasing burden on youth with T1D and their parents.
Footnotes
Acknowledgments
The authors thank the study participants. A listing of the participant study sites, investigators, and coordinators is included as follows:
University of Virginia, Center for Diabetes Technology, Charlottesville, VA: Melissa Schoelwer (PI), Marc Breton (Grant PI), Mark DeBoer (I), L.G.-F. (I), Daniel Cherñavvsky (I), Jessica Robic, E.E., Mary Voelmle, Katie Conschafter, Kimberly Morris, Charlotte Barnett, Kelly Carr, Jacob Hellmann, Matthew Kime, Mary Oliveri; Barbara Davis Center for Diabetes, University of Colorado, Anschutz Medical Campus, Aurora, CO: R.P.W. (PI), Greg Forlenza (I), G. Todd Alonso (I), Robert Slover (I), L.H.M. (I), E.C.C. (I), Emily Jost, Cari Berget, Lindsey Towers, Samantha Lange; Department of Pediatrics, Division of Pediatric Endocrinology and Diabetes, Stanford University School of Medicine: B.A.B. (PI), David Maahs (I), Rayhan Lal (I), L.E. (I), Lisa Norlander (I), K.K.H. (I), Marissa Town, Christine Weir, Kerren Smith, L.J.H., Deanna Shinksy, Julia Viana; Yale University: E.C. (PI), Stuart Weinzimer (I), Kate Weyman (I), L.C., Melinda Zgorski; Jaeb Center for Health Research: K.J.R., R.W.B., Sarah Borgman, Jessica Rusnak, L.G.K., Craig Kollman, Carlos Murphy; National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): Guillermo Arreza-Rubin (Project Scientist), Neal Green (Project Manager); iDCL Steering Committee Members: Boris Kovatchev, Sue Brown, Stacey Anderson, Marc Breton, Lori Laffel, Jordan Pinsker, Carol Levy, Yogish C. Kudva, R.P.W., B.A.B., Francis Doyle III, Eric Renard, Claudio Cobelli, Yves Reznik, Guillermo Arreza-Rubin, John Lum, R.W.B., K.J.R.; Central Laboratory—University of Minnesota Advanced Research and Diagnostic Laboratory: Robert Janicek, Deanna Gabrielson.
Author Disclosure Statement
E.C.C., L.G.K., E.C., L.C., and E.E. have no relevant disclosures to report. L.E. reports receiving consultancy fees from Tandem Diabetes Care. B.A.B. reports receiving donated supplies from Dexcom, grant support paid to Stanford from Tandem, Medtronic, Convatec, Insulet, and Lilly, and personal fees from Medtronic Diabetes, Convatec, Profusa, and Novo-Nordisk, Tandem, Insulet, Tolerion, and Profusa and holding patent 61197230 issued. K.K.H. received support from Dexcom, Inc for an investigator-initiated study and consultant fees from Lifescan Diabetes Institute, Cecelia Health, and Cercacor.
L.J.H. reports owning stock in Dexcom and Tandem Diabetes Care. L.H.M. has received speaking/consulting honoraria from Tandem Diabetes, DexCom, Inc., and Capillary Biomedical. Her institution receives research grants from Medtronic, Tandem Diabetes, DexCom, Abbott, and Insulet Corp. M.J.S. reports receiving grant support, paid to University of Virginia, from Medtronic and Tandem Diabetes Care during conduct of study and grant support from Insulet, paid to University of Virginia beginning at time of submission. K.J.R. reports receiving grant support and donated supplies, paid to the Jaeb Center for Health Research, from Abbott Diabetes Care, Beta Bionics, and Dexcom, and grant support, paid to the Jaeb Center for Health Research, from Tandem Diabetes Care. R.W.B. reports receiving grant support and donated supplies, paid to the Jaeb Center for Health Research, from Abbott Diabetes Care, Ascensia Diabetes Care US, Beta Bionics, Novo Nordisk, Roche Diabetes Care, and Tandem Diabetes Care; grant support, donated supplies, and consulting fees, paid to the Jaeb Center for Health Research from Dexcom; and consulting fees, paid to the Jaeb Center for Health Research from Bigfoot Biomedical, Eli Lilly and Company, and Insulet Corporation. R.P.W. reports receiving grant support, paid to University of Colorado, from Dexcom, Eli Lilly, and MannKind Corporation and advisory board fees from Eli Lilly and Company and grant support, paid to University of Colorado, and travel support and lecture fees from Tandem Diabetes Care. L.G.-F. reports receiving consulting/speaking fees from Abbott Diabetes Care, Astrazeneca, Dexcom, Johnson and Johnson, and Merck. L.G.-F. also has been licensed by the University of Virginia to form an LLC to distribute and charge licensing fees for the use of the Hypoglycemia Fear Survey in studies conducted by for-profit entities including pharmaceutical companies. However, there were no licensing fees involved for the use of the survey in this study. The survey is always available to use free of costs to nonprofit entities.
Funding Information
This study was funded by Tandem Diabetes, Inc., and the National Institute of Diabetes and Digestive and Kidney Diseases. Tandem Diabetes Care provided the experimental closed-loop systems used in the trial, system-related supplies including the Dexcom CGM and Roche glucometer, and technical expertise.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.