
Abstract
Background:
There exist several barriers to physical activity (PA) among adolescent girls. We therefore developed a culturally acceptable dance/fitness intervention called THANDAV (Taking High-Intensity Interval Training [HIIT] ANd Dance to Adolescents for Victory over noncommunicable diseases [NCDs]). The main aim of this study was to evaluate the THANDAV protocol among Asian Indian girls aged 10 to 17 years.
Materials and Methods:
THANDAV consisted of a 10-min routine with high- and low-intensity dance steps that was taught to 23 adolescent girls. Heart rate (HR), energy expenditure, body mass index (BMI), and blood pressure (BP) were recorded. Focused group discussions (FGDs) were conducted after the quantitative measurements were completed.
Results:
The average age of the girls was 13.9 ± 2.1 years, and the mean BMI and BP were 19.8 ± 3.3 kg/m2 and 107/68 (±8/7) mm/Hg, respectively. All participants achieved 80% of their maximum HR during the first dance and managed to sustain this HR throughout the 10-min routine. There was a significant increase in the HR (bpm) [88.7 ± 8.4 to 195.6 ± 11.8, P < 0.001] and VO2 (L/min) [0.025 ± 0.0 to 0.395 ± 0.1, P < 0.001] postintervention. The average energy cost of the activity (metabolic equivalent) was 6.3. The FGDs revealed that THANDAV was a socially acceptable, fun, and energetic form of PA.
Conclusions:
The THANDAV intervention meets HIIT norms and is a novel culturally appropriate form of PA that is enjoyable, takes little time, and can be done at home. It has the potential to be a sustainable intervention to improve cardiorespiratory fitness and prevent NCDs in Asian Indian adolescent girls.
Clinical Trials Registry of India: CTRI/2020/02/023384.
Background
Physical inactivity has been shown to be an independent contributor to noncommunicable diseases (NCDs), which account for two-thirds of all deaths worldwide. 1 Globally, one in four adults is physically inactive, and women are in general less physically active than men, across the world 2 and in India. 3 Reasons for higher physical inactivity in women include time constraints, self-consciousness, lack of confidence, physical inability, lack of encouragement from family members, discomfort with the attire, expensive club and gym memberships, inability to access exercise facilities, unfavorable weather conditions, and exercise not being considered “culturally acceptable.” 4 –6 Lack of physical activity (PA) is a major problem in adolescents as well, with 84% of adolescent girls and 78% of boys being insufficiently active across the globe as of 2010. 4
Among Asian Indian adolescents, the corresponding figures were 76.3% and 71.8%. 7 In addition to the barriers already mentioned, gadget use (including engagement with social media) is a major reason for adolescents not finding enough time to exercise. 8 More specifically among adolescent girls, social norms discouraging playing outdoors away from the home after school were the most commonly cited reason for not being able to perform sufficient exercise. 9 This decline in PA in the adolescent age group puts them at a higher risk for diabetes and NCDs, 10 and may also have deleterious effects on bone and reproductive health. 11 The health penalties of physical inactivity are particularly relevant among Asian Indians as they tend to be at higher inherent risk of developing metabolic NCDs. 12
In view of these barriers to conventional forms of exercise among adolescent Asian Indian girls, we attempted to develop a novel intervention called “THANDAV” (Taking High-Intensity Interval Training [HIIT] ANd Dance to Adolescents for Victory over NCDs) that incorporated the elements of HIIT into common popular Bollywood songs. HIIT regimens have been shown to produce significant reductions in whole body fat mass, weight, and improvement in cardiovascular fitness in both adults and adolescents. 13 Dance is an integral part of Indian culture with each state/region having its own classical dance form. Bollywood dance, which refers to dance forms picturized in the Indian film industry, also enjoys wide popularity. We hypothesized that the combination of dance and HIIT would provide the metabolic benefits of exercise in an acceptable manner to women/adolescent girls in India.
In this study, we aimed to (1) examine whether the THANDAV intervention produced 80% of maximal heart rate (HR) and met HIIT norms, (2) estimate the energy cost of this activity, (3) conduct a qualitative discussion to understand barriers, facilitators, advantages, and acceptability of the intervention, in Asian Indian girls aged 10–17 years.
Materials and Methods
Development of the HIIT-based dance protocol for adolescent girls
THANDAV is a form of freestyle dancing with flavors of Indian classical/folk dance. The THANDAV routine was developed in association with a seasoned choreographer from the South Indian film industry to ensure the ease and safety of the steps being performed. There was a 2-min high-intensity [80% of maximum HR achievement] segment followed by a 30-sec low-intensity (40%–60% maximum HR) segment, and four such repetitions constituted a single 10-min routine. The songs selected were all popular Bollywood/Indian film songs/album hits of the season. The steps were choreographed to be easily done and repetitive. Four songs were selected for a single 10-min routine.
Pilot testing the THANDAV intervention—recruitment of participants
Adolescent girls (n = 23, based on convenience sampling) aged 10–17 years were enrolled into the THANDAV study from two residential colonies in Bengaluru city in south India. The participants were not professional dancers but a few of them (10/23) had been to dance classes (either classical and contemporary) earlier. However, none of the participants had been routinely attending dance classes for 2 months before the start of this study.
A leaflet about the study was placed across two residential colonies in Bengaluru city in south India and also the message was spread through word of mouth and internal resident WhatsApp groups. Interested participants and their parents who volunteered for the study were briefed about the study. Written informed consent from a parent and assent from the adolescent were obtained before the start of the study. Data regarding any underlying medical conditions (none reported) and ability to perform exercise were collected. A unique identification number was created for all participants. The pilot study was approved by the institutional ethics committee (IEC) (Reg. No.: ECR/194/Inst/TN/2013).
Intervention and testing
The THANDAV intervention was taught by a team consisting of a choreographer, scientist, and physician (all trained dancers) as part of a 2-day workshop held at a recreational facility in Bengaluru. The girls were taught the steps and then given 3 weeks to practice and perfect the routine. Weekly calls/meetings with the participants ensured they were practicing the routine and were familiar with the steps.
The testing was performed at the Clinical Research Center, Division of Nutrition, St. John's Research Institute, Bengaluru. Participants reported to the laboratory 2 h after a meal. On arrival at the laboratory, participants were asked to sit quietly in a thermoneutral environment and relax for 15 min. After this, their baseline energy expenditure (EE), using indirect calorimetry with a face mask (MetaMax 3X; Cortex, Leipzig, Germany), 14,15 and HR were recorded.
Participants started with warm-up exercises before the start of the dance protocol. Next, electrocardiogram (ECG) limb lead electrodes were placed on the torso along with their connecting wires placed in a pouch, which was firmly attached to the participant's waist. This allowed the wires to be easily removed and attached to the portable HR monitor in a few seconds. The participants then performed the THANDAV for 10 min continuously, moving freely without any recording sensors interfering with their movement. At the end of every 2 min (HIIT portion of the dance), their ECG was recorded by connecting their limb lead wires to a portable monitor for the measurement of their HR. Their EE was also measured at the end of the 10-min dance routine. Thus, HR was recorded five times during the routine, while EE was recorded before and after. The protocol for measuring EE and HR is shown in Figure 1.
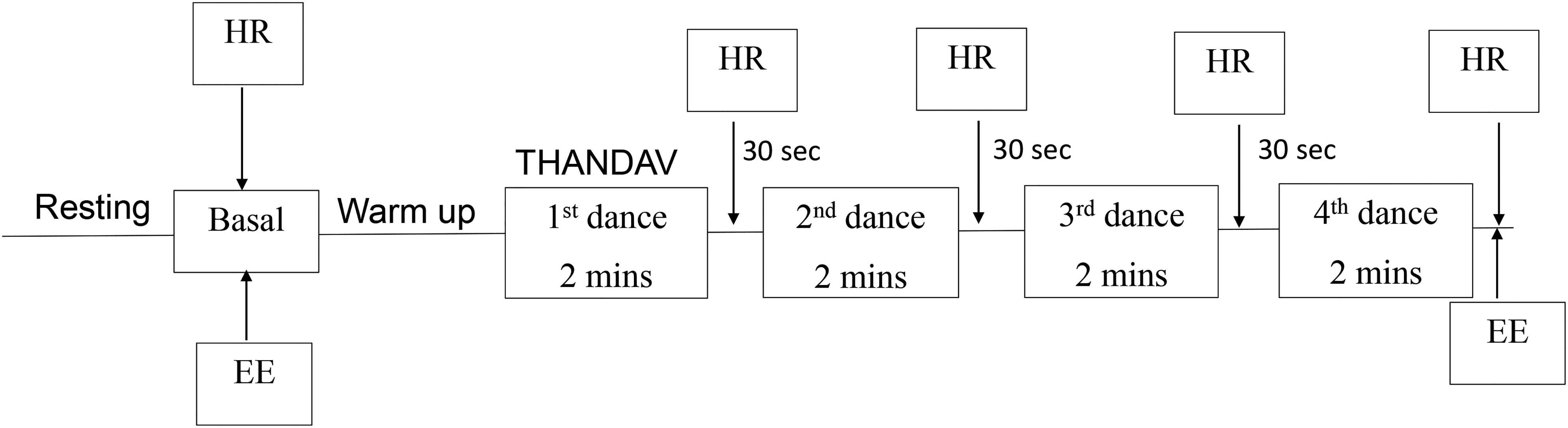
The protocol for measuring Energy Expenditure (EE) and Heart Rate (HR).
Anthropometric measurements
Height and weight were measured at the laboratory, on the day of the experiment, using standardized techniques. All the instruments were calibrated before the measurements were taken. Weight (in kilograms, kg) was measured using an electronic bathroom weighing scale (Tanita, India). Before recording the reading, it was made sure that the participants were wearing light clothing, had removed their shoes and any heavy jewelry. Height was measured to the nearest centimeter (cm) using a stadiometer (Seca, Germany) with the participants standing erect without shoes. For measuring blood pressure (BP), participants sat in a relaxed position with the arm at rest on a table. BP was recorded in the right arm to the nearest 1 mmHg using the electronic OMRON machine (Omron, Vietnam). Two readings were taken 5 min apart and their mean was taken as the final reading of BP.
All the measurements were recorded by trained professionals once the participants had consented and were enrolled for the study. All the readings were recorded in a predesigned report sheet format. A detailed report including all participant measurements was personally handed over to the parents/guardians of the respective participants in a sealed envelope, within 2 weeks after the testing was performed. All patient safety and data privacy regulations were adhered to.
Heart rate
The HR was measured using a digital monitor (Philips, Efficia monitors, CM10) that measured respiratory rate (RR) using ECG leads (part of the Philips monitor). The measurements were taken at five time points: at baseline, and the end of first, second, third, and fourth dances. The readings were taken within 10 s of completion of a HIIT dance segment. At baseline and end of the fourth song, the volume of oxygen consumed (VO2) and volume of carbon dioxide produced (VCO2) were also measured simultaneously with the HR.
Energy expenditure
The VO2 and VCO2 were measured using indirect calorimetry, MetaMax (MetaMax 3X; Cortex), and used to calculate EE using Weir's equation. 16,17 The system was calibrated before the experiments using known concentrations of O2 (15.1%) and CO2 (5.1%), and the error of the instrument was <2%. The measurements were recorded at two points: baseline and postintervention.
For the baseline measurements of VO2 and VCO2, the participants were asked to rest for 15 min, following which a mask was placed through which the participants breathed and the expired air was collected for 10 min. Another measurement was taken immediately after the dance for 10 min and the HR was measured simultaneously. EE was calculated using Weir's equation [EE (kcal/min) = 3.941*VO2 + 1.1*VCO2]. 16,17 For the estimation of baseline EE, the average measurements of VO2 and VCO2 for 5 min were considered. The postintervention EE was calculated from VO2 and VCO2 measured for initial 60 s. An exponential curve fit was applied to estimate EE at the time 0 (Fig. 2a).

Estimation of EE from HR
Each participant was individually calibrated to establish the EE and HR relationship. A calibration curve of EE against HR was made and the slope and intercept were derived for each participant. Using linear equations, EE was estimated for a given HR for each participant (Fig. 2b). The basal and postdance EE corresponding to HR is shown in Figure 2c.
Metabolic equivalent of task
The intensity of PA can be expressed relative to an individual's resting EE, referred to as a metabolic equivalent (MET) of task. An MET is defined as the resting metabolic rate, that is, the amount of oxygen consumed at rest, while sitting quietly in a chair [∼3.5 mL O2/(kg·min)] (1.2 kcal/min for a 70-kg person). As such, work at two METS requires twice the resting metabolism or 7.0 mL O2/(kg·min) and that at three METS requires three times the resting metabolism [10.5 mL O2/(kg·min)], and so on. 18,19 The EE of dance above baseline was used to calculate METs.
Qualitative study—focused group discussions
Two focused group discussions (FGDs) were conducted to assess barriers, facilitators, and acceptability of THANDAV. Discussions were conducted by a moderator (H.R.) and an observer who were trained to conduct FGDs. They first prepared an FGD guide that broadly listed the questions relevant to the study aim to be discussed. The moderator conducted the discussions with participants who were split into two groups based on their residential locations while the observer took notes. The FGD was conducted in a language familiar to all participants (English and Hindi).
The interview began with a round of introductions, followed by open-ended questions using the FGD guide. The guide questions addressed the following topics: PA performed before joining the THANDAV program, most preferred form of PA earlier, awareness about HIIT, reasons for joining the THANDAV program, their THANDAV experience, challenges faced while learning the dance loops, frequency of practicing, their motivation, changes in lifestyle after joining the program, benefits from the program and recommendations if any.
It was conducted in a comfortable room that allowed for good quality audio recording. Participant's assent and guardian consent were sought at the start of the FGD to record and use their anonymized quotes in research publications. When there was a lull or a pause in the conversation, the moderator used probes to stimulate discussion and encouraged those who were shy or less inclined to respond. Each FGD lasted for ∼45 min and afterward the tapes were cross checked for completeness. The recordings were transferred to the laptop, transcribed, and analyzed for themes.
Data analysis
All the data were entered into a secure software by a data entry expert and analyzed using SPSS version 16 and presented as mean ± standard deviation or n (%). The EE of dance above baseline was used to calculate METs. A paired t-test was done to estimate the increase in HR and EE. The body mass index (BMI) categories of participants were noted based on their BMI percentiles using the Indian Paediatric Academy growth charts for Indian children and adolescents. 20 The BMI %iles were categorized as follows: underweight (between 25th and 50th %ile), normal weight (between 50th and 75th %ile), overweight (between 75th and 95th %ile), and obese (>95th %ile).
The FGDs were audio recorded and transcribed verbatim manually. The transcripts were analyzed alongside the audio recording to ensure accurate transcriptions such that meaning was not lost. Content analysis was used to identify the barriers, facilitators, and acceptability of the intervention. Thematic conclusions were drawn in consensus using an ethnographical methodology and further interpreted. 21
Results
A total of 23 participants were included in the THANDAV pilot study testing. All participants were school students and 39% (9/23) reported playing outdoors for 30–60 min per day. As given in Table 1, the average age of the participants was 13.9 ± 2.1 years. The average body weight and BMI of participants were 49.4 ± 9.5 kg and 19.8 ± 3.3 kg/m2, respectively. Of the 23 participants, 6 were underweight, 11 normal weight, 3 were overweight, and 3 obese. The mean systolic BP was 107 ± 8.3 mmHg and the mean diastolic BP was 68 ± 7 mmHg. The average baseline HR and RR were 89.7 ± 8.4 bpm and 18.3 ± 5.2 breaths per minute, respectively.
Descriptive and Metabolic Parameters of the Study Population
BMI, body mass index; BP, blood pressure; HR, heart rate; IAP, Indian Academy of Paediatrics; SD, standard deviation.
At the end of the first dance, the average HR and RR increased to 185.3 ± 19.8 bpm and 43.0 ± 8.1 breaths per minute, respectively, as compared with baseline values. At the end of the second dance, the average HR increased to 189.9 ± 9.9 bpm, while the RR remained almost the same. By the end of the third dance, all participants had reached 90% of HR maximum (Fig. 3a).
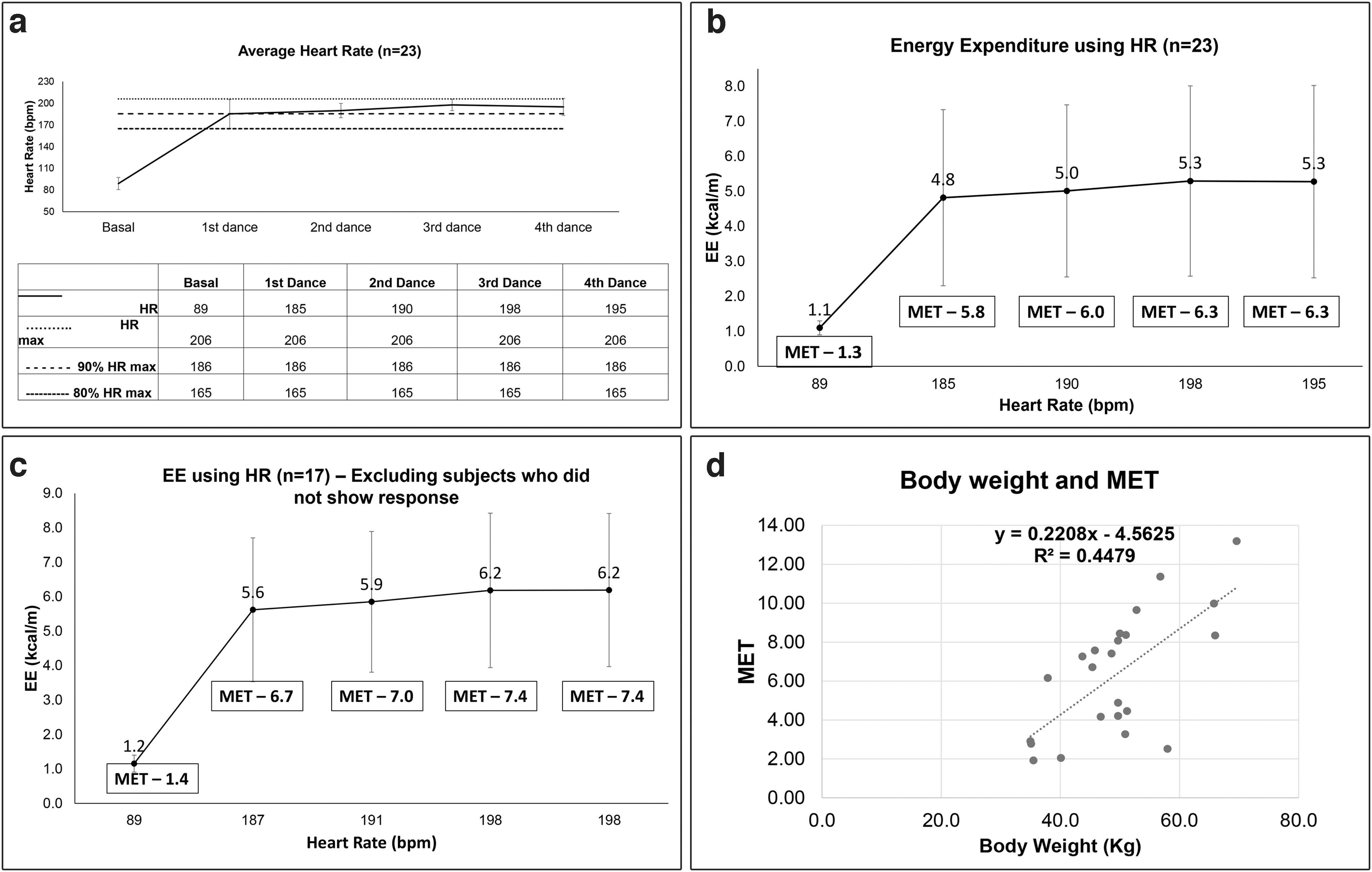
The average baseline EE was 1.2 ± 0.2 kcal/min and thereafter increased gradually (4.8 ± 2.5, 5.0 ± 2.5, and 5.3 ± 2.7 kcal/min) till the end of the third dance and then plateaued. There was a significant increase in the HR (bpm) [88.7 ± 8.4 to 195.6 ± 11.8, P < 0.001] and VO2 (L/min) [0.025 ± 0.0 to 0.395 ± 0.1, P < 0.001] postintervention. Similarly, the average MET by the end of the dance was 6.31 ± 3.29 as compared with 1.37 ± 0.3 at baseline. The average EE estimated using HR is shown in Figure 3b. However, on excluding underweight participants (n = 6) (sensitivity analysis), the average MET by the end of the dance increased significantly to 7.41 ± 2.66 as compared with 1.37 ± 0.3 at baseline (Fig. 3c).
An exploratory analysis was carried out to investigate the relationship between body weight and MET after the THANDAV routine. It was seen that the MET values increased with a rise in the body weight (R 2 = 0.45, P = 0.0005) (Fig. 3d).
Thirteen participants participated in two FGDs and based on the data obtained during this process, the conversations were transcribed and extracted to arrive at the following major five prominent themes (Table 2):
Emergent Themes from the THANDAV Focused Group Discussion
HIIT, High-Intensity Interval Training; PA, physical activity.
PA routine before THANDAV/awareness about HIIT
Reasons to join THANDAV
Experience with THANDAV
Challenges faced while learning and practising
Changes in lifestyle: benefits and recommendations.
Participants described THANDAV as a unique intervention that required less time and could be done anywhere and anytime. They had a lot of fun learning and practising dance based on peppy and popular Bollywood numbers and some folk songs along with their friends. This made the intervention enjoyable and hence while performing the dance they felt happy. They said after performing the 10-min routine, with time they would cool down easily (indicating an improvement in fitness) and their body felt very light and relaxed. They also felt energetic and more active every time they performed the THANDAV routine. They reported they wanted to learn more and had also taught friends and family the routine. Two participants reported stomach cramps during the activity (probably due to drinking excess water or lack of adequate breakfast, respectively); other than these, no adverse effects were noted. None of the participants reported an inability to perform THANDAV due to their menstrual cycle.
Discussion
There are two groups of findings from the pilot study. First, the THANDAV protocol met the HIIT norms for EE. The MET values indicated that THANDAV can be considered moderate-to-vigorous physical activity (MVPA) because the average MET was in the vigorous range (i.e., >6). Second, qualitative feedback from participants indicated the THANDAV intervention was interesting, fun, energetic, took less time to do, and was socially/culturally acceptable to Asian Indian adolescent girls.
Among the different types of PA interventions, studies have shown that HIIT has a positive effect on glucose control and overall cardiometabolic health in adults, children, and adolescents. 22 –24 The evidence suggests that a minimum of 7 weeks intervention including sessions based on running, at an intensity of >90% HRmax and 100%–130% maximal aerobic velocity for two to three times a week, can result in the greatest improvements in participant health. 25 In two different systematic reviews and meta-analyses studying the effect of HIIT in improving health-related fitness in adolescents, it was concluded that HIIT is a feasible and time-efficient approach for improving cardiorespiratory fitness in adolescents. 26,27 Reviewing high-intensity intermittent exercise, Boutcher SH 13 states that it increases both aerobic and anaerobic fitness, lowers insulin resistance, brings about significant skeletal muscle adaptations, and improves glucose tolerance.
Dance, as an art form, helps an individual to learn, enjoy, and work out at the same time. 28 It has also been shown that by manipulating the structure of dance classes, individuals may be able to obtain their daily recommended duration of MVPA. 29,30 In a recent study, 37 overweight or obese girls aged 14–18 years were randomly assigned to a 12-week group-based dance exergaming or the control group. The intervention group attended 60-min group exergaming sessions three times per week for 12 weeks. The results showed a self-reported increase in PA and reduced television/video watching. 31
In another study, 149 girls (11–18 years) were enrolled in dance classes and their PA was assessed with accelerometry for 8 consecutive days. The results showed that the dance classes contributed to 29% of the girl's total MVPA. Also, girls accumulated 70% more MVPA and 8% less sedentary behavior. 32 In another study, girls aged 7–21 years, with BMI over the 85th percentile, and at risk for weight-related problems (those with polycystic ovary syndrome, diabetes mellitus, or insulin resistance) attended a 45-min dance-based session (Zumba, fitness, Kukuwa, or African Dance) once weekly for 3–6 months. This was followed by a 15–20 min discussion about health-related topics. Postintervention, the study participants showed an increase in the Physical Activity Enjoyment Scale, decrease in systolic BP, waist circumference, triglycerides, and metabolic syndrome severity. 33
In the Indian context, it has long been considered culturally acceptable for girls and women to learn dance, and this removes one of the main barriers to PA in this population. To our knowledge, this is the first study that has integrated dance and HIIT to improve physical fitness. Feeling accepted and included while doing PA is a motivating factor for the sustainability of any activity. This was illustrated in a study on adolescents that emphasized the importance of feeling confident and not being judged for having fun when participating in any PA. 34,35 In another qualitative study by Sundar et al., adolescents reported “Mastering a physical activity, being together with friends and having fun promoted motivation to perform sports.” 36
There are not many culturally tailored PA interventions reported in the literature and even fewer when it comes to women and girls. The Latino Health Project involved a cultural adaptation of an ongoing intervention to include foods and PAs commonly used in the Latino culture. They mainly used dancing and soccer as forms of PA and conducted 20 weekly group sessions incorporating motivational interviewing techniques at a local Latino community organization. Their results showed a reduction in body weight, BMI, and systolic BP. 37
In another project called the Family Affair Program, African American girls (10–14 years) were recruited if they had a mother or primary female caregiver willing to attend concurrent intervention sessions with them. The intervention included culturally tailored PA, healthy eating, and social support for 9 months. One of the primary PA strategies was weekly group exercise classes led by female, mainly African American (all but one who was Latina) instructors that included a 5-min warm-up, a 30–45-min training session, and a 5–10-min interactive education-based cool down. Instructors provided activity modifications during the training session to accommodate the various fitness levels of the participants. The results showed positive trends in eating and PA. Also, daughters and mothers who completed the intervention reported improvements in personal relationships and communication. 38
Another study investigated the effects of dancing on postural stability of 26 female dance students and 25 healthy active female college students matched in height and weight. The dancers received 3 h dance training per week. Static and dynamic standing balances were measured by means of Biodex Stability System. The results showed that dancing resulted in better postural stability and less visual dependence on postural control in adolescent females. 39
In the case of THANDAV, the routines were based on the latest Bollywood/Indian film music/album/folk songs with which the adolescents could connect easily. This feature made THANDAV unique, interesting, and enjoyable. Easy and repetitive steps helped the participants learn them fast. The girls loved practicing and performing the THANDAV routine together and learning while teaching each other. Teaching the THANDAV routine to family and friends also gave them self-confidence, recognition, and a feeling of being fit and happy. The comfort of doing THANDAV intervention even at home and the short time required were positive points in favor of the intervention.
It has been shown that childhood and adolescent behaviors tend to track into adulthood and PA is no exception. 40 A physically active child or adolescent is likely to remain so even in adulthood, thereby reducing his/her lifetime risk of developing metabolic NCDs. 2,41 In a country like India, interventions such as THANDAV have the potential to be scalable to a larger audience. By utilizing positive peer pressure, creating a socially acceptable environment, and improving engagement to enhance sustainability, THANDAV has promise for improving health and fitness in adolescent girls. We plan to build “THANDAV” into a social media technology platform where people can share their dance videos and encourage their buddies to take up an interesting and healthier habit that will boost not just their body image but also self-confidence.
Strengths and limitations
The main strength of the study was that it is the first of its kind to evaluate a novel intervention that addresses an important need; that is, lack of PA among girls in India. The study protocol was developed by professionals, and measurements were done by experts in an established physiology laboratory allowing us to measure the volume of oxygen consumed (VO2) and VCO2 produced during the THANDAV intervention.
The main limitation of the study was the small sample size. As this was a pilot study based on convenience sampling, the generalizability of these results is limited. However, based on the learnings from this we are now set to implement THANDAV on a larger sample size of adolescent girls in a randomized trial mode. Also, we could not do continuous HR monitoring as we did not have access to Fitbits, and although we had the Polaris device, we were unable to keep the device in place as the participants jumped, twirled, and moved continuously. Another limitation is that there is a minor risk of injury if HIIT is not done properly or if done too frequently. Hence, it is not recommended to do THANDAV more than three times a week. 42 Lastly, dance though socially/culturally admissible may not be acceptable in all families.
Conclusions
The main barriers to PA among women and girls in India include time constraints and exercise not being considered “culturally acceptable.” Dance is a socially and culturally accepted form of activity in India, and hence can be utilized as a tool to improve PA levels among girls, most of whom do not meet PA recommendations. The novel THANDAV intervention, which incorporates elements of Bollywood dance into a HIIT intervention, appears to be a fun, acceptable, and potentially sustainable way to increase PA among Asian Indian girls and women. Larger randomized studies are necessary to evaluate whether this intervention can lead to sustained practice and improvements in metabolic health among participants drawn from a wider age range across the Asian Indian population.
Availability of Data and Materials
The data sets analyzed during this study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions
Conceptualization of the article and writing the initial draft were carried out by R.M.A. and H.R.; Methodology was done by S.N., S.S., R.K., A.V.K., R.M.A., and H.R.; data curation was done by S.S., S.N., and H.R.; review and editing were by all authors. All authors have read and approved the final version of the article, and agree with the order of presentation of the authors.
Acknowledgments
We are grateful to Medical Research Council, United Kingdom (NIHR and UKRI) for the funding support. We also thank University of Dundee for supporting projects that advance global health. We also wish to record the support of INSPIRED project. Also, we thank all parents for their tremendous support. Lastly, this study would not have been possible without the untiring efforts of the participating children.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project has been funded by National Institute of Health Research (NIHR) and UK Research and Innovation (UKRI) under the grant number-MR/T003626/1.