
Abstract
Background:
The COVID-19 pandemic has impacted the conduct of clinic visits. We conducted a study to evaluate two academic laboratories' fingerstick capillary blood collection kits suitable for home use for laboratory measurement of HbA1c.
Methods:
Four clinical sites recruited 240 participants (aged 4–80 years, HbA1c 5.1%–13.5%). Capillary blood samples were obtained by the participant or parent using collection kits from two laboratories (University of Minnesota Advanced Research and Diagnostic Laboratory (ARDL) and Children's Mercy Hospital Laboratory (CMH)) and mailed under varying shipping conditions by United States Postal Service to the laboratories. Comparisons were made between HbA1c measurements from capillary samples and contemporaneously obtained venous samples. The primary outcome was percentage of capillary HbA1c values within 5% of the corresponding venous values.
Results:
HbA1c values were within 5% of venous values for 96% of ARDL kit specimens shipped with a cold pack and 98% without a cold pack and 99% and 99%, respectively, for the CMH kits. R2 values were 0.98, 0.99, 0.99, and 0.99, respectively. Results appeared similar across HbA1c levels and for pediatric and adult participants. Usability survey scores were high.
Conclusions:
Capillary blood collection kits, suitable for home use, from two academic laboratories, were demonstrated to be easy to use and provided results that are comparable with those obtained from venous specimens. Based on these results, there is strong evidence that HbA1c measurements from capillary specimens obtained with these specific kits can be used interchangeably with HbA1c measurements from venous specimens for clinical research and clinical care.
Introduction
Telemedicine visits have been shown to be effective for management of diabetes. 1 –4 The importance of such visits has become greater during the COVID-19 pandemic, both for clinical care and for the conduct of research studies. Although the use of continuous glucose monitoring has provided a method to assess glycemic control remotely among continuous glucose monitor users, for many with diabetes, particularly those with type 2 diabetes (T2D) for whom self-monitoring of blood glucose may be infrequent, measurement of HbA1c is the primary method for assessing glycemic control.
The ability to obtain HbA1c measurements for both clinical care and research studies has been impacted by the restriction on clinic visits placed by many institutions as a result of the pandemic and by study participant reluctance to travel to a clinic or laboratory to have blood drawn. As a result, there has been a need to expand the use of home kits to collect a capillary blood specimen for measurement of HbA1c.
Although home kits are available to measure HbA1c through a capillary fingerstick, it is not known whether such a collection method with transportation to the laboratory under varying conditions can be as accurate as HbA1c measurements after collection through venous blood draw. To address this knowledge gap, we conducted a study to evaluate the accuracy of two academic laboratories' collection kits, suitable for home use, for laboratory measurement of HbA1c.
Methods
The study evaluated collection kits from two laboratories: the University of Minnesota Advanced Research and Diagnostic Laboratory (ARDL) and the Children's Mercy Hospital Laboratory (CMH). The study was conducted at four diabetes centers located in Florida, Georgia, Missouri, and Idaho. The protocol was approved by a central institutional review board.
Participant eligibility included age ≥2 years old, a diagnosis of type 1 diabetes (T1D) or T2D, and no known medical condition or medication that could affect HbA1c. However, there were no explicit criteria for exclusion of potential participants and no testing was performed to evaluate for anemia, renal disease, hemoglobinopathy, or pregnancy. Participants were enrolled with the goal of achieving a broad age range of adults and children and a broad range of HbA1c values.
Informed consent was obtained from participants ≥18 years old and from a parent or guardian for participants <18 years old; assent was obtained from participants 7–17 years old. Baseline data collection included demographic information, diabetes history, and education of participant or parent/guardian (subsequently referred to as parent).
Research laboratory HbA1c collection kits
During the initial phase of the study, each participant sequentially utilized both collection kits. The collection process for both kits involved filling a capillary tube with ∼5–15 μL of blood after a fingerstick, then placing the capillary tube in a collection vial and shaking.
The ARDL kit included a micro-vial containing a capillary tube, a lancet device, a Bio-Rad Hemoglobin Capillary Collection vial containing a solution of Ethylenediaminetetraacetic acid (EDTA), and a small amount of potassium cyanide (part no. 196-2051; Bio-Rad Laboratories, Hercules, CA), as well as an alcohol wipe, gauze pad, bandage, cardboard stand to hold the collection vial, paper instructions, and blood collection form. Packaging materials included a zip-close biohazard bag, an absorbent pad, and a 15.2 × 10.2 × 5.1 cm (6 × 4 × 2 in) cardboard shipping box. The shipment included a frozen cold pack (85 g (3 oz) gel pack, model no. S-13376; Uline, Pleasant Prairie, WI) inserted into the plastic specimen bag along with the sample collection vial.
The CMH kit included a microfuge tube containing a capillary tube, a lancet device, a microfuge tube containing a stabilizing solution containing EDTA, and other undisclosed preservatives (cyanide free). All three components were secured in a foam block insert that was placed inside a 5 × 3 × 3-inch customized shipping box along with the paper instructions and a sealable plastic specimen bag. The CMH kit was mailed without a cold pack.
Figure 1 shows a schematic of the capillary and venous blood collections obtained in the study. The order of using the two collection kits was determined by the last digit of the participant ID number (odd/even; for the purpose of determining the order, randomization was not considered to be necessary since the study objective did not involve a direct comparison of the different laboratories).

Schematic of capillary and venous blood collections.
Although the kits can be used at home, the sample collection was done in the clinic so that a venous blood sample could be readily obtained on the same day. The home environment was mimicked by placing the participants, plus a parent for pediatric participants, in a quiet area of the clinic to obtain the capillary samples using the collection kits unsupervised. The first kit was provided, which included instructions, blood collection tubes, and shipping materials. The instructions, which were written for ARDL and written plus a video for CMH, indicated how to do the fingerstick blood collection and then package it for shipment. The blood collection, processing, and packaging were performed by the participant or parent.
After the process for the first collection kit was completed, including packaging the sample for shipment, a brief usability survey about the collection kit instructions and process was completed by the participant or a parent (whoever primarily carried out the procedure). The mentioned process was repeated for the second collection kit.
The packaged blood samples, which included a temperature recorder (Fresh Tag 1 USB Temperature Data Logger; Freshliance Corp., Zhengzhou, China), were sent to the two laboratories by the United States Postal Service (USPS) as first-class mail.
Venous blood draw
After the capillary blood sample was obtained and packaged for the second collection kit, a venipuncture blood draw was done by clinic staff and aliquoted into three vials, one to send to each laboratory and one retained for later shipment to the laboratories for replicate HbA1c measurements. Within 4 h of collection, the vials were placed in a −80°C freezer until sent on dry ice to each central laboratory weekly by overnight carrier.
Additional optional capillary blood draws
Participants had the option of having several additional fingersticks done by study staff using the collection kits. For participants who agreed, one additional ARDL specimen was collected and sent to the laboratory without a cold pack by USPS and one additional CMH specimen was collected and sent with a cold pack. When possible, another ARDL specimen was collected and sent on dry ice with the venous samples by overnight carrier.
Central laboratory HbA1c measurement
At each of the two laboratories, upon receipt, the laboratory determined whether each specimen was analyzable. HbA1c measurements were made using the Tosoh G8 HPLC system in variant mode (Tosoh Bioscience, Inc., South San Francisco, CA) for both the venous samples and the capillary samples.
Survey
A usability survey addressing the testing kit process and experience was completed by each participant after use of the ARDL and CMH collection kits in the first phase. Surveys consisted of four or five questions on a 5-point Likert scale inquiring about ease of use of the kit, ease of use of the written instructions, ease of use of the video (CMH kit only), amount of pain in obtaining the blood sample, and overall satisfaction level.
Statistical methods
The determination that a collection kit was accurate was predefined to be ≥90% of the analyzable capillary HbA1c values within ±5% of the venous HbA1c values, based on the National Glycohemoglobin Standardization Program (NGSP) standard for laboratory HbA1c testing certification. 5 Sample size was calculated to be 240 to have 90% statistical power with a one-side alpha level of 0.05 to demonstrate that the proportion of capillary specimen HbA1c measurements within 5% of the venous HbA1c measurements was 0.90 assuming the true proportion was 95%.
Separate analyses were conducted for each collection kit comparing the HbA1c value from the capillary sample obtained with the kit with the venous value from that laboratory. For each comparison, summary statistics were computed for the proportion of fingerstick specimen values within 5% of venous values and for the distributions of differences and absolute differences. The 95% limit of agreement 6 was calculated, winsorized at the 10th and 90th percentiles to account for a small number of outliers. Mean difference was computed as capillary value minus venous value.
Summary statistics also were computed comparing the replicate venous sample measurement with the original venous sample measurement as well as comparing the ARDL venous sample with the CMH venous sample measurements. Separate exploratory analyses were performed for adult and pediatric participants and high and low HbA1c values.
Additional analyses compared results of (1) fingerstick specimens sent by USPS with and without a cold pack for both laboratories, (2) ARDL fingerstick specimens sent by USPS versus overnight carrier on dry ice, and (3) ARDL fingerstick specimens sent on dry ice with the corresponding venous specimens. Characteristics of participants and shipping metrics for discordant samples (capillary HbA1c differed from venous HbA1c by >5%) were compared with concordant samples using a logistic mixed model with concordance as the outcome, adjusting for repeated measures by participant ID and a fixed clinical site effect; P-values were adjusted for multiple comparisons using the false discovery rate procedure. Results of the surveys were tabulated separately for each type of collection kit. Analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
Results
The study included 240 participants (204 with T1D and 36 with T2D) ranging in age from 4 to 80 years (126 ≥ 18 years old and 114 < 18 years old) (Table 1). HbA1c from venipuncture ranged from 5.1% to 13.5% (mean 7.8% ± 1.6%) at the ARDL laboratory and from 5.1% to 13.2% (mean 7.9% ± 1.6%) at the CMH laboratory. Five participants did not provide a venipuncture sample for laboratory analysis. Of the remaining 235 venous samples, all were analyzed by ARDL and 223 were analyzed by CMH, with 12 samples determined to be non-analyzable.
Participant Characteristics
One participant reported nonbinary gender.
Diabetes duration missing for three participants.
Education information missing for nine participants; for pediatric participants, education of parent was reported.
Reference HbA1c missing for five people from both laboratories; reference not analyzable for 12 additional samples at CMH.
ARDL, Advanced Research and Diagnostic Laboratory; CMH, Children's Mercy Hospital; IQR, interquartile range; SD, standard deviation; T1D, type 1 diabetes; T2D, type 2 diabetes.
Evaluation of ARDL collection kit
All 240 participants obtained an ARDL collection kit capillary blood sample shipped with a cold pack. Of these, 22 samples were determined to be non-analyzable due to improper collection (n = 5), lost in transit (n = 3), or too old upon receipt (>14 days) per laboratory policy (n = 14); 4 did not have a paired reference venous sample.
Among the 214 analyzable capillary samples shipped with a cold pack, HbA1c measurements were within 5% of the ARDL venous HbA1c measurement for 95.8% (95% confidence interval [CI] 92.2%–98.1%) of samples. The mean difference was −0.02% ± 0.21% (median 0.0%, Fig. 2A) and the mean absolute difference was 0.14% ± 0.16% (median 0.1%), with 64% within 0.1% and 94% within 0.3% (Table 2 and Supplementary Table S1). R2 was 0.98. Results were similar for collection kit samples shipped without a cold pack by USPS or shipped on dry ice by overnight carrier (Table 2 and Supplementary Table S1). Across the range of HbA1c levels (Table 3 and Fig. 2B) and for pediatric and adult participants (Table 3), all point estimates exceeded 90% for the percentage of capillary values being within 5% of the venous values.
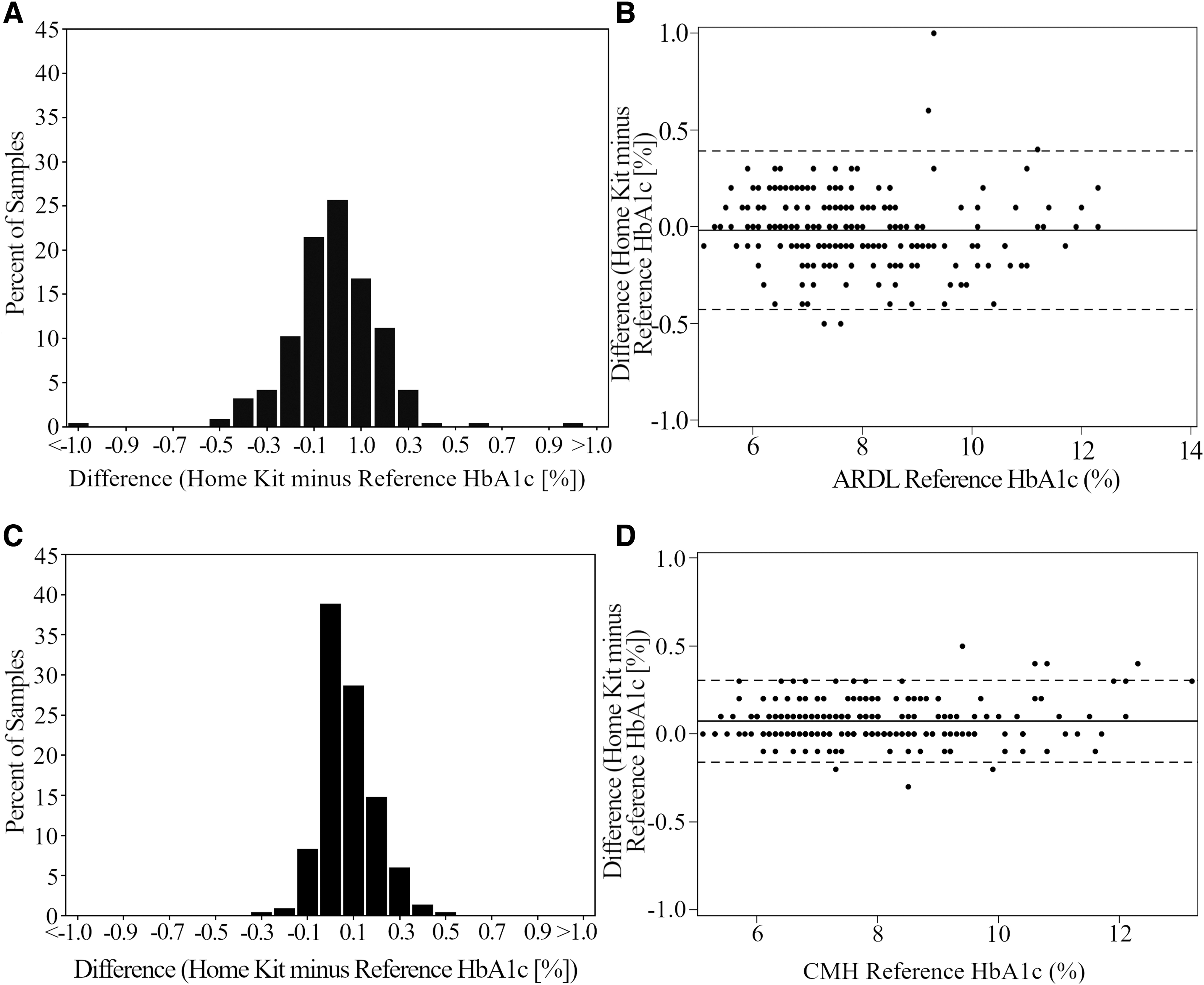
Comparison of ARDL and CMH home kit HbA1c measurements with reference venous HbA1c measurements. Bar graphs show the distribution of differences between the home kit HbA1c values and corresponding venous reference values for ARDL
Advanced Research and Diagnostic Laboratory HbA1c Home Kit Accuracy Analyses a
ARDL home kits: (1) shipped with cold pack by USPS, (2) shipped without cold pack by USPS, and (3) frozen after collection and shipped on dry ice by overnight carrier. ARDL reference is from venipuncture blood draw, frozen, and shipped on dry ice by overnight carrier. Reference samples were frozen at the site, with reference no. 1 sent to the laboratory and analyzed within ∼7 days and reference no. 2 sent and analyzed after an average of ∼50 days.
Difference = first HbA1c method minus second HbA1c method specified in each column header.
CI, confidence interval; USPS, United States Postal Service.
Advanced Research and Diagnostic Laboratory HbA1c Home Kit Accuracy Analysis According to HbA1c Level and Age
Difference = home kit HbA1c minus venous laboratory HbA1c.
Absolute value of the difference.
Comparing the two capillary samples sent by USPS with and without the cold pack, the mean difference was 0.03% ± 0.37% (median 0.0%) and the mean absolute difference was 0.11% ± 0.36% (median 0.1%) with 86% within 0.1% and 96% within 0.3% (Table 2).
HbA1c measurements from primary and replicate venous samples shipped separately (n = 110 pairs) were within 5% of each other for 95.5% (95% CI 89.7%–98.5%) of samples. The mean difference was 0.01% ± 0.21% (median 0.0%) and the mean absolute difference was 0.16% ± 0.13% (median 0.1%) with 55% within 0.1% and 95% within 0.3% (Table 2). R2 was 0.97.
The survey completed by the 175 participants and 34 parents (with 30 completers unspecified and 1 missing) indicated that 91% thought the kit was somewhat or very easy to use and none thought it was very difficult (Table 4, Supplementary Tables S3a and S4a).
Survey Results
Video was not part of the ARDL kit use instructions.
NA, not applicable.
Evaluation of CMH collection kit
All 240 participants obtained a CMH collection kit capillary sample, shipped without a cold pack. Of these, 7 kits were determined to be non-analyzable due to improper collection (n = 5) or getting lost in transit (n = 2), and 17 did not have a paired reference venous sample.
Among the 216 analyzable capillary samples shipped without a cold pack, HbA1c measurements were within 5% of the CMH venous HbA1c measurement for 99.1% (95% CI 96.7%–99.9%) of samples. The mean difference was 0.07% ± 0.12% (median 0.1%, Fig. 2C) and the mean absolute difference was 0.10% ± 0.10% (median 0.1%), with 76% within 0.1% and 98% within 0.3% (Table 5 and Supplementary Table S2). R2 was 0.99. Results were similar for collection kit samples shipped with a cold pack (Table 5 and Supplementary Table S2). Across the range of HbA1c levels (Table 6 and Fig. 2D) and for pediatric and adult participants (Table 6), all point estimates exceeded 90% for the percentage of capillary values being within 5% of the venous values.
Children's Mercy Hospital HbA1c Home Kit Accuracy Analyses a
CMH home kits: (1) shipped without cold pack by USPS, (2) shipped with cold pack by USPS, CMH reference is from venipuncture blood draw, frozen, and shipped on dry ice by overnight carrier. Reference samples were frozen at the site, with reference no. 1 sent to the laboratory within ∼7 days and reference no. 2 sent and analyzed after an average of ∼50 days.
Difference = first HbA1c method minus second HbA1c method specified in each column header.
Children's Mercy Hospital HbA1c Home Kit Accuracy According to HbA1c Level and Age
Difference = home kit HbA1c minus venous laboratory HbA1c.
Absolute value of the difference.
Comparing the capillary samples with and without the cold pack, the mean difference was −0.01% ± 0.07% (median 0.0%) and the mean absolute difference was 0.04% ± 0.06% (median 0.0%) with 95% within 0.1% and 100% within 0.3% (Table 5).
HbA1c measurements from the primary and replicate venous samples shipped separately (n = 88 pairs) were within 5% of each other for 98.9% (95% CI 93.8%–100.0%) of samples. The mean difference was 0.00% ± 0.13% (median 0.0%) and the mean absolute difference was 0.09% ± 0.09% (median 0.1%) with 82% within 0.1% and 99% within 0.3% (Table 5). R2 was 0.99.
The survey completed by 176 participants and 34 parents (with 30 completers unspecified) indicated that 86% thought the kit was somewhat or very easy to use and only one thought it was very difficult (Table 4, Supplementary Tables S3b and S4b).
Shipping logistics
For the primary assessment of each laboratory's kit (with cold pack for ARDL and without cold pack for CMH), median time from collection of blood sample to receipt at the laboratory was 5.0 days (interquartile range [IQR]: 4.0–6.0) for the ARDL laboratory and 7.0 days (IQR: 5.0–8.0) for the CMH laboratory (Supplementary Table S5). The percentage of capillary HbA1c values within 5% of the venous value was reasonably independent of the shipping time, except for a possible slight drop when the shipping time approached or exceeded 10 days (Supplementary Table S6).
For the primary assessments, median maximum temperature during the shipment to the ARDL laboratory was 27.4°C (81.3°F) (IQR: 25.0–30.1°C [77.0–86.2°F]), with 15% exceeding 32.2°C (90°F) and with the maximum being 40.3°C (104.5°F). For shipment to the CMH laboratory, median maximum temperature was 28.4°C (83.1°F) (IQR: 26.2–31.6°C [7.2–88.9°F]), with 17% exceeding 32.2°C (90°F) and the maximum being 40.6°C (105.1°F).
Evaluation of discordant capillary specimens
For capillary specimens with paired venous specimens, discrepancies between the capillary HbA1c and the venous HbA1c exceeding 5% were present for 9 (4%) of the 214 ARDL collection kits shipped with a cold pack, 5 (2%) of the 201 ARDL kits shipped without a cold pack, 1 (<1%) of the 205 CMH kits shipped with a cold pack, and 2 (1%) of the 216 CMH kits shipped without a cold pack (Supplementary Table S6). Pooled together, there were 10 (3%) discordant samples among 394 HbA1c measurements from pediatric (<18 years old) participants and 7 (2%) among 442 HbA1c measurements from adult (≥18 years old) participants.
There was no obvious pattern that distinguished the discordant samples from the concordant samples with respect to participant age, education level, race, HbA1c level, or maximum temperature during shipping. Although shipping transit times did not significantly differ comparing discordant and concordant cases (P = 0.35), there was a suggestion that discordant cases more frequently had transit times of 10 or more days than concordant cases; 5 of 60 (8.3%) with transit time of 10 or more days were discordant compared with 12 of 776 (1.5%) with transit time of <10 days.
There were 199 participants who had a kit sample and a venous sample sent to both the ARDL and CMH laboratories. Among the 199, 190 (95%) of kit sample HbA1c values were within 5% of the venous sample at both laboratories, 2 were within 5% at ARDL but not CMH, and 7 were within 5% at CMH but not ARDL; none were outside the 5% limit at both laboratories.
Discussion
The study results indicate that HbA1c can be accurately measured from a fingerstick capillary blood sample obtained by a patient or parent and shipped to a central laboratory. Both the ARDL and the CMH collection kits for obtaining capillary blood samples easily exceeded the prespecified criterion of having at least 90% of the HbA1c measurements within 5% of the venous blood measurement, and both kits were perceived by the study participants to be easy to use.
The results were consistent across the ranges of HbA1c levels and age (both pediatric and adult). It has been the ARDL's standard to include a cold pack in the shipment and CMH's standard to not have a cold pack, but for both laboratories, the results indicated that the inclusion of a cold pack in the shipment of the capillary specimens did not seem to matter. Likewise, the results were not affected by temperature during shipment even when it exceeded 32.2 or 37.8°C (90 or 100°F) or 100°F. Shipping time also did not seem to be a factor, at least through 10 days.
The results indicate that measuring HbA1c from a capillary sample obtained by an adult with diabetes or parent of a child with diabetes and mailed to a laboratory is feasible. In addition to validating the collection of an HbA1c sample with a fingerstick, the main importance of these findings is twofold. First, in research studies with virtual study visits from home by necessity due to the pandemic or by design, there is now a validated, highly accurate, and reproducible method for measuring HbA1c utilizing the collection kits from either of the two laboratories. Second, for pediatric patients, the results indicate that a venipuncture, which can be challenging to obtain particularly for young children, is not necessary for measurement of HbA1c if one of the kits from these laboratories is used to obtain a capillary specimen.
To be able to broadly generalize the study results, participants included both adults and children with a range of education levels and with both low and high HbA1c levels represented. To assure variation in shipping times and climatic conditions, the study included four geographically dispersed sites, with a portion of the study being conducted during summer months wherein ambient temperature during shipping might be expected to be high, particularly from the two sites in the south. USPS first-class mail was used for shipping since this method would be easiest for patients to use from home. Since there were some shipments that took >14 days to arrive at the laboratory, USPS priority mail might be a better approach to minimize the likelihood of a substantially delayed delivery.
Clinical laboratories that wish to implement methods used in this study should comply with applicable regulations, which, in the United States, would entail a validation of the device by the laboratory and a comment in the report that the method falls under the laboratory-developed test category.
In summary, the study has demonstrated that use of these two capillary blood collection kits that are suitable for home use, with standard postal service shipping to a laboratory, is feasible. Based on our results, there is strong evidence that HbA1c measurements from fingerstick capillary specimens obtained with the two kits evaluated in the study are as accurate as measurements from venous samples, indicating validity of the collection–measurement method. However, these results should be considered to apply to just the kits from these two laboratories, using the methods for processing employed in the study, and not be generalized to other collection kits.
Footnotes
Authors' Contributions
R.W.B. wrote and edited the article. L.E.B. performed statistical analyses and wrote/edited the article. J.W.L., C.K., V.B.L., M.S., M.J.H., B.B., J.T.C., A.A.K., U.G., D.L., J.G.A., M.C., D.G., T.J., and M.A.C. contributed to discussion and reviewed/edited the article.
Acknowledgments
Listing of clinical sites, laboratories, and coordinating center involved in the study. Rocky Mountain Clinical Research: Mark Sulik, Pharm D, CCRP; David Liljenquist, MD; Myrna Lee, CRC; Joann Malone, MA, CCRC; Samantha Thueson. University of Florida: Michael J. Haller, MD; Janey G. Adams, BS; Anastasia Albanese-O'Neill, PhD, APRN; Marilyn Mitchell, MA. Atlanta Diabetes Associates: Bruce Bode, MD; Margaret Clements, PA-C, Alexia Lockwood-Oliviera, Blake Winslett, Laura Sutton, Harvey Salley. Children's Mercy Hospital (Clinical Center and Laboratory): Mark A. Clements, MD, PhD; Uttam Garg, PhD; Joseph T. Cernich, MD; Terri Johnson, MLS (ASCP); Darlene Brenson-Hughes, CCRC; Dara Watkins, MA, CCRP; Cassandra McClain, MHA, CCRC; Rebekah Elliot; Sarah Albert; Sean Tucker, MLS (ASCP); Tasha Kusnir, MLS (ASCP); Dipika Patel, MLS (ASCP); Natalie Sligar, MLS (ASCP); An Hoang; Kelsye Howell, RN. Advanced Research Diagnostic Laboratory, University of Minnesota: Anthony A. Killeen, MD, PhD; Deanna Gabrielson, BS; Julie Idzorek, MT (ASCP); Marcia Aaby, MT (ASCP); Hly Vang. JAEB Center for Health Research: Roy W. Beck, MD, PhD; John W. Lum, MS; Victoria Barnes-Lomen, MS; Laura E. Bocchino, MPH; Craig Kollman, PhD; Carlos Murphy; Paige Miller.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for the study was provided by the Leona M. and Harry B. Helmsley Charitable Trust.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.