
Abstract
Background:
Advanced hybrid closed-loop (AHCL) systems represent the next step of automation intended to maximize normoglycemia in people with type 1 diabetes (T1D). In the AHCL MiniMed 780G system, different algorithm glucose targets for insulin infusion are available and autocorrection boluses are delivered. The aim was to prospectively evaluate the impact of the implementation of this AHCL system in a clinical setting.
Materials and Methods:
T1D subjects using a sensor-augmented pump with predictive low-glucose suspend (SAP-PLGS) were upgraded to AHCL. Baseline, every 3 days, 2-week and 1-month sensor and pump data were downloaded. Glucose target was set to 100 mg/dL and active insulin time to 2 h for all the subjects. Time in different glucose ranges was compared.
Results:
Fifty-two T1D subjects were included (age: 43 ± 12 years, 73% females, diabetes duration: 27 ± 11 years, HbA1c: 7.2% ± 0.9%, time in SAP-PLGS: 5 ± 2 years). Time in range (TIR) 70–180 mg/dL increased from 67.3% ± 13.6% at baseline to 79.6% ± 7.9% at 1 month (P = 0.001). Time in hyperglycemia >180 and >250 mg/dL decreased from 29.4% ± 15.1% to 17.3% ± 8.6% and from 6.9% ± 7.8% to 2.5% ± 2.4%, respectively (P = 0.001). No differences in time in hypoglycemia <70 or <54 mg/dL were found. Time in Auto Mode was 97% ± 4%, and autocorrection insulin was 31% ± 14% of bolus insulin. Four hours postprandial glucose was improved from 162 ± 26 mg/dL at baseline to 142 ± 16 mg/dL at 1 month (P = 0.001). No severe hypoglycemia or diabetic ketoacidosis episodes occurred.
Conclusion:
AHCL systems allow well-controlled T1D patients to rapidly increase their TIR. The most aggressive settings allow optimal outcomes in TIR, without increasing hypoglycemia frequency.
Introduction
Sensor-augmented pumps (SAP) have been shown to improve glycemic control and reduce the frequency of hypoglycemia, compared to conventional pump therapy, in people with type 1 diabetes (T1D). Automation in these systems has evolved from insulin infusion suspension “on low” (SAP-LGS) to predictive low-glucose suspend function (SAP-PLGS), to increase hypoglycemia protection. 1,2 Real-world data have confirmed the efficacy of SAP shown in randomized clinical trials. 3 –5
Hybrid closed-loop (HCL) systems represent the next step in automation. In these systems, an insulin pump automatically infuses microboluses of insulin, based on glucose sensor values, according to a control algorithm. 6,7 The first commercialized HCL system, The Medtronic MiniMed 670G, infuses microboluses of insulin to reach a glucose target of 120 mg/dL. The pivotal trial showed a 5.5% increase in time in range (TIR) 70–180 mg/dL. 8,9 Also, real-life data have shown improved outcomes and the superiority of 670G over SAP-PLGS. 10 –15
The advanced hybrid closed-loop (AHCL) systems are meant to maximize time in normoglycemia and reduce the burden on people with T1D. The Medtronic MiniMed 780G infuses microboluses of insulin to different algorithm glucose targets, that is, 100, 110, and 120 mg/dL. The 780G system also infuses autocorrection insulin boluses to a fixed glucose target of 120 mg/dL. 16,17 The pivotal trial has shown a TIR 70–180 mg/dL of 74.5% after 3 months of use of the 780G system in 157 adolescents and adults with T1D, with improved outcomes reached using the most aggressive algorithm glucose target of 100 mg/dL. 18 A precommercial multinational randomized crossover trial has shown a reduction in time in hyperglycemia, without increasing hypoglycemia, in 113 adolescents and young adults, compared to the 670G HCL system. 19
The 780G system received regulatory approval in Europe in June 2020 and it was launched in October 2020 in many European countries.
Our study aimed to evaluate the efficacy of the AHCL system Medtronic MiniMed 780G in users of SAP-PLGS in real-life clinical practice.
Materials and Methods
A prospective longitudinal intervention study was designed. T1D subjects using the Medtronic MiniMed 640G system, with PLGS activated, were selected and upgraded to the AHCL system.
Two training sessions, of 3 h duration, were performed. Auto Mode was started after 5–10 days of Manual Mode for system initialization. The algorithm glucose target was set to 100 mg/dL for all the patients. Autocorrection was activated and active insulin time was programmed as 2 h. The carbohydrate to insulin ratios remained unchanged. The patients were instructed to use a temporal glucose target of 150 mg/dL when the risk of hypoglycemia was high, such as during exercise. Alarms were set to 70 mg/dL for low alarm and 250 mg/dL at nighttime and 220 mg/dL during daytime for high alarm, for all the patients, independently of their baseline alarm settings.
Automatic downloads were obtained, every 24 h, from subjects using a mobile phone linked to the pump. Weekly manual downloads were recommended for the subjects with no mobile phone linked with the pump, to remotely assess the safety of the system. Phone contact with a diabetes nurse was available to all the patients and was proactively encouraged. According to routine practice, clinical visits were maintained, and the system settings were adjusted according to each diabetologist's clinical judgment.
Baseline point-of-care HbA1c was measured by Afinion™ AS100. Sensor data and pump data were downloaded using the CareLink System® software. Baseline data were downloaded from the SAP-PLGS system and 780G downloads were collected 2 weeks and 1 month following the start of Auto Mode, including 2 weeks of data for every time point, that is, baseline, 2 weeks, and 1 month. In addition, pump and sensor data from every 3 days of use of the system were downloaded. TIR 70–180 mg/dL, time <70 and <54 mg/dL, and time >180 and >250 mg/dL were evaluated. In the SAP-PLGS system, time in different glucose ranges was calculated from the sensor data recorded in the CSV file exported by the CareLink System software. The same mean absolute relative difference was communicated for sensor Guardian sensor 3® in both systems. Changes in postprandial control were evaluated by comparing preprandial sensor glucose and postprandial sensor glucose for every meal, at baseline and during the 2-week and 1-month follow-up evaluations.
The protocol was conducted according to the Declaration of Helsinki principles and it was approved by the Institutional Research Ethics Committee (date: October 22, 2020). All the participants signed a written informed consent agreeing to participate in the study.
Data analysis was conducted using SPSS statistics software v22. Results are presented as mean ± standard deviation values. A paired Student's t-test was used for the analysis of differences. For unpaired samples, the independent samples t-test was used. A McNemar test was used to compare proportions for paired data. Correlation analyses were performed using the Pearson method. A P-value <0.05 was considered statistically significant.
Results
Fifty-two T1D adolescents and adults, between 15 and 65 years, were included in the study. Baseline characteristics are shown in Table 1. One additional patient (male, 25 years old) decided to stop using the system after 4 days in Auto Mode, due to unwillingness to give some control over to the system (baseline TIR 70–180 mg/dL: 67%, TIR 70–180 mg/dL after 4 days: 85%, both time <70 and <54 mg/dL: 0%), and he was excluded from the analysis. Baseline active insulin time was 3.5 ± 0.8 h. Fifty-eight percent of the subjects (n = 30) were using faster aspart insulin in the pump, both at baseline and during the study.
Baseline Demographic Characteristics
n = 52. Data are expressed as mean standard deviation unless otherwise expressed.
BMI, body mass index; CS, Clarke score; GS, Gold score; SAP-PLGS, sensor-augmented pump with predictive low glucose suspend function; SH, severe hypoglycemia episodes.
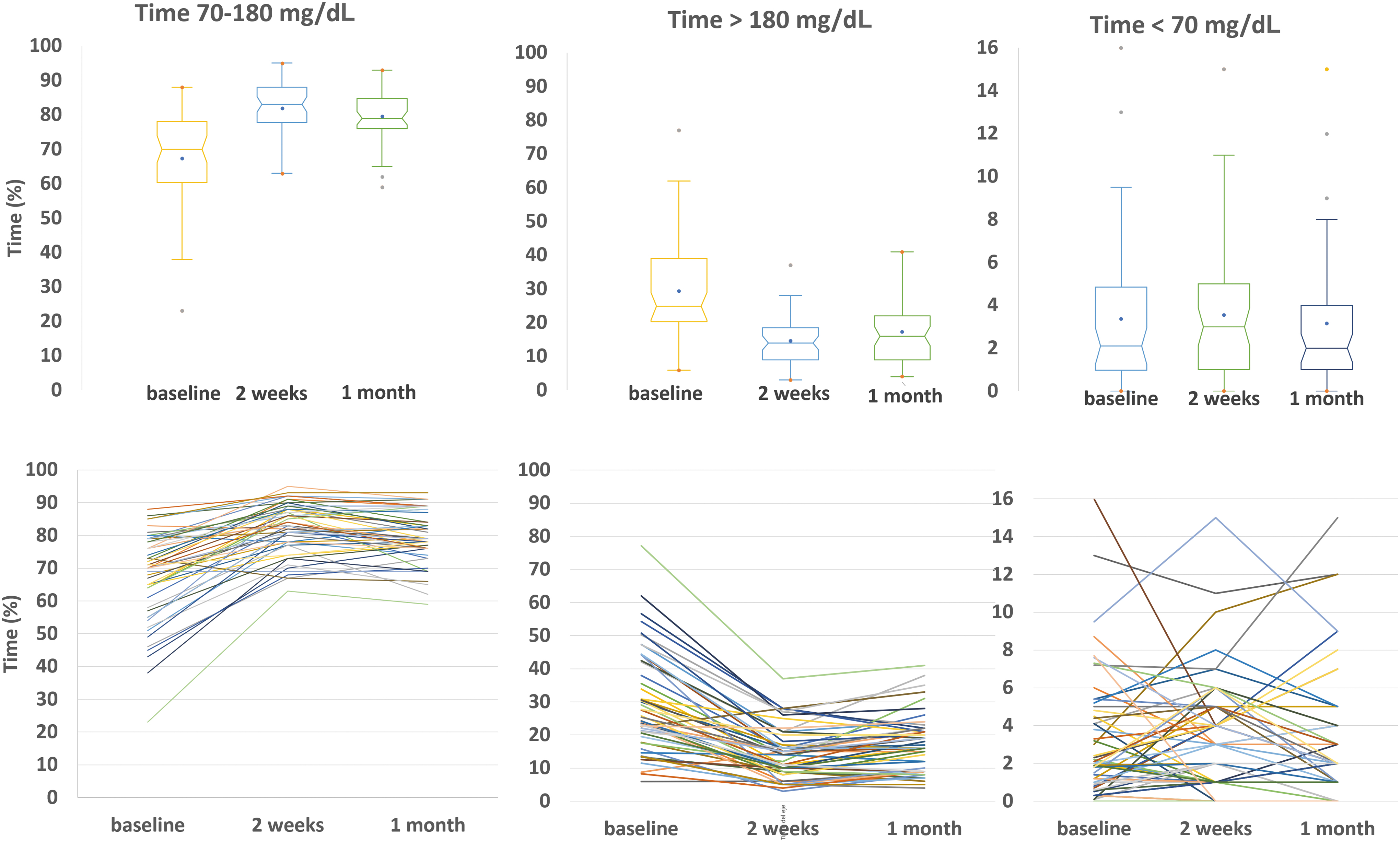
TIR 70–180 mg/dL increased from 67.3% ± 13.6% at baseline to 81.9% ± 7.8.% at 2 weeks and to 79.6% ± 7.9% at 1 month. This improvement was due to a reduction in time in hyperglycemia >180 mg/dL, from 29.4% ± 15.1% at baseline to 14.5% ± 7.7% at 2 weeks and to 17.3% ± 8.6% at 1 month. Time >250 mg/dL was also reduced from 6.9% ± 7.8% at baseline to 1.9% ± 2.0% at 2 weeks and to 2.5% ± 2.4% at 1 month (all P = 0.001). No differences in time in hypoglycemia were seen at 2 weeks or 1 month (Table 2). A 15% increase in TIR 70–180 mg/dL was detected from the first 3 days of use of the system, from 67.3% at baseline to 82.7%, and a 10% to 15% improvement was maintained in all the 3-day periods during the first month. The TIR 70–180 mg/dL, time >180, >250, <70, and <54 mg/dL at baseline, after 2 weeks and 1 month of use of the AHCL system, along with data every 3 days of use of the AHCL, are represented in Figures 1 and 2. Data from all the individuals are shown in Figure 2. No severe hypoglycemia of diabetic ketoacidosis episodes occurred during the study.
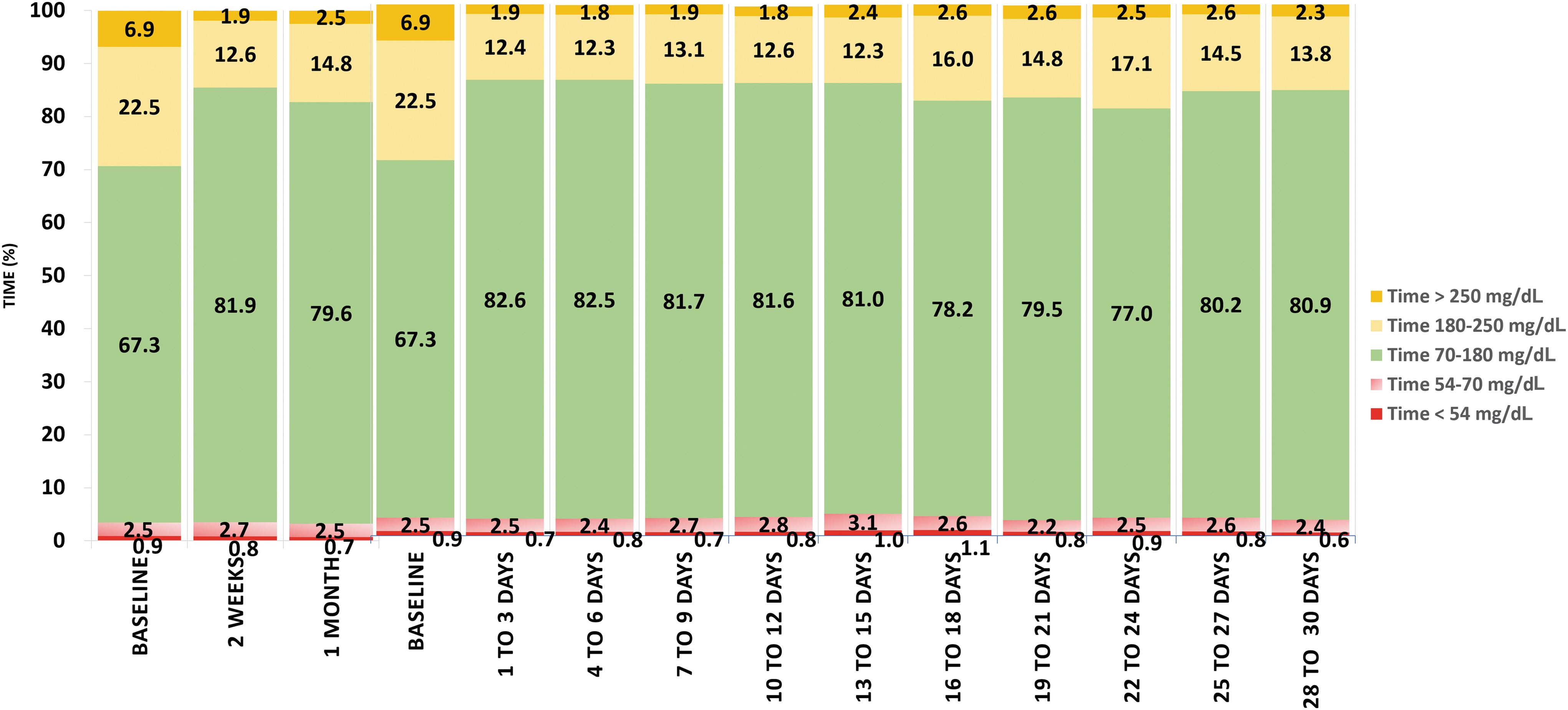
Left: time 70–180, >180, >250, <70, and <54 mg/dL at baseline (SAP-PLGS) and after 2 weeks and 1 month of use of the AHCL system. Right: time 70–180, >180, >250, <70, and <54 mg/dL at baseline (SAP-PLGS) and during every 3 days of use of AHCL in the first month of use of AHCL system. AHCL, advanced hybrid closed-loop; SAP-PLGS, sensor-augmented pump with predictive low-glucose suspend function.
Glycemic Outcomes After 2 Weeks and 1 Month of Use of Advanced Hybrid Closed-Loop System, Compared to Baseline (Sensor-Augmented Pump with Predictive Low-Glucose Suspend)
Bold values mean significant difference.
n = 52.
2 Weeks to baseline.
1 Month to baseline.
AHCL, advanced hybrid closed-loop; CV, coefficient of variation; GMI, glucose management indicator; SD, standard deviation; SMBG, self-monitoring of blood glucose; TIR, time in range.
The fraction of subjects with glucose management indicator (GMI) ≤7% increased from 62% (n = 32) at baseline to 94% (n = 49) at 2 weeks (P = 0.001) and to 89% (n = 46) at 1 month (P = 0.007). The percentage of subject with TIR 70–180 mg/dL >70% increased from 46% (n = 24) at baseline to 89% (n = 46) at 2 weeks and to 85% (n = 44) at 1 month (both P = 0.001). The percentage of patients with the optimal combination of TIR 70–180 mg/dL >70% and time <70 mg/dL <4% increased from 31% (n = 16) at baseline to 50% (n = 26) at 2 weeks (P = 0.031) and to 60% (n = 31) at 1 month (P = 0.003). The percentage of patients with TIR 70–180 mg/dL >70% and time <54 mg/dL <1% increased from 29% (n = 15) at baseline to 42% (n = 22) at 2 weeks and at 1 month (P = 0.024). The percentage of subjects who increased their TIR 70–180 mg/dL at least a 5% was 83% (n = 43) at 2 weeks and 75% (n = 39) of the at the 1-month evaluation.
At the 1-month evaluation, autocorrection insulin represented 31% ± 14% (8.6 ± 5.8 U/day) of total bolus insulin and 29 ± 10 autocorrection boluses were delivered per day. An increase in the total daily insulin dose was found, compared to baseline [43.6 ± 20.0 U/day at baseline vs. 47.4 ± 24.1 U/day at 1 month, 0.6 ± 0.2 U/(kg·day) at baseline vs. 0.7 ± 0.3 U/(kg·day) at 1 month, P = 0.001], along with an increase in the percentage of bolus insulin (48.6% ± 11.7% at baseline vs. 58.3% ± 7.4% at 1 month, P = 0.001) (Table 2). A significant negative correlation was found between the percentage of autocorrection insulin and the TIR 70–180 mg/dL (Pearson coefficient r: −0.752, P = 0.001). Patients with TIR 70–180 mg/dL >70% received a lower percentage of autocorrection insulin than patients who did not reach the 70% target (28% ± 10% vs. 51% ± 6%, P = 0.001).
At the end of the study, time in Auto Mode was 97% ± 4% and the number of exits from Auto Mode to Manual Mode was 0.8 ± 0.7 per week. The main reason for exit to Manual Mode was “Auto Mode disabled by the user,” which accounted for 0.3 exits per week and “end of sensor life,” which accounted for 0.2 exits per week.
No changes in active insulin time or algorithm glucose targets were performed during the study.
The number of meals per day was increased from 3.1 ± 1.0 at baseline to 3.7 ± 0.9 at 1 month (P = 0.001) with an increase in carbohydrate intake from 138 ± 75 g/day at baseline to 155 ± 84 g/day at 1 month (P = 0.025). No significant differences in carbohydrate to insulin ratios were found in any of the daily meals.
At baseline, preprandial sensor glucose was 151 ± 27 mg/dL and 4-h postprandial sensor glucose was 162 ± 26 mg/dL. At 1 month, preprandial sensor glucose was 143 ± 25 mg/dL and 4-h postprandial sensor glucose was 142 ± 16 mg/dL (P = 0.001 compared to baseline). The mean 4 h-postprandial increase was 11 mg/dL at baseline and −1 mg/dL at 1 month (P = 0.002).
The mean 3 h postprandial glucose increase was 12 mg/dL at baseline, from 151 ± 27 to 163 ± 27 mg/dL. The mean 2 h postprandial glucose increase, at the 1-month evaluation, was 11 mg/dL, from 143 ± 25 to 154 ± 23 mg/dL. The same time cutoff was not available in the CareLink System for both SAP-PLGS and AHCL.
There was a positive correlation between the 2 and 4 h postprandial sensor glucose and the percentage of autocorrection bolus insulin at the 1-month evaluation (Pearson coefficient r = 0.774 and 0.723, respectively, both P = 0.001).
Discussion
Our study shows an immediate improvement in glycemic control after implementing the Medtronic MiniMed 780G AHCL system in adults and adolescents with T1D in a real-life clinical context. A 12.3% increase in TIR 70–180 mg/dL was achieved in the first month of use of the system, in well-controlled and experienced SAP-PLGS users. A nearly completely suppressed risk of major hyperglycemia was found. No changes in the frequency of hypoglycemia were seen; in this sense, it must be emphasized that the time in the hypoglycemia ranges was already low at baseline, below the international consensus recommendation, 20,21 thus further improvement using AHCL would not be expected. The most aggressive settings available in the system were selected for all the patients from the beginning of the study to the end of the evaluation period, that is, an algorithm glucose target of 100 mg/dL and 2 h of active insulin time.
More than 80% of the people with T1D were able to reach the target of GMI ≤7% and stay between 70 and 180 mg/dL for >70% of the time, as recommended by international consensus. 20,21 The percentage of individuals who achieved both recommendations, a TIR 70–180 mg/dL >70% and a time <70 mg/dL <4%, increased from 31% at baseline to 60% at the 1-month evaluation. Also, the percentage of patients with TIR 70–180 mg/dL >70% and time <54 mg/dL <1% increased from 29% at baseline to 42% at 1 month.
In the pivotal study, Carlson et al. 18 found an improvement in TIR 70–180 mg/dL from 68.8% to 74.5%, after 3 months of use of the 780G system. In a subgroup of 26 subjects, the algorithm glucose target was set to 100 mg/dL and active insulin time was set to 2 h and the outcomes were improved in comparison to the whole cohort, with a TIR 70–180 mg/dL of 78.8% and 2.6% of time <70 mg/dL. Our data confirm that aggressive settings from the start are safe, as no severe hypoglycemia episodes were observed and time <54 and <70 mg/dL were below recommended levels, and that these settings allow a greater improvement in glycemic control.
A study from New Zealand has shown a 12.5% increase, from 57.9% to 70.4%, in TIR 70–180 mg/dL over SAP-PLGS after 1 month in 59 children and adults, along with improved sleep quality. 22,23 The recently published FLAIR study has shown a TIR 70–180 mg/dL of 67% with 780G, compared to 63% with 670G and a time in hyperglycemia >180 mg/dL of 34% with 780G compared to 37% with 670G, after 3 months of use, in a challenging population of adolescents and young adults with a poorer baseline glycemic control previously using the 670G system. 19
In the specific analysis of the outcomes of every 3 days of use of the 780G system, we found an extremely rapid response in TIR 70–180 mg/dL and time in hyperglycemia, with a 15% improvement in TIR 70–180 mg/dL after only 3 days of use of the system, which was maintained between 10% and 15% throughout all the 3-day periods in the first month of use of the system. To the best of our knowledge, no other reports of the very early outcomes with the use of the MiniMed 780G system have been communicated. The previous studies report outcomes only after 1 to 3 months of use of the 780G system, but not during the first days or weeks of use. 18,19,22 The immediate increase in TIR 70–180 mg/dL with the use of the MiniMed 670G system has been shown to be 4.3%, from 77.3% to 81.6%, after 2 weeks, in a very well-controlled adult population in Colombia, and 11.1%, from 54% to 65.1%, after 3 days with the 670G system, in a cohort of 30 children in Qatar. 24,25
In our group, we had previously described the benefit related to different levels of automation between pumps and sensors. With the evolution from SAP-LGS to SAP-PLGS, we found a significant reduction in time in hypoglycemia, from 4.1% to 3%, in 36 T1D patients, after 6 months of use of the 640G system. 3 In a multicentric analysis, we showed a TIR 70–180 mg/dL of 67% with SAP-PLGS in 162 subjects. 4 In comparison to SAP-PLGS, we showed an increase in TIR 70–180 mg/dL of 10%, from 63% to 73%, without changes in hypoglycemia frequency, after 3 months of use of the HCL 670G system. 13
In the present study, time in Auto Mode was 97% and the number of exits to Manual Mode was 0.8 per week. Compared to the 85% of the time in Auto Mode and the 4.2 exists per week reported with the MiniMed 670G HCL system, 13 it reflects a significant step forward into keeping the system functioning and reducing the burden on patients. Also, the number of SMBGs required by the system was lower than the number reported in the 670G system and was practically limited to the calibrations needed by the sensor. The number of alarms received per day by the patient was similar with 640G and 780G, ranging from 5 to 6, both lower than the >8 alarms per day reported with the 670G system.
A detailed evaluation of the postprandial period was performed. Better postprandial control was shown in the AHCL system, compared to SAP-PLGS. The automated basal insulin infusion added to the autocorrection boluses could help mitigate inaccurate carbohydrate estimates or delayed meal boluses, which would explain the lower postprandial increase in the AHCL system. Also, a higher percentage of autocorrection bolus insulin was related to a poorer average glycemic control and postprandial glycemic control, reflecting the fact that the system was being more challenged to reduce blood glucose levels in these scenarios.
The main limitations of our study are the short duration of evaluation, the lack of a control group and randomization, and the lack of patient satisfaction evaluation. Longer follow-up evaluations are needed to confirm these results. Also, the optimal control at baseline and the same baseline therapy in all the patients limit the extrapolation of the results to more heterogeneous populations.
The strengths of the study are the prospective design, the wide age-range of the patients, ranging from 15 to 65 years, and the real-life clinical practice conditions that could be extrapolated to similar centers in our country and other countries. Also, the standard baseline treatment and the unification of the algorithm settings allow an accurate evaluation of this aspect. To the best of our knowledge, this is the first postcommercial real-world analysis of the efficacy of the AHCL 780G system in adolescents and adults with T1D.
In conclusion, the advanced hybrid closed-loop system MiniMed 780G provides a rapid improvement in glycemic control in people with T1D with pre-existing good glycemic control in real-life conditions.
Footnotes
Authors' Contributions
All the authors declare that they made substantial contributions to the conception or design of the work, the acquisition, analysis, or interpretation of data for the work and drafting the work or revising it critically for important intellectual content. All the authors agreed to the final approval of the version to be published and to be accountable for all aspects of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.