
Abstract
Objective:
An emerging group of people with type 1 diabetes are building and using their own artificial pancreas systems (APS). Currently, these “user-led,” open-source systems are not endorsed by regulatory bodies. People face multiple challenges when building and using open-source APS (e.g., lacking required technical knowledge, difficulties sourcing hardware). We explored the experiences of adults with type 1 diabetes using open-source APS to understand how they are navigating these challenges.
Research Design and Methods:
We conducted semistructured telephone interviews (October 2018 to January 2019) with Australian adults about their experiences using an open-source APS. Interviews were recorded, transcribed, and analyzed thematically.
Results:
Participants included 23 adults with type 1 diabetes, aged 25–64 years, 10 (43%) women, with 1–34 months of experience of open-source APS. Participants used four key strategies to navigate challenges: (1) peer support, (2) self-sufficiency, (3) risk management, and (4) trade-offs. Participants relied on peer support and self-sufficiency to fill perceived gaps in professional and industry support. They felt that using an open-source solution was no riskier than previous management and demonstrated a conscious weighing-up of risks. Overall, participants felt that the experienced benefits for their physical health and quality of life outweighed the challenges and potential risks.
Conclusions:
Adults with type 1 diabetes are applying several interweaving psychosocial and practical strategies to navigate the challenges of building and using open-source APS. The findings highlight the importance of health professionals' showing support and understanding for those choosing to use an open-source APS.
Introduction
Commercial diabetes technologies have been advancing rapidly over recent years. However, these must undergo lengthy trials and industry and regulatory processes. Some people in the diabetes community have become frustrated with the resulting delay to industry providing timely solutions that are responsive to the needs of their community.
The “We Are Not Waiting” movement 1 refers to a group of people in the diabetes community who are creating their own solutions, such as open-source artificial pancreas systems (APS). Open-source APS combine continuous glucose monitors, insulin pumps, communication devices, small computers, and smartphone technology to automate insulin delivery using an algorithm. 2 This is also commonly referred to as “looping” or “do-it-yourself” (DIY) APS. However, as the term “DIY” can have negative connotations (e.g., amateur, unreliable), and the individual user benefits from the community development of these resources, in this article we refer to these technologies as “open-source APS.”
The details of how to build an open-source APS are available online. Using these community developed resources, users can build these systems supported by their community both online and in person. Although the open-source software does not currently have regulatory approvals, individuals can build an APS for their personal use. 3
A review of the emerging literature found that several benefits of open-source APS are reported consistently: “decreased HbA1c, increased time-in-range, reduced glucose variability, reduced episodes of hypoglycemia, less reliance on accuracy of carbohydrate counting, improved overnight control, and reduced cognitive burden.” 4 A recently published study has further demonstrated these glycemic benefits using a large sample size (558 participants) and a real-world, prospective design. 5 In addition, some studies have also reported improvements in subjective sleep quality, 6,7 increased confidence, increased energy, and reduced mood swings. 8
However, there are also challenges associated with open-source APS. These include sourcing hardware, a lack of technical knowledge, financial costs, having to use out-of-warranty devices (for some systems), and a potential lack of support from health professionals. 5,9 –11 Some of these challenges relate to open-source APS not being subjected to rigorous randomized-controlled trials to demonstrate safety and efficacy. Diabetes organizations in Australia, Denmark, Poland, and the United Kingdom have released position statements 12 –16 stating that although open-source APS are not regulated, people with diabetes choosing to use an open-source APS should continue to receive support from their health professional(s).
While evidence is emerging on the challenges, there is limited evidence about how people navigate these. Two studies have shown that peer support via online communities assisted in overcoming some of the encountered difficulties. 9,17 However, these studies were conducted among carers and peer mentors. To date, no studies have focused explicitly on how adults using this novel technology have navigated challenges. Understanding the strategies that people use may help those wishing to do similar and may also help health professionals to provide better support. 18,19 Thus, our aims were to explore how Australian adults with type 1 diabetes navigate the challenges associated with building and using an open-source APS.
Materials and Methods
We conducted semistructured interviews to enable participants to raise any topic they deemed important, and to describe their experiences in their own words. Ethical approval was obtained from Deakin University Human Research Ethics Committee (HEAG-H 149_2018).
Participants and recruitment
Participants were eligible if they were English-speaking adults (aged ≥18 years) living in Australia, had type 1 diabetes (for ≥1 year), and were using an open-source APS. Individuals who had been diagnosed with type 1 diabetes for less than 1 year were not considered eligible as they may still be adjusting to the diagnosis and management.
Participants were recruited via advertisements on social media, the website of the Australian Centre for Behavioural Research in Diabetes (ACBRD), and the Australian closed Facebook group, “Aussie, Aussie, Aussie, Loop, Loop, LOOP!.” Purposive sampling was used to achieve an even spread of participants across age, gender, and duration of open-source APS use (<1 year vs. >1 year).
Interview schedule and procedure
The semistructured interview schedule was designed by the authors, most of whom are experienced in health or clinical psychology and qualitative research, and one who has type 1 diabetes and personal, current experience of using an open-source APS. The interview schedule was broad, enabling exploration of participants' experiences of “looping,” including their reasons for “looping,” their perceptions of its advantages and disadvantages compared with their previous management; their confidence in and concerns about open-source APS use; and the involvement of their health professional in their decision to “loop,” their views on future APS, and their expectations of its impact on their diabetes care and daily life.
Before participating in the interview, potential participants were contacted via telephone and asked a few brief questions to determine their eligibility for the purposive sampling. Interviews were conducted by telephone and audio recorded between October 2018 and January 2019 by E.H. After the interview, participants completed a short demographic questionnaire. Audio recordings were transcribed verbatim by a professional service and checked by a member of the research team.
Data analysis
Deidentified transcripts were imported into NVivo 12 (QSR). A thematic analysis approach was conducted.
20
After familiarization with the content by listening to audio recordings and repeated reading of transcripts, a data-driven (inductive) approach was used to generate initial codes. The content of the entire data set was coded inclusively by
A coding framework was revised—to include benefits, challenges, and strategies participants used to navigate these challenges—and approved by all authors. Using the revised framework, two transcripts were double-coded by
Results
Of the 26 enquiries received, all of which were eligible, 1 person subsequently declined, and 2 did not respond to contact. A total of 23 interviews were conducted. The mean interview time was 52 min (range: 34–70 min). Participant characteristics for the 23 participants are displayed in Table 1. Demographics were only collected after the interviews were conducted, and so, details are not provided for the individuals who declined to participate.
Participants' Demographic and Clinical Characteristics (N = 23)
Data are n (%) or median (range) [interquartile range].
APS, artificial pancreas systems.
Participants described multiple challenges associated with building and using open-source APS (Table 2). Many of these challenges were common to both open-source APS and commercial APS: financial costs, lacking technical knowledge, and health professionals being unfamiliar with new technology, technical issues, and internet connectivity issues. For example, the greatest financial cost reported was that of the continuous glucose monitoring device and sensors (an integral part of all open-source APS), which are commercially approved but not necessarily reimbursed or subsidized for all users:
Challenges Faced by Participants with Type 1 Diabetes at Initiation of Open-Source Artificial Pancreas Systems and with Its Ongoing Use
“You know, the biggest hindrance of course to doing any of this is the cost of the CGM. That's obviously the biggest issue with it all” (ID6, male, duration of open-source APS use 0.4 years).
However, some of the experienced challenges were unique to building and using an open-source APS (Table 2). These included their own or others' perceptions of the potential risks involved (e.g., concerns about using older or out-of-warranty devices, or software that had not received regulatory approvals).
Other unique challenges were sourcing specific hardware (particularly second-hand, out-of-warranty devices or specialty medical equipment from overseas), lacking specific technical knowledge (coding), and a potentially time-consuming setup independent of health professional guidance. The ongoing challenges of not using a commercial device meant that they could not access formal customer support for some aspects of their management (e.g., out-of-warranty devices, questions regarding open-source APS software), and some health professionals were unwilling to support the use of an open-source APS. Finally, participants perceived an increase in the number of components they had to carry around compared with their previous management, and that using a smartphone/watch to control their open-source APS impacted their screen time use and battery drain.
Participants reported several interweaving psychosocial and practical strategies to navigate these challenges, which are detailed below. Figure 1 provides a graphical representation of strategies used to address each challenge.
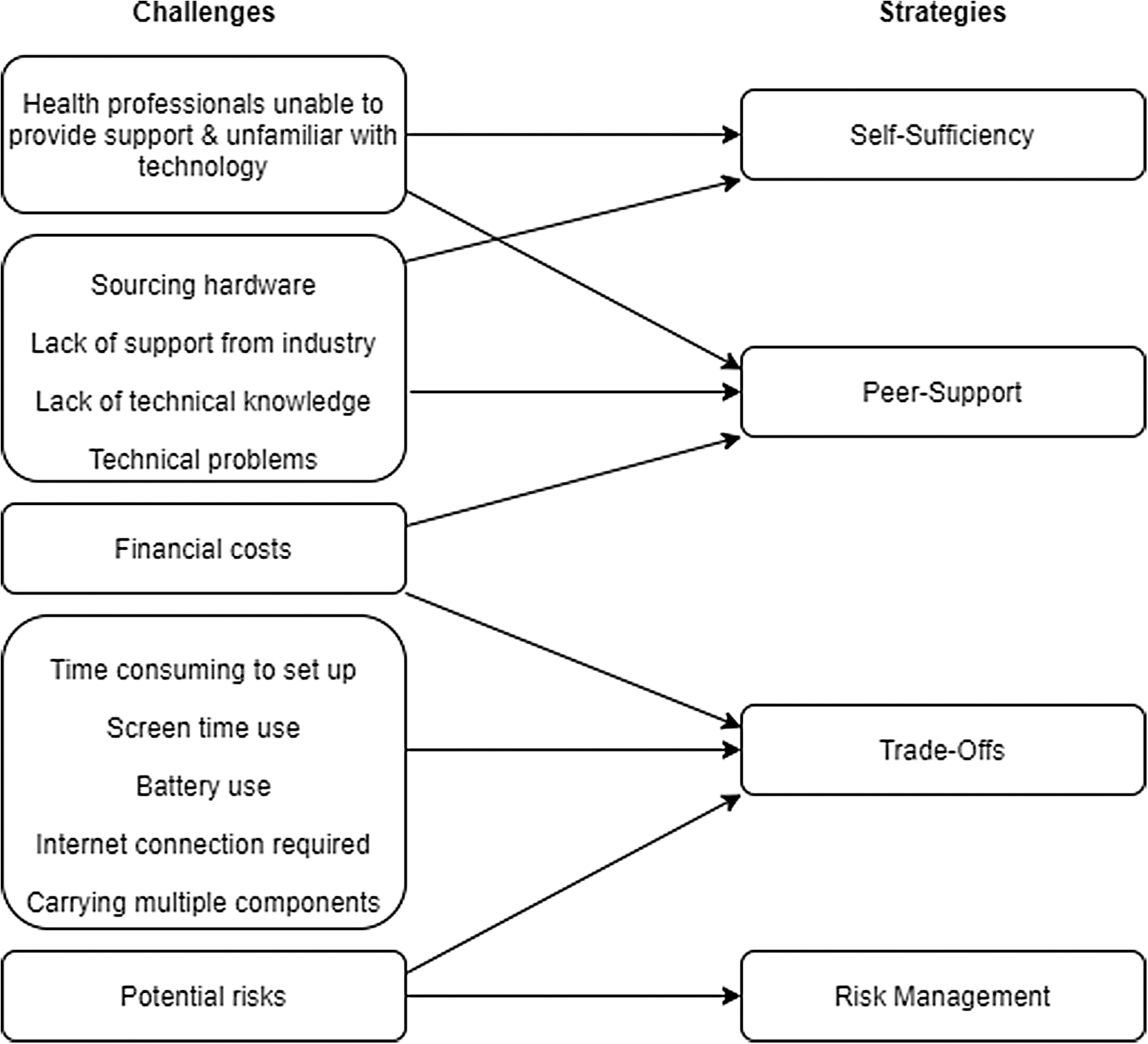
Strategies participants use to navigate the challenges of building/using open-source APS. APS, artificial pancreas systems.
Peer support
When participants needed support, they turned to other people with diabetes. Peer support communities were available online (e.g., social media groups) and at in-person gatherings. Participants described a generous community with a “pay-it-forward” mentality. Peers were described as more knowledgeable about open-source APS than health professionals. They had confidence in their peers due to their shared experience in managing type 1 diabetes and their experience with open-source APS: “I have more faith in [peer] than my own doctor…for things around looping and how to manage diabetes” (ID21, F, 0.3 years).
Participants also felt that their peers were more knowledgeable than industry customer service agents: “I posted something up on the group. Somebody came back within about ten minutes… good written information tends to rise to the top very quickly, whereas we've all had that experience where you speak to somebody in a call centre, and you know you're with the wrong person, and unless you can shake them [get rid of them], you're never going to get the answers that you want” (ID10, M, 0.4 years).
Participants generally spoke about needing to be “tech savvy” to set up their open-source APS. Some lacked this technical knowledge and struggled with issues such as programming software for the first time. For them, peer support was essential: “Through the Facebook group I think lots of technological novices as such build their own systems because they felt empowered by the support that they have to do it themselves” (ID17, M, 0.3 years).
Some also received technical support from family members, usually their partners or adult children: “My husband actually is much more tech savvy than me… He certainly helped me a lot, well in fact he does a lot of the technical side of it” (ID14, F, 0.5 years).
Participants described the online written instructions (the “docs”) on how to set up the system as “very self-explanatory” (ID3, M, 0.6 years). Participants were also able to attend “build parties,” where they met peers in-person to receive practical support in setting up their open-source APS. Once participants had finished setting up their open-source APS, they found it simpler to maintain. If they had day-to-day technical problems to troubleshoot, they were able to ask their peers online. Participants described that online peer support was easier to access than support from health professionals or manufacturers, as they received faster responses and this support was available “24/7”: “The online support today… is second to none… if I tried to get hold of my endocrinologist because I needed something tomorrow he might make an appointment for me in three weeks' time…but, I can post a question online and I get three answers within half an hour” (ID2, M, 2 years).
Peers also assisted sourcing the necessary hardware required to run an open-source APS. Participants reported being able to source parts “for free, or for very little cost” (ID23, F, 0.6 years) through peer support. Purchasing second-hand equipment was “cheaper than buying it direct from the manufacturer” (ID11, M, 0.2 years).
“Kind people are donating [insulin] pumps when they don't need them anymore…the kindness of others has been overwhelmingly wonderful” (ID21, F, 0.3 years).
Self-sufficiency
Participants described their health professionals lacking knowledge about open-source APS and being unable (sometimes unwilling) to provide support. As a result, participants had to be more active in their diabetes management and decision-making. They were both burdened and empowered by this: “You're doing it by yourself… you typically have a doctor or some person that's helping you… Doing looping, the medical professionals don't have any expertise on this. So, you're really alone. So it's, I mean, it's a huge feeling of empowerment, and that's good, but on the other hand… it would be really good to be able to do this with somebody” (ID16, M, 0.8 years).
This created a feeling of ambivalence: “It's still a huge burden. It's still frustrating. But it's changed in the sense that I feel a little more in control…it's having a crutch to help you walk…it's an extra support” (ID16, M, 0.8 years).
While participants felt less reliant on health professionals, and understood they could not endorse or provide specific advice on open-source APS, ideally, participants wanted health professionals to be more knowledgeable and supportive: “I feel more independent of [health professionals] now though, so I'm happy to look at things and to make adjustments myself. But, I think it would be a good thing for her and the team to understand the benefits, and to be able to talk about it in detail” (ID23, F, 0.6 years).
Participants described open-source APS as “a tool that actually works” (ID19, F, 0.1 years) that “empowers me to be able to manage my diabetes better” (ID1, F, 0.6 years). Participants felt a “sense of accomplishment” from successfully building an open-source APS: “I made this. I built this. Look what it's doing… you can't beat that sense of I did this, God I'm smart” (ID4, F, 1.2 years).
The use of open-source APS enabled clarity of information, and visibility of glucose levels being well managed by algorithms throughout the day and night: “The main advantage is that I have very good clarity over how my diabetes is being managed… and also a level of agency and…the ability to affect the outcome is greater…I can now kind of see and also adapt much better” (ID10, M, 0.4 years).
As a result, participants described a new (or renewed) confidence and an improved relationship with type 1 diabetes: “To be honest, I have had a massive confidence hit in general since being diagnosed…the last few months that I've been looping has given me back some of that confidence” (ID1, F, 0.6 years).
Overall, participants described that they felt more empowered, with greater personal control of their condition, compared with their previous self-management: “In 34 years of living with type 1, it's the very first time that I've felt absolutely in control of what's happening” (ID4, F, 1.2 years).
Risk management
Participants were acutely aware of the potential risks associated with using unregulated technology, such as using out-of-warranty devices, and algorithms that have not been trialed for safety/efficacy. However, participants demonstrated a conscious weighing-up of risks versus benefits: “There's risk in everything. In every decision you make or you don't make … the risk in me waiting three more years to get my blood sugar in better control” (ID 18, M, 2.8 years).
They expressed detailed understanding of the risks, but they felt it was the best option available to them at this point in time: “We're all doing it ourselves because there's not a good enough solution on the market” (ID18, M, 2.8 years).
Some participants did not perceive it as a risk to use a system developed by people with diabetes rather than by a medical company. In fact, some believed it was advantageous as the developers had built it for themselves and were therefore motivated to ensure safety: “I feel comfortable using these systems knowing that the people who are creating the systems and the algorithms behind them, are actively using that themselves and they wouldn't want to hurt themselves” (ID17, M, 0.3 years).
Furthermore, participants believed that real-world use has demonstrated that the algorithms are safe to use and are potentially more meaningful than randomized-controlled trial evidence: “There are now many, many people worldwide using that system…it hasn't been a randomised control trial where they only pick patients who are doing well…they've maintained safety in very rigorous real life situations because people with type 1 diabetes don't live in the randomised control trial world. They live in the real world” (ID4, F, 1.2 years).
Participants explained that most of the system components were approved technology, while some parts had not received regulatory approval, such as the algorithms and communication devices. Furthermore, the algorithms were automating decisions and actions that people with type 1 diabetes would have made manually: “The math isn't new. It's just the fact that it's [the algorithm] doing it again and again and again in the background” (ID8, M, 1.2 years).
Participants believed that using an algorithm to administer insulin was no different to making those decisions themselves, and no more dangerous than the usual self-management: “Some people have a fear about an algorithm determining how much insulin goes into your body but that's no different to you making a mistake or giving insulin and forgetting to eat” (ID12, M, 1 year).
Participants carried backup options of all the necessary parts in the event of hardware failure: “I carry numerous spare pumps, spare phone, spare CGM, spare systems with me at all times so that if any one part of the system fell over I can be Looping again within half an hour” (ID2, M, 2 years).
Participants also knew that if the software failed, their system would turn off and the insulin pump would revert to previous manual settings: “At the end of the day, if the looping software on my phone fails, my pump just reverts to its basic standard” (ID6, M, 0.4 years).
Trade-offs
Although there were challenges associated with open-source, participants reported that using an open-source APS was worth it for the benefits they experienced. They referred to making “trade-offs,” for example, persevering with initial, short-term challenges involved in building the system to experience valuable, long-lasting benefits. Setting up an open-source APS required a considerable initial personal investment of time, effort, and sometimes, money (which was often supported by their peers). Participants also listed ongoing benefits that made these early difficulties worth it, such as a reduction in cognitive burden and spending less time on diabetes management tasks every day: “Looping has gifted me an extra hour of non-diabetes time every day for the rest of my life” (ID2, M, 2 years).
After participants set up their open-source APS, there were also ongoing challenges that they were unable to resolve, such as financial costs, screen time use, battery use, internet connectivity issues, and the need for carrying multiple components. Participants traded these off against the ongoing benefits they experienced compared with previous management, such as improved sleep quality, more stable, predictable, and in-range glucose levels, and the freedom to think less about their diabetes. For example, although there were ongoing financial costs associated with running an open-source APS, participants considered this acceptable: “There's ongoing costs… But, personally I'm always happy to foot that with this closed system, it's just making my life so much easier” (ID17, M, 0.3 years).
Not only did participants believe that using an open-source APS was better than their previous forms of diabetes management, they also reported that open-source APS provided benefits not offered by current commercial systems. They appreciated the interoperability, customizability, and ability to evolve that was specific to an open-source APS.
“I will never, never, ever consider looking at a commercial based system…The algorithm that I use is updated weekly. We add patient led innovation. We're able to customise, personalise and add additional features and benefits every day. And, we can keep improving upon a system without the need for clinical trial, testing, evaluation and then approvals” (ID2, M, 2 years).
As a result of the health benefits and improved quality of life that participants experienced, they were more hopeful about their future with diabetes and expected to live longer and have a decreased risk of diabetes-related complications: “[Previously] I thought I might lose my toes and I might be in a wheelchair one day. [Now] I have more hope that I will be extending my quality of life as well as quantity so that I can hopefully just be a grandma” (ID19, F, 0.1 years).
Overall, participants reported that “the rewards outweigh the cons” (ID7, F, 0.3 years), and it is “all worthwhile” (ID8, M, 1.2 years).
Discussion
In recent years, people with diabetes have created their own user-led, open-source APS, without support from health professionals or industry. In this study, we have identified several interweaving strategies that people with diabetes are using to help them to navigate the challenges associated with doing this: peer support, self-sufficiency, risk management, and trade-offs.
Peer support has moved from an adjunct to a primary role, filling a gap in professional and industry support. Some see their peers as more knowledgeable and easier to access compared with traditional support. Participants are highly self-sufficient, sourcing hardware themselves, solving technical issues with the help of peers, and feel empowered by the additional control and understanding they experience. When it comes to managing the perceived risks of using open-source APS, they are using a process of rationalizing and planning to navigate these challenges. People have multiple backup components and plans in case something goes wrong. Finally, they are making conscious trade-offs, weighing up the pros and cons of using their open-source APS to obtain the outcomes that they have always hoped for.
Overall, participants felt that the benefits for their physical health and quality of life outweighed the challenges and potential risks.
Diabetes management has always been “do-it-yourself”: people with diabetes have always had to navigate the challenges of accessing and managing their care every day themselves. 21 Furthermore, people with diabetes have been modifying their own devices for decades. 2 Although participants were using a “do-it-yourself” system, they perceived that they were not doing this alone: they were supported by their peers.
The current study shows how people are navigating the unique challenges brought about by the nature of this open-source technology and the switch from a health professional-driven approach to one that is user-driven. Our study has several novel findings, and also provides support to existing literature.
Our study is the first to provide in-depth data on the role of peer support in navigating the challenges of open-source APS from the perspective of adults using this technology. Our study further supports existing studies on open-source APS showing that peer support is essential for sourcing hardware and assisting with a lack of technical knowledge. 9,17
A particularly novel finding in this study was that participants referred to remaining on their previous diabetes management approach as a risk, due to higher HbA1c and the potential health implications of this (e.g., increased risk of complications). Participants described thoughtful approaches to the risks involved in building and using an open-source APS and, by doing so, felt confident that this posed no greater risk than, and eliminated some risks posed by, their previous management. Participants weighed up risks and decided how they defined a risk. 22
Another important finding was participants' trust in their system compared with commercial systems, which may be due to the level of control they had, having built it and customized it themselves. A commercial hybrid closed loop (HCL) trial showed that participants attempted to override their system when they did not trust it or did not feel satisfied with the targets set by industry. 23 Participants in our study demonstrated both trust and control. A key factor in people discontinuing use of commercial HCL systems is that they believe they can achieve better glucose outcomes, more easily, without the HCL. 24 Comparatively, our participants reported greater satisfaction with their glucose levels than they had experienced with their previous management, and it was easier to achieve.
A key strength of this study is the use of an in-depth qualitative study design to explore this topic, which has not been researched previously. However, there are also limitations of this method and our recruitment strategies.
Our study recruited people in Australia, and their experiences may be different to those living in other countries. As we recruited from social media groups, these participants may have been more likely than the broader community of adults with type 1 diabetes to use online communities to seek support. Potentially, those who did not experience challenges may not have needed to utilize these online communities or those who experienced the greatest challenges may have already discontinued their use of open-source APS. Our study is also subject to self-selection bias, as these people may be somehow more motivated, engaged, or privileged in their diabetes care than the broader community.
The interviews were conducted between late 2018 and early 2019, and as this technology is rapidly changing, some findings may no longer apply. One of the strengths of this study was the diversity in the length of time using open-source APS among the sample, which offered different perspectives. Many participants were early adopters (or pioneers) of this approach: one-third had been using an open-source APS for over a year.
Consequently, there may be some recall bias regarding early experiences among these relatively long-term users. These participants were also using open-source APS before there was clear guidance for health professionals; the Diabetes Australia position statement was launched in Australia in August 2018. 12 Therefore, this sample may have faced additional challenges that are no longer applicable to those who are choosing to use and build an open-source APS today.
Furthermore, we only interviewed those who were currently using an open-source APS. Therefore, our results may be overly positive as we have not interviewed people who did not proceed with building or using an open-source APS. They may have been unable to overcome the challenges we have identified, or they experienced other challenges or barriers we have not detailed here. Future studies are needed among these groups to identify these additional challenges and barriers to using open-source APS.
An important finding in line with previous research 7 was that participants cited a lack of health professional understanding and support as one of the main challenges they experienced. Although participants in our study understood that health professionals could not endorse or provide specific advice on open-source APS, ideally they wanted health professionals to be more knowledgeable and supportive. Previous research has shown that the majority of people with diabetes using open-source APS do not feel that health professionals have a good understanding of the approach, 7 and this is supported by surveys and workshops among health professionals. 25,26 Health professionals also report they feel that they have limited knowledge on open-source APS and are therefore cautious due to a lack of confidence and clarity on what is permitted. 25,26
The use of open-source APS may add complexity to the relationship between health professionals, creating a scenario where the user is potentially more knowledgeable about the technology and data than the health professionals. This is in contrast to previous clinical practice, where health professionals were considered the experts. 27 Health professionals are faced with a dilemma 27 : on one hand is their perceived liability, but, on the other, they have a duty of care to support the persons with diabetes to manage their condition in a way that best suits them to achieve the best outcomes possible. 28
The challenges associated with new technologies are not new: historically, there have often been skepticism and caution from health professionals toward unfamiliar diabetes technology, such as continuous subcutaneous insulin infusion 29 and self-monitoring glucose levels at home. 30 These techniques were once considered revolutionary 30 and potentially dangerous 31 but are now widely accepted as the standard of type 1 diabetes care. This has demonstrated to health professionals that people with diabetes can manage their condition themselves. 31 Open-source APS is just another (although more user-driven) example of technology moving forward. There is a need for formal clinical guidelines to be developed in collaboration with those using open-source APS, to inform health professionals on best practice. 25
Conclusions
In summary, this study provides novel data on the strategies that adults with type 1 diabetes are using to navigate the challenges of open-source APS. It is evident that the world of diabetes care is evolving rapidly, and that people with diabetes are no longer relying on industry or health professionals to provide the solutions they need. As we progress toward fully automated APS becoming the norm, it is vital that health professionals adopt a person-centered approach to diabetes technology 32 and are informed about the latest developments. People with diabetes are not waiting.
Footnotes
Acknowledgments
We thank the people with type 1 diabetes for volunteering their time and insights to this study.
Authors' Contributions
The interview schedule was designed by C.H., J.Sp., R.S, T.S, and E.H. Participant recruitment and management were conducted by C.H. and E.H. All interviews were conducted by E.H. The data were analyzed by
Author Disclosure Statement
No competing financial interests exist.
Funding Information